

Abstract
Platelet-activating factor (PAF) promotes glomerular extracellular matrix (ECM) deposition, primarily through activation of the protein kinase C (PKC) pathway. The present study was designed to investigate whether atorvastatin, which mediates a protective effect against glomerular ECM deposition and diabetic neuropathy, may interfere with the PKC-transforming growth factor-β1 (TGF-β1) pathway in a model of human mesangial cells (HMCs) exposed to a high glucose (HG) and lysophosphatidylcholine (LPC) environment. HMCs were divided into three treatment groups: Control, high glucose and lysophosphatidylcholine (HG+LPC), and HG+LPC+atorvastatin. Cells were cultured for 24 h. The levels of the ECM-associated molecules collagen IV (Col IV) and fibronectin (Fn) in the supernatant were detected using an ELISA kit. PKC-β1, TGF-β1 and PAF-receptor gene expression was detected by reverse transcription-quantitative polymerase chain reaction. PKC-β1 and TGF-β1 protein expression was detected by western blotting, and the subcellular localization of PKC-β1 was assessed using immunofluorescence. The results indicated that atorvastatin may reduce the secretion of ECM components (Fn and Col IV) in HMCs in a HG and LPC environment, by inhibiting the increase in PAF secretion and the activation of the PKC-TGF-β1 signaling pathway.
Keywords: platelet-activating factor, high glucose and lysophosphatidylcholine, protein kinase C, extracellular matrix, atorvastatin
Introduction
Diabetic neuropathy (DN) is an important microvascular complication of diabetes. The principal pathological alterations in DN include hypertrophic mesangial cells (MCs), the abnormal deposition of the extracellular matrix (ECM) and renal interstitial fibrosis (1). Fibronectin (Fn) is an important component of the ECM. Fn is primarily synthesized in the early stages of DN and is associated with the local inflammatory reaction of the kidney (2). Collagen IV (Col IV) is one of the major components of the basement membrane. Increased synthesis leads to glomerulosclerosis (3). Additionally, chronic inflammation is associated with abnormal ECM deposition. These alterations are involved in the occurrence and development of DN (4). Platelet-activating factor (PAF) has been reported to be a strong inflammatory factor and may damage renal tissue in a variety of ways (5). A high glucose (HG) and lysophosphatidylcholine (LPC) environment increases the expression of inflammatory cytokines, leading to the stimulation of MCs and endothelial cells to continuously synthesize PAF, ECM and protein kinase C-β1 (PKC-β1) (5). PKC is aberrantly activated in the diabetic kidney, which causes an increase in PKC-β1 activity and the deposition of ECM proteins, including Fn and Col IV (6).
In addition to their lipid lowering effects, statins may inhibit 3-hydroxy-3-methylglutaryl coenzyme A reductase (7). Studies have reported that atorvastatin may significantly reduce the plasma levels of C-reactive, interleukin (IL)-1β, IL-6, tumor necrosis factor-α and other inflammatory markers in patients with Alzheimer's disease (8). Furthermore, statins inhibit HG- and LPC-induced secretion of the ECM (9). These notable effects of statins may be present due to their lipid-lowering and anti-inflammatory actions, in addition to their pleiotropic effects. As a result, statins have been used not only in cardiovascular disease, but for other conditions, including DN (10). However, more evidence in properly designed trials is required to determine whether the protective effect of atorvastatin on the kidney is associated with PAF and PKC-β1. In the present study, it was demonstrated that atorvastatin may reduce the secretion of Fn and Col IV in human (H)MCs in a HG and LPC environment, by reducing the increase in PAF secretion via inhibition of PKC-transforming growth factor-β1 (TGF-β1) signaling.
Materials and methods
Cell culture
Immortalized HMCs (donated by Professor Sun Zilin, Department of Endocrinology, Zhongda Hospital affiliated with Southeast University, Nangjing, China) (11), were obtained by double transfection with T-SV40 and H-ras proto-oncogene. These cells retain the basic morphology and biological characteristics of normal human glomerular MCs (12). The cells were maintained in a sterile incubator with 10% fetal calf serum (Invitrogen; Thermo Fisher Scientific, Inc., Waltham, MA, USA) and Dulbecco's modified Eagle's medium (DMEM; Thermo Fisher Scientific Inc.) in a humidified atmosphere with 5% CO2 at 37°C. When cells had reached 90% confluency, cells were seeded into 6-well plates (6×105 cells/well) and then incubated at 37°C and 5% CO2 for 12 h.
Cells were then divided into three groups: A, control [5.5 mmol/l D-glucose (Enzo Life Sciences, Inc., Farmingdale, NY, USA)] (11); B, HG+LPC group [30 mmol/l D-glucose+20 mg/l LPC (Sigma-Aldrich; Merck KGaA, Darmstadt, Germany)]; C, atorvastatin [30 mmol/l D-glucose+20 mg/l LPC+10 µmol/l atorvastatin (Pfizer Inc., New York, NY, USA)]. Group C was pretreated with atorvastatin for 1 h prior to the addition of 30 mmol/l D-glucose and 20 mg/l LPC. Following ≥24 h, the supernatant of all three groups was collected and the experiments were repeated three times.
ELISA analysis
The expression levels of Fn, Col IV and PAF in the supernatant of each group was determined by ELISA. Human FN ELISA kit (NeoScientific, Cambridge, MA, USA; cat. no. HF0011), Human Col IV ELISA kit (NeoScientific; cat. no. HC0787), Human PAF ELISA kit (NeoScientific; cat. no. HP0596). The method was performed according to the manufacturer's protocol Each group was set up in three wells in order to repeat the experiment three times.
Detection of PAF receptor (PAF-R), GADPH, PKC-β1 and TGF-β1 expression in HMCs by reverse transcription-quantitative polymerase chain reaction (RT-qPCR). Total RNA was extracted using TRIzol reagent (Invitrogen; Thermo Fisher Scientific, Inc.), according to the manufacturer's protocol. The RT reaction was performed using the Revert Aid First Strand cDNA Synthesis reagent (Fermentas; Thermo Fisher Scientific, Inc.) at 42°C for 15 min and 95°C for 3 min, followed by 4°C for 5 min; according to the manufacturer's protocol. PAF-R primer sequences were as follows: Forward, 5′-TGCCCCTGCTACAGGCACCA-3′ and reverse, 5′-TGCTGTAAACAATCGGGAAGAG-3′. GAPDH primers sequences were as follows: Forward, 5′-ACACCCACTCCTCCACCTTT-3′ and reverse, 5′-TTACTCCTTGGAGGCCATGT-3.
