

Abstract
Previous research has shown that neighborhood-level variables such as social deprivation, social fragmentation or rurality are related to suicide risk, but most of these studies have been conducted in the U.S. or northern European countries. The aim of this study was to analyze the spatio-temporal distribution of suicide in a southern European city (Valencia, Spain), and determine whether this distribution was related to a set of neighborhood-level characteristics. We used suicide-related calls for service as an indicator of suicide cases (n = 6,537), and analyzed the relationship of the outcome variable with several neighborhood-level variables: economic status, education level, population density, residential instability, one-person households, immigrant concentration, and population aging. A Bayesian autoregressive model was used to study the spatio-temporal distribution at the census block group level for a 7-year period (2010–2016). Results showed that neighborhoods with lower levels of education and population density, and higher levels of residential instability, one-person households, and an aging population had higher levels of suicide-related calls for service. Immigrant concentration and economic status did not make a relevant contribution to the model. These results could help to develop better-targeted community-level suicide prevention strategies.
Introduction
Suicide is a major social and public health problem worldwide1. In 2012, there were over 800,000 suicide deaths around the world2. Europe is the WHO region with the highest rates of suicide worldwide, with 14.1 per 100,000 inhabitants, followed by the European Union, where the rates are around 11 per 100,0003. In Spain, where this study was conducted, and according to 2015 data, suicide was the first leading external cause of death, 1.9 times more than road traffic injuries, and 12.6 times more than homicides4. In the same year, 3,602 people died by suicide, which represents almost 10 suicides a day5. The problem is even greater if we take into account parasuicide (i.e., suicide attempts), which cannot be easily measured. Despite the social and economic costs of suicide in our societies, there is still a lack of prevention strategies that can adequately deal with this phenomenon6,7. Focusing on the range of variables that could explain suicidal behavior from different levels of analysis may help to design better-informed preventive actions.
Recently, a growing number of studies have suggested that neighborhood-level variables have an impact on suicide risk beyond individual-level factors8–11. Starting from the research of Congdon12, these studies point to the link between suicide risk and three sets of factors: social deprivation, social fragmentation, and rurality8,9,13,14. Neighborhood social deprivation, measured by different indicators such as poverty rate, unemployment, occupational social class, and education level, has been positively linked with suicide in a number of studies9,14–16. Neighborhood social fragmentation also has shown a positive relationship with suicide risk9,14. Indicators such as high levels of residential instability, high percentage of one-person households, and high divorce rates have been related to higher risks of suicide behavior, even after controlling for social deprivation10,17. Another stream of research studies has compared rural and urban areas in suicide risk, suggesting that the risk of suicide is higher in rural areas18,19. Research using population density as a proxy of rurality has also shown that areas with higher population density have lower risks of suicide9,20.
In addition to these variables, other neighborhood-level indicators have also been explored as predictors of suicide risk. For example, some research has focused on the relationship between ethnic density and suicide rates18,21,22. This relationship, however, is still inconclusive. Although some studies have found higher suicide rates in areas with high density of ethnic minorities21–23, other found no such significant relationship18.
Finally, although age has been positively linked to suicide risk at the individual level—i.e., higher suicide rates among older people6,8,24—the influence of this variable at the neighborhood-level has received less research attention. Some research suggests, however, that neighborhoods with higher levels of population aging (i.e., the ratio of elderly to young populations), tend to show higher suicide rates15.
Present Study
The aim of this study was to analyze the spatio-temporal distribution of suicide-related calls for service in a southern European city (Valencia, Spain), and whether this distribution was related to a set of neighborhood-level characteristics: economic status, education level, residential instability, one-person households, population density, immigrant concentration, and population aging. We used suicide-related calls for service as an indicator of suicidal behavior. This measure captures all calls for service received by the police related to suicide and parasuicide interventions, and has previously been considered as an indicator of suicidal behavior25.
A Bayesian spatio-temporal approach was used to deal with the methodological biases usually present in ecological studies such as overdispersion or spatial autocorrelation26,27. This methodological approach is common in public health analysis26–28 and is increasingly being used in the geographical study of suicide14,15,29–36.
