

Abstract
Gastrointestinal (GI) motility disorders are commonly present in critical illness. Up to 60% of critically ill patients have been reported to experience GI dysmotility of some form necessitating therapeutic intervention. It has been attributed to various factors, related to both the underlying disease and the therapeutic interventions undertaken. The assessment of motility disturbances can be challenging in critically ill patients, as the available tests used to detect abnormal motility have major limitations in the setting of an Intensive Care Unit. Critically ill patients with GI dysmotility require a multifaceted treatment approach that addresses multiple causes and utilizes multiple pharmacological pathways. In this review, we discuss the pathophysiology, assessment and management of GI dysmotility in critically ill patients.
Keywords: Gastrointestinal motility, gastrointestinal dysmotility, critically ill
Introduction
Gastrointestinal (GI) motility disturbances are common in critical illness. Up to 60% of critically ill patients have been reported to experience GI dysmotility of some form necessitating therapeutic intervention. GI dysmotility has significant clinical consequences, being associated with feeding intolerance and malnutrition, gastroesophageal reflux (GER), bacterial overgrowth, and translocation. Recently, remarkable progress has been made in understanding the pathophysiology of GI motility in critical illness. Predominant motility abnormalities seen in Intensive Care Unit (ICU) patients include esophagus dysmotility, antral hypomotility, delayed gastric emptying, and reduced migrating motor complexes (Fig. 1).
Figure 1.
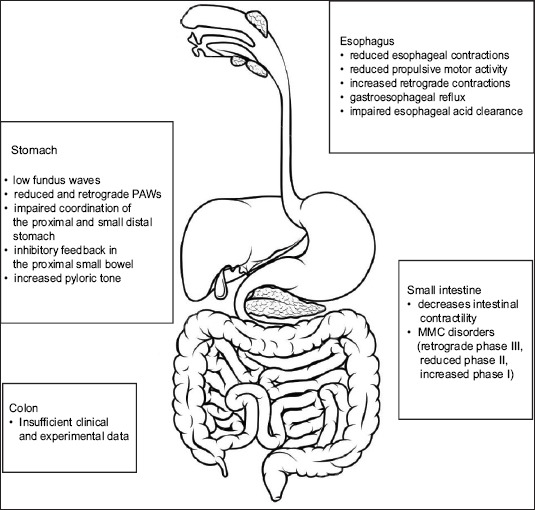
Causes of motility disorders in the gastrointestinal tract
PAWs, propagated antral waves; MMC, migrating motor complex.
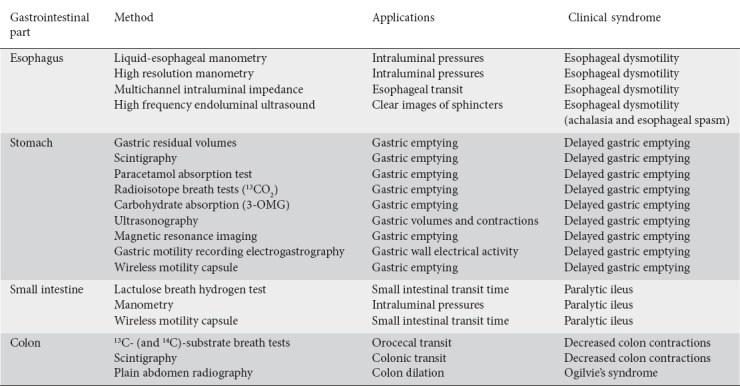
The diagnosis of GI motility disturbances can be challenging in critically ill patients, as the available tests used to detect abnormal motility have significant limitations in the ICU setting. Recognition of the type and site of an intestinal motility disorder is essential to guide the therapy and improve the outcome (Table 1). Reintam et al studied the prognostic value of the GI failure (GIF) score, a combination of intra-abdominal pressure and feeding intolerance. They showed that the GIF score might serve as an independent risk factor for ICU mortality. GIF score may also have a predictive value in addition to the sequential organ failure assessment score in outcome prediction [1]. Nevertheless, at present, there is a lack of evidence regarding clinical validation of the GIF score. Clinical symptoms such as nausea, vomiting, pain, flatus, and distention may be underestimated in the vast majority of ICU patients. Amongst the clinical signs, bowel sound auscultation has been proposed as a means of monitoring bowel motility in critically ill patients, though its sensitivity and specificity in identifying ileus are relatively low [2]. Over the last few years, novel methods of electronic monitoring have been tested, aiming to eliminate the background noise and standardize the evaluation of bowel sounds, though at present they are used mainly for research proposals [3].
Table 1.
Diagnostic methods of gastrointestinal dysmotility in critically ill patients
Concerning treatment, new general and therapeutic measures have been introduced during the last decade. Prokinetic pharmacotherapies are currently the mainstay for the management of disordered upper GI motility.
The purpose of the current review is to discuss the pathophysiology, clinical manifestations, assessment, and treatment options of GI motility disturbances in critically ill patients.
Esophageal motility disorders
The main functions of the esophagus are to transport food and fluids from the pharynx to the stomach, to prevent the passive diffusion of substances from the food into the blood, and to prevent the reflux of gastric contents into the esophagus. Food transportation from the pharynx to the stomach is attained by coordinated peristaltic contractions initiated in the upper esophagus, which temporally follows a descending wave of inhibition. The tone of the lower esophageal sphincter is critical to esophageal function. Maintenance of adequate sphincter tone is crucial for preventing the reflux of gastric contents, under positive pressures relative to the esophagus due to their location in the peritoneal cavity. The esophagus musculature consists of skeletal muscles in the upper third, smooth muscles in the lower third and a mixture of skeletal and smooth muscles in the middle part. The propulsive activity of the upper esophagus is controlled by the nucleus ambiguus of the vagus nerve, whereas the dorsal motor nucleus of the vagus nerve and the myenteric plexus control smooth muscle peristalsis [4].
Quantitative and qualitative esophageal motility disorders are commonly seen in critically ill patients, mainly in the form of reduced esophageal contractions, reduced propulsive motor activity and increased retrograde contractions, attributed to various factors related to both the underlying disease and numerous pharmaceutic interventions. Kolbel et al, in a pilot study of 15 mechanically ventilated patients, reported that, regardless of the underlying disease, the administration of sedatives and opioids is associated with a significant reduction in esophageal propulsive motility, thus implicating opioids and sedatives in the pathophysiology of esophageal motility disturbances in critical illness [5].
In critically ill patients, esophagus motility disorders are associated with significant clinical consequences related to GER and impaired esophageal acid clearance. The incidence of GER is substantially higher in the majority of patients during mechanical ventilation. Numerous potential mechanisms have been implicated in the presence of GER during mechanical ventilation, including the dynamic deterioration of salivary clearance, the pharmacological inhibition of esophageal motility—mainly with sedatives and paralyzing agents—the presence of high gastric volume and a supine body position. Nasogastric intubation, a common intervention in critically ill patients, has been proposed as a causative factor of GER [6], and a positive correlation has been reported between the duration of nasogastric intubation and the degree of erosive esophagitis. Furthermore, Nind et al have shown that reflux episodes in mechanically ventilated patients occur predominantly as a result of low or absent lower esophageal sphincter pressure (LESP), often with a superimposed cough or strain [7]. Factors that are associated with low LESP, such as sepsis, hypoventilation or hemorrhagic shock, may also contribute to the pathogenesis of GER in mechanically ventilated patients [8,9]. GER may significantly affect the mobility of critically ill patients, leading to gastric content aspiration and erosive esophagitis. Approximately 50-75% of mechanically ventilated patients experience at least one episode of pulmonary aspiration due to GER during mechanical ventilation [10].