PKC-β1 primer sequences were as follows: Forward, 5′-GGGGGCGACCTCATGTAT-3′ and reverse, 5′-GCAATTTCTGCAGCGTAAAA-3′. TGF-β1 primer sequences were as follows: Forward, 5′-ACTACTACGCCAAGGAGGTCAC-3′ and reverse, 5′-TGCTTGAACTTGTCATAGATTTCG-3′. Primers were designed using Premier Oligo 5 and Primer 6.22 software (Premier Biosoft International, Palo Alto, CA, USA). qPCR assays were performed using a QuantStudio 5 Real-Time PCR System (Thermo Fisher Scientific, Inc.) in a 20 µl PCR volume using iQ SyBr Green Supermix for 10 sec at 95°C, followed by 40 cycles of 56°C for 20 sec and 72°C for 10 sec. The quantification cycle (2−ΔΔCq) method was used to calculate the relative changes in expression levels (13). Each sample was prepared in triplicate, and the results are expressed as the mean of three independent experiments.
Western blotting
The cells were lysed using a HMC lysis buffer (Promega Corporation, Madison, WI, USA). Lysates were transferred into an Eppendorf tube and centrifuged at 12,000 × g for 15 min at 4°C. The supernatant was collected, and the concentration of protein was determined by ultraviolet spectroscopy (14). Protein (50 µg) were separated by 5% SDS-PAGE (Bio-Rad Laboratories Inc., Hercules, CA, USA) and transferred onto a nitrocellulose membrane (Bio-Rad Laboratories, Inc.). The membrane was incubated in TBS with 0.1% Tween-20 (TBST) and 5% fat-free milk for 1 h at 37°C. The proteins were detected with the addition of primary antibodies which were left to incubate overnight at 4°C (Sigma-Aldrich; Merck KGaA). The dilution ratios were as follows: TGF-β1 (Santa Cruz Biotechnology, Inc., Dallas, TX, USA; cat. no. SC-130348; 1:2,000); PKC-β1 (Santa Cruz Biotechnology, Inc.; cat. no. SC-8393; 1:400) and GAPDH (Santa Cruz Biotechnology, Inc.; cat. no. SC-32233; 1:3,000). Following washing with TBST, membranes were incubated with horseradish peroxidase-conjugated secondary antibodies (Santa Cruz Biotechnology, Inc.; cat. no. SC-516245; 1:5,000) for 1 h at 4°C, followed by additional washes with TBST. Protein bands were visualized by enhanced chemiluminescence (Pierce; Thermo Fisher Scientific, Inc.). The Scion Image 4.03 system (National Institutes of Health, Bethesda, MD, USA) was used to quantify band intensity, and results are expressed as the mean of three independent experiments.
Antibodies, immunoprecipitation and immunoblotting
Cells (2×104 cells/ml) were cultured on coverslips in 24-well plates and serum-starved for 24 h. The cells were subsequently fixed with 4% paraformaldehyde for 5 min at −20°C and blocked for 30 min in 0.2% Triton X-100 in PBS. The cells were incubated with aforementioned primary antibodies (1:50) overnight at 4°C, followed by fluorescein isothiocyanate-conjugated secondary anti-mouse IgG antibodies (Dako; Agilent Technologies, Inc., Santa Clara, CA, USA) for 1 h in the dark at room temperature. Following three washes in PBS, coverslips were placed on slides and visualized by confocal microscopy (magnification, ×400). Fluorescence intensity was analyzed using Image J software (version 1.48; National Institutes of Health).
Statistical analysis
All data are presented as the mean ± standard deviation. Data was analyzed using SPSS 18.0 software (SPSS, Inc., Chicago, IL, USA) for Windows. Multigroup comparisons of the means were performed using one-way analysis of variance test followed by the Newman-Keuls post hoc test. Differences between two groups were assessed by Student's t-test. α=0.05 and P<0.05 was considered to indicate a statistically significant difference.
Results
Atorvastatin inhibits the expression of Fn and Col IV in HMCs
Levels of Fn and Col IV in the supernatant of the HG+LPC group were significantly higher compared with the control group (P<0.05). In the presence of atorvastatin their levels were significantly decreased (Table I; Figs. 1 and 2).
Table I.
Effects of atorvastatin on Fn (mg/l) and Col IV (µg/l) in human mesangial cells.
| Group | Fn (mg/l) | Col IV (µg/l) |
|---|---|---|
| Control | 3.90±0.43 | 4.54±0.74 |
| HG+LPC | 7.89±0.34a | 16.32±1.55a |
| HG+LPC+atorvastatin | 5.17±0.34b | 10.80±1.70b |
P<0.05 vs. control group
P<0.05 vs. HG+LPC group. Each group was cultured for 24 h and the experiment was repeated three times. Fn and Col IV levels in cell culture supernatants were detected by ELISA. Fn, fibronectin; Col IV, collagen IV; HG, high glucose; LPC, lysophosphatidylcholine.
Figure 1.
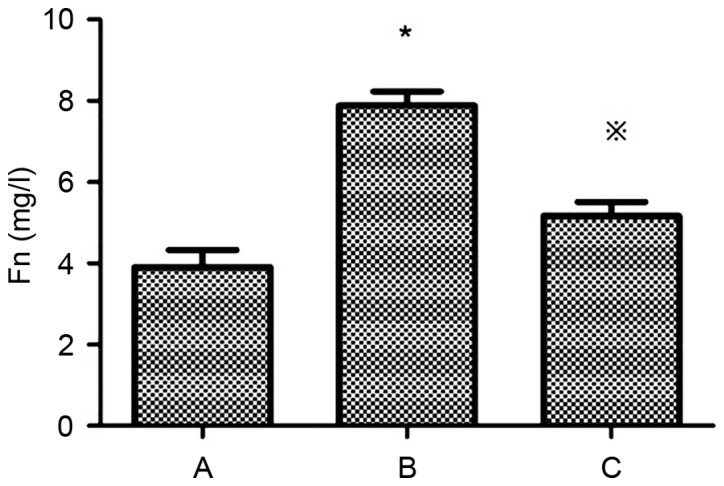
Effects of atorvastatin on Fn (mg/l) in human mesangial cells. The level of Fn in each group was detected by ELISA. Group A, control (5.5 mmol/l D-glucose); Group B, HG+LPC group (30 mmol/l D-glucose+20 mg/l LPC); Group C, atorvastatin group (30 mmol/l D-glucose+20 mg/l LPC+10 µmol/l atorvastatin). Data represents the mean ± standard deviation of three independent experiments. *P<0.05 vs. group A; ※P<0.05 vs. group B. Fn, fibronectin; HG, high glucose; LPC, lysophosphatidylcholine.