Previous research has shown that high-resolution studies taking a small-area approach are more appropriate than other levels of aggregation with lower resolution (such as districts, counties or cities) for assessing spatial variations and neighborhood influences on suicide risk14,37. Similarly, they have shown the importance of taking into account a temporal approach when analyzing social problems in the neighborhood. More specifically, studies on suicide have shown the relevance of a temporal perspective, which could improve our knowledge of this outcome37. A previous study analyzed the baseline distribution of suicide-related calls comparing different spatial and spatio-temporal models and it showed that using a spatio-temporal approach improved the results obtained with a purely spatial model37. Research has also shown that yearly studies could mask the effect of seasonality found in suicide events1,37,38, and therefore using shorter temporal periods, such as seasons, is more appropriate37. Thus, we chose a spatio-temporal approach for this study.
This study therefore analyzes the influence of a set of neighborhood-level characteristics on the spatio-temporal distribution of suicide calls for service using census block groups (the smallest area available), and trimesters as the temporal unit in a Southern European city. To the best of our knowledge, this is the first study that has used a Bayesian spatio-temporal modeling approach to analyze neighborhood influences on the spatio-temporal distribution of suicide-related calls in a Southern European city.
Methods
Study area and time
Valencia is the third largest city in Spain, with a population of 790,201 inhabitants (2016 data)39. The census block group—the smallest administrative unit available—was used as the proxy for the neighborhood. The city of Valencia has 552 census block groups (population range 630–2,845).
The number of suicide-related calls for service was used as the outcome variable. Valencia Police Department provided data of all suicide-related calls requiring police intervention in the city of Valencia from 2010 to 2016. There were 6,537 calls in this period, of which 142 were related to suicide deaths, and 6,395 to suicide attempts. The address where the incident leading to a police intervention occurred was geocoded and located on the map of Valencia. Each year count was divided in 3-month periods to assess seasonality (period 1 = January to March, period 2 = April to June, period 3 = July to September, and period 4 = October to December). Thus, the outcome variable was divided into 28 periods.
Covariates
Several indicators were collected for each census block group. In line with previous studies, indicators of social deprivation, social fragmentation and population density were assessed9,14, as well as the variables population aging and immigrant concentration. Data was collected from the official records of the statistics office of Valencia City Hall corresponding to the year 2013. These indicators did not present significant differences across the years of the study, so the central year was selected.
Social deprivation indicators
Two variables were used as social deprivation indicators: economic status and education level. For economic status an index was constructed through an unrotated factor analysis using several highly correlated economic indicators, including cadastral value, percentage of high-end cars, percentage of financial businesses (number of businesses related to finances and insurances activities by the total of businesses), and percentage of commercial businesses (number of businesses related to commercial activities by the total of businesses). For the second variable, the average education level of neighborhood residents was measured on a 4-point scale, where 1 = less than primary education, 2 = primary education, 3 = secondary education, and 4 = college education.
Social fragmentation
We used two indicators to measure social fragmentation: residential instability and one-person households. The residential instability variable was calculated as the proportion of the population that had moved into or out of each census block group during the previous year (rate per 1,000 inhabitants). One-person households were measured as the number of households with only one person per total number of households.
Population density
Population density per square kilometer was used as a proxy of rurality.
Population aging index
An index of the population aging (i.e., the ratio of elderly to youth populations) was measured as the number of people aged 65 years or over per hundred people under the age of 15 years old.
Immigrant concentration
This was measured as the percentage of immigrant population in each census block group.
Seasonality
To explore the effect of seasonality, a dummy variable was introduced creating three binary variables that account for the first three trimesters; the fourth trimester was selected as the reference.
Table 1 shows the descriptive statistics for all the variables.
Table 1.
Variables (Mean, Standard Deviation, Minimum and Maximum Values) at the Census Block Group and Year Level (2013 data).
| Variable | Mean (SD) | Min | Max |
|---|---|---|---|
| Deprivation | |||
| Economic status | |||
| Property values (€) | 260.10 (74.61) | 111.50 | 590.70 |
| High-end cars (%) | 5.75 (3.62) | 1.30 | 24.80 |
| Commercial businesses (%) | 34.03 (9.21) | 7.50 | 66.40 |
| Financial businesses (%) | 18.15 (7.77) | 0 | 43.20 |
| Education level | 3.15 (0.33) | 2.39 | 3.86 |
| Population Density | 3,346 (1,736.94) | 107 | 13,112 |
| Fragmentation | |||
| Residential instability | 268.00 (87.98) | 91.10 | 649.80 |
| One-person households | 32.72 (6.58) | 15.46 | 54.78 |
| Aging index | 151.20 (60.00) | 16.20 | 501.10 |
| Immigrant concentration (%) | 13.28 (6.53) | 1.90 | 40.20 |
| Suicide-related calls | 0.26 (0.57) | 0 | 7 |
Abbreviations: SD, standard deviation; Min, minimum; Max, maximum.
