

Abstract
Chromosome 22q11.2 deletion syndrome (22q11.2DS) is a complex developmental disorder with serious medical, cognitive and emotional symptoms across the lifespan. This genetic deletion also imparts a lifetime risk for developing schizophrenia that is 25–30 times that of the general population. The origin of this risk is multifactorial and may include dysregulation of the stress response and immunological systems in relation to brain development. Vitamin D is involved in brain development and neuroprotection, gene transcription, immunological regulation and influences neuronal signal transduction. Low levels of vitamin D are associated with schizophrenia, depression and anxiety in the general population. Yet, little is known about how vitamin D levels in children with 22q11.2DS could mediate risk of psychosis in adulthood. Blood plasma levels of vitamin D were measured in children aged 7–16 years with (n = 11) and without (n = 16) 22q11.2DS in relation to parent reports of children’s anxiety and atypicality. Anxiety and atypicality in childhood are risk indicators for the development of schizophrenia in those with 22q11.2DS and the general population. Children with 22q11.2DS had lower vitamin D levels, as well as elevated anxiety and atypicality compared with typical peers. Higher levels of anxiety, depression and internalizing problems but not atypicality were associated with lower levels of vitamin D. Vitamin D insufficiency may relate to higher levels of anxiety and depression, in turn contributing to the elevated risk of psychosis in this population. Further study is required to determine casual linkages between anxiety, stress, mood and vitamin D in children with 22q11.2DS.
Keywords: developmental disorder, DiGeorge syndrome, genetic deletion, schizophrenia risk, velocardiofacial syndrome
Chromosome 22q11.2 deletion syndrome (22q11.2DS)
22q11.2DS gives rise to a complex syndrome (formerly known as DiGeorge or velocardiofacial syndrome), with a prevalence of ~1:4000 live births and is characterized by serious medical, cognitive and socioemotional difficulties starting in infancy and extending into adulthood. Strikingly, 25–30% of these children will go on to develop a schizophrenia spectrum disorder in adulthood.1–3 The origin of this risk is not yet known but likely arises from a combination of genetic diathesis and environmental factors. Stress resulting in chronically elevated glucocorticoids (GC) and decreases in immunocompetence of a vulnerable immune system have been posited as important factors.4
Although the resulting phenotype of the deletion often varies, the majority of microdeletions in 22q11.2DS are either 3 megabases (Mb) in size or 1.5 Mb.1 Cognitive deficits are often reported in individuals with the deletion such as attention deficit/hyperactivity disorder5 lowered pre-pulse inhibition,6 and intellectual impairment.7,8 Elevated anxiety is one of the most commonly reported psychological symptoms9–12 occurring throughout the lifespan of individuals with the deletion, and is especially prevalent in children and adolescents along with mood disorders.13 Anxiety at time one is also associated with greater risk of psychosis at time two in adolescents with 22q11.2DS.14,15
Vitamin D
Vitamin D is a steroid hormone primarily recognized for its role in developing and maintaining bone health via regulation of calcium and phosphorus absorption and homeostasis. Pronounced vitamin D deficiency occurs when vitamin D levels are below 20 ng/ml; whereas individuals with levels between 21 and 29 ng/ml considered insufficient16 and levels between 30 and 32 ng/ml considered borderline insufficient.17 Concentrations of the vitamin D receptor (VDR) are significantly higher in skeletal muscle of individuals with sufficient vitamin D levels compared with those with insufficient levels.18,19 Insufficient vitamin D may be involved with the pathogenesis of several extraskeletal disorders including endocrine,20 autoimmune21,22 and several psychological disorders in the general population. Decreased vitamin D levels have been associated with anxiety, depression and schizophrenia,23–27 with low levels of vitamin D in neonates associated with a two-fold increased risk of developing schizophrenia later in life.28
Vitamin D can be obtained as vitamin D3 through UV light irradiation of a skin precursor, 7-dehydrocholesterol, or can be ingested from the diet as vitamin D3. Vitamin D is then processed in the liver, and binds to the vitamin D binding protein (DBP). Hydroxylation at this step produces the most common circulating form of vitamin D, 25(OH)D before finally being converted to the active hormonal form 1,25(OH)2D. The conversion of vitamin D to an active form occurs mainly in the kidneys via 1α-hydroxylation reaction catalyzed by the mitochondrial enzyme 1(OH)ase, or cytochrome P450 27B1 (CYP27B1),29 while the cytochrome P450 enzyme 24-hydroxylase (CYP24A1) inactivates vitamin D.30 These enzymes were originally believed to only be involved in the renal conversion of vitamin D to an active form. However, CYP27B1 and CYP24A1 along with the VDR have also been identified in several areas including the brain,31,32 indicating local synthesis in these regions rather than reliance on renal production of active vitamin D. In particular, the hypothalamus, substantia nigra and cornu ammonis (CA) 1-region and CA2 pyramidal cells in the hippocampus express high levels of the VDR.31 Local synthesis of vitamin D depends on the efficiency of CYP27B1 and availability of 25(OH)D for activation,33 while sufficient levels of 1,25(OH)2D and expression of VDR are necessary for vitamin D to have a biological effect.34
The VDR is similar to receptors in the nuclear steroid receptor family,35 with expression patterns also similar to estrogen, GC and androgen receptors.31,36 The receptor complex which forms following ligand binding to the VDR initiates transcription of several genes by binding to vitamin D response elements in the promoter region.37 In addition to the genomic pathway, vitamin D can also influence signal transduction through activation of cellular signaling pathways including the phosphatidylinositol-3 kinase and mitogen-activated protein kinase (MAPK).38
Vitamin D appears to play a neuroprotective role in the brain by regulating neurotrophic signaling crucial for neuronal development and health,39 modulating inflammation by inhibiting proinflammatory cytokines40 and regulating proteins that decrease reactive oxygen species.41 Vitamin D increases synthesis of both brain-derived neurotrophic factor, which has been implicated in the pathogenesis of schizophrenia,42 and glialderived neurotrophic factor,43 which is particularly important for dopaminergic survival and function. Vitamin D modulates inflammation by decreasing proinflammatory cytokines such as interleukin 6 (IL-6) via upregulation of the MAPK pathway.44 IL-6 has been reported as elevated45,46 and associated with lower hippocampal volume47 in schizophrenia patients.
Vitamin D and metabolism in 22q11.2DS
22q11.2DS affects structural and functional development of numerous organs. Calcification of renal48 and brain tissue49 has been reported, as well as growth retardation and hearing loss50 and abnormalities of the thymus and parathyroid glands.51 Abnormal development of the pharyngeal arches may result in hypoplastic parathyroid glands and thymus51 and consequent hypoparathyroidism.52 Similar to patients with schizophrenia,53 thymic abnormalities in children with 22q11.2DS can include reduced T-cell populations and immunodeficiency associated with an increased risk of infection during childhood.54
Hypoparathyroidism is associated with hypocalcemia-induced seizures in infants with 22q11.2DS,55 and was originally believed to be a transient symptom occurring during the prenatal period. However, more recent studies have suggested that hypoparathyroidism and hypocalcemia in 22q11.2DS2DS can continue into adulthood.55,56 Inadequate levels of parathyroid hormone secretion contribute to hypocalcemia in several ways including inadequate stimulation of renal 1α-hydroxylase activity, an enzyme necessary for vitamin D activation. As a result, insufficient 1,25-dihydroxy vitamin D (1,25(OH)2D), the active metabolite of vitamin D, is generated for intestinal absorption of calcium.57 In addition to hypocalcemia, low vitamin D concentrations have also been reported in adults with 22q11.2DS.58 Vitamin D supplementation is recommended for all patients with 22q11.2DS to correct hypocalcemia, while some cases may require treatment with calcitriol.56,59
Although vitamin D is recommended for adult and pediatric patients with 22q11.2DS as a treatment or prophylaxis against hypocalcemia,56,59 little is known about the role vitamin D plays in the etiopathology of mental illness including anxiety, depression and schizophrenia in people with 22q11.2DS. More specifically for neonates and children with 22q11.2DS, vitamin D levels may have differential effects on brain maturation associated with critical windows of developmental timing.60 In addition, animal models of vitamin D deficiency such as the VDR null mouse model display several phenotypes that are also associated with 22q11.2DS including increased anxiety and impaired pre-pulse inhibition;61 hearing loss;62 growth retardation and hypocalcemia;61,63 and brain calcification.64
The Behavior Assessment Scale for Children, 2nd Edition (BASC-2) – Parent Report subscales that measure parental impressions of their children’s anxiety and atypicality are valid predictors of prodromal psychotic symptoms in adolescence, suggesting children exhibiting both of these behaviors may be at the greatest risk of developing schizophrenia in children with 22q11.2DS.7 The atypicality subscale of the BASC-2 appears to be a valid measure of prodromal symptoms and are consistent with the development of schizophrenia in the adolescents without a known genetic deletion.65 Given the association between atypicality, anxiety and the development of psychosis, these findings demonstrate the need to identify additional biological mechanisms that may influence this relationship in individuals with 22q11.2DS as well as in the general population.