Numerous diagnostic tests have been proposed for the assessment of esophagus dysmotility in critically ill patients, though with limited feasibility in the ICU setting [11]. Multichannel intraluminal impedance is a catheter-based method of detecting intraluminal bolus movement within the esophagus, using differences in resistance to alternating electrical current at various sites in the esophagus. In combination with liquid esophageal manometry, it can provide functional details about bolus transit in patients with esophageal motility abnormalities. It measures both viscous and liquid impedance [12], and it has been reported that the viscous test solution detects more esophageal function abnormalities than liquid testing alone [13]. High-resolution manometry has a higher number of pressure sensors and can measure the pressure pattern throughout the entire esophagus [14]. High-frequency endoluminal ultrasound has also been proposed as a means of evaluating motor abnormalities. In ambulatory patients, motility disorders, such as achalasia and esophageal spasm, have been investigated with this method, since it provides clear images of the components of the high-pressure zone of the distal and proximal esophagus, though its usage in the ICU setting is limited to research purposes only.
Stomach
The primary gastric functions are mixing and propelling food particles at a rate that facilitates the absorption of nutrients by enhancing the time they are in contact with the mucosa. Two distinct motor functional zones are recognized in the stomach: the proximal zone, which includes the fundus and the proximal third of the corpus of the stomach acting as a reservoir, and the distal zone, comprising the antrum and pylorus, which together with the proximal duodenum delivers chyme at a metered rate into the absorptive mucosa of the small intestine. The gastric reservoir function is mainly vagally and intrinsically mediated, implicating the importance of the intact function of the vagus for gastric motility. The distal stomach mixes the food with the antral contractions and regulates the outflow to the duodenum [15]. The gastric peristalsis and mixing are induced by slow waves and action potentials produced by the interstitial cells of Cajal. They are also influenced by hormonal and extrinsic neural signals and reflexes (e.g., enterogastric, gastrocolic) [1]. Gastric reservoir function and peristalsis occur during and shortly after meals, whereas during fasting the main motility pattern that is observed is the migrating motor complex.
Gastric motility can be markedly abnormal in critically ill patients, resulting in slow and delayed gastric emptying, food intolerance, and inadequate nutrition. Delayed gastric emptying is the most common gastric dysmotility pattern, in critically ill patients and has been associated with increasing severity of illness. The main pathophysiological mechanisms underlying the delayed gastric emptying in these patients are primary motor dysfunction, impaired coordination of the proximal and distal stomach, inhibitory feedback in the proximal small bowel, and a combination of the above. The impaired proximal gastric function is characterized by delayed and excessive relaxation and abolition of a dose-dependent increase in proximal gastric volume. Furthermore, fundus waves are significantly low, both at baseline and during duodenal nutrient infusion. Distal stomach dysmotility mainly involves an impaired antro-pyloro-duodenal response. A prospective case-controlled study has demonstrated a quantitative reduction in propagated antral waves (PAWs) with markedly abnormal characteristics. PAWs in critically ill patients were spread over a shorter distance, were more likely to be retrograde, rarely involved the duodenum, and in most instances they appeared to be associated with a closed pylorus [16,17].
Intrinsic myogenic activity, neural signals from the gastric myenteric plexus, parasympathetic and sympathetic nervous systems, and several hormones regulate smooth muscle activity in the stomach [18]. Common metabolic disorders associated with critical illness may induce gastric dysmotility. Hyperglycemia (glucose >140 mg/dL) has been associated with a significant reduction in gastric duodenum and jejunum motility. Hyperglycemia-induced gastric dysmotility is characterized by a reduction of phase II migrating motor complex waves [19]. Hypoxia and hypercapnia induce a significant decrease in gastric tone and motility, effects that are probably mediated by both arterial chemoreceptors and direct metabolic effects of hypoxia in muscle cells and enteric neurons.
Delayed gastric emptying has also been attributed to factors related both to the underlying disease that led to critical illness and to specific therapeutic interventions. Delayed gastric emptying is more frequently present in the elderly and in patients with brain and spinal cord injury. Up to 50% of mechanically ventilated patients and 80% of patients with intracranial hypertension will present delayed gastric emptying [20-22]. An additional factor for GI dysmotility is the administration of inotropes (dopamine, adrenergic agonist), sedatives and opiates. Propofol has been reported to be an independent predictor of gastric feeding intolerance, whereas there are conflicting results for the use of opioids [23,24]. Several studies suggest that hormones secreted by the GI tract may be implicated in the regulation of GI motility, metabolism, mucosal growth and immune function [25]. Ghrelin, an orexigenic hormone, has been shown to accelerate gastric emptying when given exogenously. Critically ill patients have been reported to have a more than 50% reduction in ghrelin’s plasma levels, suggesting that ghrelin probably contributes to delayed gastric emptying, weight loss, and decreased appetite in critically ill patients [26]. Increased levels of cholecystokinin and peptide YY, which both typically slow gastric emptying, have also been reported in the acute phase of critical illness [27]. Recent evidence suggests that gastric motility is mainly regulated by the hormone motilin. In healthy subjects, motilin accelerates gastric emptying by inducing anterograde contractions in the stomach. Motilin plasma levels increase cyclically every 90-120 min during the interdigestive fasting period, and this cyclical release of motilin disappears after ingestion of a meal. These cyclical peaks of plasma motilin are synchronized with strong peristaltic contractions initiated from the stomach and migrating to the duodenum and small intestine (phase III activity). Although fasting motilin plasma concentrations have been shown to be similar in critically ill patients and healthy subjects, plasma motilin levels are significantly higher in the patients during nutrient infusion. Furthermore, in critically ill patients there is an inverse relationship between the peak increase in plasma motilin concentrations and the peak change in proximal gastric volume induced by duodenal nutrient stimulation—a finding that may explain the persistence in interdigestive GI contractile activity and the impaired proximal gastric relaxation during enteral feeding in these patients [28].
Gastric dysmotility in critical illness may be assessed using both direct and indirect methods; in general, the preference of the method depends on the requirements of the physician/investigator. Intermittent measurement of gastric residual volumes (GRVs) is the most common practice for evaluation of gastric motility and feeding tolerance in ICU patients receiving enteral feeding. However, despite its widespread use, the utility and the significance of GRVs remain controversial, as substantial evidence is lacking regarding the correlation between GRV and gastric emptying. Moreover, this practice is deficient in standardization and is exceedingly affected by patient positioning, technique, tube location and diameter, the use of prokinetic drugs, and the composition of the liquid nutrient. In an observational study, 25% of ICU patients with GRV >150 mL—considered a cutoff for the interruption of enteral feeding in many ICUs—had normal gastric emptying [29]. Furthermore, regular GRV monitoring seems to be the main reason for discontinuation of the enteral nutrition [30]. A randomized study (NUTRIA), showed that the absence of gastric volume monitoring was not inferior to routine residual gastric volume monitoring regarding ICU-related infections, diarrhea, duration of the mechanical ventilation, length of ICU stay and mortality rates [31,32]. Additionally, several randomized controlled trials showed that a lower GRV cutoff was no safer than a higher cutoff. Consequently, the 2006 SCCM/ASPEN guidelines raised the GRV target to <500 mL. More recently, two randomized controlled trials concluded that it was safe to stop checking GRVs entirely [33,34]. In the light of this evidence, SCCM/ASPEN currently recommend the elimination of GRVs completely from routine care. GRVs should probably be monitored only in high-risk patients (e.g., abdominal surgery patients) [35]. In the research setting, particularly when studying smaller cohorts, GRVs are too imprecise, so usually direct or indirect methods are used (Table 1). Indirect tests, such as carbohydrate absorption (3-OMG) or radio-isotope breath tests (13CO2), are minimally invasive and have modest intra-subject variability. They are useful when studying the effect of an intervention thought to have a potent effect on gastric emptying in larger cohorts, particularly when researchers use a crossover design. The breath test is based on the detection of 13C-octanoate in the exhaled air following the consumption of a 13C-octanoic-acid–labeled test meal. The 13C-labeled substrate is absorbed in the duodenum, metabolized in the liver, and excreted as breath 13CO2. This test correlates gastric emptying with the 13CO2 enrichment of breath that can be measured at regular intervals over a 3-4-h period [36]. Ghoos et al have reported an excellent correlation between the gastric emptying parameters determined by the breath test and scintigraphy in healthy subjects [37]. However, in ICU patients with multi-organ dysfunction, the accuracy of the method is significantly low.