Data analysis
A conditionally independent Poisson distribution was used to model the number of suicide-related calls for service. Specifically, the outcome in each census block group and each period was expressed as follows:
| 1 |
where is a fixed quantity representing the expected number of calls in census block group during period t in proportion to the population in Valencia in this census block group. is the log relative risk for every area and period.
Two different models were used. Both models included a spatio-temporal effect via the . We followed an autoregressive approach, which combines autoregressive time series and spatial modeling using a spatio-temporal structure where relative risks are both spatially and temporally dependent40. The log relative risk for the first period was defined as:
| 2 |
while the relative risks for the following periods were defined as:
| 3 |
where is the intercept, is the mean deviation of the risk in the period t, represents the temporal correlation between the spatial effects of each period, and and refer to structured and unstructured spatial random effects, respectively.
We incorporated a , which represents the mean deviation of the risk in trimester . The fourth trimester was selected as the reference, and the other three trimesters were compared to it.
The first model only accounted for this spatial-temporal effect and included seasonality as a covariate, while the second model incorporated different covariates to analyze the influence of neighborhood-level characteristics in the outcome. Seven covariates were introduced to this second model: economic status, education level, residential instability, one-person households, population density, population aging index, and immigrant concentration. The final model was as follows:
| 4 |
where is the vector of covariates, and is the vector of regression coefficients.
A Bayesian approach was followed for both models. Accordingly, appropriate prior distributions were assigned for the parameters, namely, vague Gaussian distributions for the fixed effects ; was specified as an improper uniform distribution; the autoregressive term was modeled as a uniform over the whole space ; and the structured effect was specified by a conditional spatial autoregressive (CAR) model41:
| 5 |
where represents the number of neighboring areas of each census block group , indicates the values of the vector except the component , is the standard deviation parameter, and is the units neighbors of census block group . The unstructured spatial effect was modeled by means of independent identically distributed Gaussian random variables . Finally, uniform distributions were used for the three hyperparameters , following the structure of the hierarchical Bayesian models.
In order to test the robustness, a sensitivity analysis was conducted using different prior distributions for the hyperparameters. The posterior distributions showed consistent results (see Supplementary Table S1).
To implement the models, simulation techniques based on Markov Chain Monte Carlo (MCMC) were used with the software R42 and the R2WinBUGS package. Three chains with 50,000 iterations were generated, and the first 10,000 were discarded as burn-in. The deviance information criterion (DIC) was used to compare models and select the best fit: the smaller the DIC, the better the fit43.
Results
The results of the two Bayesian autoregressive models are presented in Table 2.
Table 2.
Mean, standard deviation and 95% credible interval of the parameters of the autoregressive models.
| Model 1 (Autoregressive model without covariates) | Model 2 (Autoregressive model with covariates) | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | 95% CrI | Mean | SD | 95% CrI | |||
| Intercept | −0.362 | 0.045 | −0.450 | −0.275 | −0.136 | 0.528 | −1.265 | 0.767 |
| Economic status | −0.029 | 0.057 | −0.141 | 0.082 | ||||
| Education level | −0.269 | 0.160 | −0.645 | −0.021 | ||||
| Density | −0.015 | 0.002 | −0.018 | −0.012 | ||||
| Residential instability | 0.001 | 0.001 | 0.000 | 0.002 | ||||
| One-person households | 0.002 | 0.000 | 0.002 | 0.003 | ||||
| Aging | 0.002 | 0.000 | 0.001 | 0.002 | ||||
| Immigrant concentration | −0.007 | 0.008 | −0.024 | 0.009 | ||||
| Trimester 1 | −0.122 | 0.057 | −0.230 | −0.008 | −0.119 | 0.053 | −0.220 | −0.014 |
| Trimester 2 | 0.093 | 0.059 | −0.024 | 0.208 | 0.093 | 0.058 | −0.019 | 0.206 |
| Trimester 3 | 0.118 | 0.053 | 0.016 | 0.227 | 0.119 | 0.054 | 0.011 | 0.222 |
| 0.359 | 0.019 | 0.323 | 0.398 | 0.377 | 0.021 | 0.337 | 0.416 | |
| 0.160 | 0.030 | 0.102 | 0.220 | 0.144 | 0.080 | 0.011 | 0.256 | |
| 0.106 | 0.032 | 0.051 | 0.178 | 0.106 | 0.030 | 0.055 | 0.166 | |
| ρ | 0.903 | 0.009 | 0.885 | 0.919 | 0.881 | 0.011 | 0.859 | 0.900 |
| DIC | 24,577 | 24,546.7 | ||||||
Abbreviations: SD, standard deviation; CrI, credible interval; σθ, standard deviation spatially unstructured term; σϕ standard deviation structured term; σ∝, standard mean deviation of the risk; ρ temporal correlation.