To date, little is known about what role vitamin D levels in children with 22q11.2DS could mediate risk of psychosis in adulthood despite evidence that vitamin D plays an important role in the development of disorders such as schizophrenia, depression and anxiety in the general population. Thus, the aim of this study was to determine if vitamin D availability related to behavioral markers of risk for developing psychosis in children with 22q11.2DS. We hypothesized that lower levels of plasma 25(OH)D (i.e. total 25(OH)D3 and 25(OH)D2; hereafter, ‘vitamin D’) in children with 22q11.2DS would be related to higher levels of anxiety and atypical behavior as reported by their parents.
Method
All methods were approved by the University of New Orleans (UNO) Institutional Review Board.
Participants
As part of a larger ongoing study and based on the availability of a blood sample, participants were 11 (seven boys and four girls; mean age: 12 years and 7 months, range = 9–16, S.D. = 2.06) with a diagnosis of 22q11.2DS confirmed via florescence in situ hybridization and 16 (10 boys and six girls; mean age: 11 years and 3 months, range = 7–16, S.D. = 2.30) typically developing (TD) and a parent/guardian of each child.
Psychological measures
Parents completed the BASC-2,66 which is a standardized and highly comprehensive metric of children’s behavior and emotions. Children’s intelligence was measured using the Weschler Intelligence Scale for Children, 4th Edition.67
Blood collection, storage and vitamin D assay
Blood was collected in sodium citrate-coated tubes by a trained phlebotomist at the Touro Hospital Imaging Center in New Orleans with extensive pediatric experience. Samples were then transported to UNO for processing, storage and subsequent analysis. Within 1 h of collection, blood samples were centrifuged at room temperature for 10 min at 3000 rpm and the resulting plasma supernatant was aliquoted into multiple 2 ml cryotubes and stored at −80°C until analysis.
Vitamin D assay procedures
225-OH vitamin D was measured in plasma samples using a Vitamin D EIA kit (Cayman Chemical, Ann Arbor, MI, USA). Plasma samples were purified by stripping vitamin D from the DBP according to the kit protocol to prevent binding protein interference. Two volumes of acetone were added to sample aliquots in 2 ml cryotubes before the samples were vortexed and centrifuged at 10 000 g for 10 min. The supernatant was then removed and placed into a fresh 2 ml cryotubes before being evaporated in an Eppendorf Vacufuge Concentrator (Hamburg, Germany) and reconstituted with the provided buffer in an amount equal to the original sample volume.
25-Hydroxy vitamin D3 enzyme-linked immunosorbent assay (ELISA) standards (original concentration 2.5 μg/ml) were prepared via serial dilution using the provided buffer for final concentrations of 25, 12.5, 6.25, 3.12, 1.56, 0.78, 0.39 and 0.19 ng/ml. Vitamin D-acetlycholinesterase (AChE) tracer and vitamin D ELISA monoclonal antibody were each reconstituted in 6 ml of ELISA buffer. Next, 50 μl of each standard and triplicates of 50 μl samples were loaded onto a 96-well plate. A quantity of 50 μl of the vitamin D AChE tracer and 50 μl of the vitamin D ELISA monoclonal antibody were then added to standards and samples before covering the plate and incubating for 24 h at room temperature. Following the incubation, wells were emptied and rinsed five times with wash buffer. Ellman’s reagent was reconstituted in 20 ml of ultrapure water and 20 μl was added to each well.
The 96-well plate was then covered to reduce evaporation and placed on an orbital shaker for 75 min before being read at a wavelength of 412 nm on a BioTek Eon spectrophotometers (BioTek, Winooski, VT, USA). Absorbances of non-specific binding wells were subtracted from standards and sample wells and a standard curve generated for interpolation of vitamin D concentrations (ng/ml) in sample wells using Gen5 analysis software (BioTek).
Results
Vitamin D measures
Bootstrapping at the 95 percentile confidence interval (CI) and 1000 resamples were used for all statistical analyses because of small sample sizes and unequal groups. First, an initial univariate ANOVA was conducted with vitamin D sample concentration as the dependent variable (DV), diagnosis (Dx: 22q11.2DS v. TD) as an independent variable (IV) with AGE and SEX as covariates. AGE and SEX were not significant predictors in the model and excluded in a follow-up ANOVA using the same DV and IV as outlined above. This showed a significant effect of diagnosis [F(1,25) = 9.05, P = 0.006, η2 = 2.66, bootstrapped 95% CI = 31.17, 35.66]. As shown in Fig. 1, plasma vitamin D levels were lower in the group of children with 22q11.2DS (M = 30.09 ng/ml) compared with the TD group (M = 36.73 ng/ml).
Fig. 1.
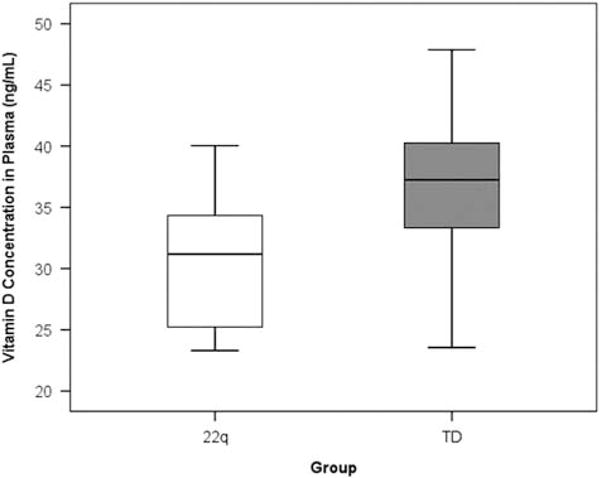
Plasma vitamin D concentrations (ng/ml) are lower in a group of children with chromosome 22q11.2 deletion syndrome compared with a group of typically-developing children.
As part of a post-hoc analysis to further explore vitamin D levels in relation to genetic diagnosis, participants were dummy-coded into high (⩾30 ng/ml) and low (<30 ng/ml) groups independent of genetic diagnosis and a Pearson’s χ2 test of independence was conducted to examine group composition of individuals with high and low vitamin D levels. There were significantly more children with borderline to deficient (<30 ng/ml) blood levels of vitamin D in the 22q11.2DS group than in the TD group [χ2(1, n = 27) = 5.80, P = 0.016].
Psychological measures
BASC-2 parent report data were available for nine children with 22q11.2DS and 13 TD children. Univariate analysis of covariance were conducted to determine which of the particular BASC-2 parent report scales differed between groups. Age and sex were included as covariates in the analysis, Bonferroni correction was applied to adjust for multiple comparisons. As shown in Table 1, groups differed on all BASC-2 scales with the exception of aggression and conduct problems.
Table 1.
