

Abstract
Purpose
To determine the associations between patterns of substance use and sexual risk-taking among female adolescents with and without histories of maltreatment.
Methods
Data are from a prospective cohort study examining the impact of maltreatment on subsequent female adolescent sexual health (n = 504). Participants averaged 18.24 (SD = 1.12) years in age, and approximately 63% had substantiated incidences of maltreatment filed with Child Protective Services prior to age 18. The present study used latent class analysis to examine patterns in adolescent substance use, and negative binomial regression models to examine the links between patterns of substance use and sexual risk-taking and to determine whether these associations were moderated by adolescents’ maltreatment status.
Results
Six classes emerged from latent class analysis labeled: abstainers (25% of sample); polysubstance users - early initiators (13%); polysubstance users - late initiators (23%); alcohol and cannabis users - late initiators (9%); alcohol users - late initiators (18%); and tobacco users (12%). Patterns of adolescent polysubstance use were associated with the highest levels of sexual risk-taking, and patterns of late initiated polysubstance use, late initiated alcohol use, and tobacco use were more strongly related to sexual risk-taking for female adolescents with histories of maltreatment.
Conclusion
This study is the first to determine the specific patterns of substance use that are more strongly related to sexual risk-taking for maltreated female adolescents. By doing so, this study demonstrates how a person-centered approach can facilitate our understanding of how to best leverage sexual risk-taking prevention efforts.
Keywords: adolescence, sexual risk-taking, substance use, maltreatment, latent class analysis
Introduction
Substance use poses a serious public health concern for adolescents within the United States [1,2]. Early initiation of substance use and polysubstance use (i.e., concurrent use of two or more substances) during adolescence increase the risk of experiencing a number of negative outcomes, including participating in sexual risk-taking [3–5]. The health consequences associated with sexual risk-taking during adolescence may be most prominent among female adolescents, who have a higher risk of acquiring a STI than their male counterparts when condoms are not used during sex [6]. Adolescent pregnancy is also linked to sexual risk-taking and is a concern for females as it is related to premature birth, poor prenatal care, and educational achievement [7,8]. In an attempt to facilitate the development of more targeted interventions that can assist with preventing such outcomes, researchers employing person-centered methods have uncovered subgroups of adolescents characterized by individual differences in patterns of substance use [9]. Critically, early evidence suggests that these groups diverge in their sexual risk-taking behavior [10,11]. However, research has yet to determine whether or not these relationships vary across etiologically meaningful variables, such as child maltreatment (i.e., experiences of neglect, physical, sexual, and/or emotional abuse). In line with transactional models of maltreatment, evidence indicates that experiences of maltreatment have the potential to interact with risk factors and enhance their effects in non-additive ways [12,13]. Given that maltreatment has been linked to both adolescent substance use [14] and sexual risk-taking [15–17], it follows that the relationships between specific patterns of adolescent substance use and sexual risk-taking may be more pronounced for adolescents who have been maltreated. The present study addresses this hypothesis and uses latent class analysis to determine if specific patterns of substance use are more strongly related to sexual risk-taking for female adolescents with histories of maltreatment.
Substance use and sexual risk-taking
Evidence indicates that earlier initiation [18,19] and use of substances [4,20,21] have the potential to impact adolescents’ sexual health by increasing their risk of participating in sexual risk-taking. Among female adolescents, tobacco use is related to decreased condom use during sex [22,23] and a greater number of sexual partners [5]. Studies have also linked earlier initiation of alcohol to less condom use [18] and earlier initiation of cannabis use to a greater numbers of lifetime sexual partners [19]. While these studies contribute to our understanding of the substance use and sexual risk-taking relationship, evidence indicating that a great deal of heterogeneity exists within adolescent substance use [24] points to a need for person-centered research that considers the links between varying patterns of substance use and sexual risk-taking.