Model 1 represents the autoregressive model without covariates, while Model 2 incorporates the effect of the covariates of the study. Note that Model 2 showed a relevant decrease in the DIC (30.3 units of decrease), and was therefore selected as the final model.
In this final model, indicators of social deprivation (education level), social fragmentation (residential instability and one-person households), and population density were associated with higher levels of suicide-related calls for service. Population aging was also relevant to the model. All these variables showed a posterior probability of being over or under zero higher than 95% (i.e., their 95% credible intervals did not include zero). Economic status and immigrant concentration, however, did not show a relevant relationship with the outcome, including zero in the 95% credible interval. These results indicate that areas with lower education level, lower levels of population density, higher residential instability and concentration of one-person households, and higher population aging have higher levels of suicide-related calls for service.
The seasonality effect was also relevant. Specifically, results show that the estimated number of suicide-related calls increases in the second and the third trimesters (i.e., from April and September), with a higher increase in the third trimester. In contrast, in the first trimester the estimated number of suicide-related calls is lower. The first and third trimesters had a 95% credible interval where zero was not included. For the second trimester, although its 95% credible interval includes zero, the posterior probability of being positive was 0.948, so we considered its effect relevant.
The Bayesian autoregressive model used allows us to analyze both spatial and temporal trends. Figure 1 shows the relative risk for a sample of the periods: the four trimesters of 2010, 2013 and 2016 (see Supplementary Fig. S1 for all maps). This figure reflects the differences between census block groups in each year, where areas with relative risks greater than 1 indicate an above-average probability. The general pattern shows that the highest risks are concentrated in some areas of the center, the north-west and the east of the city. These risks are higher in the second and the third trimester than in the first and the fourth.
Figure 1.

Relative risk for the four trimesters of 2010, 2013 and 2016 (maps created by the software R version 3.4.3., available in https://www.R-project.org).
Regarding the temporal pattern, the parameter had a value of 0.88, indicating a high temporal correlation between a particular trimester and its predecessor. Figure 2 shows the temporal effect for each trimester. Despite the increasing trend over the years (there is no evidence of stabilization), this increase was not constant, but we found some clear peaks within the year as a result of the seasonality effect. Therefore, it is important to take into account seasonality to better capture the temporal trend of suicide-related calls for service.
Figure 2.
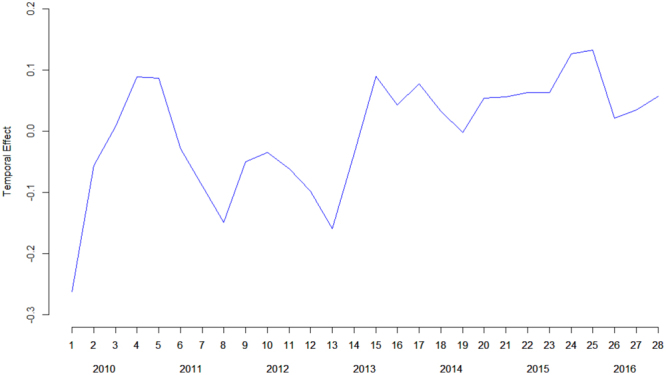
Temporal effect during the period (2010–2016).
Discussion
This study explored the influence of neighborhood-level characteristics on the spatio-temporal distribution of suicide-related calls for service in Valencia, Spain. An autoregressive model following a Bayesian approach was conducted to assess both spatial and temporal effects. Although previous studies have shown the relationship between ecological variables and the risk of suicide11,14,30,33, to the best of our knowledge there are no studies assessing the geography of suicide in South European countries using a small area approach44.
Our results showed that neighborhoods with lower levels of education and population density, and higher levels of residential instability, higher concentration of one-person households, and higher population aging had higher levels of suicide-related calls for service. These results are in line with previous research suggesting that social deprivation, social fragmentation, and low population density are closely related to suicide risk at the community level8–11,13,15,45.