Figure 2.
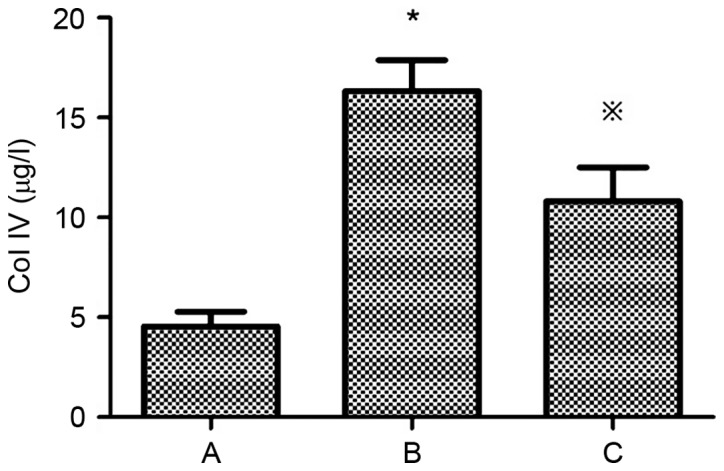
Effects of atorvastatin on Col IV (µg/l) in human mesangial cells. The level of Col IV in each group was detected by ELISA. Group A, control (5.5 mmol/l D-glucose); Group B, HG+LPC group (30 mmol/l D-glucose+20 mg/l LPC); Group C, atorvastatin group (30 mmol/l D-glucose+20 mg/l LPC+10 µmol/l atorvastatin). Data represents the mean ± standard error of three independent experiments. *P<0.05 vs. group A; ※P<0.05 vs. group B. Col IV, collagen IV; HG, high glucose; LPC, lysophosphatidylcholine.
Atorvastatin inhibits the expression of PAF and PAF-R mRNA in HMCs
Compared with the control group, the expression of PAF and PAF-R mRNA was significantly higher in the HG+LPC group (P<0.05). Atorvastatin inhibited the increase in PAF content in the supernatant of HMCs (P<0.05) (Table II; Fig. 3), in addition to the expression of the PAF-R mRNA gene in the HG+LPC environment (P<0.05; Table II; Fig. 4).
Table II.
Effects of atorvastatin on the expression of PAF and PAF-R mRNA gene in human mesangial cells.
| Group | PAF (pg/ml) | PAF-R mRNA expression |
|---|---|---|
| Control | 48.72±2.55 | 1.0±0 |
| HG+LPC | 101.1±3.00a | 2.48±0.18a |
| HG+LPC+atorvastatin | 73.03±5.55b | 1.01±0.11b |
P<0.05 vs. control group
P<0.05 vs. HG+LPC group. Each group was cultured for 24 h and the experiment was repeated three times. The level of PAF in each group was detected by ELISA. Detection of PAF-R gene expression in mesangial cells was by reverse transcription-quantitative polymerase chain reaction. PAF, platelet-activating factor; PAF-R, platelet-activating factor-receptor; HG, high glucose; LPC, lysophosphatidylcholine.
Figure 3.
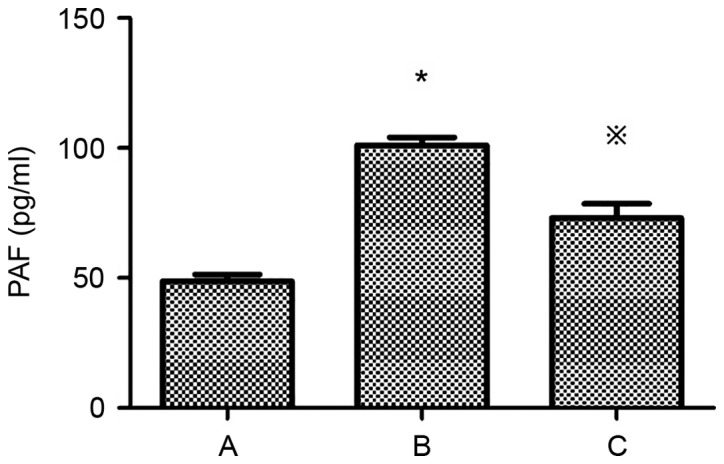
Effects of atorvastatin on PAF (pg/ml) in human mesangial cells. The level of PAF in each group was detected by ELISA. Group A, control (5.5 mmol/l D-glucose); Group B, HG+LPC group (30 mmol/l D-glucose+20 mg/l LPC); Group C, atorvastatin group (30 mmol/l D-glucose+20 mg/l LPC+10 µmol/l atorvastatin). Data represents the mean ± standard error of three independent experiments. *P<0.05 vs. group A; ※P<0.05 vs. group B. PAF, platelet-activating factor; HG, high glucose; LPC, lysophosphatidylcholine.
Figure 4.
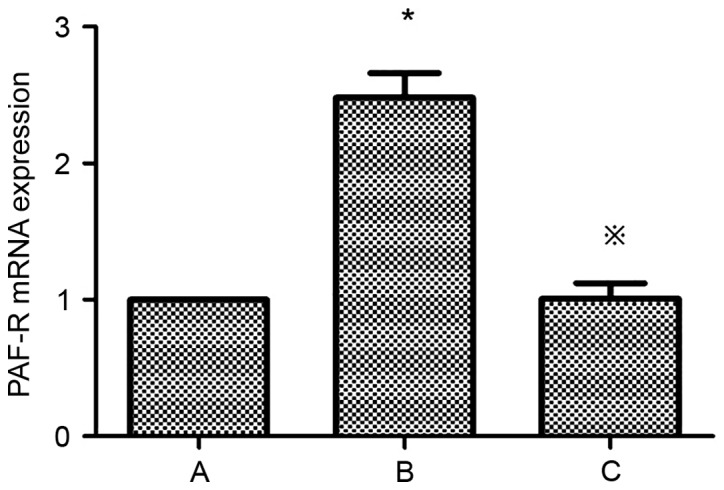
Effects of atorvastatin on PAF-R mRNA expression in HMCs. Detection of PAF-R gene expression in HMCs was detected by reverse transcription-quantitative polymerase chain reaction. Group A, control (5.5 mmol/l D-glucose); Group B, HG+LPC group (30 mmol/l D-glucose+20 mg/l LPC); Group C, atorvastatin group (30 mmol/l D-glucose+20 mg/l LPC+10 µmol/l atorvastatin). Data represents the mean ± standard error of three independent experiments.*P<0.05 vs. group A; ※P<0.05 vs. group B. PAF-R, platelet-activating factor-receptor; HMCs, human mesangial cells; HG, high glucose; LPC, lysophosphatidylcholine.