The paracetamol absorption test (PAT) is an alternative indirect method of assessing gastric emptying through peak plasma concentrations of paracetamol and can be easily performed in the ICU setting. Paracetamol is absorbed quickly and completely by the small intestine; hence, rapid gastric emptying is correlated with early peak concentrations of paracetamol [38]. A significant correlation between PAT and scintigraphy has been reported regarding the evaluation of gastric emptying. PAT is contraindicated in patients with hypersensitivity, hepatic or renal dysfunction, because of the increased risk of toxicity.
Ultrasonography is a noninvasive method that has recently been introduced for the evaluation of gastric emptying, antral wall motion, transpyloric flow and gastric accommodation [39]. Studies have shown high correlation in t1/2 liquid emptying time between ultrasonography and scintigraphy [40,41]. However, the accuracy of this method depends on the experience and skills of the operator and so far it lacks validation in critically ill patients [42].
For studying the effect of a less potent gastrokinetic drug, for a parallel design study, or when more precise measurement is required, direct tests, such as scintigraphy, are more suitable and remain the gold standard. Gastric scintigraphy evaluates gastric emptying by measuring the gastric transit of a radio-labeled meal with a gamma camera. Nevertheless, the feasibility of scintigraphy in the assessment of critically ill patients is limited, as it is time-consuming (average duration of 2-4 h) and necessitates the transportation of patient outside the ICU [43].
Magnetic resonance imaging is a newer method that has been used to measure gastric emptying [44] and accommodation [45]. Gastric emptying is measured after administration of a liquid meal containing gadolinium tetra-azacyclododecane tetra-acetic acid. It is a noninvasive test but has significant limitations, such as the transfer of the ICU patients, the cost, and the fact that it can only be performed with the patient in a supine position, which is a drawback for gastric emptying, especially of liquids [46]. Gastric motility recording electrogastrography has been used to evaluate the basic electrical activity of the stomach, but it is impractical in the ICU setting because of the prolonged recordings [47]. Manometry has been employed in ICU patients to measure gastric antrum, proximal and distal duodenum pressures [48], whereas barostat methods have not been used in trials.
Small intestine
Normally the primary motility functions in the small intestine are peristalsis, segmentation, and the migrating motor complexes during fasting periods. Motility function in the small intestine is controlled by myogenic characteristics, extrinsic and intrinsic nerve circuits, interstitial cells, hormones, and reflexes mediating the central nervous and immune system. The enteric nervous system, and mainly the myenteric plexus, seems to be the dominant regulator of the small intestine. The pathogenesis of small intestine motility disturbances in critical illness remains mostly uncertain. Sepsis overall slows upper GI transit and decreases intestinal contractility by causing dysfunction of small bowel muscularis. Excessive fluid administration has been demonstrated to cause intestinal edema, which may contribute to small bowel dysmotility [49]. Small intestine dysmotility may have a significant impact on critically ill patients’ outcomes, since previous studies have shown that it influences nutrient and drug absorption rates [50-52]. Moreover, intestinal stasis has been linked to bacterial overgrowth, potentially leading to bacterial translocation, systemic inflammatory response syndrome, sepsis, and multiple organ dysfunction syndromes. The most common clinical manifestation of small intestine dysmotility in critically ill patients is the presence of paralytic ileus.
Several diagnostic methods have been proposed for the assessment of small intestine dysmotility. The lactulose breath hydrogen test measures small intestinal transit indirectly through orocecal transit. This test is based on the fact that lactulose, administered orally, cannot be absorbed by the GI and is metabolized by colonic bacteria. The hydrogen produced is absorbed from the circulation and excreted through the lungs, indirectly indicating the orocecal transit [53]. A series of studies have shown a good correlation between lactulose breath hydrogen testing and scintigraphy when performed simultaneously with lactulose in the test meal [54-56]. However, Miller et al showed that lactulose directly accelerates small intestinal transit [57]. Small bowel manometry has also been used successfully to measure small bowel pressure waves in ICU patients.
An alternative novel technique, the wireless capsule technology, may be useful for evaluating intestinal motility in critical care patients. Measurement of GI motility with this technique is accomplished with an ingested radiocapsule that measures pressure, pH, and temperature and transmits these signals to a receiver outside the body. The method was first introduced for the evaluation of motility and transit time in ambulatory patients suffering from functional motility disorders, such as irritable bowel syndrome, functional dyspepsia, and chronic idiopathic constipation. The efficacy of the wireless motility capsule in critically ill patients was recently evaluated in two prospective studies [58,59]. Rauch et al reported a statistically significant delay in gastric emptying, intestinal transit and whole-gut transit time in a group of critically ill trauma patients. The main advantage of the wireless motility capsule in critically ill patients is that it provides an evaluation of the motility of the whole gut, eliminating the use of multiple methods. However, the presence of only one pressure sensor limits its efficacy in the evaluation of propagation and contractile forms of GI dysmotility [60].
Colon dysmotility in critical illness
There is limited evidence with regard to colon dysmotility in critical illness. During sepsis, the colon has its distinct characteristics in comparison with the small bowel, as different types of leukocyte infiltrate, and varying levels of inducible nitric oxide synthase and cyclooxygenase-2 are expressed. Although the amplitude and frequency of both colon and small intestine contraction are suppressed during endotoxin injection (or cecal ligation and puncture), there may be an anatomical explanation for these pathophysiological differences [44].
Although constipation represents the most common clinical manifestation of colon dysmotility in critically ill patients, colon dysmotility in these patients may rarely present in the form of acute pseudo-obstruction. Acute pseudo-obstruction (ACPO), also referred to as Ogilvie’s syndrome, is defined as a clinical syndrome characterized by impairment of intestinal propulsion, which may bear a resemblance to intestinal obstruction, in the absence of a mechanical cause. Acute intestinal pseudo-obstruction may also involve the small intestine and most frequently occurs in patients with stroke, myocardial infarction, peritonitis, sepsis, and postoperatively in orthopedic surgery, cesarean section, cardiovascular or lung surgery [61-63]. The pathophysiology underlying ACPO remains rather unclear, with the prevailing hypothesis being an imbalance in colonic autonomic innervation in the setting of other predisposing factors. The clinical hallmark of ACPO is the presence of dilation of the colon on a plain radiograph. The dilation favorably involves the cecum and the ascending and transverse colon, although the left colon, including the rectum, may also be affected. The prognosis of acute intestinal pseudo-obstruction varies with the underlying clinical condition.