Economic status and immigrant population did not make a relevant contribution to the model. Previous studies have found a negative relationship between economic status and suicide-related outcomes9,10,14,30. The use of different measures of economic status may explain these differences, as these studies usually included variables such as income and unemployment, which were not available for the present study. In our case, education level was the deprivation variable with the greatest contribution to the model.
Regarding the results for immigrant concentration, it is important to take into account differences Spain has from other countries. Previous studies were mostly conducted in English-speaking and northern European countries, and usually focused on ethnic differences or indigenous people, where they found a positive association between suicide rates and percentage of ethnic minorities9,21,23,46. However, some cultural factors may influence the relationship between immigration and suicide rates. In Valencia, the largest immigrant group is from Latin American countries (34%). A shared dominant language in Spain and Latin America could facilitate social integration in the community more than in English speaking countries, and may be a protective factor against suicidal behavior. Future research would benefit from cross-cultural studies to analyze the differences among countries in the relationship between suicide and immigration rates.
Furthermore, we found a seasonality effect, with a peak of calls in the second (April to June) and third (July to September) trimesters, and a decrease in the other two. These results are similar to previous research suggesting that suicide rates increase in spring and summer24,38,47,48. These results indicate the importance of taking seasonality into account when conducting a temporal analysis of suicide trends. Our results also showed an important increase in the number of suicide-related calls for service from 2010. The results suggest that suicide-related calls for service increased over the study period (2010–2016), and that there was no stabilization by the end of 2016. Future studies would benefit from incorporating long-term data, including the following years, to further analyze the evolution of suicide trends.
This study has both strengths and limitations. Its strengths include its location in a southern European city, as noted above, where there is a lack of studies on suicide at the neighborhood level37. Our results suggest that, despite the differences between countries, some neighborhood-level characteristics associated with suicide in the U.S. and northern European cities can also explain suicide variations in a southern European city. This paper, thus, provides new evidence about the spatio-temporal distribution of suicide calls in southern European cities and the neighborhood-level characteristics that may be related to this distribution. However, it is important to be cautious as this study was conducted in one specific city. Future research would benefit from conducting studies with a similar approach in other South-Europe cities.
This study used census block groups, which is more appropriate for addressing biases associated to aggregate data49. Moreover, we used an autoregressive model following a Bayesian approach. The Bayesian autoregressive model has been found to perform better than other spatio-temporal models, and some studies have showed that it provides a slightly better fit in terms of DIC50. The Bayesian approach also has some advantages over the frequentist perspective. Bayesian models let researchers incorporate prior information, and also address issues such as overdispersion and spatial autocorrelation26,27,31. The Bayesian approach is increasingly being used to analyze social outcomes such as crime or violence49,51–58, and also to study suicide31,32,37.
Among the limitations, as we noted before, some commonly used variables such as income levels or unemployment were not available at the census block group level. Individual characteristics (such as the person’s gender or age) were also unavailable. Future research would benefit from analyzing the possible different spatial patterns according to the sex or the age of the person making the suicide-related call for service in Valencia. Furthermore, this study is based on calls for service, and other commonly used measures of suicidal behavior (such as hospitalizations or medical records) were not analyzed. In addition, although our results suggest an increase in suicide-related calls for service, the study period was limited and does not allow us to draw strong conclusions. Clearly, future studies need to incorporate longer periods of time in order to further analyze the temporal trend of suicide-related calls for service. Finally, despite the autoregressive model having a better performance than other models, it requires a high computation time due to the complexity of the model and the considerable time periods covered by this study37,50.
In conclusion, this study illustrates the relevance of a number of ecological variables in explaining suicide-related calls for service. Addressing these neighborhood risk factors and focusing on the high-risk areas with a higher increase in suicide-related calls for service could help to develop better targeted community-level suicide prevention strategies.
Electronic supplementary material
Acknowledgements
This study was supported by the Spanish Ministry of Economy and Competitiveness (PSI2014-54561-P and MTM2016-77501-P). M.M. was supported by the FPU program of the Spanish Ministry of Education, Culture and Sports (FPU2013/00164). We wish to thank PROTECPOL (Cátedra de Protección Ciudadana y Policía Local de Valencia), and José Serrano, Chief of the Valencia City Police Department, for their support and assistance in collecting the data for this study.
Author Contributions
M.M. prepared data, carried out the statistical analysis and wrote the paper; E.G. conceived the study, supervised the analysis and wrote the paper; A.L-Q. designed the analysis, supervised the analysis and wrote the paper; and M.L. conceived the study and wrote the paper. All authors read and approved the final manuscript.
Competing Interests
The authors declare no competing interests.