Mean difference Behavior Assessment Scale for Children, 2nd Edition T-scores between children with chromosome 22q11.2 deletion syndrome and typically developing (TD) controls
| Direction | Mean difference T-score | S.E. | F | P | |
|---|---|---|---|---|---|
| Atypicality | 22qDS > TD | 16.92 | 4.95 | 11.77 | 0.004 |
| Anxiety | 22qDS > TD | 16.39 | 4.25 | 14.88 | 0.002 |
| Depression | 22qDS > TD | 14.52 | 3.82 | 14.44 | 0.002 |
| Internalizing problems | 22qDS > TD | 20.77 | 3.27 | 40.42 | 0.000 |
| Attention problems | 22qDS > TD | 20.72 | 4.26 | 23.62 | 0.000 |
| Hyperactivity | 22qDS > TD | 19.13 | 5.82 | 10.81 | 0.005 |
| Aggression | 22qDS = TD | 5.43 | 3.10 | 3.07 | 0.100 |
| Conduct problems | 22qDS = TD | 3.79 | 3.82 | 0.98 | 0.337 |
| Externalizing problems | 22qDS > TD | 10.38 | 3.69 | 7.91 | 0.013 |
| Somatization | 22qDS > TD | 19.54 | 5.39 | 13.16 | 0.002 |
| Withdrawal | 22qDS > TD | 17.44 | 5.50 | 10.07 | 0.006 |
| Behavioral symptoms index | 22qDS > TD | 20.04 | 3.38 | 35.14 | 0.000 |
| Adaptability | TD > 22qDS | 15.94 | 3.95 | 16.30 | 0.001 |
| Leadership | TD > 22qDS | 27.53 | 2.66 | 107.08 | 0.000 |
| Activities of daily living | TD > 22qDS | 23.70 | 3.54 | 44.70 | 0.000 |
| Functional communication | TD > 22qDS | 25.07 | 3.53 | 50.47 | 0.000 |
| Adaptive skills | TD > 22qDS | 26.05 | 2.83 | 84.74 | 0.000 |
| Social skills | TD > 22qDS | 18.14 | 4.18 | 18.81 | 0.001 |
Bonferroni’s correction was used to adjust for multiple comparisons (P < 0.05).
As shown in Table 2, children with 22q11.2DS had lower mean full-scale intelligence quotient (IQ) scores than TD children. Children with 22q11.2DS also had lower verbal and perceptual comprehension, working memory and processing speed index scores than TD children.
Table 2.
Mean full-scale and subscale IQ scores in children with and without chromosome 22q11.2 deletion syndrome measured using the Weschler Intelligence Scale for Children, 4th Edition (WISC-IV)
| WISC-IV scale | Diagnosis | n | Mean | S.D. | t | P |
|---|---|---|---|---|---|---|
| Full-scale IQ | 22q | 12 | 77.8333 | 15.53198 | −6.47 | 0.0001 |
| TD | 21 | 111.0952 | 13.4235 | −5.58 | 0.0001 | |
| Verbal comprehension index | 22q | 12 | 85.1667 | 13.49635 | −4.67 | 0.0001 |
| TD | 21 | 111.8571 | 13.07014 | −3.92 | 0.0001 | |
| Perceptual comprehension index | 22q | 12 | 83.8333 | 14.44635 | −6.11 | 0.0001 |
| TD | 21 | 106.7143 | 13.01208 | −6.47 | 0.0001 | |
| Working memory index | 22q | 12 | 83.8333 | 19.80741 | −5.58 | 0.0001 |
| TD | 21 | 107.381 | 14.55155 | −4.67 | 0.0001 | |
| Processing speed index | 22q | 12 | 74.5 | 10.37917 | −3.92 | 0.0001 |
| TD | 21 | 106.3333 | 16.19979 | −6.11 | 0.0001 |
TD, typically developing.
As the a priori hypothesis was that lower vitamin D levels would be associated with elevated anxiety and atypicality. A multivariate ANOVA (MANOVA) was conducted with parent-reported BASC-2 anxiety and atypicality subscales as DVs, diagnosis as the IV, with age and sex as covariates. Age and sex were not significant and thus removed from a follow-up MANOVA using anxiety and atypicality as DVs and Dx as an IV. This revealed a significant multivariate effect for anxiety and atypicality in relation to Dx [F(2,19) = 14.02, P < 0.0001, η2 = 0.60]. Univariate analyses between groups indicated a main effect for group for parent-reported BASC-2 anxiety [F(1,20) = 8.66, P < 0.008, η2 = 0.30] and atypicality [F(1,20) = 14.73, P < 0.001, η2 = 0.42]. As shown in Fig. 2, as a group, parents of children with 22q11.2DS report their children as being more anxious (22q11.2DS: T-score M = 63.00 v. TD: T-Score M = 50.69) and exhibiting more atypical behavior (22q11.2DS: T-score M = 61.22 v. TD: T-score M = 45.31) compared with the group of parents of TD children.
Fig. 2.
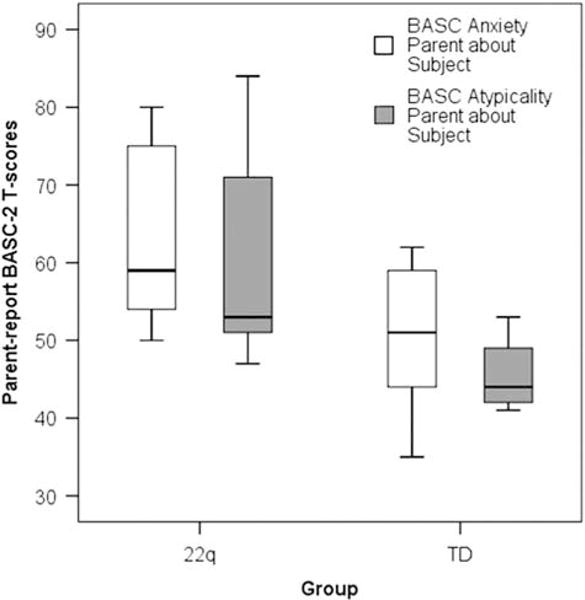
Parent reports of their child’s anxiety and atypicality as measured using the Behavior Assessment Scale for Children, 2nd Edition in children with and without chromosome 22q11.2 deletion syndrome (22q11.2DS). Children with 22q11.2DS are reported to have higher anxiety and more atypical behavior compared with their typically-developing peers.
Next, Pearson’s correlation analyses were conducted with the hypotheses that higher levels of parent-reported anxiety and atypicality regarding their child would relate to vitamin D blood concentrations. Based on the results thus far, one-tailed test was selected. As shown in Fig. 3, higher levels of anxiety [r(22) = −0.31, P = 0.04] were negatively correlated with vitamin D blood concentrations. However, BASC-2 atypicality scores were not related to vitamin D concentrations [r(22) = 0.039, P = 0.43].
Fig. 3.
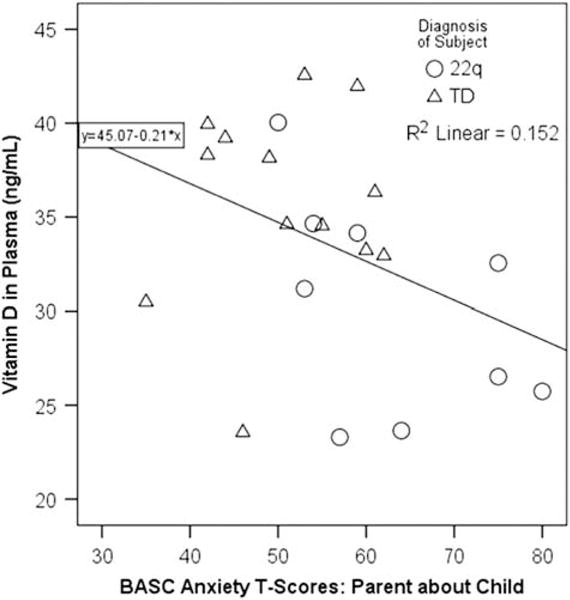
Lower levels of plasma vitamin D are associated with higher levels of anxiety as reported by parents using the Behavior Assessment Scale for Children, 2nd Edition. TD, typically developing.