Management of GI dysmotility
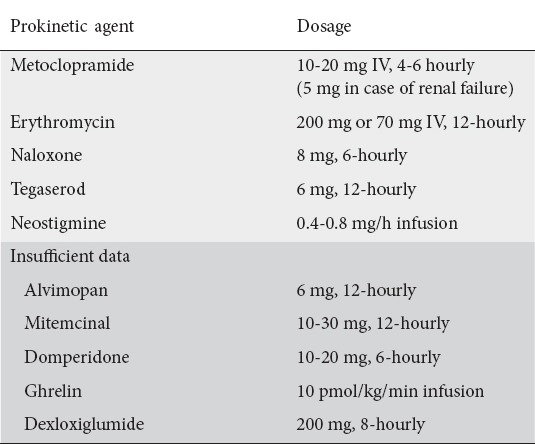
In the context of the general management of the ICU patient, several measures have been proposed for the treatment and prevention of gut dysmotility. These include patient posture, adjustment of electrolyte imbalances, control of blood glucose, appropriate management of catecholamines and drugs used for analgosedation, early enteral feeding, and use of prokinetic agents (Table 2) [64].
Table 2.
Prokinetic drugs used in management of gastrointestinal dysmotility
Glucose control
Hyperglycemia has been shown to have a negative effect on antral motor activity. Reduced fundic tone, inhibition of antral pressure waves and stimulation of pyloric pressure waves have been observed with glucose levels above 15 mmol/L. Additionally, several studies showed that a high blood glucose concentration is a positive predictor of delayed gastric emptying. Although evidence is currently lacking regarding the effect of hyperglycemia on GI motility in critically ill patients, glucose control should be considered as a measure to prevent GI dysmotility [65,66].
Enteral feeding tubes
Enteral nutrition is a conventional method for nutritional supplementation in critically ill patients with intestinal failure. Percutaneous endoscopic gastrostomy (PEG) is indicated for patients with an intact functional GI tract requiring long-term nutritional support (>30 days) [67]. Feeding tubes can be inserted directly into the stomach, endoscopically or under radiological guidance. PEG tube insertion has been shown to be the most cost-efficient and safe method compared to surgical gastrostomy [71]. It has been reported that 13-40% of patients with PEG placement experience minor complications, such as maceration due to leakage of gastric contents around the tube and peristomal pain [68-70]. Serious complications have been reported in only 0.4-4.4%, including peristomal leakage-associated peritonitis, necrotizing fasciitis of the anterior abdominal wall, gastric bleeding, internal organ injury, tumor seeding at the PEG site, and death. Post-pyloric tubes are appropriate for patients with severe GER and gastroparesis [88]. Long-term jejunal feeding can be achieved endoscopically with jejunal tubes through the PEG and direct percutaneous endoscopic jejunostomy. Retrograde dislodgement of the jejunal extension tube, tube obstruction and mechanical failure have been described as the most common device-related complications [72].
Prokinetic agents
The second therapeutic approach involves the administration of prokinetic agents such as metoclopramide, cisapride, and, more recently, erythromycin.
Metoclopramide
Metoclopramide is a drug commonly used for its antiemetic and prokinetic effects. It is a D2 antagonist—in both the central nervous system and peripheral tissues—a 5-hydroxytryptamine (5HT) 3 antagonist and 5HT4 agonist. The prokinetic effect is pharmacologically caused by the D2 receptor blockade and by the 5HT4 agonism [73]. It improves GI peristalsis, while increasing gastric emptying and patients’ tolerance of enteral nutrition [74,75]. It should be noted that prokinetic agents (metoclopramide, domperidone) given either intravenously or intramuscularly have been proven to facilitate the post-pyloric placement of nasojejunal tubes [76]. Although well-designed clinical trials are lacking, current evidence suggests that metoclopramide has a moderate prokinetic effect in critically ill patients. Compared to erythromycin, metoclopramide has a lower prokinetic effect [77]. Concerning the effect of metoclopramide in reducing the incidence of ventilator-associated pneumonia in patients receiving nasogastric enteral feeding, two randomized studies failed to prove any positive effect [78,79]. The primary side-effects of metoclopramide are nausea and extrapyramidal symptoms (dyskinesia, dystonia, convulsions, hypertonia, and tremor). Extrapyramidal manifestations are very rare (0.003%) and are mainly present in patients who require chronic use of metoclopramide.
Erythromycin
Erythromycin is a macrolide antibiotic that increases gastric motility by stimulating enteric nerves and smooth muscle and triggering a phase of the migrating myoelectric complex. Because of that effect, it has been used in diabetics with gastroparesis who were unresponsive to other treatment [80]. The antral motor effects of erythromycin in humans are mediated via different pathways. The induction of a premature activity front is mediated through activation of an intrinsic cholinergic pathway, while the induction of enhanced antral contractile activity may be mediated via a pathway potentially involving activation of a muscular receptor. These effects on gastric motility have been measured in the past by paracetamol absorption (PAT) in critically ill patients [81]. A double-blind, randomized controlled trial concluded that erythromycin is useful in the short term for delayed gastric emptying. Compared to placebo, administration of erythromycin was associated with more successful enteral feeding at both 1 and 12 h. No significant difference between the two groups was found 24 h after infusion, suggesting that administration once or twice daily may be sufficient to provide the prokinetic effect [82]. Similar results were reported in previous studies in critically ill patients and trauma patients [83,84]. Prolonged administration (>3-4 days) of erythromycin is associated with reduced efficacy. Nguyen et al found that by 24 h of erythromycin administration successful enteral feeding was achieved in 87% of ICU patients. However, the treatment became significantly less effective on day 3 (47%), while on day seven only 30% of patients were still feeding tolerant [77]. Erythromycin’s effect as a prokinetic agent is dose-dependent [85]. Low doses stimulate an antral activity front (phase III), which migrates into the duodenum and is possibly mediated by activation of an intrinsic cholinergic pathway, whereas high doses induce strong contractions of the antrum, which are not propagated and thus transit may be slower [86]. These contractions are possibly mediated via a pathway that involves activation of a muscular receptor. However, the optimal dosage for accelerating gastric emptying in the critical care setting remains uncertain. The recent cloning of the motilin receptor may help to clarify the correct dose at a molecular level [87]. One concern regarding the use of erythromycin as a prokinetic is the possible development of resistance to it as an antibiotic agent. Nevertheless, the dosage of erythromycin that is usually required to increase gastric emptying has no antibiotic effect and the risk remains theoretical. Erythromycin may promote cardiac arrhythmias through prolongation of the QT interval, including the potentially fatal ventricular arrhythmia torsades de pointes [88]. QT prolongation is due to the delayed repolarization that is thought to be the result of the blockage of human ether-a-go-go-related gene (HERG) potassium channels [89]. Several risk factors are known to increase the risk of torsades de pointes, including age, female sex, hypokalemia, history of previous QT prolongation or cardiac arrhythmia, structural heart disease and poor left ventricular function. The risk of arrhythmias is also increased with the concurrent administration of antifungal drugs (ketoconazole, itraconazole, fluconazole, astemizole and terfenadine), antiarrhythmic drugs (disopyramide, procainamide, amiodarone, sotalol, and quinidine), calcium channel blockers (diltiazem and verapamil), haloperidol and pimozide [90]. However, no serious cardiac toxicities have been reported in clinical trials, probably because of the short duration of administration [77,91]. Other non-serious adverse effects include hypotension, abdominal pain, nausea, vomiting, and diarrhea [92,93]. Watery diarrhea is the most common and can occur in up to 25% of enterally fed patients. The use of erythromycin is contraindicated in patients with myasthenia gravis, since it may trigger a myasthenic crisis [94].