Footnotes
Electronic supplementary material
Supplementary information accompanies this paper at 10.1038/s41598-018-25268-0.
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Hawton K, van Heeringen K. Suicide. Lancet. 2009;373:1372–1381. doi: 10.1016/S0140-6736(09)60372-X. [DOI] [PubMed] [Google Scholar]
- 2.World Health Organization. Monitoring health for the sustainable development goals (World Health Organization, 2016).
- 3.European Union. Causes of death - standardised death rate by residence (Eurostat, 2017).
- 4.Fundación Salud Mental España. Suicidios España 2015 (Fundación Salud Mental España, 2017).
- 5.Instituto Nacional de Estadística. INEbase, Defunciones según la causa de muerte 2015. http://www.ine.es/dynt3/inebase/index.htm?padre=1171 (2017).
- 6.Fundación Salud Mental España. Observatorio del suicidio en España (Fundación Salud Mental España, 2016).
- 7. World Health Organization. Preventing suicide. A global imperative (World Health Organization, 2014).
- 8.Burnley IH. Socioeconomic and spatial differentials in mortality and means of committing suicide in New South Wales, Australia, 1985–91. Soc. Sci. Med. 1995;41:687–698. doi: 10.1016/0277-9536(94)00378-7. [DOI] [PubMed] [Google Scholar]
- 9.Congdon P. The spatial pattern of suicide in the US in relation to deprivation, fragmentation and rurality. Urban Stud. 2011;48:2101–2122. doi: 10.1177/0042098010380961. [DOI] [PubMed] [Google Scholar]
- 10.Hawton K, et al. The influence of the economic and social environment on deliberate self-harm and suicide: an ecological and person-based study. Psychol. Med. 2001;31:827–836. doi: 10.1017/S0033291701003993. [DOI] [PubMed] [Google Scholar]
- 11.Rehkoff DH, Buka SL. The association between suicide and the socio-economic characteristics of geographical areas: A systematic review. Psychol. Med. 2006;36:145–157. doi: 10.1017/S003329170500588X. [DOI] [PubMed] [Google Scholar]
- 12.Congdon P. Suicide and parasuicide in London: A small-area study. Urban Stud. 1996;33:137–158. doi: 10.1080/00420989650012194. [DOI] [Google Scholar]
- 13.Johnson AM, Woodside JM, Johnson A, Pollack JM. Spatial patterns and neighborhood characteristics of overall suicide clusters in Florida from 2001 to 2010. Am. J. Prev. Med. 2016;52:e1–e7. doi: 10.1016/j.amepre.2016.07.032. [DOI] [PubMed] [Google Scholar]
- 14.Congdon P. Assessing the impact of socioeconomic variables on small area variations in suicide outcomes in England. Int.J. Environ. Res. Public Health. 2013;10:158–177. doi: 10.3390/ijerph10010158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Yoon TH, Han J, Jung-Choi K, Khang YH. Deprivation and sucide mortality across 424 neighborhoods in Seoul, South Korea: a Bayesian spatial analysis. Int. J. Public Health. 2015;60:969–976. doi: 10.1007/s00038-015-0694-7. [DOI] [PubMed] [Google Scholar]
- 16.Helbich M, Plener PL, Hartung S, Blüml V. Spatiotemporal suicide risk in Germany: A longitudinal study 2007–11. Sci. Rep. 2017;7:7673. doi: 10.1038/s41598-017-08117-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Evans J, Middleton N, Gunnell D. Social fragmentation, severe mental illness and suicide. Soc. Psyc. Psych. Epid. 2004;39:165–170. doi: 10.1007/s00127-004-0733-9. [DOI] [PubMed] [Google Scholar]
- 18.Knipe DW, et al. Regional variation in suicide rates in Sri Lanka between 1955 and 2011: A spatial and temporal analysis. BMC Public Health. 2017;17:193–206. doi: 10.1186/s12889-016-3961-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.McCarthy JF, et al. Suicide among patients in the veterans affairs health system: Rural-urban differences in rates, risks, and methods. Am. J. Public Health. 2012;102(Suppl 1):S111–S117. doi: 10.2105/AJPH.2011.300463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Stark C, et al. Population density and suicide in Scotland. Rural Remote Health. 2007;7:672–684. [PubMed] [Google Scholar]
