

Abstract
Rilpivirine is associated with a good efficacy and safety profile. However, data from real-life settings are scarce.
Methods
We investigated the durability, safety and efficacy of Rilpivirine-based antiretroviral therapy in a prospective, observational, multicenter study.
Results
We enrolled 499 HIV-infected patients, 360 (72.1%) males, mean age 43.4 ± 10.5 years, mean CD4 600 ± 327 cell/μL, mean HIV-RNA 3.80 ± 1.15 log10 cp/mL. After a median follow up of 16 months, 81 (16.2%) interruptions were reported, 36 (7.2%) of which for adverse events (16 of grade ≥3), most commonly neurological and gastrointestinal. We observed virological failures in only 8 (1.6%) patients. Naive patients showed a significant reduction in eGFR at week 24, 48 and 72 and in total cholesterol (TC)/HDL ratio at week 48 (p=0.007). In patients switching from PI we found a significant decrease at week 24 and 48 in TC and triglycerides at week 24, 48 and 72. eGFR showed a significant decrease at week 48 and 72. TC/HDL ratio showed a statistically significant decrease at week 24 (p=0.0008) and 72 (p=0.04). A significant increase at week 24 and 48 in AST and ALT values was observed. Patients switching from TDF/FTC/EFV showed a reduction in HDL, total cholesterol and triglycerides at week 24 and 48 and in eGFR at all follow up times. TC/HDL ratio showed a significant decrease at week 48 (p=0.01). CDC stage C and antiretroviral-experience (especially Protease Inhibitors) were associated with RPV discontinuation.
Conclusion
In conclusion, our data confirm Rilpivirine efficacy, safety and tolerability with improvement in lipid profile. Although hepatic and renal events rarely caused discontinuation, liver and kidney parameters should be monitored.
Keywords: HIV-1, combination antiretroviral therapy, NNRTI, cohort study, naive, experienced patients
Introduction
Rilpivirine (RPV) is a non-nucleoside reverse-transcriptase inhibitor (NNRTI) indicated at first in naive patients with an HIV-RNA of <100,000 copies/mL and CD4 count >200 cells/mm3. Since 2013, it has also been used for treatment-experienced patients with virological suppression and without NNRTI-resistance mutations. RPV is available as a single drug (RPV, 25 mg tablet) or co-formulated with tenofovir and emtricitabine (TDF/FTC/RPV, 245/200/25 mg tablet) or with tenofovir alafenamide and emtricitabine (TAF/FTC/RPV, 25/200/25 mg tablet) in a single tablet regimen.1,2 In the current European AIDS Clinical Society guidelines, RPV remains a recommended regimen for antiretroviral-naive HIV-infected patients with an HIV-RNA of <100,000 copies/mL and CD4 count >200 cells/mm3.3 Furthermore, in the latest Department of Health and Human Services guidelines, RPV is recommended as initial regimen in certain clinical situations, underlining that a RPV-based regimen is effective and tolerable, but has some disadvantages when compared with integrase inhibitor-based regimens, which are actually the recommended initial regimens for most people with HIV.4
RPV is a substrate of hepatic cytochrome P450 3A4, and therefore, drugs that induce or inhibit the action of this isoenzyme may alter serum RPV levels. Rifamycins, anticonvulsivants, and St. John’s wort may decrease RPV concentrations and should be avoided.1,2 Macrolides, azole, and protease inhibitors (PIs) may increase RPV levels. Some pharmacodynamics interactions exist: since an acidic gastric environment is necessary for absorption, proton pump inhibitors should not be given to patients taking RPV.1,2 To guarantee sufficient absorption, RPV should be taken with food (a meal of at least 500 kcal is required).5
As with other NNRTIs, drug interactions and a low resistance barrier have to be considered.
Data from clinical studies have suggested that TDF/FTC/RPV is associated with a good safety profile, especially with regard to lipid metabolism. An improvement of lipid parameters was observed with RPV compared with efavirenz (EFV) or PI, with a decrease in total and low-density lipoprotein cholesterol (LDL) and triglycerides.6–8
Headache, insomnia, and central nervous system (CNS) symptoms (depressive and suicidal disorders) occur less frequently than with EFV.6,7 A mild rash can occur in the first week and treatment is usually continued. Few data are available on efficacy and safety of RPV-based treatment in clinical practice from observational cohorts.
Our aim is to describe the durability, safety, and efficacy of a combination antiretroviral therapy (cART) regimen including RPV in real life. Specifically, we evaluated the modification of estimated glomerular filtration rate (eGFR) and liver and lipid profile in naive and experienced patients, most of whom switched to RPV from a PI or a TDF/FTC/EFV-based regimen.
Methods
The SCOLTA Project is a prospective, observational, multi-center study created to assess the incidence of adverse events (AEs) in patients receiving new antiretroviral drugs in clinical practice. It is an online pharmacovigilance program involving 22 Italian Infectious Disease Departments. The approving coordinating center is ASST Fatebenefratelli Sacco-Milano, Italy.