To test the mediating role of vitamin D plasma level in the association between group and anxiety, a 95% bootstrap CI was utilized. A diagnosis of 22q11.2DS had a direct relationship with anxiety (β = 15.5, P = 0.005, 95% CI = 5.30, 25.70) and an inverse relationship with vitamin D levels (β = −6.85, P = 0.013, 95% CI = −12.02, −1.69). Plasma levels of vitamin D had an inverse relationship with anxiety (β = −1.19, P = 0.016, 95% CI = −2.13, −0.258). The direct effect of diagnosis on anxiety controlling for vitamin D levels was not significant (β = 11.22, P = 0.074, 95% CI = −1.26, 23.69). The indirect effect from group to anxiety was also not statistically different from 0 (β = 4.08, P = 0.25, 95% CI = −2.67, 14.88). Though analyses indicate partial mediation, there is no evidence of complete mediation through vitamin D levels. The model is illustrated in Fig. 4.
Fig. 4.
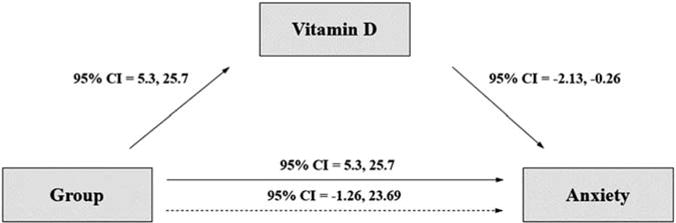
Structural equation model. CI, confidence interval.
A posteriori analyses were then conducted to examine potential relationships between other BASC-2 parent report scale findings and vitamin D levels using a series of Pearson’s correlations. Results indicated that vitamin D concentrations were negatively associated with depression [r(17) = −0.49, P = 0.02] and internalizing problems [r(17) = −0.54, P = 0.01], and positively associated with activities of daily living [r(17) = 0.43, P = 0.04]. Three follow-up mediation analyses were then conducted to investigate a possible mediating role of vitamin D concentration in the association between group and the BASC-2 depression, internalizing problems and activities of daily living subscales.
A diagnosis of 22q11.2DS had a direct relationship with depression (β = 13.99, P = 0.003, 95% CI = 5.64, 22.33). Vitamin D concentrations had an inverse relationship with depression (β = −0.27, P = 0.048, 95% CI = −0.545, −0.003). The direct effect of group on depression controlling for vitamin D concentration was significant (β = 12.38, P = 0.03, 95% CI = 1.73, 23.03). The indirect effect from group to depression controlling for vitamin D was not statistically different from 0 (95% CI = −6.37, 8.17). Therefore, vitamin D did not mediate this relationship.
A diagnosis of 22q11.2DS had a direct relationship with internalizing problems (β = 19.33, P = 0.000, 95% CI = 12.20, 26.47). Vitamin D concentration had an inverse relationship with internalizing problems (β = −108, P = 0.025, 95% CI = −2.01, −0.16). The direct effect of group on internalizing problems remained significant when controlling for vitamin D (β = 18.25, P = 0.001, 95% CI = 9.11, 27.40). The indirect effect from group to internalizing problems was not statistically different from 0 (95% CI = −3.71, 10.16). Vitamin D did not mediate this relationship.
A diagnosis of 22q11.2DS had an inverse relationship with activities of daily living (β = −22.24, P = 0.0001, 95% CI = −30.25, −14.22). Vitamin D concentrations were not significantly associated with activities of daily living in a linear regression model (β = 0.974, P = 0.087, 95% CI = −0.16, 2.12). The direct effect of group on activities of daily living remained significant when controlling for vitamin D concentration (β = −23.82, P = 0.0001, 95% CI = −34.04, −13.60). The indirect effect from group to activities of daily living was not statistically different from 0 (95% CI = −4.25, 9.00). Thus, vitamin D did not mediate this relationship either.
Possible associations between vitamin D and measures of intelligence were examined using Pearson’s correlations. Vitamin D concentration was positively associated with fullscale IQ, r(26) = 0.41, P = 0.037, as well as the Perceptual Reasoning Index, r(26) = 0.50, P = 0.009. There were no significant correlations with the remaining IQ indexes.
Discussion
The children with 22q11.2DS in the current study have elevated anxiety and atypical behavior compared with TD children according to parent reports using the BASC-2. Children with 22q11.2DS also had lower blood levels of vitamin D compared with the TD group and lower levels of vitamin D was correlated with higher levels of anxiety but not of atypicality.
In addition to the risk of developmental malformations leading to altered parathyroid function and decreased levels of vitamin D, haploinsufficiency of genes involved in vitamin D signaling may place 22q11.2DS individuals at a greater risk of psychosis. Interactions of the functional copy of a gene or genes with environmental factors, deficient genes outside the microdeletion or some combination may serve as necessary catalysts for the development of psychosis.1 The mitochondrial gene proline dehydrogenase (PRODH) is transcriptionally modulated by vitamin D, and is located within the 22q 1.5 Mb microdeletion.68 PRODH encodes the PRODH/proline oxidase enzyme that catalyzes the first step in catabolism of the glutamatergic neuromodulator proline. PRODH mutations can result in hyperprolinemia, which has been reported in patients with 22q11.2DS69 and associated with schizophrenia in the general population70 but this linkage is less clear for those with 22q11.2DS.68 More recently, Clelland et al.71 identified a mechanistic basis for one-third of the association between schizophrenia and vitamin D insufficiency, where vitamin D insufficiency leads to elevated proline levels and dysregulation of neurotransmission due to decreased expression of PRODH.
PRODH expression may partially explain the association found in the current study between vitamin D insufficiency and anxious behaviors, as PRODH has also been associated with stress reactivity and anxiety.72 While only four children in the current study had insufficient levels, six more had borderline low recommended levels of vitamin D. Further, while anxiety is a commonly reported symptom in children with 22q11.2DS, it is also one of the symptoms closely linked to the onset of psychosis.13,73 The 22q11.2DS children in our sample with deficient vitamin D levels also had the highest levels of anxiety.
Recently, a positive correlation was found between levels of serum vitamin D and right hippocampal gray matter volume in schizophrenia patients.74 Reduced hippocampal volumes have also been reported in children and adults with 22q11.2DS,75,76 which could reflect an atrophying process due to stress and associated chronic GC exposure in addition to an atypical maturational process.4 A recent series of experiments examining GC exposure in an animal model of depression lends support to this hypothesis, and suggests that hippocampal vitamin D signaling may be involved in a compensatory adaptive response to allostatic load induced by chronic stress.32,77,78
Lower vitamin D levels associated with impaired cognitive function has been reported in a number of studies.79,80,81 Similarly, for children in the current study, lower full-scale IQ and poorer perceptual reasoning was associated with lower vitamin D blood concentrations.
Exposure to chronic unpredictable mild stress increased expression of vitamin D produced locally in rat hippocampal neurons, but did not change serum levels. Such stress exposure also increased expression of CYP27B1/CYP24A1/VDR expression in the hippocampus,32 whereas a follow-up study found that repeated intraperitoneal injections of a low dose (0.2 mg/kg) of the synthetic GC dexamethasone led to a significantly greater reduction in expression of hippocampal CYP27B1, CYP24A1 and VDR proteins, compared with a high dose (2 mg/kg). The authors suggest that these results may reflect a U-shaped relationship that varies depending on the severity and duration of stress exposure; suppressing hippocampal vitamin D signaling in response to moderate stress and gradually augmenting in an adaptive response to more chronic stress. Eventually, increases in GC exposure lead to atrophy and impaired neurogenesis,82 and vitamin D signaling is only moderately activated.32 Conversely, vitamin D has been shown to be protective against hippocampal GC excess,83 and a recent in vitro study suggests that vitamin D may decrease GC receptor sensitivity.84 In contrast to the U-shaped response of vitamin D signaling proposed by Jiang et al.,32 the relationship between GC levels and hippocampal neural health tend to follow an inverted U-shaped relationship,85,86 suggesting possible feedback between vitamin D and GC signaling.
The neural diathesis–stress model proposed by Walker et al.87 suggests that vulnerability to the hypothalamic-pituitary-adrenal (HPA) system during early development interacts with several factors occurring during the adolescent period such as chronic stress, and may contribute to the onset of psychotic disorders such as schizophrenia. Furthermore, cortisol levels are significantly associated with anxiety,88,89 stressful life events90 and stress intolerance89,91,92 in individuals at ultra-high risk for the development of schizophrenia.