- 21.Johansson LM, et al. The influence of ethnicity and social and demographic factors on Swedish suicide rates. A four year follow-up study. Soc. Psyc. Psyc. Epid. 1997;32:165–170. doi: 10.1007/BF00794616. [DOI] [PubMed] [Google Scholar]
- 22.Neeleman J, Wilson-Jones C, Wessely S. Ethnic density and deliberate self-harm: A small area study in southeast London. J. Epidemiol. Community Health. 2001;55:85–90. doi: 10.1136/jech.55.2.85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Neeleman J, Wessely S, Lewis G. Suicide acceptability in African and White Americans; the role of religion. J. Nerv. Ment. Dis. 1998;186:12–16. doi: 10.1097/00005053-199801000-00003. [DOI] [PubMed] [Google Scholar]
- 24.Santurtún, M., Santurtún, A. & Zarrabeitia, M. T. Does the environment affect suicide rates in Spain? A spatiotemporal analysis. Revista de Psiquiatría y Salud Mental In press (2017). [DOI] [PubMed]
- 25.Matheson FI, et al. Assessment of police calls for suicidal behavior in a concentrated urban setting. Psychiatr. Serv. 2005;56:1606–1609. doi: 10.1176/appi.ps.56.12.1606. [DOI] [PubMed] [Google Scholar]
- 26.Bernardinelli L, et al. Bayesian analysis of space-time variation in disease risk. Stat. Med. 1995;14:2433–2443. doi: 10.1002/sim.4780142112. [DOI] [PubMed] [Google Scholar]
- 27.Haining R, Law J, Griffith D. Modelling small area counts in the presence of overdispersion and spatial autocorrelation. Comput. Stat. Data An. 2009;53:2923–2937. doi: 10.1016/j.csda.2008.08.014. [DOI] [Google Scholar]
- 28.Waller, L. A. & Gotway, C. A. Applied spatial statistics for public health data (John Wiley and Sons, 2004).
- 29.Carcach C. A spatio-temporal analysis of suicide in El Salvador. BMC Public Health. 2017;17:339–349. doi: 10.1186/s12889-017-4251-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Chang SS, et al. Geography of suicide in Taiwan: Spatial patterning and socioeconomic correlates. Health Place. 2011;17:641–650. doi: 10.1016/j.healthplace.2011.01.003. [DOI] [PubMed] [Google Scholar]
- 31.Congdon P. Bayesian models for spatial incidence: a case study of suicide using the BUGS program. Health Place. 1997;3:229–247. doi: 10.1016/S1353-8292(97)00017-8. [DOI] [Google Scholar]
- 32.Congdon P. Monitoring suicide mortality: a Bayesian approach. Eur. J. Popul. 2000;16:251–284. doi: 10.1023/A:1026587810551. [DOI] [Google Scholar]
- 33.Hsu CY, Chang SS, Lee EST, Yip PSF. Geography of suicide in Hong Kong: Spatial patterning, and socioeconomic correlates and inequalities. Soc. Sci. Med. 2015;130:190–203. doi: 10.1016/j.socscimed.2015.02.019. [DOI] [PubMed] [Google Scholar]
- 34.Qi X, Mengersen K, Tong S. Socio-environmental drivers and suicide in Australia: Bayesian spatial analysis. BMC Public Health. 2014;4:681–690. doi: 10.1186/1471-2458-14-681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Rostami M, Jalilian A, Ghasemi S, Kamali A. Suicide mortality risk in Kermanshah Province, Iran: a county-level spatial analysis. Epidemiol. Biostat. Public Health. 2016;13:e11829-1–7. [Google Scholar]
- 36.Santana P, et al. Suicide in Portugal: Spatial determinants in a context of economic crisis. Health Place. 2015;35:85–94. doi: 10.1016/j.healthplace.2015.07.001. [DOI] [PubMed] [Google Scholar]
- 37.Marco M, et al. Spatio-temporal analysis of suicide-related emergency calls. Int. J. Environ. Res. Public Health. 2017;14:735–747. doi: 10.3390/ijerph14070735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Woo JM, Okusaga O, Postolache TT. Seasonality of suicidal behavior. Int. J. Environ. Res. Public Health. 2012;9:531–547. doi: 10.3390/ijerph9020531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Statistics Office. Padrón Municipal de Habitantes a 1 de Enero de 2016 (Statistics Office, Valencia Town Hall, 2017).