Recent studies in critically ill patients support the efficacy of a combination of different prokinetics as first-line therapy for feeding intolerance. The combination of erythromycin and metoclopramide has been shown to achieve the highest efficacy of feeding tolerance with the lowest incidence of tachyphylaxis. In a double-blind, randomized study, the use of combination therapy was significantly more effective than erythromycin alone. Combination therapy was also associated with a lesser degree of drug tachyphylaxis and up to 60% of patients remained responsive at day 7 of treatment [95]. A more recent study demonstrated that combined treatment with metoclopramide 10 mg/6 h and a single low-dose IV erythromycin (10 mg/h) best facilitates gastric emptying in critically ill, mechanically ventilated patients [96]. Other novel gastrokinetic drugs, such as non-antibiotic motilin agonists, ghrelin agonists, or cholecystokinin antagonists (e.g., dexloxiglumide), could be of interest but have yet to be investigated.
Concluding remarks
GI dysmotility and feeding intolerance are common amongst critically ill patients and have been associated with significant complications that may lead to increased morbidity and mortality. Currently, treatment with prokinetics is considered as the first-line therapeutic option, as it may improve gastric emptying and nutrition delivery. Novel methods for GI motility assessment and management are required to reduce the incidence of GI dysmotility-induced complications and improve patients’ outcomes.
Biography
University Hospital of Heraklion, Medical School, University of Crete, Heraklion, Crete, Greece
Footnotes
Conflict of interest: None
References
- 1.Reintam A, Parm P, Kitus R, Starkopf J, Kern H. Gastrointestinal failure score in critically ill patients:a prospective observational study. Crit Care. 2008;12:R90. doi: 10.1186/cc6958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Li B, Tang S, Ma YL, Tang J, Wang B, Wang JR. Analysis of bowel sounds application status for gastrointestinal function monitoring in the intensive care unit. Crit Care Nurs Q. 2014;37:199–206. doi: 10.1097/CNQ.0000000000000019. [DOI] [PubMed] [Google Scholar]
- 3.Hadjileontiadis LJ. Wavelet-based enhancement of lung and bowel sounds using fractal dimension thresholding—Part I:methodology. IEEE Trans Biomed Eng. 2005;52:1143–1148. doi: 10.1109/TBME.2005.846706. [DOI] [PubMed] [Google Scholar]
- 4.Furness JB, Callaghan BP, Rivera LR, Cho HJ. The enteric nervous system and gastrointestinal innervation:integrated local and central control. Adv Exp Med Biol. 2014;817:39–71. doi: 10.1007/978-1-4939-0897-4_3. [DOI] [PubMed] [Google Scholar]
- 5.Kölbel CB, Rippel K, Klar H, Singer MV, van Ackern K, Fiedler F. Esophageal motility disorders in critically ill patients:a 24-hour manometric study. Intensive Care Med. 2000;26:1421–1427. doi: 10.1007/s001340000630. [DOI] [PubMed] [Google Scholar]
- 6.Nagler R, Spiro HM. Persistent gastroesophageal reflux induced during prolonged gastric intubation. N Engl J Med. 1963;269:495–500. doi: 10.1056/NEJM196309052691003. [DOI] [PubMed] [Google Scholar]
- 7.Nind G, Chen WH, Protheroe R, et al. Mechanisms of gastroesophageal reflux in critically ill mechanically ventilated patients. Gastroenterology. 2005;128:600–606. doi: 10.1053/j.gastro.2004.12.034. [DOI] [PubMed] [Google Scholar]
- 8.Park H, Calrk E, Cullen JJ, Conklin JL. Effect of endotoxin on opossum oesophageal motor function. Neurogastroenterol Motil. 2000;12:215–221. doi: 10.1046/j.1365-2982.2000.00202.x. [DOI] [PubMed] [Google Scholar]
- 9.LiCalzi LK, Biancani P, Behar J, Kerstein MD. Effect of hemorrhagic hypotension and hypoventilation on lower esophageal sphincter pressure. Ann Surg. 1980;192:53–57. doi: 10.1097/00000658-198007000-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.DeLegge MH. Aspiration pneumonia:incidence, mortality, and at-risk populations. JPEN J Parenter Enteral Nutr. 2002;26(6 Suppl):S19–S24. doi: 10.1177/014860710202600604. [DOI] [PubMed] [Google Scholar]
- 11.Miller L, Dai Q, Korimilli A, Levitt B, Ramzan Z, Brasseur J. Use of endoluminal ultrasound to evaluate gastrointestinal motility. Dig Dis. 2006;24:319–341. doi: 10.1159/000092886. [DOI] [PubMed] [Google Scholar]
- 12.Clayton SB, Rife C, Kalbfleisch JH, Castell DO. Viscous impedance is an important indicator of abnormal esophageal motility. Neurogastroenterol Motil. 2013;25:563–e455. doi: 10.1111/nmo.12117. [DOI] [PubMed] [Google Scholar]
- 13.BasseriB Pimentel M, Shaye OA, Low K, Soffer EE, Conklin JL. Apple sauce improves detection of esophageal motor dysfunction during high-resolution manometry evaluation of dysphagia. Dig Dis Sci. 2001;56:1723–1728. doi: 10.1007/s10620-010-1513-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.van Hoeij FB, Bredenoord AJ. Clinical application of esophageal high-resolution manometry in the diagnosis of esophageal motility disorders. J Neurogastroenterol Motil. 2016;22:6–13. doi: 10.5056/jnm15177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rhoades R, Bell DR. Medical physiology:principles for clinical medicine. 3rd edition. Baltimore: Lippincott Williams & Wilkins; 2008. [Google Scholar]
- 16.Chapman M, Fraser R, Vozzo R, et al. Antro-pyloro-duodenal motor responses to gastric and duodenal nutrient in critically ill patients. Gut. 2005;54:1384–1390. doi: 10.1136/gut.2005.065672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Nguyen NQ, Fraser RJ, Bryant LK, Chapman M, Holloway RH. Diminished functional association between proximal and distal gastric motility in critically ill patients. Intensive Care Med. 2008;34:1246–1255. doi: 10.1007/s00134-008-1036-5. [DOI] [PubMed] [Google Scholar]
- 18.Rostas JW, 3rd, Mai TT, Richards WO. Gastric motility physiology and surgical intervention. Surg Clin North Am. 2011;91:983–999. doi: 10.1016/j.suc.2011.06.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Björnsson ES, Urbanavicius V, Eliasson B, Attvall S, Smith U, Abrahamsson H. Effects of hyperglycemia on interdigestive gastrointestinal motility in humans. Scand J Gastroenterol. 1994;29:1096–1104. doi: 10.3109/00365529409094894. [DOI] [PubMed] [Google Scholar]