The Project has an Internet site (http://www.cisai.info) where grade 3 and 4 AEs are recorded (http://rcc.tech-resintl.com/tox_tables.htm). The SCOLTA Project currently includes 3 cohorts: RPV, elvitegravir/cobicistat/TDF/FTC, and dolutegravir. Patients who start taking a cohort drug are consecutively enrolled in that cohort and asked to give written informed consent. To date, no one has refused. As this is an observational study, the choice of therapy is entirely up to the individual physicians and patients in each center. Patients are followed up according to the standards of each center. The study has been approved by the ethics committee of the coordinating and the participating centers. At baseline, clinical characteristics, laboratory variables, cART history, and comorbidities are recorded. Data regarding enrolled patients are registered at 6-month intervals, and AEs, therapy interruptions, and their causes are notified when they are clinically observed. AEs are described according to the Division of AIDS table.9 Complete data collection and follow-up procedures for the cohorts are described elsewhere.10,11 Virological failure (VF) or discontinuation was defined by the clinicians according to current guidelines.3,4 eGFR was calculated using the Modification of Diet in Renal Diseases formula.
Statistical analysis
Data were described using mean (± SD) for normally distributed continuous variables, median (interquartile range, IQR) for not normally distributed continuous variables, and frequency (%) for categorical and ordinal variables. At univariate analyses, differences between groups (naive and experienced) were evaluated by means of analysis of variance, Mann–Whitney U-test, chi-square test, and Cochrane–Mantel–Hanszel test. Changes from baseline were analyzed using Student’s t-test for paired data.
Treatment interruption was evaluated using the Kaplan–Meier curve; variables were compared using the log-rank test. To simultaneously account for several potential confounders, we determined the hazard ratio (HR) and corresponding 95% CI of discontinued RPV by the Cox proportional hazards models, including variables associated at univariate analysis in the model.
Ethical approval
The SCOLTA Project has been approved by the ethical committees of the coordinating and the participating centers. All patients enrolled in the study gave written informed consent.
Results
Enrolment started in January 2013 and is ongoing. A total of 499 HIV-infected patients were included in the study, 360 (72.1%) of whom were males and 456 (91.4%) were Caucasian. In 390 (78.2%) patients, the risk factor for HIV acquisition was sexual intercourse. Mean age at enrolment was 43.4±10.5 years. Centers for Disease Control and Prevention (CDC) stage was A in 310 (62.1%) patients, mean CD4+ cell count was 600±327 cell/μL, and mean HIV-RNA when detectable was 3.80±1.15 log10 cp/mL; 138 (27.7%) were naive and 361 (72.3%) were experienced. Median duration of previous regimens in experienced patients was 6.4 years (IQR: 2.9–13.1 years). Ten (2.0%) subjects started therapy with viral load (VL) >100,000 copies/mL, 5 of whom were naive and 5 experienced (1.4% vs 3.6%, p=0.11). Ninety-seven (19.5%) patients were hepatitis C virus antibody (HCV-Ab) positive: 12 (8.8%) were naive and 85 (23.6%) were treatment experienced. The most common treatment was TDF/FTC/RPV in 455 patients (91.2%) followed by abacavir/lamivudine + RPV in 21 patients (4.2%). Demographic and clinical characteristics of patients are summarized in Table 1. As expected, naive and cART-experienced patients were significantly different with regard to age, HIV transmission category, CDC stage, and CD4+ count, as well as HCV coinfection, blood lipids, including total cholesterol/high-density lipoprotein cholesterol (TC/HDL) ratio, transaminase levels, and eGFR.
Table 1.