- 40.Martínez-Beneito MA, López-Quílez A, Botella-Rocamora P. An autoregressive approach to spatio-temporal disease mapping. Stat. Med. 2008;27:2874–2889. doi: 10.1002/sim.3103. [DOI] [PubMed] [Google Scholar]
- 41.Besag J, York J, Mollié A. Bayesian image restoration, with two applications in spatial statistics. Ann. Inst. Stat. Math. 1991;43:1–20. doi: 10.1007/BF00116466. [DOI] [Google Scholar]
- 42.R Core Team R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. www.R-project.org (2013).
- 43.Spiegelhalter DJ, Best NG, Carlin BP, Van Der Linde A. Bayesian measures of model complexity and fit. J. R. Stat. Soc. Ser. B. 2002;64:583–639. doi: 10.1111/1467-9868.00353. [DOI] [Google Scholar]
- 44.Álvaro-Meca A, Kneib T, Gil-Prieto R. & Gil de Miguel, A. Epidemiology of suicide in Spain, 1981–2008: A spatiotemporal analysis. Public Health. 2013;127:380–385. doi: 10.1016/j.puhe.2012.12.007. [DOI] [PubMed] [Google Scholar]
- 45.Helbich M, et al. Urban-rural inequalities in suicide mortality: a comparison of urbanicity indicators. Int. J. Health Geogr. 2017;16:39. doi: 10.1186/s12942-017-0112-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Philip J, et al. Relationship of social network to protective factors in suicide and alcohol use disorder intervention for rural Yup’ik Alaska Native youth. Psychosocial Intervention. 2016;25:45–54. doi: 10.1016/j.psi.2015.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Christodoulou C, et al. Suicide and seasonality. Acta Psychiat. Scand. 2011;125:127–146. doi: 10.1111/j.1600-0447.2011.01750.x. [DOI] [PubMed] [Google Scholar]
- 48.Silveira ML, et al. Seasonality of suicide behavior in Northwest Alaska: 1990–2009. Public Health. 2016;137:35–43. doi: 10.1016/j.puhe.2016.02.010. [DOI] [PubMed] [Google Scholar]
- 49.Gracia E, et al. The spatial epidemiology of intimate partner violence: Do neighborhoods matter? Am. J. Epidemiol. 2015;182:58–66. doi: 10.1093/aje/kwv016. [DOI] [PubMed] [Google Scholar]
- 50.Anderson C, Ryan LM. A comparison of spatio-temporal disease mapping approaches including an application to ischaemic heart disease in New South Wales, Australia. Int. J. Environ. Res. Public Health. 2017;14:146–161. doi: 10.3390/ijerph14020146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Law J, Quick M, Chan P. Bayesian spatio-temporal modeling for analysis local patterns of crime over time at the small-area level. J. Quant. Criminol. 2014;30:57–78. doi: 10.1007/s10940-013-9194-1. [DOI] [Google Scholar]
- 52.Freisthler B, Weiss RE. Using Bayesian space-time models to understand the substance use environment and risk for being referred to child protective services. Subst. Use Misuse. 2008;43:239–251. doi: 10.1080/10826080701690649. [DOI] [PubMed] [Google Scholar]
- 53.Cunradi CB, Mair C, Ponicki W, Remer L. Alcohol outlets, neighborhood characteristics, and intimate partner violence: Ecological analysis of a California city. J. Urban Health. 2011;88:191–200. doi: 10.1007/s11524-011-9549-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Sparks CS. Violent crime in San Antonio, Texas: An application of spatial epidemiological methods. Spat. Spatiotemporal. Epidemiol. 2011;2:301–309. doi: 10.1016/j.sste.2011.10.001. [DOI] [PubMed] [Google Scholar]
- 55.Marco M, Gracia E, Martín-Fernández M, López-Quílez A. Validation of a Google Street View-based neighborhood disorder observational scale. J. Urban Health. 2017;94:190–198. doi: 10.1007/s11524-017-0134-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Marco M, Gracia E, López-Quílez A. Linking neighborhood characteristics and drug-related police interventions: A Bayesian spatial analysis. ISPRS Int. J. Geo-Inf. 2017;6:65. doi: 10.3390/ijgi6030065. [DOI] [Google Scholar]
- 57.Gracia E, López-Quílez A, Marco. M, Lila M. Mapping child maltreatment risk: A 12-year spatio-temporal analysis of neighborhood influences. Int. J. Health Geogr. 2017;16:38. doi: 10.1186/s12942-017-0111-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Marco M, et al. Neighborhood characteristics, alcohol outlet density, and alcohol-related calls-for-service: A spatiotemporal analysis in a wet drinking country. Int. J. Geo-Inf. 2017;6:380. doi: 10.3390/ijgi6120380. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.