Future studies with larger samples of children with 22q11.2DS examining this potential relationship between chronic GC activation, hippocampal morphometry and vitamin D levels over multiple measures are warranted. Chronic stress may lead to GC-induced reduction in hippocampal expression of VDR and P450 enzymes involved in vitamin D activation. Hippocampal neurons in individuals with 22q11.2 deletion may already be vulnerable before chronic stress due to several factors including vitamin D insufficiency. Vitamin D insufficiency combined with exposure to chronic stress may be sufficient to further reduce expression of VDR and CYP27B1/CYP27A1 in the hippocampus, leading to a decrease in local production of vitamin D. As suggested by Jiang et al.,78 over time reduced expression of VDR/CYP27B1/CYP27A1 may leave hippocampal neurons vulnerable to GC-induced cell death and further increase the risk for pathologies such as anxiety, depression and the development of schizophrenia.
This is the first study to show an association between vitamin D levels and anxiety in children with 22q11.2DS. Lower vitamin D levels have been reported in other groups of children with intellectual disabilities93,94 and in adults with anxiety disorders, depression and schizophrenia.23,27,95,96 There is evidence of vitamin D as a mediating factor for developing anxiety in patients who suffered a stroke.97 Nevertheless, the relationship between lower vitamin D levels and anxiety or mood is not a foregone conclusion with ambiguous findings in relation to depression and anxiety in adult populations and when comparing men and women.96,98 Lower vitamin D levels may arise from metabolic dysfunction, medication usage, among a number of potential causes that include reduced activity and exposure to sunlight,99 which may be a common issue for children with neurodevelopmental disorders and intellectual impairment.93,94
Some notable limitations should be considered when interpreting the results of this study. Sample size was limited and there were more TD children than children with 22q11.2DS. Bootstrapping and limiting hypothesis testing to anxiety and atypicality was done to improve statistical power but likely misses more nuanced psychological profiling in relation to vitamin D levels. Larger samples would also allow for more complex statistical models that can better separate anxiety levels from diagnosis and ‘normal’ v. ‘insufficient’ vitamin D levels within groups. Seasonality was not taken into account for this study. Differences in vitamin D levels may be a result of individual lifestyle factors. No data were available on prenatal vitamin D status. Interpreting self-report data from children with neurodevelopmental disorders can be complicated by their understanding of the questions, their self-awareness and communication ability. The age range, although controlled for in analyses, may also be a confounding factor in the current study. Finally, participants were not asked to fast for 24 h before the blood draw; however, fasting is not necessary to obtain a vitamin D level100 given the 2–3-week-long circulating half-life of 25(OH)D.99
Recent evidence from animal models suggests that vitamin D deficiency during development v. adulthood may lead to different alterations in the brain, suggesting potential critical windows with outcomes depending on precise timing of deficiency.60 Further research is needed to elucidate the effects of vitamin D deficiency in a larger sample of individuals with 22q11.DS, and in particular, to examine the interaction of vitamin D insufficiency over time and during critical windows of development with other known risk factors for psychosis such as exposure to chronic stress and co-occurrence of other disorders.
Anxiety, comorbid with depression, may be of particular concern in children with 22q11.2DS, as stress-coping resources may already be depleted due to complications occurring as a result of the genetic disorder.12 Given the overlap of psychiatric disorders linked to chronic GC exposure and vitamin D insufficiency, additional studies of these factors in children with 22q11.2DS may provide targets for the prevention of psychosis in this vulnerable population. Based upon the current preliminary findings, further study will be required to clearly elucidate the role of vitamin D, anxiety and depression in children with 22q11.2DS using larger sample sizes and controlling for factors which can influence vitamin D levels such as lifestyle activities, seasonality, diet and other health-related issues which may arise as a result of the deletion phenotype.
Acknowledgments
The authors thank the families who participated in this study. They also thank Lily Turcan, Lauryn Burleigh, Rachel Bacigalupi and David Stephenson for their assistance in collecting data and the UNO Department of Biology and Dr. Wendy Schluchter for the use of their rotary evaporator.
Financial Support
This work was supported by a research grant from the National Institute of Mental Health (Beaton 5R00MH086616-05).
Footnotes
Conflicts of Interest
None.
Ethical Standards
The authors assert that all procedures contributing to this work comply with the Ethical Principles and Guidelines for the Protection of Human Subjects and with the Helsinki Declaration of 1975, as revised in 2008, and has been approved by the institutional committee at the University of New Orleans.
References
- 1.Karayiorgou M, Simon TJ, Gogos JA. 22q11.2 microdeletions: linking DNA structural variation to brain dysfunction and schizophrenia. Nat Rev Neurosci. 2010;11:402–416. doi: 10.1038/nrn2841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shprintzen RJ, Higgins AM, Antshel K, et al. Velo-cardio-facial syndrome. Curr Opin Pediatr. 2005;17:725–730. doi: 10.1097/01.mop.0000184465.73833.0b. [DOI] [PubMed] [Google Scholar]
- 3.Tang SX, Yi JJ, Calkins ME, et al. Psychiatric disorders in 22q11.2 deletion syndrome are prevalent but undertreated. Psychol Med. 2014;44:1267–1277. doi: 10.1017/S0033291713001669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Beaton EA, Simon TJ. How might stress contribute to increased risk for schizophrenia in children with chromosome 22q11.2 deletion syndrome? J Neurodev Disord. 2011;3:68–75. doi: 10.1007/s11689-010-9069-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gothelf D, Gruber R, Presburger G, et al. Methylphenidate treatment for attention-deficit/hyperactivity disorder in children and adolescents with velocardiofacial syndrome: an open-label study. J Clin Psychiatry. 2003;64:1163–1169. doi: 10.4088/jcp.v64n1004. [DOI] [PubMed] [Google Scholar]
- 6.Sobin C, Kiley-Brabeck K, Karayiorgou M. Associations between prepulse inhibition and executive visual attention in children with the 22q11 deletion syndrome. Mol Psychiatry. 2005;10:553–562. doi: 10.1038/sj.mp.4001609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Antshel KM, Shprintzen R, Fremont W, et al. Cognitive and psychiatric predictors to psychosis in velocardiofacial syndrome: a 3-year follow-up study. J Am Acad Child Adolesc Psychiatry. 2010;49:333–344. [PMC free article] [PubMed] [Google Scholar]
- 8.Swillen A, Vandeputte L, Cracco J, et al. Neuropsychological, learning and psychosocial profile of primary school aged children with the velo-cardio-facial syndrome (22q11 deletion): evidence for a nonverbal learning disability? Child Neuropsychol. 1999;5:230–241. doi: 10.1076/0929-7049(199912)05:04;1-R;FT230. [DOI] [PubMed] [Google Scholar]