- 20.Heyland DK, Tougas G, King D, Cook DJ. Impaired gastric emptying in mechanically ventilated, critically ill patients. Intensive Care Med. 1996;22:1339–1344. doi: 10.1007/BF01709548. [DOI] [PubMed] [Google Scholar]
- 21.Deane AM, Summers MJ, Zaknic AV, et al. Glucose absorption and small intestinal transit in critical illness. Crit Care Med. 2011;39:1282–1288. doi: 10.1097/CCM.0b013e31820ee21f. [DOI] [PubMed] [Google Scholar]
- 22.Ott L, Young B, Phillips R, et al. Altered gastric emptying in the head-injured patient:relationship to feeding intolerance. J Neurosurg. 1991;74:738–742. doi: 10.3171/jns.1991.74.5.0738. [DOI] [PubMed] [Google Scholar]
- 23.Rhoney DH, Parker D Jr, Formea CM, Yap C, Coplin WM. Tolerability of bolus versus continuous gastric feeding in brain-injured patients. Neurol Res. 2002;24:613–620. doi: 10.1179/016164102101200456. [DOI] [PubMed] [Google Scholar]
- 24.Schurizek BA, Willacy LH, Kraglund K, Andreasen F, Juhl B. Antroduodenal motility, pH and gastric emptying during balanced anaesthesia:comparison of pethidine and fentanyl. Br J Anaesth. 1989;62:674–682. doi: 10.1093/bja/62.6.674. [DOI] [PubMed] [Google Scholar]
- 25.Baynes KC, Dhillo WS, Bloom SR. Regulation of food intake by gastrointestinal hormones. Curr Opin Gastroenterol. 2006;22:626–631. doi: 10.1097/01.mog.0000245537.43142.63. [DOI] [PubMed] [Google Scholar]
- 26.Luttikhold J, de Ruijter FM, van Norren K, et al. Review article:the role of gastrointestinal hormones in the treatment of delayed gastric emptying in critically ill patients. Aliment Pharmacol Ther. 2013;38:573–583. doi: 10.1111/apt.12421. [DOI] [PubMed] [Google Scholar]
- 27.Toumadre JP, Barclay M, Fraser R, et al. Small intestinal motor patterns in critically ill patients after major abdominal surgery. Am J Gastroenterol. 2001;96:2418–2426. doi: 10.1111/j.1572-0241.2001.03951.x. [DOI] [PubMed] [Google Scholar]
- 28.Nguyen NQ, Fraser RJ, Bryant L. Abnormalities in plasma motilin response to small intestinal nutrient stimulation in critically ill patients. Gastroenterology. 2010;138:S405. [Google Scholar]
- 29.Cohen J, Aharon A, Singer P. The paracetamol absorption test:a useful addition to the enteral nutrition algorithm? Clin Nutr. 2000;19:233–236. doi: 10.1054/clnu.2000.0097. [DOI] [PubMed] [Google Scholar]
- 30.O'Meara D, Mireles-Cabodevila E, Frame F, et al. Evaluation of delivery of enteral nutrition in critically ill patients receiving mechanical ventilation. Am J Crit Care. 2008;17:53–61. [PubMed] [Google Scholar]
- 31.Reignier J, Mercier E, Le Gouge A, et al. Clinical Research in Intensive Care and Sepsis (CRICS) Group. Effect of not monitoring residual gastric volume on risk of ventilator-associated pneumonia in adults receiving mechanical ventilation and early enteral feeding:a randomized controlled trial. JAMA. 2013;309:249–256. doi: 10.1001/jama.2012.196377. [DOI] [PubMed] [Google Scholar]
- 32.Hurt RT, McClave SA. Gastric residual volumes in critical illness:what do they really mean? Crit Care Clin. 2010;26:481–490. doi: 10.1016/j.ccc.2010.04.010. [DOI] [PubMed] [Google Scholar]
- 33.Poulard F, Dimet J, Martin-Lefevre L, et al. Impact of not measuring residual gastric volume in mechanically ventilated patients receiving early enteral feeding:a prospective before-after study. JPEN J Parenter Enteral Nutr. 2010;34:125–130. doi: 10.1177/0148607109344745. [DOI] [PubMed] [Google Scholar]
- 34.Tume LN, Bickerdike A, Latten L, Davies S, Lefèvre MH, Nicolas GW, Valla FV. Routine gastric residual volume measurement and energy target achievement in the PICU:a comparison study. Eur J Pediatr. 2017;176:1637–1644. doi: 10.1007/s00431-017-3015-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.McClave SA, Martindale RG, Vanek VW, et al. Society of Critical Care Medicine. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient:Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) JPEN J Parenter Enteral Nutr. 2009;33:277–316. doi: 10.1177/0148607109335234. [DOI] [PubMed] [Google Scholar]
- 36.Lee JS, Camilleri M, Zinsmeister AR, Burton DD, Kost LJ, Klein PD. A valid, accurate, office based non-radioactive test for gastric emptying of solids. Gut. 2000;46:768–773. doi: 10.1136/gut.46.6.768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ghoos YF, Maes BD, Geypens BJ, et al. Measurement of gastric emptying rate of solids by means of a carbon-labeled octanoic acid breath test. Gastroenterology. 1993;104:1640–1647. doi: 10.1016/0016-5085(93)90640-x. [DOI] [PubMed] [Google Scholar]
- 38.Medhus AW, Lofthus CM, Bredesen J, Husebye E. Gastric emptying:the validity of the paracetamol absorption test adjusted for individual pharmacokinetics. Neurogastroenterol Motil. 2001;13:179–185. doi: 10.1046/j.1365-2982.2001.00249.x. [DOI] [PubMed] [Google Scholar]
- 39.Simonian HP, Maurer AH, Knight LC, et al. Simultaneous assessment of gastric accommodation and emptying:studies with liquid and solid meals. J Nucl Med. 2004;45:1155–1160. [PubMed] [Google Scholar]
- 40.Holt S, Cervantes J, Wilkinson AA, Wallace JH. Measurement of gastric emptying rate in humans by real-time ultrasound. Gastroenterology. 1986;90:918–923. doi: 10.1016/0016-5085(86)90868-1. [DOI] [PubMed] [Google Scholar]
- 41.Irvine EJ, Tougas G, Lappalainen R, Bathurst NC. Reliability and interobserver variability of ultrasonographic measurement of gastric emptying rate. Dig Dis Sci. 1993;38:803–810. doi: 10.1007/BF01295904. [DOI] [PubMed] [Google Scholar]
- 42.Moreira TV, McQuiggan M. Methods for the assessment of gastric emptying in critically ill, enterally fed adults. Nutr Clin Pract. 2009;24:261–273. doi: 10.1177/0884533609332176. [DOI] [PubMed] [Google Scholar]
- 43.Couturier O, Bodet-Milin C, Querellou S, Carlier T, Turzo A, Bizais Y. Gastric scintigraphy with a liquid-solid radiolabelled meal:performances of solid and liquid parameters. Nucl Med Commun. 2004;25:1143–1150. doi: 10.1097/00006231-200411000-00013. [DOI] [PubMed] [Google Scholar]
- 44.Schwizer W, Fraser R, Borovicka J, Crelier G, Boesiger P, Fried M. Measurement of gastric emptying and gastric motility by magnetic resonance imaging (MRI) Dig Dis Sci. 1994;39:101S–103S. doi: 10.1007/BF02300384. [DOI] [PubMed] [Google Scholar]