Atorvastatin inhibits the expression of TGF-β1 in HMCs
TGF-β1 expression is upregulated in HMCs in the presence of PAF, HG and LPC. TGF-β1 mRNA (Table III; Fig. 5) and protein (Fig. 6) expression levels were increased in HMCs treated with HG+LPC relative to the control (P<0.05). Expression was significantly lower in cells treated with atorvastatin compared with those treated with HG+LPC only (P<0.05).
Table III.
Effects of atorvastatin on the expression of TGF-β1 mRNA gene human mesangial cells.
P<0.05 vs. control group
P<0.05 vs. HG+LPC group. Each group was cultured for 24 h and the experiment was repeated three times. Detection of TGF-β1 mRNA expression was by reverse transcription-quantitative polymerase chain reaction. TGF-β1, transforming growth factor-β1; HG, high glucose; LPC, lysophosphatidylcholine.
Figure 5.
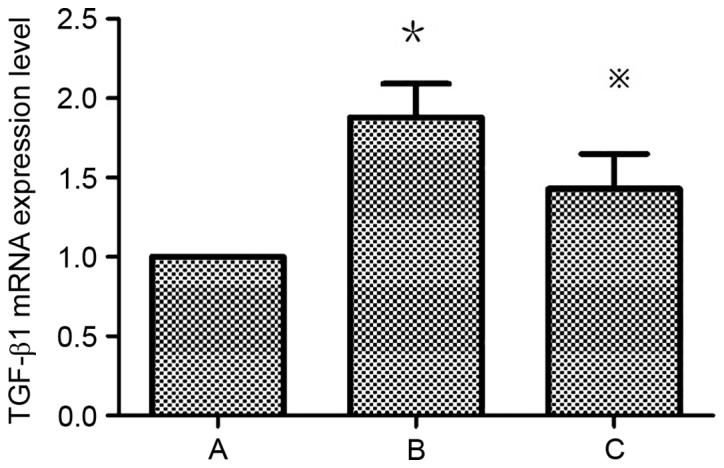
TGF-β1 mRNA expression in human mesangial cells under various treatment conditions. Expression levels were determined relative to that of GAPDH by reverse transcription-quantitative polymerase chain reaction. Group A, control (5.5 mmol/l D-glucose); Group B, HG+LPC group (30 mmol/l D-glucose+20 mg/l LPC); Group C, atorvastatin group (30 mmol/l D-glucose+20 mg/l LPC+10 µmol/l atorvastatin). Data represents the mean ± standard error of three independent experiments. *P<0.05 vs. group A; ※P<0.05 vs. group B. TGF-β1, transforming growth factor-β1; HG, high glucose; LPC, lysophosphatidylcholine.
Figure 6.
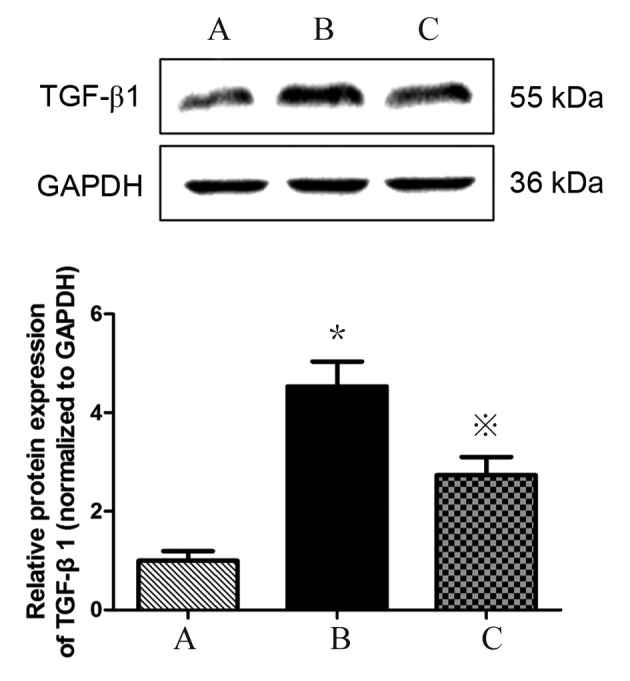
TGF-β1 protein expression in human mesangial cells under various treatment conditions. Protein expression levels were determined by western blotting, with GAPDH used as a loading control. Group A, control; Group B, HG+LPC; Group C, HG+LPC+atorvastatin. Data represents the mean ± standard error of three independent experiments. *P<0.05 vs. group A, ※P<0.05 vs. group B. TGF-β1, transforming growth factor-β1; HG, high glucose; LPC, lysophosphatidylcholine.
Atorvastatin inhibits the expression of PKC-β1 in HMCs
Detection of PKC-β1 mRNA expression in HMCs in each group by RT-qPCR revealed that mRNA levels were significantly higher in the HG+LPC group compared with the control (P<0.05). The expression was significantly higher in the HG+LPC group compared with cells treated with HG+LPC+atorvastatin (P<0.05). Thus, atorvastatin may inhibit the expression of PKC-β1 mRNA in HMCs (Table IV; Fig. 7).
Table IV.
PKC-β1 mRNA expression in each group (2‒ΔΔCq).
P<0.05 vs. control group
P<0.05 vs. HG+LPC group. Each group was cultured for 24 h and the experiment was repeated three times. Detection of PKC-β1 mRNA expression in human mesangial cells was by reverse transcription-quantitative polymerase chain reaction. PKC-β1, protein kinase C-β1; HG, high glucose; LPC, lysophosphatidylcholine.