Comparison of naive and experienced patients starting a rilpivirine-based combination antiretroviral therapy
| Naive (N=138, 27.7%)
|
Experienced (N=361, 72.3%)
|
p-value | |||
|---|---|---|---|---|---|
| N or mean or median | % or SD or IQR | N or mean or median | % or SD or IQR | ||
| TDF/FTC/RPV N (%) | 134 | 97.1 | 321 | 88.9 | |
| RPV/other N (%) | 4 | 2.9 | 40 | 11.1 | 0.004 |
| Gender N (%) | |||||
| Female | 35 | 25.4 | 104 | 28.8 | |
| Male | 103 | 74.6 | 257 | 71.2 | 0.44 |
| Age (years) | 38.1 | 10.3 | 45.5 | 9.9 | <0.0001 |
| Ethnicity N (%) | |||||
| Caucasian | 125 | 90.6 | 331 | 91.7 | |
| Other | 13 | 9.4 | 30 | 8.3 | 0.69 |
| HIV transmission category N (%) | |||||
| IVDU | 8 | 5.8 | 71 | 19.7 | |
| Homo/heterosexual | 124 | 89.9 | 266 | 73.7 | |
| Other or unknown | 6 | 4.3 | 24 | 6.6 | 0.0003 |
| CDC stage (1 missing) N (%) | |||||
| A | 107 | 77.5 | 203 | 56.2 | |
| B | 25 | 18.1 | 88 | 24.4 | |
| C | 6 | 4.4 | 70 | 19.4 | <0.0001 |
| CD4 count (cells/μL) N (%) | |||||
| <200 | 9 | 6.5 | 18 | 5.0 | |
| 200–349 | 46 | 33.3 | 37 | 10.2 | |
| ≥350 | 83 | 60.2 | 306 | 84.8 | <0.0001 |
| Undetectable HIV viral load N (%) | − | − | 70 | 19.4 | − |
| Lipodystrophy N (%) | 5 | 3.6 | 55 | 15.2 | 0.0004 |
| HCV antibody positive (2 missing) N (%) | 12 | 8.8 | 85 | 23.6 | 0.0002 |
| HCV-RNA positive (n=87) N (%) | 2 | 18.2 | 49 | 64.5 | 0.006 |
| Previous treatment including N (%): | |||||
| PI | − | − | 162 | 44.9 | |
| TDF/FTC/EFV | − | − | 135 | 37.4 | − |
| Other drugs | − | − | 64 | 17.7 | |
| Total cholesterol (md/dL)* | 165.0 | 35.4 | 188.4 | 42.1 | <0.0001 |
| HDL-C (md/dL)* | 40.8 | 13.2 | 48.5 | 16.7 | <0.0001 |
| Triglycerides (md/dL)** | 98.5 | 68.5–133.5 | 120 | 85–168 | <0.0001 |
| Blood glucose (md/dL)* | 87.8 | 20.4 | 91.6 | 21.2 | 0.07 |
| AST (U/L)** | 23 | 17–29 | 24 | 19–32 | 0.03 |
| ALT (mg/dL)** | 24 | 18–31 | 28 | 21–42 | 0.0001 |
| eGFR (mg/dL)** | 104 | 90–115 | 93 | 80–108 | <0.0001 |
Note: Data are expressed and mean ± standard deviation (SD)* or median and interquartile range (IQR)**.
Abbreviations: ALT, alanine transaminase; AST, aspartate transaminase; EFV, efavirenz; eGFR, estimated glomerular filtration rate; FTC, emtricitabine; HCV, hepatitis C virus; HDL-C, high-density lipoprotein cholesterol; IVDU, intravenous drug user; PI, protease inhibitor; RPV, rilpivirine; TDF, tenofovir.
The proportion of naive patients reaching virologic success (HIV-RNA load <50 cp/mL) was 88.7%, 89.8%, and 93.2% at week 24, 48, and 72, respectively, whereas the corresponding figures in treatment-experienced patients were 89.3%, 91.5%, and 96.2%, respectively. Patients switching from TDF/FTC/EFV maintained viral suppression at 93.7%, 96%, and 94.6% at week 24, 48, and 72, respectively, whereas in those switching from a PI, the percentages were 86.8%, 87.8%, and 97.7%, respectively.
After a median follow-up of 16 months (IQR: 9–21 months), 81 (16.2%) patients discontinued RPV treatment: 11 in the naive group and 70 in the experienced one.
Discontinuations of therapy occurred for the following reasons: 36 (7.2%) AEs, 17 (3.4%) lost to follow-up, 4 (0.8%) therapy simplification, 7 (1.4%) patient’s decision/low adherence, and 7 (1.4%) other motivations such as drug–drug interactions and pregnancy. Eight (1.6%) VFs occurred: 1 (0.7%) in a naive patient and 7 (1.9%) in experienced ones. Among them, 1 subject had initiated treatment with VL >100,000 copies/mL, 1 who switched from a PI had a VL=59 copies/mL at enrolment, and the remaining 5 had a suppressed VL (3 were previously on PI and 2 on TDF/FTC/EFV). Two patients were also co-infected with HCV.
Two (0.4%) experienced patients died, 1 from myocardial infarction and 1 from heart valve rupture. Among AE-related interruptions, 16 were ≥3 grade reactions. In particular, we registered 1 acute renal failure, 1 grade 4 ALT elevation, 1 hepatotoxicity, 4 gastrointestinal toxicity, 2 rashes, 3 arthralgia, and 1 tachypnea/asthenia. Five patients reported grade 3–4 symptoms related to CNS toxicity (insomnia, dizziness, depression, headache, and 1 unspecified) and a psychiatric event was also described. In 4 cases, interruption was due to more than 1 AE.
Among patients who interrupted RPV because of grade 1–2 AEs, we found 2 liver events (transaminase increase and unspecified hepatitis), 3 rashes, 3 gastrointestinal toxicities, 3 arthralgia, 1 asthenia, 3 CNS events (dizziness, psychomotor agitation, and 1 unspecified), 4 renal impairment, and 1 worsening lipoaccumulation.
The median time to AE-related treatment interruption was 7.5 (IQR: 2.0–14.5) in experienced and 12 (IQR: 4.5–18.5) months in naive patients. Dermatologic, gastrointestinal and, to a lesser extent, CNS AEs causing discontinuation occurred early (<6 months), whereas all renal AEs occurred after 12 months.
Reasons for interruption are shown in Table 2.
Table 2.
