

Abstract
Ticks are obligate parasites on animals and sometimes humans. They usually suck the blood of the hosts and can carry various infectious diseases as a vector. Otoacariasis is the presence of ticks and mites within the ear canal and relatively common in domestic and wild animals. However, tick infestations of human ear canals are rarely reported in the scientific literature and hardly occur in developed countries. Herein, we report a rare case of otoaracariasis involving Haemaphysalis longicornis . A 9-year-old girl living in a suburb presented with otalgia of left ear for 1 day. Otoscopic examination revealed a huge insect occluding the tympanic membrane. Tick removal and washing of external auditory canal was done successfully. The causative tick was identified as the H. longicornis. To our knowledge, this is the first reported case of human otoacariasis by a H. longicornis in Korea.
Keywords: Ixodidae, Tick bites, Tick infestations
INTRODUCTION
Haemaphysalis species belong to the Family Ixodidae (hard ticks) and consist of approximately 150 species worldwide. They are blood sucking parasites and widely distributed around the world. Haemaphysalis longicornis is the most common species among them. They are found in Australia, New Zealand, several islands and countries in Western Pacific Rims, Korea, Japan, and China which has moderate and humid climates. They dwell in domestic animals such as cattle, horse, sheep, dogs, but also in wild mammals and humans. They are as small as 2 to 3 mm when unfed, but increase in size up to 9×7 mm1,2.
They can be vectors of viral, bacterial and even protozoan infection. They are known to transmit several diseases such as Q-fever, Lyme disease, theileriosis, severe fever with thrombocytopenia syndrome and Russian summer-spring disease. Moreover, they cause systemic hypersensitivity and local foreign body reaction.
Otoacariasis is the infestation of the ear canal with ticks or mites and is well known problems in animals. Human otoacariasis, however, is found rarely in the medical literature. A few cases are reported from under developed areas in Sri Lanka, South Africa, and Nepal3,4. Herein, we report a rare case of H. longicornis tick in the external auditory canal.
CASE REPORT
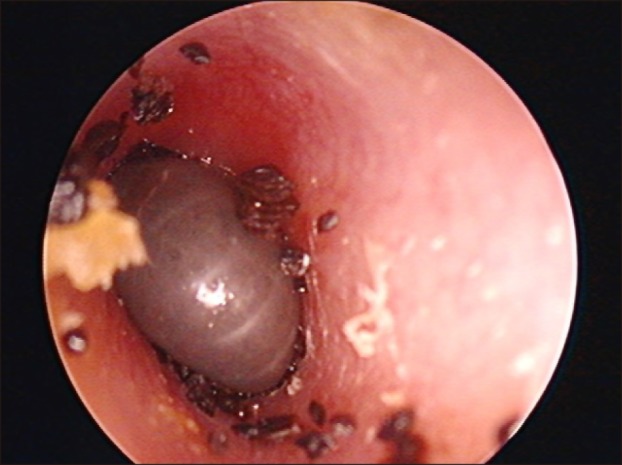
A 9-year-old girl presented with abrupt-onset otalgia of left ear for 1 day at an outpatient department. She had no fever or other systemic symptoms at presentation. A few months ago, she had been treated with otitis media without any complications. Her parents denied of any other medical or trauma history. She had been to Gangwon-do, rural area, for a family trip several days ago. She didn't have any contact with animals during the journey. The laboratory findings, including complete blood count, urine analysis and blood chemistry were within normal limits. On otoscopic examination, a large, shiny deep brown-colored material and multiple small brownish particles were blocking the ear canal so that tympanic membrane could not be seen (Fig. 1). The patient underwent foreign body removal and irrigation of ear canal with normal saline and ethanol was done. The tympanic membrane was intact. The patient did not complain of any pain or hearing impairment after removal of ticks. There were no ticks, eggs or any discharge in the following examinations in one and four weeks.
Fig. 1. Otoscopic examination revealed a large hard tick attached to the tympanic membrane.
The extracted tick was deep brown, 8.5×7.0 mm-sized mass (Fig. 2). It had a dorsal scutum and hypostome in front of the body, which are the characteristics of family Ixodidae. It showed inornate scutum without eyes and festoon in posterior part of the body. The article ii in the pedipalp showed lateral projection beyond the basis capitulum. These features made the tick as general Haemaphysalis . It also had an internal spur on coxa I and a large spur projecting posteriorly on the dorsal side of the article iii in the pedipulp. Y shaped anal groove was surrounding the posterior part of the anus and the dental formula of hypostome was 5/5. According to these features, the tick was identified as female H. longicornis.
Fig. 2. Microscopic findings of extracted tick identified as Haemaphysalis longicornis . (A) Dorsal view, ×8. (B) Ventral view, ×8. (C) Capitulum, ×32. (D) Legs, ×16.