Figure 7.
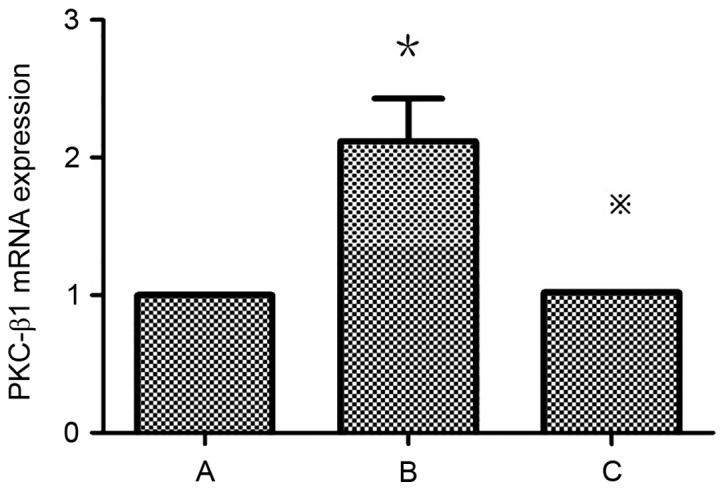
PKC-β1 mRNA expression in human mesangial cells under various treatment conditions. Expression levels were determined relative to that of GAPDH by reverse transcription-quantitative polymerase chain reaction. Group A, control (5.5 mmol/l D-glucose; Group B, HG+LPC group (30 mmol/l D-glucose+20 mg/l LPC); Group C, atorvastatin group (30 mmol/l D-glucose+20 mg/l LPC+10 µmol/l atorvastatin. Data represents the mean ± standard error of three independent experiments. *P<0.05 vs. group A, ※P<0.05 vs. group B. PKC-β1, protein kinase C-β1; HG, high glucose; LPC, lysophosphatidylcholine.
Detection of PKC-β1 protein expression in HMCs in each group by western blotting
PKC-β1 protein (Fig. 8) expression levels were significantly increased in HMCs treated with HG+LPC relative to the control (P<0.05). Expression levels were significantly lower in cells treated with atorvastatin compared with those treated with HG+LPC only (P<0.05).
Figure 8.

PKC-β1 protein expression in human mesangial cells under various treatment conditions. Protein expression levels were determined by western blotting, with GAPDH used as a loading control. Group A, control; Group B, HG+LPC; Group C, HG+LPC+atorvastatin. Data represents the mean ± standard error of three independent experiments. *P<0.05 vs. group A, ※P<0.05 vs. group B. PKC-β1, protein kinase C-β1; HG, high glucose; LPC, lysophosphatidylcholine.
Effect of atorvastatin on the expression and localization of PKC-β1 in HMCs
In control cells, PKC-β1 immunofluorescence was diffusely distributed throughout the cytoplasm, with no membrane or nuclear localization. Treatment with HG and LPC increased PKC-β1 protein expression levels, and induced the translocation of the protein from the cytoplasm to the nucleus. These effects were reduced in cells treated with atorvastatin (Fig. 9).
Figure 9.

Immunocytofluorescent analysis of PKC-β1 localization in human mesangial cells under various treatment conditions. PKC-β1 was detected by immunocytofluorescence and visualized by confocal microscopy. Magnification, ×400. Group A, control; Group B, HG+LPC; Group C, HG+LPC+atorvastatin. PKC-β1, protein kinase C-β1; HG, high glucose; LPC, lysophosphatidylcholine.
Mean fluorescence intensity of PKC-β1 in HMCs under various treatment conditions
The mean fluorescence intensity of PKC-β1 in HMCs was significantly increased in the HG+LPC group compared with the control (P<0.05). The addition of atorvastatin to the HG+LPC environment significantly reduced the mean fluorescence intensity (P<0.05; Table V; Fig. 10).
Table V.
Mean fluorescence intensity of PKC-β1 in human mesangial cells under various treatment conditions.
| Group | Mean fluorescence intensity |
|---|---|
| Control | 11.80±2.57 |
| HG+LPC | 48.92±7.70a |
| HG+LPC+atorvastatin | 18.53±3.74b |
P<0.05 vs. control group
P<0.05 vs. HG+LPC group. Each group was cultured for 24 h and the experiment was repeated three times. PKC-β1, protein kinase C-β1; HG, high glucose; LPC, lysophosphatidylcholine.
Figure 10.
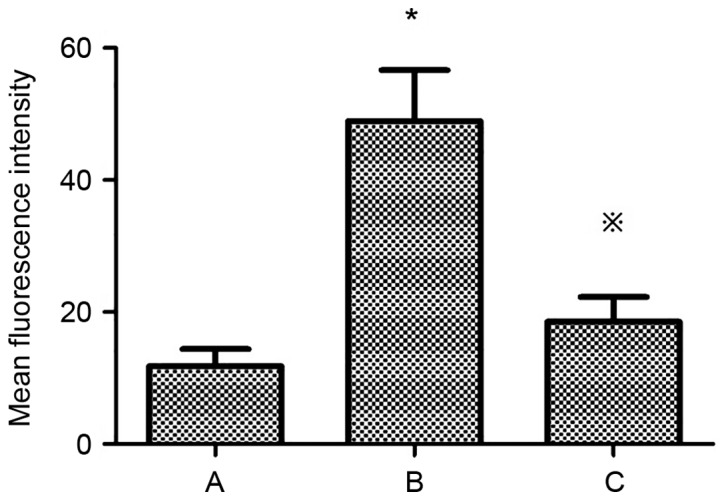
Mean fluorescence intensity of PKC β1 in human mesangial cells under various treatment conditions. Group A, control (5.5 mmol/l D-glucose); Group B, HG+LPC group (30 mmol/l D-glucose+20 mg/l LPC); Group C, atorvastatin group (30 mmol/l D-glucose+20 mg/l LPC+10 µmol/l atorvastatin). Data represents the mean ± standard error of three independent experiments. *P<0.05 vs. group A, ※P<0.05 vs. group B. PKC-β1, protein kinase C-β1; HG, high glucose; LPC, lysophosphatidylcholine.