- 45.Choi MG, Kim Bwm, Choo KY, et al. Measurement of gastric accommodation and emptying of a solid meal by magnetic resonance imaging. Gastroenterology. 2000;118:A388–A389. [Google Scholar]
- 46.Faas HM, Rades T, Roche HL. Measurement of intragastric distribution of drugs by MRI in humans-a liposomal drugmodel. Gastroenterology. 1999;116:A991. [Google Scholar]
- 47.Parkman HP, Hasler WL, Barnett JL, Eaker EY American Motility Society Clinical GI Motility Testing Task Force. Electrogastrography:a document prepared by the gastric section of the American Motility Society Clinical GI Motility Testing Task Force. Neurogastroenterol Motil. 2003;15:89–102. doi: 10.1046/j.1365-2982.2003.00396.x. [DOI] [PubMed] [Google Scholar]
- 48.Dive A, Moulart M, Jonard P, Jamart J, Mahieu P. Gastroduodenal motility in mechanically ventilated critically ill patients:a manometric study. Crit Care Med. 1994;22:441–447. doi: 10.1097/00003246-199403000-00014. [DOI] [PubMed] [Google Scholar]
- 49.Holte K, Sharrock NE, Kehlet H. Pathophysiology and clinical implications of perioperative fluid excess. Br J Anaesth. 2002;89:622–632. doi: 10.1093/bja/aef220. [DOI] [PubMed] [Google Scholar]
- 50.Schwartz MP, Samsom M, Renooij W, et al. Small bowel motility affects glucose absorption in a healthy man. Diabetes Care. 2002;25:1857–1861. doi: 10.2337/diacare.25.10.1857. [DOI] [PubMed] [Google Scholar]
- 51.Greiff JM, Rowbotham D. Pharmacokinetic drug interactions with gastrointestinal motility modifying agents. Clin Pharmacokinet. 1994;27:447–461. doi: 10.2165/00003088-199427060-00004. [DOI] [PubMed] [Google Scholar]
- 52.Sachdev AH, Pimentel M. Gastrointestinal bacterial overgrowth:pathogenesis and clinical significance. Ther Adv Chronic Dis. 2013;4:223–231. doi: 10.1177/2040622313496126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Bond JH, Jr, Levitt MD, Prentiss R. Investigation of small bowel transit time in man utilizing pulmonary hydrogen (H2) measurements. J Lab Clin Med. 1975;85:546–555. [PubMed] [Google Scholar]
- 54.Sciarretta G, Furno A, Mazzoni M, Garagnani B, Malaguti P. Lactulose hydrogen breath test in orocecal transit assessment. Critical evaluation by means of scintigraphic method. Dig Dis Sci. 1994;39:1505–1510. doi: 10.1007/BF02088056. [DOI] [PubMed] [Google Scholar]
- 55.Caride VJ, Prokop EK, Troncale FJ, Buddoura W, Winchenbach K, McCallum RW. Scintigraphic determination of small intestinal transit time:comparison with the hydrogen breath technique. Gastroenterology. 1984;86:714–720. [PubMed] [Google Scholar]
- 56.Madsen JL, Larsen NE, Hilsted J, Worning H. Scintigraphic determination of gastrointestinal transit times. A comparison with breath hydrogen and radiologic methods. Scand J Gastroenterol. 1991;26:1263–1271. doi: 10.3109/00365529108998623. [DOI] [PubMed] [Google Scholar]
- 57.Miller MA, Parkman HP, Urbain JL, et al. Comparison of scintigraphy and lactulose breath hydrogen test for assessment of orocecal transit:lactulose accelerates small bowel transit. Dig Dis Sci. 1997;42:10–18. doi: 10.1023/a:1018864400566. [DOI] [PubMed] [Google Scholar]
- 58.Rauch S, Krueger K, Turan A, You J, Roewer N, Sessler DI. Use of wireless motility capsule to determine gastric emptying and small intestinal transit times in critically ill trauma patients. J Crit Care. 2012;27(534):e7–e12. doi: 10.1016/j.jcrc.2011.12.002. [DOI] [PubMed] [Google Scholar]
- 59.Rauch S, Krueger K, Turan A, Roewer N, Sessler DI. Determining small intestinal transit time and pathomorphology in critically ill patients using video capsule technology. Intensive Care Med. 2009;35:1054–1059. doi: 10.1007/s00134-009-1415-6. [DOI] [PubMed] [Google Scholar]
- 60.Lee YY, Erdogan A, Rao SS. How to assess regional and whole gut transit time with wireless motility capsule. J Neurogastroenterol Motil. 2014;20:265–270. doi: 10.5056/jnm.2014.20.2.265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Ogilvie H. Large-intestine colic due to sympathetic deprivation;a new clinical syndrome. Br Med J. 1948;2:671–673. doi: 10.1136/bmj.2.4579.671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Wells CI, O'Grady G, Bissett IP. Acute colonic pseudo-obstruction:A systematic review of aetiology and mechanisms. World J Gastroenterol. 2017;23:5634–5644. doi: 10.3748/wjg.v23.i30.5634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Delgado-Aros S, Camilleri M. Pseudo-obstruction in the critically ill. Best Pract. Res Clin Gastroenterol. 2003;17:427–444. doi: 10.1016/s1521-6918(03)00023-4. [DOI] [PubMed] [Google Scholar]
- 64.Chapman MJ, Nguyen NQ, Deane AM. Gastrointestinal dysmotility:clinical consequences and management of the critically ill patient. Gastroenterol Clin North Am. 2011;40:725–739. doi: 10.1016/j.gtc.2011.09.003. [DOI] [PubMed] [Google Scholar]
- 65.Ukleja A. Altered GI motility in critically Ill patients:current understanding of pathophysiology, clinical impact, and diagnostic approach. Nutr Clin Pract. 2010;25:16–25. doi: 10.1177/0884533609357568. [DOI] [PubMed] [Google Scholar]
- 66.Chan LN. A “gutsy move”:tackling enteral feeding intolerance in critically ill patients. Nutr Clin Pract. 2010;25:10–12. doi: 10.1177/0884533609357434. [DOI] [PubMed] [Google Scholar]
- 67.Itkin M, DeLegge MH, Fang JC, et al. Cardiovascular and Interventional Radiological Society of Europe. Multidisciplinary practical guidelines for gastrointestinal access for enteral nutrition and decompression from the Society of Interventional Radiology and American Gastroenterological Association (AGA) Institute, with endorsement by Canadian Interventional Radiological Association (CIRA) and Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Gastroenterology. 2011;141:742–765. doi: 10.1053/j.gastro.2011.06.001. [DOI] [PubMed] [Google Scholar]
- 68.Halkier BK, Ho CS, Yee AC. Percutaneous feeding gastrostomy with the Seldinger technique:review of 252 patients. Radiology. 1989;171:359–362. doi: 10.1148/radiology.171.2.2495560. [DOI] [PubMed] [Google Scholar]
- 69.Hull MA, Rawlings J, Murray FE, et al. Audit of outcome of long-term enteral nutrition by percutaneous endoscopic gastrostomy. Lancet. 1993;341:869–872. doi: 10.1016/0140-6736(93)93072-9. [DOI] [PubMed] [Google Scholar]
- 70.Grant MD, Rudberg MA, Brody JA. Gastrostomy placement and mortality among hospitalized Medicare beneficiaries. JAMA. 1998;279:1973–1976. doi: 10.1001/jama.279.24.1973. [DOI] [PubMed] [Google Scholar]