Comparison of treatment interruptions in naive and experienced patients receiving a rilpivirine-based cART
| Naive
|
Experienced
|
p-value | |||
|---|---|---|---|---|---|
| Number | % | Number | % | ||
| No | 127 | 92.0 | 291 | 80.6 | |
| Yes | 11 | 8.0 | 70 | 19.4 | 0.002 |
| Reason for interruption | |||||
| Death | 0 | 0 | 2 | 2.9 | |
| Virological failure | 1 | 9.1 | 7 | 10.0 | |
| Adverse events | 4 | 36.4 | 32 | 45.7 | |
| Grade 1–2 | 2 | 18 | |||
| Grade 3–4 | 2 | 14 | |||
| Lost at follow-up | 2 | 18.2 | 15 | 21.4 | |
| Other | 4 | 36.4 | 14 | 20.0 | 0.79 |
Abbreviation: cART, combination antiretroviral therapy.
At univariate analysis, subjects who withdrew from treatment were more frequently females than males (23.7% vs 13.3%, log-rank p=0.02), over 45 years old (20.1% vs 12.7%, log rank p=0.01), in stage C rather than A or B (25.0% vs 14.7%, log rank p=0.003), experienced (19.4% vs 8.0%, log rank p=0.0003), and among experienced patients more frequently switching from PI than from TDF/FTC/EFV (27.0% vs 15.4%, log rank p=0.02).
With the Cox model, including variables that were statistically significant at univariate analyses, we confirmed the role of being in CDC stage C (HR for treatment interruption 1.76, 95% CI: 1.04–2.98, reference category A+B) and experienced (HR: 2.47, 95% CI: 1.27–4.81, reference category naive). Limiting the analysis to experienced patients, a switch from PI (HR: 2.51, 95% CI: 1.17–5.38) but not from TDF/FTC/EFV, compared with other previous regimens (mainly NRTI based and Integrase Inhibitor based), represented a risk factor for RPV discontinuation. When we compared switching from PI with switching from TDF/FTC/EFV, we found that the risk was still higher (HR: 1.89, 95% CI: 1.08–3.30).
Follow-up evaluation
Treatment naive
Among naive patients with available follow-up data at week 24, 48, and 72, we found a significant reduction in eGFR at all follow-up times (−8.9±15.6 mL/min/1.73 m2, p<0.0001; −12.0±18.8 mL/min/1.73 m2, p<0.0001; and 9.1±17.3 mL/min/1.73 m2, p<0.0001, respectively) as shown in Figure 1. Regarding lipid profile, we did not observe significant changes in total cholesterol, HDL-cholesterol, and triglycerides during follow-up. TC/HDL ratio showed a decrease that reached a statistical significance at week 48 (−0.41; p=0.0007). Furthermore, blood glucose, aspartate alanine transaminase (ALT), and alanine transaminase (ALT)levels did not show significant modifications when compared with baseline values.
Figure 1.

Changes from baseline to 24, 48, and 72 weeks in eGFR (A), lipid profile (B–D), and AST and ALT (E, F) in patients switching to rilpivirine from previous treatment.
Abbreviations: ALT, alanine transaminase; AST, aspartate transaminase; EFV, efavirenz; eGFR, estimated glomerular filtration rate; FTC, emtricitabine; HDL, High-density lipoprotein; PI, protease inhibitor; TDF, tenofovir.
Treatment experienced
Our cohort also included 361 (72.3%) experienced patients: 162 (44.9%) switched from boosted PI-based regimen (43.8% atazanavir, 32.1% darunavir, 14.2% lopinavir, and 9.9% other PIs), 135 (37.4%) from a regimen based on TDF/FTC/EFV, and 64 (17.7%) switched from other regimens (13 integrase inhibitor-based regimens and 51 others). Changes in eGFR, lipid profile, blood glucose, AST, and ALT are shown in Figure 1.
The patients who switched from a PI-based regimen showed a slight but statistically significant decrease in TC (−15.0±35.6 mg/dL, p<0.0001 at 24 weeks; and −9.9±35.2 mg/dL at 48 weeks p=0.007) and triglycerides levels at week 24, 48, and 72 (−27±105 mg/dL, p=0.004; −34±86 mg/dL, p=0.0002; −49.9±89.5 mg/dL, p=0.0003, respectively), and a slight and nonsignificant (both from a statistical and clinical point of view) reduction change in HDL cholesterol (Figure 1). A significant reduction in eGFR was observed at week 48 (−4.4±18.3 mL/min/1.73 m2, p=0.02) and at week 72 (−7.3±17.3 mL/min/1.73 m2, p=0.004). TC/HDL ratio showed a decrease that was statistically significant at week 24 (−0.29; p=0.0008) and 72 (−0.35; p=0.04), whereas at week 48, it showed a trend toward significance (−0.20; p=0.05), as shown in Figure 2. On the contrary, we observed a slight but significant increase in AST (6 ± 15 IU/mL, p<0.0001 and 10±31 UI/mL, p=0.002) and ALT values (11±24 IU/mL, p<0.0001 and 15±66 IU/mL, p=0.02) at week 24 and 48, but not at week 72, as shown in Figure 1.