Discussion
Statins have the potential to be used to treat DN. This disease is thought to be triggered by abnormal ECM deposition and a decrease in the glomerular filtration rate. Morphometric studies on HMCs in a HG environment provide convincing evidence that Col IV and Fn are increased, which partially explains the occurrence of glomerular sclerosis and renal failure (15,16). Genetic and environmental factors contribute to renal failure. For example, patients with diabetes may have increased concentrations of PAF, a potent pro-inflammatory factor implicated in the pathogenesis of DN (17). Under certain stimuli, various cell types may secrete PAF, including platelets, endothelial cells and MCs (18). The primary source of PAF, however, is the kidney, in which 20–25% of PAF is secreted by MCs (19). MCs are the principal component of the glomerular filtration barrier and excessive expression of PAF may cause damage to this interface. A previous study reported that PAF is able to promote the secretion of the ECM (20). Excessive secretion of ECM deposition in MCs results in the development of glomerular sclerosis (20). The PAF-R is a G protein coupled receptor that is expressed on MCs. The binding of PAF triggers downstream signaling pathways resulting in the production of effector molecules, including arachidonic acid, prostacyclin and TGF-β1 which, in turn, regulate ECM secretion (5,21). The expression of PAF-R mRNA has been detected in all cells of the kidney, and its levels depend on the amount of PAF present. In a model of unilateral ureteral obstruction, PAF-R expression increased by 70-fold (22), revealing that an inflammatory environment may stimulate the kidney to secrete PAF, and the increase in PAF secretion, in turn, increases the expression of the PAF-R. In a mixed culture model of rat and human MCs, it was demonstrated that PAF was able to upregulate ECM secretion (23); a corresponding increase in Fn and Col IV was additionally observed in this model (24). To support this observation, it was confirmed in the present study that pretreatment of the HMCs with HG and LPC significantly increased Col IV and Fn via the induction of PAF.
Inflammatory factors promote the expression of TGF-β1 by activating the PKC-dependent pathway; this stimulates the synthesis of Fn (16). In line with this statement, a rise in PAF activity in the cells exposed to HG+LPC was observed in the present study, which was concomitant with an increase in Fn, Col IV and PKC-β1. PAF has detrimental effects in MCs, and this may be through the activation of the PKC-β1 signaling pathway, which leads to increased expression of ECM proteins (16). It has been previously reported that HG may activate the PKC-β1 pathway and promote the secretion of TGF-β1 in MCs. TGF-β1 may further stimulate the synthesis of collagen III and IV, Fn and other ECM components (15). Consistent with these findings, the present study demonstrated that an increase in PAF expression in cells exposed to HG+LPC was associated with increased levels of PKC-β1 and TGF-β1. This finding may indicate that PAF induces a molecular cascade that activates PKC-β1, leading to ECM accumulation and glomerular sclerosis (21).
Statins have been widely used as lipid-lowering drugs to exert a protective effect on endotheliocytes. Statins reduce cardiovascular morbidity and mortality in patients with end-stage renal disease (25). This effect of statins may be due to their lipid-lowering effects, in addition to their pleiotropic effects, including the ability to promote endothelial repair, and reduce inflammation and oxidative stress (26). Atorvastatin inhibits the HG-induced secretion of Col IV and Fn, mesangial matrix deposition and mesangial cell proliferation (27,28). Atorvastatin has been reported to have anti-fibrotic effects in chronic kidney disease (9). Essentially, atorvastatin has the ability to reduce glomerular mesangial ECM deposition, and thus delay the progression of glomerular sclerosis (29). A previous study demonstrated that statins inhibit the production of PAF, and this action may be through the inhibition of TGF-β1 and reactive oxygen species as well as the expression of other cytokines, in addition to mothers against decapentaplegic homolog protein expression in glomerular MCs, thus inhibiting Fn and Col IV secretion (9). A recent report observed that statins may suppress PAF production (30), and they may therefore effectively treat cardiovascular diseases, and conditions including diabetes (31) and DN (32). The present study revealed that atorvastatin reduced the PAF content in MCs in a HG and LPC environment. This may be associated with the upregulation of PAF-acetylhydrolase activity (33), leading to an increase in PAF degradation and thus reducing the renal protective effect of ECM secretion in the culture model. The present study additionally demonstrated that the expression of the PAF-R gene in the HMCs in the atorvastatin-pretreated group was significantly decreased compared with the HG and LPC group. This suggested that atorvastatin may inhibit the expression of the PAF-R gene in HMCs induced by HG and LPC. The expression of the PAF-R gene in MCs is associated with nuclear factor-κB (NF-κB) activity. HG and LPC may activate the PKC-NF-κB pathway in MCs, which subsequently increases the transcription of the PAF-R gene (34). However, the present study identified that when the PAF-R gene was significantly increased, PKC-β1 and TGF-β1 were increased. Therefore, it may be hypothesized that atorvastatin may inhibit the expression of the PAF-R gene in HG and LPC induced HMCs by inhibiting the activation of TGF-β1, and inhibiting the PKC pathway. However, the specific mechanism remains unclear and requires further investigation.
In the present study, the expression of PKC-β1 mRNA and protein in HMCs pretreated with atorvastatin was significantly lower compared with groups treated with HG and LPC alone. Immunofluorescence indicated that the expression of PKC-β1 in the cytoplasm and nucleus was additionally reduced, suggesting that atorvastatin may inhibit the activation of the PKC pathway under the conditions of HG and LPC. Simvastatin inhibits inflammatory and oxidative stress by inhibiting the activation of the PKC pathway, thus exerting a protective effect in patients with chronic kidney disease (35). Atorvastatin may inhibit the expression of TGF-β1, which may alleviate the local inflammatory reaction of the kidney (36). In the present study, suppression of PKC-β1 signaling by atorvastatin is partly responsible for the reduced levels of PAF and ECM. These results all suggest that atorvastatin may alter the activation of the PKC-β1/TGF-β1 pathway to reduce ECM secretion in HMCs stimulated by HG and LPC, although the specific mechanism remains unclear and further research is required.
In conclusion, the results of the present study suggested that atorvastatin may reduce the secretion of ECM proteins (Fn and Col IV) by inhibiting the secretion of PAF, the expression of PAF-R, and the activation of the PKC-β1/TGF-β1 signaling pathway in HMCs under HG and LPC conditions. Additionally, these findings revealed that atorvastatin may delay glomerular fibrosis by inhibiting the PKC-β1/TGF-β1 signaling pathway in HMCs. This mechanism may contribute to the efficiency of atorvastatin for the treatment of DN.