- 9.Angkustsiri K, Leckliter I, Tartaglia N, et al. An examination of the relationship of anxiety and intelligence to adaptive functioning in children with chromosome 22q11. 2 deletion syndrome. J Dev Behav Pediatr. 2012;33:713–720. doi: 10.1097/DBP.0b013e318272dd24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Fung WLA, McEvilly R, Fong J, et al. Elevated prevalence of generalized anxiety disorder in adults with 22q11.2 deletion syndrome. Am J Psychiatry. 2010;167:998. doi: 10.1176/appi.ajp.2010.09101463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Niarchou M, Zammit S, van Goozen SH, et al. Psychopathology and cognition in children with 22q11. 2 deletion syndrome. Br J Psychiatry. 2014;204:46–54. doi: 10.1192/bjp.bp.113.132324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Stephenson DD, Beaton EA, Weems CF, Angkustsiri K, Simon TJ. Identifying patterns of anxiety and depression in children with chromosome 22q11. 2 deletion syndrome: comorbidity predicts behavioural difficulties and impaired functional communications. Behav Brain Res. 2014;276:190–198. doi: 10.1016/j.bbr.2014.05.056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Schneider M, Van der Linden M, Menghetti S, et al. Predominant negative symptoms in 22q11.2 deletion syndrome and their associations with cognitive functioning and functional outcome. J Psychiatr Res. 2014;48:86–93. doi: 10.1016/j.jpsychires.2013.10.010. [DOI] [PubMed] [Google Scholar]
- 14.Gothelf D, Feinstein C, Thompson T, et al. Risk factors for the emergence of psychotic disorders in adolescents with 22q11.2 deletion syndrome. Am J Psychiatry. 2007;164:663–669. doi: 10.1176/ajp.2007.164.4.663. [DOI] [PubMed] [Google Scholar]
- 15.Gothelf D, Schneider M, Green T, et al. Risk factors and the evolution of psychosis in 22q11. 2 deletion syndrome: a longitudinal 2-site study. J Am Acad Child Adolesc Psychiatry. 2013;52:1192–1203, e1193. doi: 10.1016/j.jaac.2013.08.008. [DOI] [PubMed] [Google Scholar]
- 16.Grober U, Spitz J, Reichrath J, Kisters K, Holick M. Vitamin D: update 2013: from rickets prophylaxis to general preventive healthcare. Dermatoendocrinol. 2013;5:331–347. doi: 10.4161/derm.26738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Willis KS, Smith DT, Broughton KS, Larson-Meyer DE. Vitamin D status and biomarkers of inflammation in runners. Open Access J Sports Med. 2012;3:35–42. doi: 10.2147/OAJSM.S31022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Pojednic RM, Ceglia L, Lichtenstein AH, Dawson-Hughes B, Fielding RA. Vitamin D receptor protein is associated with interleukin-6 in human skeletal muscle. Endocrine. 2014;49:512–520. doi: 10.1007/s12020-014-0505-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Pojednic RM, Ceglia L, Olsson K, et al. Effects of 1, 25-dihydroxyvitamin D3 and vitamin D3 on the expression of the vitamin D receptor in human skeletal muscle cells. Calcif Tissue Int. 2015;96:256–263. doi: 10.1007/s00223-014-9932-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Muscogiuri G, Palomba S, Caggiano M, et al. Low 25 (OH) vitamin D levels are associated with autoimmune thyroid disease in polycystic ovary syndrome. Endocrine. 2015;53:538–542. doi: 10.1007/s12020-015-0745-0. [DOI] [PubMed] [Google Scholar]
- 21.Adorini L, Penna G. Control of autoimmune diseases by the vitamin D endocrine system. Nat Clin Pract Rheumatol. 2008;4:404–412. doi: 10.1038/ncprheum0855. [DOI] [PubMed] [Google Scholar]
- 22.Holick MF. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am J Clin Nutr. 2004;80:1678S–1688S. doi: 10.1093/ajcn/80.6.1678S. [DOI] [PubMed] [Google Scholar]
- 23.Cieslak K, Feingold J, Antonius D, et al. Low vitamin D levels predict clinical features of schizophrenia. Schizophr Res. 2014;159:543–545. doi: 10.1016/j.schres.2014.08.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Graham KA, Keefe RS, Lieberman JA, et al. Relationship of low vitamin D status with positive, negative and cognitive symptom domains in people with first-episode schizophrenia. Early Interv Psychiatry. 2014;9:397–405. doi: 10.1111/eip.12122. [DOI] [PubMed] [Google Scholar]
- 25.Itzhaky D, Amital D, Gorden K, et al. Low serum vitamin D concentrations in patients with schizophrenia. Isr Med Assoc J. 2012;14:88–92. [PubMed] [Google Scholar]
- 26.Kjaergaard M, Waterloo K, Wang CEA, et al. Effect of vitamin D supplement on depression scores in people with low levels of serum 25-hydroxyvitamin D: nested case-control study and randomised clinical trial. Br J Psychiatry. 2012;201:360–368. doi: 10.1192/bjp.bp.111.104349. [DOI] [PubMed] [Google Scholar]
- 27.Maddock J, Berry DJ, Geoffroy M-C, Power C, Hyppönen E. Vitamin D and common mental disorders in mid-life: cross-sectional and prospective findings. Clin Nutr. 2013;32:758–764. doi: 10.1016/j.clnu.2013.01.006. [DOI] [PubMed] [Google Scholar]
- 28.McGrath JJ, Burne TH, Féron F, Mackay-Sim A, Eyles DW. Developmental vitamin D deficiency and risk of schizophrenia: a 10-year update. Schizophr Bull. 2010;36:1073–1078. doi: 10.1093/schbul/sbq101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Jones G, Prosser DE, Kaufmann M. Cytochrome P450-mediated metabolism of vitamin D. J Lipid Res. 2013;55:13–31. doi: 10.1194/jlr.R031534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Jones G, Prosser DE, Kaufmann M. 25-Hydroxyvitamin D-24-hydroxylase (CYP24A1): its important role in the degradation of vitamin D. Arch Biochem Biophys. 2012;523:9–18. doi: 10.1016/j.abb.2011.11.003. [DOI] [PubMed] [Google Scholar]
- 31.Eyles DW, Smith S, Kinobe R, Hewison M, McGrath JJ. Distribution of the vitamin D receptor and 1α-hydroxylase in human brain. J Chem Neuroanat. 2005;29:21–30. doi: 10.1016/j.jchemneu.2004.08.006. [DOI] [PubMed] [Google Scholar]
- 32.Jiang P, Zhang W-Y, Li H-D, et al. Stress and vitamin D: altered vitamin D metabolism in both the hippocampus and myocardium of chronic unpredictable mild stress exposed rats. Psychoneuroendocrinology. 2013;38:2091–2098. doi: 10.1016/j.psyneuen.2013.03.017. [DOI] [PubMed] [Google Scholar]
- 33.Schuster I. Cytochromes P450 are essential players in the vitamin D signaling system. Biochim Biophys Acta. 2011;1814:186–199. doi: 10.1016/j.bbapap.2010.06.022. [DOI] [PubMed] [Google Scholar]
- 34.Haussler MR, Mangelsdorf DJ, Komm BS, et al. Proceedings of the 1987 Laurentian Hormone Conference. Elsevier BV; 1988. Molecular biology of the vitamin D hormone; pp. 263–305. [DOI] [PubMed] [Google Scholar]
- 35.Mangelsdorf DJ, Thummel C, Beato M, et al. The nuclear receptor superfamily: the second decade. Cell. 1995;83:835–839. doi: 10.1016/0092-8674(95)90199-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Prüfer K, Veenstra TD, Jirikowski GF, Kumar R. Distribution of 1,25-dihydroxyvitamin D3 receptor immunoreactivity in the rat brain and spinal cord. J Chem Neuroanat. 1999;16:135–145. doi: 10.1016/s0891-0618(99)00002-2. [DOI] [PubMed] [Google Scholar]
- 37.Christakos S, Dhawan P, Liu Y, Peng X, Porta A. New insights into the mechanisms of vitamin D action. J Cell Biochem. 2003;88:695–705. doi: 10.1002/jcb.10423. [DOI] [PubMed] [Google Scholar]