Figure 2.
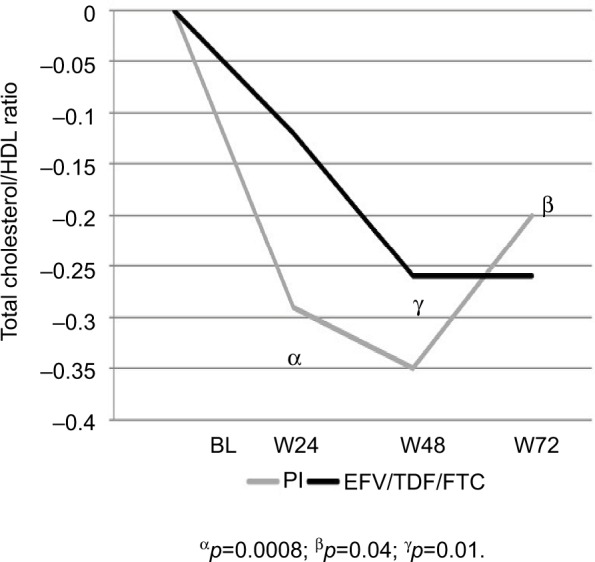
Changes in total cholesterol/HDL ratio from baseline to 24, 48, and 72 weeks.
Abbreviations: EFV, efavirenz; FTC, emtricitabine; HDL, high-density lipoprotein; PI, protease inhibitor; TDF, tenofovir.
The patients switching from a TDF/FTC/EFV regimen showed a statistically significant reduction in eGFR at all follow-up times (−7.5±16.1 mL/min/1.73 m2, p<0.0001, −8.0±19.7 mL/min/1.73 m2, p=0.0004 and −10.2±16.7 mL/min/1.73 m2, p=0.0004). A statistically significant reduction was observed at week 24 and 48 in total cholesterol (−16.7±27.5 mg/dL, p<0.0001, −23.5±30.3 mg/dL, p<0.0001) and triglycerides (−17±65 mg/dL, p=0.006, and −24±66 mg/dL, p=0.001). HDL-cholesterol showed a significant reduction at week 24 and 48 (−2.8±8.4 mg/dL, p=0.0004 and −3.2±9.1 mg/dL, p=0.002, respectively), but not at week 72. TC/HDL ratio showed a decrease at week 24 that became significant at week 48 (−0.26±0.88 mg/dL; p=0.01), as shown in Figure 2. AST and ALT levels did not vary markedly during the observation period (Figure 1).
Discussion
In this study, we described the efficacy, safety, and tolerability of a cART regimen, including RPV in 499 HIV-infected patients. In this real-life setting, after a median follow-up of 16 months, 81 (16.2%) patients had discontinued RPV treatment, mainly because of AEs, the interruptions of treatment with RPV occurs mainly in experienced patients rather than in naive subjects (8.9% vs 2.9%).
In the study period, we observed VF in 8 patients (1.6%), 1 of whom was naive (0.7%) and 7 (1.9%) were treatment experienced.
Available data on RPV efficacy are mostly derived from clinical trials in both naive and experienced patients.
In naive patients, RPV has been comparatively tested with EFV in 3 large trials. In 2 of these (ECHO and THRIVE), both Phase III, in 1368 patients, a comparable effect with better tolerability was observed at 48–96 weeks,6,7 and VF rates were 10% vs 6%, respectively, whereas in the sub-analysis by baseline VL (≤100,000 copies/mL), VF reached the same proportion in the 2 arms (5%).12 In the third trial (STaR), the 2 single-table regimens TDF/FTC/RPV and TDF/FTC/EFV were compared. This randomized, open-label trial included 786 patients and demonstrated non-inferior efficacy, including superiority in patients with HIV-RNA ≤100,000 cp/mL.12 In the overall study population, after 48 weeks, 86% of TDF/FTC/RPV vs 82% of TDF/FTC/EFV patients achieved undetectable VL and VF in the overall population and in the population with HIV-RNA <100000. In the overall population, VF rate was 8.1% for TDF/FTC/RPV vs 5.6% for TDF/FTC/EFV, whereas the corresponding figure in patients with HIV-RNA ≤100,000 copies/mL was 5% and 3.2%, respectively.13 The incidence of VF was higher for RPV, but was observed mostly in patients with baseline HIV-RNA>100,000 copies/mL. Improved tolerability was shown in patients receiving TDF/FTC/RPV compared with TDF/FTC/EFV.13
In this study, the proportion of naive patients reaching virologic success was similar to that observed in the randomized trials described above, thus confirming the efficacy of RPV in clinical practice.6,7,12,13
In an observational study, after a median of 2.6 months, VF occurred in 3 patients (1%) switched from a PI-based regimen.14
In the SPIRIT trial, 476 treatment-experienced patients with viral suppression were randomized to remain on their PI-based regimen or switch to RPV, and VF was observed in 2.5% of patients.8
In this study, the proportion of VF in patients with HIV≤100,000 copies/mL resulted lower than that of clinical trials and similar to that of other observational studies with shorter follow-up.