- 71.Dormann AJ, Huchzermeyer H. Endoscopic techniques for enteral nutrition:standards and innovations. Dig Dis. 2002;20:145–153. doi: 10.1159/000067486. [DOI] [PubMed] [Google Scholar]
- 72.Kwon RS, Banerjee S, Desilets D, et al. ASGE Technology Committee. Enteral nutrition access devices. Gastrointest Endosc. 2010;72:236–248. doi: 10.1016/j.gie.2010.02.008. [DOI] [PubMed] [Google Scholar]
- 73.Albibi R, McCallum RW. Metoclopramide:pharmacology and clinical application. Ann Intern Med. 1983;98:86–95. doi: 10.7326/0003-4819-98-1-86. [DOI] [PubMed] [Google Scholar]
- 74.Janssen P, Harris MS, Jones M, et al. The relation between symptom improvement and gastric emptying in the treatment of diabetic and idiopathic gastroparesis. Am J Gastroenterol. 2013;108:1382–1391. doi: 10.1038/ajg.2013.118. [DOI] [PubMed] [Google Scholar]
- 75.Fraser RJ, Bryant L. Current and future therapeutic prokinetic therapy to improve enteral feed intolerance in the ICU patient. Nutr Clin Pract. 2010;25:26–31. doi: 10.1177/0884533609357570. [DOI] [PubMed] [Google Scholar]
- 76.Hu B, Ye H, Sun C, et al. Metoclopramide or domperidone improves post-pyloric placement of spiral nasojejunal tubes in critically ill patients:a prospective, multicenter, open-label, randomized, controlled clinical trial. Crit Care. 2015;19:61. doi: 10.1186/s13054-015-0784-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Nguyen NQ, Chapman MJ, Fraser RJ, Bryant LK, Holloway RH. Erythromycin is more effective than metoclopramide in the treatment of feed intolerance in critical illness. Crit Care Med. 2007;35:483–489. doi: 10.1097/01.CCM.0000253410.36492.E9. [DOI] [PubMed] [Google Scholar]
- 78.Yavagal DR, Karnad DR, Oak JL. Metoclopramide for preventing pneumonia in critically ill patients receiving enteral tube feeding:a randomized controlled trial. Crit Care Med. 2000;28:1408–1411. doi: 10.1097/00003246-200005000-00025. [DOI] [PubMed] [Google Scholar]
- 79.Nassaji M, Ghorbani R, Frozeshfard M, Mesbahian F. Effect of metoclopramide on nosocomial pneumonia in patients with nasogastric feeding in the intensive care unit. East Mediterr Health J. 2010;16:371–374. [PubMed] [Google Scholar]
- 80.Annese V, Lombardi G, Frusciante V, Germani U, Andriulli A, Bassotti G. Cisapride and erythromycin prokinetic effects in gastroparesis due to type 1 (insulin-dependent) diabetes mellitus. Aliment Pharmacol Ther. 1997;11:599–603. doi: 10.1046/j.1365-2036.1997.00177.x. [DOI] [PubMed] [Google Scholar]
- 81.Dive A, Miesse C, Galanti L, et al. Effect of erythromycin on gastric motility in mechanically ventilated critically ill patients:a double-blind, randomized, placebo-controlled study. Crit Care Med. 1995;23:1356–1362. doi: 10.1097/00003246-199508000-00008. [DOI] [PubMed] [Google Scholar]
- 82.Chapman MJ, Fraser RJ, Kluger MT, Buist MD, De Nichilo DJ. Erythromycin improves gastric emptying in critically ill patients intolerant of nasogastric feeding. Crit Care Med. 2000;28:2334–2337. doi: 10.1097/00003246-200007000-00026. [DOI] [PubMed] [Google Scholar]
- 83.Reignier J, Bensaid S, Perrin-Gachadoat D, Burdin M, Boiteau R, Tenaillon A. Erythromycin and early enteral nutrition in mechanically ventilated patients. Crit Care Med. 2002;30:1237–1241. doi: 10.1097/00003246-200206000-00012. [DOI] [PubMed] [Google Scholar]
- 84.Berne JD, Norwood SH, McAuley CE, et al. Erythromycin reduces delayed gastric emptying in critically ill trauma patients:a randomized, controlled trial. J Trauma. 2002;53:422–425. doi: 10.1097/00005373-200209000-00004. [DOI] [PubMed] [Google Scholar]
- 85.Otterson MF, Sarna SK. Gastrointestinal motor effects of erythromycin. Am J Physiol. 1990;259:G355–G363. doi: 10.1152/ajpgi.1990.259.3.G355. [DOI] [PubMed] [Google Scholar]
- 86.Coulie B, Tack J, Peeters T, Janssens J. Involvement of two different pathways in the motor effects of erythromycin on the gastric antrum in humans. Gut. 1998;43:395–400. doi: 10.1136/gut.43.3.395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Feighner SD, Tan CP, McKee KK, et al. Receptor for motilin identified in the human gastrointestinal system. Science. 1999;284:2184–2188. doi: 10.1126/science.284.5423.2184. [DOI] [PubMed] [Google Scholar]
- 88.Tonini M, De Ponti F, Di Nucci A, Crema F. Review article:cardiac adverse effects of gastrointestinal prokinetics. Aliment Pharmacol Ther. 1999;13:1585–1591. doi: 10.1046/j.1365-2036.1999.00655.x. [DOI] [PubMed] [Google Scholar]
- 89.Lu HR, Vlaminckx E, Van Water, Rohrbacher J, Hermans A, Gallacher DJ. In-vitro experimental models for the risk assessment of antibiotic-induced QT prolongation. Eur J Pharmacol. 2007;577:222–232. doi: 10.1016/j.ejphar.2007.07.070. [DOI] [PubMed] [Google Scholar]
- 90.Roden DM. Drug-induced prolongation of the QT interval. N Engl J Med. 2004;350:1013–1022. doi: 10.1056/NEJMra032426. [DOI] [PubMed] [Google Scholar]
- 91.Ng E, Shah VS. Erythromycin for the prevention and treatment of feeding intolerance in preterm infants. Cochrane Database Syst Rev. 2008;3:CD001815. doi: 10.1002/14651858.CD001815.pub2. [DOI] [PubMed] [Google Scholar]
- 92.Mangoni AA, Close JC, Rodriguez S, et al. Acute hypotensive effects of oral cisapride and erythromycin in healthy subjects. Br J Clin Pharmacol. 2004;58:223–224. doi: 10.1111/j.1365-2125.2004.02118.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Ringel AF, Jameson GL, Foster ES. Diarrhea in the intensive care patient. Crit Care Clin. 1995;11:465–477. [PubMed] [Google Scholar]
- 94.Absher JR, Bale JF., Jr Aggravation of myasthenia gravis by erythromycin. J Pediatr. 1991;119:155–156. doi: 10.1016/s0022-3476(05)81058-3. [DOI] [PubMed] [Google Scholar]
- 95.Hawkyard CV, Koerner RJ. The use of erythromycin as a gastrointestinal prokinetic agent in adult critical care:benefits versus risks. J Antimicrob Chemother. 2007;59:347–358. doi: 10.1093/jac/dkl537. [DOI] [PubMed] [Google Scholar]
- 96.Hersch M, Krasilnikov V, Helviz Y, Zevin S, Reissman P, Einav S. Prokinetic drugs for gastric emptying in critically ill ventilated patients:analysis through breath-testing. J Crit Care. 2015;30(655):e7–e13. doi: 10.1016/j.jcrc.2014.12.019. [DOI] [PubMed] [Google Scholar]