DISCUSSION
H. longicornis is three-host tick and live for 77~123 days. It requires three different hosts at each of the stages (larva, nymph, adult) to complete a life cycle. Female ticks undergo asexual or bisexual reproduction depending on their environment. H. longicornis is the only species in Order Ixodida, which can reproduce in both ways (parthenogenesis and gamogenesis). They usually reproduce asexually in most habitats; however, gamogenesis is relatively common in Korea and Japan. They lay 100~2,000 eggs which hatch into larvae after 27.5~38.6 days. The larvae live within plants until they run into the host where they feed on blood. In about 5 days, they detach from the host and become nymphs. The nymphs and adult ticks follow the same cycle again5.
Ticks accidently infest human during field work or close contact with pets. The most affected sites of human tick bites are skin such as perianal area, groin area, axillae and extremities. They penetrate the skin of the hosts using their capitula and enzymes with local anesthetic and anticoagulant effect. The complete removal of mouth parts embedded into the host is important when detaching the ticks. At times, waiting for several days can be a natural way of treatment since the tick falls off its host into after fully engorged. However, it is not the case when the tick is stuck in the ear canal. Gentle and skillful removal methods are required since complications may occur during extraction. When too much pressure is applied to tick's body, it can raise the risk of tick-borne-disease transmission. Ear drum injuries by inexperienced personnel should be avoided. In our case, the tick was removed from the ear canal under general anesthesia by a microforcep after paralyzed with lidocaine. If lidocaine is not present, glycerin or chloroform can be used alternatively6. After that, irrigation using 70% ethanol and saline was done. Iwasaki et al. introduced stepwise method. Excision of the tick's abdomen and suctioning of body fluid was done first, followed by removal of dead tick after several days without complications7.
According to the study in Sri Lanka, females and children under 10 years were risk groups of human otoacariasis8. Since there are more families with pets in Korea, the chances of close contact with animals are increasing. The most common symptom of the otoacariasis is otalgia, followed by otorrhea, bleeding, and tinnitus9. Facial palsy was also reported in several cases of the intraaural tick10. Other possible complications include transmission of tick borne diseases.
H. longicornis is widely distributed throughout Korea. However, it mostly infests cattle. Human bite by this species is very rare worldwide. Besides, infestations of the ear canal by ticks are much unusual than tick bite. To our knowledge, this is the first case of human otoacariasis by H. longicornis.
Footnotes
CONFLICTS OF INTEREST: The authors have nothing to disclose.
References
- 1.Roh DK, Jang IG, Cho BK, Son SJ, Lee IY, Lee WK. Tick bite by haemaphysalis longicornis Neumann: laboratory observation of the causative tick. Korean J Dermatol. 1999;37:631–636. [Google Scholar]
- 2.Hoogstraal H, Roberts FH, Kohls GM, Tipton VJ. Review of Haemaphysalis (kaiseriana) Longicornis Neumann (resurrected) of Australia, New Zealand, New Caledonia, Fiji, Japan, Korea, and Northeastern China and USSR, and its parthenogenetic and bisexual populations (Ixodoidea, Ixodidae) J Parasitol. 1968;54:1197–1213. [PubMed] [Google Scholar]
- 3.Dilrukshi PR, Yasawardene AD, Amerasinghe PH, Amerasinghe FP. Human otoacariasis: a retrospective study from an area of Sri Lanka. Trans R Soc Trop Med Hyg. 2004;98:489–495. doi: 10.1016/j.trstmh.2003.12.008. [DOI] [PubMed] [Google Scholar]
- 4.Cakabay T, Gokdogan O, Kocyigit M. Human otoacariasis: Demographic and clinical outcomes in patients with ear-canal ticks and a review of literature. J Otol. 2016;11:111–117. doi: 10.1016/j.joto.2016.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Barker SC, Walker AR. Ticks of Australia. The species that infest domestic animals and humans. Zootaxa. 2014;(3816):1–144. doi: 10.11646/zootaxa.3816.1.1. [DOI] [PubMed] [Google Scholar]
- 6.Fegan D, Glennon J. Intra-aural ticks in Nepal. Lancet. 1996;348:1313. doi: 10.1016/S0140-6736(05)65794-7. [DOI] [PubMed] [Google Scholar]
- 7.Iwasaki S, Takebayashi S, Watanabe T. Tick bites in the external auditory canal. Auris Nasus Larynx. 2007;34:375–377. doi: 10.1016/j.anl.2006.09.013. [DOI] [PubMed] [Google Scholar]
- 8.Somayaji KS, Rajeshwari A. Human otoacariasis. Indian J Otolaryngol Head Neck Surg. 2007;59:237–239. doi: 10.1007/s12070-007-0069-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gökdoğan O, Çakabay T, Baran H, Karabulut B, Tasdemir C, Vatansever Z. Otoacariasis: demographic and clinical outcomes of patients with ticks in the ear canal. Braz J Otorhinolaryngol. 2016;82:416–421. doi: 10.1016/j.bjorl.2015.07.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Indudharan R, Dharap AS, Ho TM. Intra-aural tick causing facial palsy. Lancet. 1996;348:613. doi: 10.1016/s0140-6736(05)64827-1. [DOI] [PubMed] [Google Scholar]