We observed a 7.2% rate of AE-related discontinuation that included 8 (1.6%) CNS events.
In the STaR trial, RPV was well tolerated, although CNS side effects occurred, but were less intense than those seen with EFV. Fewer AE-related discontinuations were observed (2.5% vs 8.7%, respectively), as well as fewer serious AEs (7.4% vs 13.8%), in the RPV than EFV arm.13 In the SPIRIT study, only 7 participants, out of 297 (2.4%) in the RPV arm, discontinued treatment because of AE, thus confirming that the switch was safe and better tolerated compared with continuing PI treatment.8
In the study by Gianotti et al,14 the most frequent causes of AE-related interruptions were gastrointestinal toxicity (6 cases, all of dyspepsia/epigastric pain), followed by a reduction in eGFR values (5 cases) and neurological toxicity (4 cases; headache in 2, dizziness in 1, and depressed mood in 1).
In an Italian multicenter study including 508 patients on a cART simplified to an single tablet regimen including RPV, in a median follow-up of 196 days, 31 (6.1%) patients discontinued the regimen. VF occurred in 8 (1.6%) patients.15
In this study, interruptions caused by AEs were higher than the above-mentioned clinical trials (7.2% vs 2.5% in the STaR and 2.4% in the SPIRIT trial),13,14,8 Different rates of interruptions were also shown in comparison with the previously reported observational studies, even though it should be noted that our patients were followed up for a significantly longer period.
With regard to durability, patients in CDC stage C and treatment experienced were independently associated with treatment interruptions in Cox model. Limiting the analysis to experienced patients, switching from PI, but not from TDF/FTC/EFV, comparing with other previous regimens represented a risk factor for RPV discontinuation. When we compared switching from PI to switching from TDF/FTC/EFV, we found that the risk was still higher.
Taken together, these results seem to suggest that patients in a more advanced stage and those with a longer treatment history are at higher risk of stopping RPV from any cause, and therefore, candidates should be carefully selected. Furthermore, patients switching from PI are at an even higher risk, probably due to a combination of patients’ characteristics, including more advanced disease.
We also further investigated the modification of eGFR and liver and lipid profile in naive and experienced patients during follow-up.
In the naive population, starting a regimen with RPV was not associated with a significant change in lipid profile, since we found an immediate decrease of total cholesterol that was not confirmed during follow-up and an elevation of triglycerides, even if not statistically significant. This study confirmed the minimal impact on fasting TC, HDL, and triglycerides in the naive population as previously seen in the literature.13
With experienced patients, we found that a switch to a RPV-based regimen was associated with an improvement in total cholesterol and triglycerides levels, regardless of whether the patients were switched from a PI- or NNRTI-based regimen.
A beneficial effect on lipid profile in experienced patients has already been reported in the SPIRIT trial,14 and in some observational studies, showing the decrease in TC, LDL, and triglycerides after switching from any regimen, although more marked when from boosted PI.8,14,15
To better clarify the clinical impact of the lipid modification related to RPV therapy in this study, we investigated the TC/HDL ratio, known as a strong predictor of coronary heart disease.16
Different from what seen in other observational study,14 we found the reduction of TC/HDL ratio statistically significant during the follow-up period at week 24 and 72 in patients switching from PI and at week 48 in both naive and those switching from TDF/FTC/EFV.
Modification of the cART regimen could be an important strategy to reduce cardiovascular risk, together with lifestyle modification, smoking cessation, and other interventions on modifiable risk factors. Our data show that, in a real-life scenario, RPV-based regimens, mostly co-formulated as TDF/FTC/RPV, are associated with a lipid-friendly profile. Of note, switching to RPV seems beneficial both in patients previously receiving PI or TDF/FTC/EFV and in naives and is associated with a significant reduction of TC/HDL ratio in a longer follow-up with respect to other previous studies. Taken together, these results suggest that RPV could contribute to reduced cardiovascular risk over time.
The observed reduction in eGFR was expected, since RPV has been known to cause the inhibition of the organic cation transporter, the active transporter of creatinine in the proximal renal tubule.17 It has been shown that it occurs in the first few weeks of treatment and does not usually worsen thereafter. However, changes in eGFR do not necessarily reflect changes in true GFR, as calculated by iohexol clearance.18,19 In our sample, this reduction was slight but statistically significant, both in patients starting first-line therapy with a RPV-based regimen and in cART-experienced ones in line with previous reports of clinical trials.8
The observational design of this study does not allow us to conclude that these changes were due to the introduction of TDF or RPV or both. However, the described change in eGFR did not seem to have effects on clinical management. In fact, in only 5 cases, the changes in eGFR were considered clinically relevant and led to treatment interruptions.