- 38.Sequeira VB, Rybchyn MS, Tongkao-on W, et al. The role of the vitamin D receptor and ERp57 in photoprotection by 1α,25-dihydroxyvitamin D3. Mol Endocrinol. 2012;26:574–582. doi: 10.1210/me.2011-1161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Bernd P. The role of neurotrophins during early development. Gene Expr. 2008;14:241–250. doi: 10.3727/105221608786883799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Barker T, Martins TB, Hill HR, et al. Circulating proinflammatory cytokines are elevated and peak power output correlates with 25-hydroxyvitamin D in vitamin D insufficient adults. Eur J Appl Physiol. 2013;113:1523–1534. doi: 10.1007/s00421-012-2582-7. [DOI] [PubMed] [Google Scholar]
- 41.Ibi M, Sawada H, Nakanishi M, et al. Protective effects of 1α, 25-(OH)2D3 against the neurotoxicity of glutamate and reactive oxygen species in mesencephalic culture. Neuropharmacology. 2001;40:761–771. doi: 10.1016/s0028-3908(01)00009-0. [DOI] [PubMed] [Google Scholar]
- 42.Favalli G, Li J, Belmonte-de-Abreu P, Wong AHC, Daskalakis ZJ. The role of BDNF in the pathophysiology and treatment of schizophrenia. J Psychiatr Res. 2012;46:1–11. doi: 10.1016/j.jpsychires.2011.09.022. [DOI] [PubMed] [Google Scholar]
- 43.Wang Y, Chiang YH, Su TP, et al. Vitamin D3 attenuates cortical infarction induced by middle cerebral arterial ligation in rats. Neuropharmacology. 2000;39:873–880. doi: 10.1016/s0028-3908(99)00255-5. [DOI] [PubMed] [Google Scholar]
- 44.Zhang Y, Leung DYM, Richers BN, et al. Vitamin D inhibits monocyte/macrophage proinflammatory cytokine production by targeting MAPK phosphatase-1. J Immunol. 2012;188:2127–2135. doi: 10.4049/jimmunol.1102412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Miller GE, Chen E, Parker KJ. Psychological stress in childhood and susceptibility to the chronic diseases of aging: moving toward a model of behavioral and biological mechanisms. Psychol Bull. 2011;137:959–997. doi: 10.1037/a0024768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Schwieler L, Larsson MK, Skogh E, et al. Increased levels of IL-6 in the cerebrospinal fluid of patients with chronic schizophrenia – significance for activation of the kynurenine pathway. J Psychiatry Neurosci. 2015;40:126–133. doi: 10.1503/jpn.140126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Kalmady SV, Venkatasubramanian G, Shivakumar V, et al. Relationship between interleukin-6 gene polymorphism and hippocampal volume in antipsychotic-naïve schizophrenia: evidence for differential susceptibility? PLoS ONE. 2014;9:e96021. doi: 10.1371/journal.pone.0096021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Yong DEJ, Booth P, Baruni J, et al. Chromosome 22q11 microdeletion and congenital heart disease – a survey in a paediatric population. Eur J Pediatr. 1999;158:566–570. doi: 10.1007/s004310051148. [DOI] [PubMed] [Google Scholar]
- 49.Sieberer M, Haltenhof H, Haubitz B, et al. Basal ganglia calcification and psychosis in 22q11.2 deletion syndrome. Eur Psychiatry. 2005;20:567–569. doi: 10.1016/j.eurpsy.2005.04.002. [DOI] [PubMed] [Google Scholar]
- 50.Jyonouchi S, McDonald-McGinn DM, Bale S, Zackai EH, Sullivan KE. CHARGE (coloboma, heart defect, atresia choanae, retarded growth and development, genital hypoplasia, ear anomalies/deafness) syndrome and chromosome 22q11.2 deletion syndrome: a comparison of immunologic and nonimmunologic phenotypic features. Pediatrics. 2009;123:e871–e877. doi: 10.1542/peds.2008-3400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Kar P, Ogoe B, Poole R, Meeking D. Di-George syndrome presenting with hypocalcaemia in adulthood: two case reports and a review. J Clin Pathol. 2005;58:655–657. doi: 10.1136/jcp.2004.023218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Kapadia CR, Kim YE, McDonald-McGinn DM, Zackai EH, Katz LEL. Parathyroid hormone reserve in 22q11.2 deletion syndrome. Genet Med. 2008;10:224–228. doi: 10.1097/GIM.0b013e3181634edf. [DOI] [PubMed] [Google Scholar]
- 53.Kinney DK, Hintz K, Shearer EM, et al. A unifying hypothesis of schizophrenia: abnormal immune system development may help explain roles of prenatal hazards, post-pubertal onset, stress, genes, climate, infections, and brain dysfunction. Med Hypotheses. 2010;74:555–563. doi: 10.1016/j.mehy.2009.09.040. [DOI] [PubMed] [Google Scholar]
- 54.McLean-Tooke A, Spickett GP, Gennery AR. Immunodeficiency and autoimmunity in 22q11.2 deletion syndrome. Scand J Immunol. 2007;66:1–7. doi: 10.1111/j.1365-3083.2007.01949.x. [DOI] [PubMed] [Google Scholar]
- 55.Taylor S, Morris G, Wilson D, Davies S, Gregory J. Hypoparathyroidism and 22q11 deletion syndrome. Arch Dis Child. 2003;88:520–522. doi: 10.1136/adc.88.6.520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Cheung ENM, George SR, Costain GA, et al. Prevalence of hypocalcaemia and its associated features in 22q11.2 deletion syndrome. Clin Endocrinol. 2014;81:190–196. doi: 10.1111/cen.12466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Wheeler AL, Shoback DM. Clinical presentation of hypoparathyroidism. In: Brandi LM, Brown ME, editors. Hypoparathyroidism. Springer; Milan: 2015. pp. 155–165. [Google Scholar]
- 58.Brauner R, de Gonneville ALH, Kindermans C, et al. Parathyroid function and growth in 22q11.2 deletion syndrome. J Pediatr. 2003;142:504–508. doi: 10.1067/mpd.2003.156. [DOI] [PubMed] [Google Scholar]
- 59.Bassett AS, McDonald-McGinn DM, Devriendt K, et al. Practical guidelines for managing patients with 22q11. 2 deletion syndrome. J Pediatr. 2011;159:332–339, e331. doi: 10.1016/j.jpeds.2011.02.039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Cui X, Gooch H, Groves NJ, et al. Vitamin D and the brain: key questions for future research. J Steroid Biochem Mol Biol. 2015;148:305–309. doi: 10.1016/j.jsbmb.2014.11.004. [DOI] [PubMed] [Google Scholar]
- 61.Kalueff AV, Lou Y-R, Laaksi I, Tuohimaa P. Impaired motor performance in mice lacking neurosteroid vitamin D receptors. Brain Res Bull. 2004;64:25–29. doi: 10.1016/j.brainresbull.2004.04.015. [DOI] [PubMed] [Google Scholar]
- 62.Zou J, Minasyan A, Keisala T, et al. Progressive hearing loss in mice with a mutated vitamin D receptor gene. Audiol Neurootol. 2008;13:219–230. doi: 10.1159/000115431. [DOI] [PubMed] [Google Scholar]
- 63.Burne T, McGrath J, Eyles D, Mackaysim A. Behavioural characterization of vitamin D receptor knockout mice. Behav Brain Res. 2005;157:299–308. doi: 10.1016/j.bbr.2004.07.008. [DOI] [PubMed] [Google Scholar]
- 64.Kalueff A, Loseva E, Haapasalo H, et al. Thalamic calcification in vitamin D receptor knockout mice. Neuroreport. 2006;17:717–721. doi: 10.1097/01.wnr.0000215770.79281.e4. [DOI] [PubMed] [Google Scholar]
- 65.Thompson E, Kline E, Reeves G, Pitts SC, Schiffman J. Identifying youth at risk for psychosis using the behavior assessment system for children. Schizophr Res. 2013;151:238–244. doi: 10.1016/j.schres.2013.09.022. [DOI] [PubMed] [Google Scholar]
- 66.Reynolds CR, Kamphaus RW. Manual for Behavior Assessment System for Children. AGS Publishing; Circle Pine, MN: 1992. [Google Scholar]
- 67.Wechsler D. WISC-IV Technical and Interpretive Manual. The Psychological Corporation; San Antonio, TX: 2003. [Google Scholar]
- 68.Mowry B, Holmans P, Pulver A, et al. Multicenter linkage study of schizophrenia loci on chromosome 22q. Mol Psychiatry. 2004;9:784–795. doi: 10.1038/sj.mp.4001481. [DOI] [PubMed] [Google Scholar]