Acknowledgements
The authors gratefully acknowledge Professor Sun Zilin from the Zhongda Hospital Affiliated with Southeast University (Nangjing, China), for the donation of immortalized human mesangial cells. The authors would also like to thank the Science and Research Center, Guilin Medical University (Guilin, China) for their technical support.
Funding
The present study was supported by the National Natural Science Foundation of China. Grant: Research on the relationship between insulin resistance of podocytes in diabetic neuropathy (grant no. 81560148).
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Authors' contributions
SXZ designed the study. YHX and XYH performed the experiments, and YHX was the major contributor in the writing of the manuscript. QH and FY analyzed the data. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
References
- 1.Shao Y, Lv C, Wu C, Zhou Y, Wang Q. Mir-217 promotes inflammation and fibrosis in high glucose cultured rat glomerular mesangial cells via Sirt1/HIF-1α signaling pathway. Diabetes Metab Res Rev. 2016;32:534–543. doi: 10.1002/dmrr.2788. [DOI] [PubMed] [Google Scholar]
- 2.Chang ZL, Beezhold DH, Personius CD, Shen ZL. Fibronectin cell-binding domain triggered transmembrane signal transduction in human monocytes. J Leukoc Biol. 1993;53:79–85. doi: 10.1002/jlb.53.1.79. [DOI] [PubMed] [Google Scholar]
- 3.Liu Y, Wang Z, Yin W, Li Q, Cai M, Zhang C, Xiao J, Hou H, Li H, Zu X. Severe insulin resistance and moderate glomerulosclerosis in a minipig model induced by high-fat/high-sucrose/high-cholesterol diet. Exp Anim. 2007;56:11–20. doi: 10.1538/expanim.56.11. [DOI] [PubMed] [Google Scholar]
- 4.Yiu WH, Lin M, Tang SC. Toll-like receptor activation: From renal inflammation to fibrosis. Kidney Int Suppl (2011) 2014;4:20–25. doi: 10.1038/kisup.2014.5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Fragopoulou E, Iatrou C, Antonopoulou S, Ruan XZ, Fernando RL, Powis SH, Moorhead JF, Varghese Z. Platelet-activating factor (PAF) increase intracellular lipid accumulation by increasing both LDL and scavenger receptors in human mesangial cells. J Lab Clin Med. 2006;147:281–289. doi: 10.1016/j.lab.2006.01.004. [DOI] [PubMed] [Google Scholar]
- 6.Koya D, Jirousek MR, Lin YW, Ishii H, Kuboki K, King GL. Characterization of protein kinase C beta isoform activation on the gene expression of transforming growth factor-beta, extracellular matrix components, and prostanoids in the glomeruli of diabetic rats. J Clin Invest. 1997;100:115–126. doi: 10.1172/JCI119503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Banach M, Dinca M, Ursoniu S, Serban MC, Howard G, Mikhailidis DP, Nicholls S, Lip GY, Glasser S, Martin SS, et al. A PRISMA-compliant systematic review and meta-analysis of randomized controlled trials investigating the effects of statin therapy on plasma lipid concentrations in HIV-infected patients. Pharmacol Res. 2016;111:343–356. doi: 10.1016/j.phrs.2016.06.005. [DOI] [PubMed] [Google Scholar]
- 8.Zhao L, Zhao Q, Zhou Y, Zhao Y, Wan Q. Atorvastatin may correct dyslipidemia in adult patients at risk for Alzheimer's disease through an anti-inflammatory pathway. CNS Neurol Disord Drug Targets. 2016;15:80–85. doi: 10.2174/1871527315999160111160143. [DOI] [PubMed] [Google Scholar]
- 9.Song CY, Kim BC, Lee HS. Lovastatin inhibits oxidized low-density lipoprotein-induced plasminogen activator inhibitor and transforming growth factor-beta1 expression via a decrease in Ras/extracellular signal-regulated kinase activity in mesangial cells. Transl Res. 2008;151:27–35. doi: 10.1016/j.trsl.2007.09.008. [DOI] [PubMed] [Google Scholar]
- 10.Kom GD, Schwedhelm E, Maas R, Schneider L, Benndorf R, Böger RH. Impact of atorvastatin treatment on platelet-activating factor acetylhydrolase and 15-F(2trans)-isoprostane in hypercholesterolaemic patients. Br J Clin Pharmacol. 2007;63:672–679. doi: 10.1111/j.1365-2125.2006.02832.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Zhou SX, Lei MX, Zhao JJ, Chen HL. The study of the effects of platelet activating factor (PAF) on the relation between the endothelial cell and mesangial cells exposed to high glucose and high lysophosphatidylcholine. Chin J Diabetes. 2010;18:591–593. (In Chinese) [Google Scholar]
- 12.Sraer JD, Delarue F, Hagege J, Feunteun J, Pinet F, Nguyen G, Rondeau E. Stable cell lines of T-SV40 immortalized human glomerular mesangial cells. Kidney Int. 1996;49:267–270. doi: 10.1038/ki.1996.38. [DOI] [PubMed] [Google Scholar]
- 13.Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) method. Methods. 2001;25:402–408. doi: 10.1006/meth.2001.1262. [DOI] [PubMed] [Google Scholar]
- 14.Zhu D, Qian F, Wu Y, Jones DS, Rowe C, Narum DL, Duffy P, Miller LH, Saul A. Determination of protein concentration for protein-protein conjugates using ultraviolet absorption. J Immunol Methods. 2013;387:317–321. doi: 10.1016/j.jim.2012.10.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Meier M, Park JK, Overheu D, Kirsch T, Lindschau C, Gueler F, Leitges M, Menne J, Haller H. Deletion of protein kinase C-beta isoform in vivo reduces renal hypertrophy but not albuminuria in the streptozotocin-induced diabetic mouse model. Diabetes. 2007;56:346–354. doi: 10.2337/db06-0891. [DOI] [PubMed] [Google Scholar]