Regarding liver safety, we found a statistically significant increase in AST and ALT values, at all follow-up times in patients who switched from a PI-based regimen, whereas no significant changes were observed in those switching from TDF/FTC/EFV and in naives. Our data are, in part, similar to those described in the switch study by Gianotti et al14 in which a statistically significant increase of AST, but not of ALT, was found. The ALT increase, in our cases, could possibly be related to the higher HCV co-infection rate in our experienced patients (23.6% vs 15%) and also to the longer follow-up duration. Although we observed only 4 discontinuations due to hepatic toxicity, our results highlight the need for a monitoring of AST and ALT values during follow-up.
This study has some limitations that should be acknowledged. First, this is a cohort study in an observational setting, so confounding could not be completely ruled out. Second, the reasons for switching to a RPV-containing regimen or starting RPV in naive patients were not available. Third, the causes of discontinuation are those reported by the physician and therefore subjective by definition. Clinicians’ strategies may also slightly vary in different clinical centers.
Nevertheless, we believe that our results could provide clinicians with some useful information on the “real-world” experience with RPV-containing regimens.
In conclusion, the results of this study confirm the efficacy, safety, and tolerability in clinical practice of a regimen containing RPV for first-line therapy or for a switch in pretreated HIV-1-infected patients. In particular, we confirm the positive impact of a regimen including RPV on lipid profile as seen in clinical trials and observational studies. Although rare, hepatic events can occur, and this suggests a monitoring of liver toxicity during follow-up.
Acknowledgments
The authors thank all the patients and physicians who were involved in this study. The Coordinamento Italiano Studio Allergie e Infezione da HIV (C.I.S.A.I.) comprises the following members: Paolo Maggi, Chiara Bellacosa, Carmen Rita Santoro; Bologna: Leonardo Calza, Eleonora Magistrelli; Busto Arsizio: Tiziana Quirino, Barbara Menzaghi, Maddalena Farinazzo; Cagliari: Marzia Garau, Goffredo Angioni, Chiara Bolliri, Marta Motzo; Catania: Benedetto Maurizio Celesia, Maria Gussio, Mauro Maresca; Cesena: Carmela Grosso; Chieti: Jacopo Vecchiet, Katia Falasca, Claudio Ucciferri; Firenze (S.M. Annunziata): Francesca Vichi; Firenze (Careggi): Canio Martinelli, Elena Salomoni, Paola Corsi; Genova (Galliera): Giovanni Penco, Giovanni Cenderello, Alberto Venturini; Genova (S.Martino): Antonio Di Biagio, Lucia Taramasso, Laura Ambra Nicolini; Lecco: Paolo Bonfanti, Chiara Molteni; Messina: Giuseppe Nunnari, Giovanni Pellicanò; Milano (Sacco, I Divisione): Laura Carenzi, Simone Passerini, Carlo Magni; Milano (Sacco, II Divisione): Laura Valsecchi, Laura Cordier; Milano (Sacco, CMI): Stefano Rusconi, Valeria Colombo; Monza: Nicola Squillace, Valentina Ferroni, Valeria Pastore; Padova: Marzia Franzetti; Pavia: Roberto Gulminetti, Alberto Gatti Comini; Perugia: Giuseppe De Socio, Aria Patacca, Giorgia Angeli; Pescara: Giustino Parruti, Donatella Cibelli; Sanremo: Chiara Dentone; Sassari: Maria Stella Mura, Giordano Madeddu, Paola Bagella, Vito Fiore, Francesca Peruzzu; Torino: Giancarlo Orofino, Marta Guastavigna.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Edurant® (rilpivirine) tablets, EU summary of product characteristics [webpage on the Internet] Janssen-Cilag; Feb, 2013. [Accessed October 2, 2017]. Available from: http://www.medicines.org.uk/EMC/medicine/25490/SPC/Edurant+25+mg+tablets/#DOCREVISION. [Google Scholar]
- 2.EVIPLERA 200 mg/25 mg/245 mg film-coated tablets Summary of product characteristics [webpage on the Internet] Gilead Sciences. Feb, 2013. [Accessed October 2, 2017]. Available from: http://www.medicines.org.uk/emc/medicine/25518/SPC/
- 3.European AIDS Clinical Society 2017 Guidelines on the Use of Anti-retroviral Drugs for Treating and Preventing HIV Infection (Version 9.0) 2017 Oct; [Google Scholar]
- 4.Panel on Antiretroviral Guidelines for Adults and Adolescents Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents Department of Health and Human Services. [Accessed October 17, 2017]. Available from: http://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf.