- 69.Goodman B, Rutberg J, Lin W, Pulver A, Thomas G, Geraghty M. Hyperprolinaemia in patients with deletion (22)(q11. 2) syndrome. J Inherit Metab Dis. 2000;23:847–848. doi: 10.1023/a:1026773005303. [DOI] [PubMed] [Google Scholar]
- 70.Clelland CL, Read LL, Baraldi AN, et al. Evidence for association of hyperprolinemia with schizophrenia and a measure of clinical outcome. Schizophr Res. 2011;131:139–145. doi: 10.1016/j.schres.2011.05.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Clelland JD, Read LL, Drouet V, et al. Vitamin D insufficiency and schizophrenia risk: evaluation of hyperprolinemia as a mediator of association. Schizophr Res. 2014;156:15–22. doi: 10.1016/j.schres.2014.03.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Roussos P, Giakoumaki SG, Bitsios P. A risk PRODH haplotype affects sensorimotor gating, memory, schizotypy, and anxiety in healthy male subjects. Biol Psychiatry. 2009;65:1063–1070. doi: 10.1016/j.biopsych.2009.01.003. [DOI] [PubMed] [Google Scholar]
- 73.Schneider M, Debbané M, Bassett AS, et al. Psychiatric disorders from childhood to adulthood in 22q11.2 deletion syndrome: results from the international consortium on brain and behavior in 22q11.2 deletion syndrome. Am J Psychiatry. 2014;171:627–639. doi: 10.1176/appi.ajp.2013.13070864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Shivakumar V, Kalmady SV, Amaresha AC, et al. Serum vitamin D and hippocampal gray matter volume in schizophrenia. Psychiatry Res. 2015;233:175–179. doi: 10.1016/j.pscychresns.2015.06.006. [DOI] [PubMed] [Google Scholar]
- 75.Debbané M, Schaer M, Farhoumand R, Glaser B, Eliez S. Hippocampal volume reduction in 22q11.2 deletion syndrome. Neuropsychologia. 2006;44:2360–2365. doi: 10.1016/j.neuropsychologia.2006.05.006. [DOI] [PubMed] [Google Scholar]
- 76.DeBoer T, Wu Z, Lee A, Simon TJ. Hippocampal volume reduction in children with chromosome 22q11.2 deletion syndrome is associated with cognitive impairment. Behav Brain Funct. 2007;3:54. doi: 10.1186/1744-9081-3-54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Jiang P, Xue Y, Li H-D, et al. Dysregulation of vitamin D metabolism in the brain and myocardium of rats following prolonged exposure to dexamethasone. Psychopharmacology. 2014;231:3445–3451. doi: 10.1007/s00213-014-3440-6. [DOI] [PubMed] [Google Scholar]
- 78.Jiang P, Zhang L, Zhu W, et al. Chronic stress causes neuroendocrine-immune disturbances without affecting renal vitamin D metabolism in rats. J Endocrinol Invest. 2014;37:1109–1116. doi: 10.1007/s40618-014-0191-5. [DOI] [PubMed] [Google Scholar]
- 79.Jorde R, Mathiesen EB, Rogne S, et al. Vitamin D and cognitive function: the Tromsø Study. J Neurol Sci. 2015;355:155–161. doi: 10.1016/j.jns.2015.06.009. [DOI] [PubMed] [Google Scholar]
- 80.Van der Schaft J, Koek H, Dijkstra E, Verhaar H, van der Schouw Y, Emmelot-Vonk M. The association between vitamin D and cognition: a systematic review. Ageing Res Rev. 2013;12:1013–1023. doi: 10.1016/j.arr.2013.05.004. [DOI] [PubMed] [Google Scholar]
- 81.Wehr H, Bednarska-Makaruk M. Vitamin D and cognition. Adv Psychiatry Neurol. 2016;25:49–53. [Google Scholar]
- 82.Sigwalt AR, Budde H, Helmich I, et al. Molecular aspects involved in swimming exercise training reducing anhedonia in a rat model of depression. Neuroscience. 2011;192:661–674. doi: 10.1016/j.neuroscience.2011.05.075. [DOI] [PubMed] [Google Scholar]
- 83.Obradovic D, Gronemeyer H, Lutz B, Rein T. Cross-talk of vitamin D and glucocorticoids in hippocampal cells. J Neurochem. 2006;96:500–509. doi: 10.1111/j.1471-4159.2005.03579.x. [DOI] [PubMed] [Google Scholar]
- 84.Ansari NN, Spilioti E, Kalotychou V, et al. Vitamin D decreases in vitro glucocorticoid sensitivity via down regulation of glucocorticoid receptor expression. Endocr Abstr. 2015 37 OC5.2. [Google Scholar]
- 85.Diamond DM, Bennett MC, Fleshner M, Rose GM. Inverted-U relationship between the level of peripheral corticosterone and the magnitude of hippocampal primed burst potentiation. Hippocampus. 1992;2:421–430. doi: 10.1002/hipo.450020409. [DOI] [PubMed] [Google Scholar]
- 86.Joëls M. Corticosteroid effects in the brain: U-shape it. Trends Pharmacol Sci. 2006;27:244–250. doi: 10.1016/j.tips.2006.03.007. [DOI] [PubMed] [Google Scholar]
- 87.Walker E, Mittal V, Tessner K. Stress and the hypothalamic pituitary adrenal axis in the developmental course of schizophrenia. Annu Rev Clin Psychol. 2008;4:189–216. doi: 10.1146/annurev.clinpsy.4.022007.141248. [DOI] [PubMed] [Google Scholar]
- 88.Corcoran CM, Smith C, McLaughlin D, et al. HPA axis function and symptoms in adolescents at clinical high risk for schizophrenia. Schizophr Res. 2012;135:170–174. doi: 10.1016/j.schres.2011.11.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Karanikas E, Antoniadis D, Garyfallos GD. The role of cortisol in first episode of psychosis: a systematic review. Curr Psychiatry Rep. 2014;16:503. doi: 10.1007/s11920-014-0503-7. [DOI] [PubMed] [Google Scholar]
- 90.Labad J, Stojanovic-Pérez A, Montalvo I, et al. Stress biomarkers as predictors of transition to psychosis in at-risk mental states: roles for cortisol, prolactin and albumin. J Psychiatr Res. 2015;60:163–169. doi: 10.1016/j.jpsychires.2014.10.011. [DOI] [PubMed] [Google Scholar]
- 91.Karanikas E, Garyfallos G. Role of cortisol in patients at risk for psychosis mental state and psychopathological correlates: a systematic review. Psychiatry Clin Neurosci. 2015;69:268–282. doi: 10.1111/pcn.12259. [DOI] [PubMed] [Google Scholar]
- 92.Pruessner M, Béchard-Evans L, Boekestyn L, et al. Attenuated cortisol response to acute psychosocial stress in individuals at ultra-high risk for psychosis. Schizophr Res. 2013;146:79–86. doi: 10.1016/j.schres.2013.02.019. [DOI] [PubMed] [Google Scholar]
- 93.Frighi V, Morovat A, Stephenson MT, et al. Vitamin D deficiency in patients with intellectual disabilities: prevalence, risk factors and management strategies. Br J Psychiatry. 2014;205:458–464. doi: 10.1192/bjp.bp.113.143511. [DOI] [PubMed] [Google Scholar]
- 94.Grant WB, Wimalawansa SJ, Holick MF, et al. Emphasizing the health benefits of vitamin D for those with neurodevelopmental disorders and intellectual disabilities. Nutrients. 2015;7:1538–1564. doi: 10.3390/nu7031538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Bicíková M, Dusková M, Vítku J, et al. Vitamin D in anxiety and affective disorders. Physiol Res. 2015;64:S101–S103. doi: 10.33549/physiolres.933082. [DOI] [PubMed] [Google Scholar]
- 96.Black LJ, Jacoby P, Allen KL, et al. Low vitamin D levels are associated with symptoms of depression in young adult males. Aust N Z J Psychiatry. 2014;48:464–471. doi: 10.1177/0004867413512383. [DOI] [PubMed] [Google Scholar]
- 97.Wu C, Ren W, Cheng J, et al. Association between serum levels of vitamin D and the risk of post-stroke anxiety. Medicine. 2016;95:e3566. doi: 10.1097/MD.0000000000003566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Bertone-Johnson ER. Vitamin D and the occurrence of depression: causal association or circumstantial evidence? Nutr Rev. 2009;67:481–492. doi: 10.1111/j.1753-4887.2009.00220.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911–1930. doi: 10.1210/jc.2011-0385. [DOI] [PubMed] [Google Scholar]
- 100.Moyad MA. Heart Health = Urologic Health and Heart Unhealthy = Urologic Unhealthy: rapid review of lifestyle changes and dietary supplements. Urol Clin North Am. 2011;38:359–367. doi: 10.1016/j.ucl.2011.05.004. [DOI] [PubMed] [Google Scholar]