- 16.Tahara A, Tsukada J, Tomura Y, Yatsu T, Shibasaki M. Vasopressin increases type IV collagen production through the induction of transforming growth factor-beta secretion in rat mesangial cells. Pharmacol Res. 2008;57:142–150. doi: 10.1016/j.phrs.2008.01.003. [DOI] [PubMed] [Google Scholar]
- 17.Davignon J. Emphasis on pleiotropic effects, a new paradigm shift? Coron Artery Dis. 2004;15:223–225. doi: 10.1097/01.mca.0000131571.06897.da. [DOI] [PubMed] [Google Scholar]
- 18.Alfaro V. Role of histamine and platelet-activating factor in allergic rhinitis. J Physiol Biochem. 2004;60:101–111. doi: 10.1007/BF03168446. [DOI] [PubMed] [Google Scholar]
- 19.Tsoupras AB, Fragopoulou E, Nomikos T, Iatrou C, Antonopoulou S, Demopoulos CA. Characterization of the de novo biosynthetic enzyme of platelet activating factor, DDT-insensitive cholinephosphotransferase, of human mesangial cells. Mediators Inflamm. 2007;2007:27683. doi: 10.1155/2007/27683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Reznichenko A, Korstanje R. The role of platelet-activating factor in mesangial pathophysiology. Am J Pathol. 2015;185:888–896. doi: 10.1016/j.ajpath.2014.11.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Honda ZI, Ishii S, Shimizu T. Platelet-activating factor receptor. J Biochem. 2002;131:773–779. doi: 10.1093/oxfordjournals.jbchem.a003164. [DOI] [PubMed] [Google Scholar]
- 22.Asano KK, Taniguchi SS, Nakao AA, Watanabe TT, Kurokawa KK. Distribution of platelet activating factor receptor mRNA along the rat nephron segments. Biochem Biophys Res Commun. 1996;225:352–357. doi: 10.1006/bbrc.1996.1179. [DOI] [PubMed] [Google Scholar]
- 23.Ruiz-Ortega M, Bustos C, Plaza JJ, Egido J. Overexpression of extracellular matrix proteins in renal tubulointerstitial cells by platelet-activating-factor stimulation. Nephrol Dial Transplant. 1998;13:886–892. doi: 10.1093/ndt/13.4.886. [DOI] [PubMed] [Google Scholar]
- 24.Ruiz-Ortega M, Largo R, Bustos C, Gómez-Garre D, Egido J. Platelet-activating factor stimulates gene expression and synthesis of matrix proteins in cultured rat and human mesangial cells: Role of TGF-beta. J Am Soc Nephrol. 1997;8:1266–1275. doi: 10.1681/ASN.V881266. [DOI] [PubMed] [Google Scholar]
- 25.Kopecky C, Genser B, Drechsler C, Krane V, Kaltenecker CC, Hengstschläger M, März W, Wanner C, Säemann MD, Weichhart T. Quantification of HDL proteins, cardiac events, and mortality in patients with type 2 diabetes on hemodialysis. Clin J Am Soc Nephrol. 2015;10:224–231. doi: 10.2215/CJN.06560714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tremoulet AH. The role of statins in inflammatory vasculitides. Autoimmunity. 2015;48:177–180. doi: 10.3109/08916934.2015.1027818. [DOI] [PubMed] [Google Scholar]
- 27.Kolavennu V, Zeng L, Peng H, Wang Y, Danesh FR. Targeting of RhoA/ROCK signaling ameliorates progression of diabetic nephropathy independent of glucose control. Diabetes. 2008;57:714–723. doi: 10.2337/db07-1241. [DOI] [PubMed] [Google Scholar]
- 28.Mooradian AD, Haas M. Statins ameliorate glomerular permeability changes in streptozotocin-induced diabetic rats. Am J Ther. 2007;14:41–45. doi: 10.1097/01.mjt.0000245236.88942.fb. [DOI] [PubMed] [Google Scholar]
- 29.Song Y, Li C, Cai L. Fluvastatin prevents nephropathy likely through suppression of connective tissue growth factor-mediated extracellular matrix accumulation. Exp Mol Pathol. 2004;76:66–75. doi: 10.1016/j.yexmp.2003.08.002. [DOI] [PubMed] [Google Scholar]
- 30.Jaikumkao K, Pongchaidecha A, Chattipakorn N, Chatsudthipong V, Promsan S, Arjinajarn P, Lungkaphin A. Atorvastatin improves renal organic anion transporter 3 and renal function in gentamicin-induced nephrotoxicity in rats. Exp Physiol. 2016;101:743–753. doi: 10.1113/EP085571. [DOI] [PubMed] [Google Scholar]
- 31.Pahan K. Lipid-lowering drugs. Cell Mol Life Sci. 2006;63:1165–1178. doi: 10.1007/s00018-005-5406-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Tsoupras AB, Iatrou C, Frangia C, Demopoulos CA. The implication of platelet activating factor in cancer growth and metastasis: Potent beneficial role of PAF-inhibitors and antioxidants. Infect Disord Drug Targets. 2009;9:390–399. doi: 10.2174/187152609788922555. [DOI] [PubMed] [Google Scholar]
- 33.Noto H, Hara M, Karasawa K, Iso-O N, Satoh H, Togo M, Hashimoto Y, Yamada Y, Kosaka T, Kawamura M, et al. Human plasma platelet activating factor acetylhydrolase binds to all them urine lipoproteins, conferring protection again stoxidatives tress. Arterioscler Thromb Vasc Biol. 2003;23:829–835. doi: 10.1161/01.ATV.0000067701.09398.18. [DOI] [PubMed] [Google Scholar]
- 34.Park CW, Kim JH, Lee JH, Kim YS, Ahn HJ, Shin YS, Kim SY, Choi EJ, Chang YS, Bang BK. High glucose-induced intercellular adhesion molecule-1(ICAM-1) expression through an osmotic effect in rat mesangial cells is PKC-NF-kappa B-dependent. Diabetologia. 2000;43:1544–1553. doi: 10.1007/s001250051567. [DOI] [PubMed] [Google Scholar]
- 35.Zhang F, Sun D, Chen J, Guan N, Huo X, Xi H. Simvastatin attenuates angiotensin II-induced inflammation and oxidative stress in human mesangial cells. Mol Med Rep. 2015;11:1246–1251. doi: 10.3892/mmr.2014.2871. [DOI] [PubMed] [Google Scholar]
- 36.Vincent JL, Spapen H, Bakker J, Webster NR, Curtis L. Phase II multicenter clinical study of the platelet-activating factor receptor antagonist BB-882 in the treatment of sepsis. Crit Care Med. 2000;28:638–642. doi: 10.1097/00003246-200003000-00006. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.