- 5.Crauwels HM, van Heeswijk RP, Buelens A, Stevens M, Boven K, Hoetelmans RM. Impact of food and different meal types on the pharmacokinetics of rilpivirine. J Clin Pharmacol. 2013;53(8):834–840. doi: 10.1002/jcph.107. [DOI] [PubMed] [Google Scholar]
- 6.Cohen CJ, Molina JM, Cahn P, et al. THRIVE Study Group Efficacy and safety of rilpivirine (TMC278) versus efavirenz at 48 weeks in treatment-naive HIV-1-positive patients: pooled results from the phase 3 double-blind randomized ECHO and THRIVE Trials. J Acquir Immune Defic Syndr. 2012;60(1):33–42. doi: 10.1097/QAI.0b013e31824d006e. [DOI] [PubMed] [Google Scholar]
- 7.Molina JM, Cahn P, Grinsztejn B, et al. ECHO Study Group Rilpivirine versus efavirenz with tenofovir and emtricitabine in treatment-naive adults infected with HIV-1 (ECHO): a phase 3 randomised double-blind active-controlled trial. Lancet. 2011;378(9787):238–246. doi: 10.1016/S0140-6736(11)60936-7. [DOI] [PubMed] [Google Scholar]
- 8.Palella FJ, Jr, Fisher M, Tebas P, et al. Simplification to rilpivirine/emtricitabine/tenofovir disoproxil fumarate from ritonavir-boosted protease inhibitor antiretroviral therapy in a randomized trial of HIV-1 RNA-suppressed participants. AIDS. 2014;28(3):335–344. doi: 10.1097/QAD.0000000000000087. [DOI] [PubMed] [Google Scholar]
- 9.U.S. Department of Health and Human Services, National Institutes of Health, National Institute of Allergy and Infectious Diseases, Division of AIDS Division of AIDS (DAIDS) Table for Grading the Severity of Adult and Pediatric Adverse Events, version 2.0. Nov, 2014. [Accessed October 2, 2017]. Available from: http://rsc.techres.com/Document/safetyandpharma-covigilance/DAIDS_AE_GRADING_TABLE_v2_NOV2014.pdf.
- 10.Madeddu G, De Socio GV, Ricci EC, et al. I.S.A.I. Group, Italy Muscle symptoms and creatine phosphokinase elevations in patients receiving raltegravir in clinical practice: results from the SCOLTA project long-term surveillance. Int J Antimicrob Agents. 2015;45(3):289–294. doi: 10.1016/j.ijantimicag.2014.10.013. [DOI] [PubMed] [Google Scholar]
- 11.Bonfanti P, Martinelli C, Ricci E, et al. CISAI Group (Italian Coordinators for the Study of Allergies HIV Infection) An Italian approach to postmarketing monitoring: preliminary results from the SCOLTA (Surveillance Cohort Long-Term Toxicity Antiretrovirals) project on the safety of lopinavir/ritonavir. J Acquir Immune Defic Syndr. 2005;39(3):317–320. doi: 10.1097/01.qai.0000164248.56722.3c. [DOI] [PubMed] [Google Scholar]
- 12.Behrens G, Rijnders B, Nelson M, et al. Rilpivirine versus efavirenz with emtricitabine/tenofovir disoproxil fumarate in treatment-naïve HIV-1-infected patients with HIV-1 RNA ≤100,000 copies/mL: week 96 pooled ECHO/THRIVE subanalysis. AIDS Patient Care STDS. 2014;28(4):168–175. doi: 10.1089/apc.2013.0310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Cohen C, Wohl D, Arribas JR, et al. Week 48 results from a randomized clinical trial of rilpivirine/emtricitabine/tenofovir disoproxil fumarate vs. efavirenz/emtricitabine/tenofovir disoproxil fumarate in treatment-naive HIV-1-infected adults. AIDS. 2014;28(7):989–997. doi: 10.1097/QAD.0000000000000169. [DOI] [PubMed] [Google Scholar]
- 14.Gianotti N, Poli N, Nozza S, et al. Efficacy and safety in clinical practice of a rilpivirine, tenofovir and emtricitabine single-tablet regimen in virologically suppressed HIV-positive patients on stable antiretroviral therapy. J Int AIDS Soc. 2015;18(1):20037. doi: 10.7448/IAS.18.1.20037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Pinnetti C, Di Giambenedetto S, Maggiolo F, et al. Simplification to co-formulated rilpivirine/emtricitabine/tenofovir in virologically suppressed patients: data from a multicenter cohort. J Int AIDS Soc. 2014;17(4 Suppl 3):19812. doi: 10.7448/IAS.17.4.19812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Castelli WP, Abbott RD, McNamara PM. Summary estimates of cholesterol used to predict coronary heart disease. Circulation. 1983;67(4):730–734. doi: 10.1161/01.cir.67.4.730. [DOI] [PubMed] [Google Scholar]
- 17.Moss DM, Liptrott NJ, Curley P, Siccardi M, Back DJ, Owen A. Rilpivirine inhibits drug transporters ABCB1, SLC22A1, and SLC22A2 in vitro. Antimicrob Agents Chemother. 2013;57(11):5612–5618. doi: 10.1128/AAC.01421-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Maggi P, Montinaro V, Rusconi S, et al. The problem of renal function monitoring in patients treated with the novel antiretroviral drugs. HIV Clin Trials. 2014;15(3):87–91. doi: 10.1310/hct1503-87. [DOI] [PubMed] [Google Scholar]
- 19.Capetti A, Rizzardini G. Cobicistat: a new opportunity in the treatment of HIV disease? Expert Opin Pharmacother. 2014;15(9):1289–1298. doi: 10.1517/14656566.2014.920008. [DOI] [PubMed] [Google Scholar]