Latent classes of adolescent substance use
A growing area of research uses latent class analysis to address the heterogeneity in adolescent substance use [9]. Compared to variable-centered approaches that attempt to describe relationships between variables across individuals, person-centered methods aim to describe population heterogeneity by identifying homogenous and mutually exclusive subgroups (i.e., classes) that are differentiated by patterns across variables within individuals. This approach is preferred over simple cross-tabulation methods because it is able to account for measurement error in responses to questions and because the items used to model the latent categorical variable may be derived from different domains [25]. Studies using this approach have most often used indicators of substance use types to identify classes of adolescent users, and have most consistently found patterns characterized by: (1) low probabilities of any substance use; (2) alcohol use; (3) concurrent use of alcohol and cannabis use; and (4) concurrent use of alcohol, tobacco, and cannabis use [9].
Only two studies have examined the links between latent classes of adolescent substance use and sexual risk-taking. Bohnert and colleague’s (2014) study of adolescents from urban community health clinics examined correlates of adolescent substance use classes and found that those comprising a class characterized by concurrent alcohol, tobacco, and cannabis use reported the greatest number of sexual partners within the last year, followed by cannabis users, and abstainers [10]. More recently, Swartzendruber and colleagues (2016) study of African American adolescent females found that those engaging in concurrent alcohol and cannabis use were at greater risk of acquiring an STI or unplanned pregnancy than alcohol users or cannabis users [11]. These studies demonstrate the utility of a latent class approach by identifying patterns of adolescent substance use that are associated with the greatest levels of risk for participating in sexual risk-taking. To build upon these efforts, research is now needed that determines for whom these relationships are the most salient.
The case for considering adolescents’ history of maltreatment
Past research underscores the importance of considering adolescents’ history of maltreatment when investigating relationships between maladaptive behaviors. First, maltreatment is linked to substance use [26] and sexual risk-taking [27], and therefore should be considered when investigating the relationship between substance use and sexual risk-taking to avoid confounding results. Second, elevated levels of co-occurring symptomatology exist among maltreated individuals [12], underscoring the importance of considering this at-risk population when investigating the substance use and sexual risk-taking link. Third, rather than potentiating the effects of risk factors in an additive manner, researchers have found complex transactions between maltreatment and risk factors [28]. Given the heterogeneity underlying adolescent substance use, it is possible that maltreatment may interact with varying patterns of substance use in unique and meaningful ways that have implications for the prevention of sexual risk-taking.
The current study
The present study uses latent class analysis to determine the patterns of substance use that are more strongly related to sexual risk-taking for female adolescents with histories of maltreatment. The insight gained from this study will inform more targeted prevention programming for an underserved and high-risk population. Drawing on data from a longitudinal cohort study examining the impact of maltreatment on sexual development, we address the following research questions: What are the patterns of substance use among female adolescents, and can these patterns be distinguished by their sexual risk-taking? Are the associations between patterns of substance use and sexual risk-taking moderated by female adolescents’ maltreatment status?
Methods
The sample was comprised of maltreated (n = 275) and non-maltreated (n = 239) female adolescents between 14 and 17 years of age at study entry. These participants were drawn from the catchment area of a large urban children’s hospital in the Midwest. Specifically, adolescents with substantiated incidences of maltreatment including physical abuse (32%), sexual abuse (47%), or physical neglect (16%) within the previous 12-months were recruited from local Child Protective Services (CPS) agencies. Adolescent females with no prior CPS involvement were recruited from a primary care health center and were matched to at least one maltreated female on age, ethnicity-race, family income, and family composition (single- or two-parent household). Eligible participants were female, fluent in English, had a stable residence for a minimum of 12-months, and had the permission of a legal guardian to participate.
Subsequent to receiving approval by the local Institutional Review Board, caregivers and adolescents attended lab visits to provide informed consent and to complete questionnaires and semi-structured interviews. Data were collected between 2007 and 2012. The retention rate was notably high, 97%. All participants completed annual assessments up to 4 years or until age 19.
Following adolescents’ participation in the study, CPS records were reviewed to determine lifetime CPS involvement for each adolescent. A total of 44 adolescents from the original control condition were identified to have had a substantiated incident of maltreatment prior to age 18, and therefore were included in the final maltreatment condition. Because we were unable to confirm or disconfirm maltreatment for ten participants in the non-maltreated condition, they were not included in the following analyses. Descriptive statistics of the final analytic sample of 504 adolescents included in the current study are presented in Table 1. These adolescents averaged 18.24 (SD = 1.12) years in age at their last assessment. The majority identified as African American (47%) or White/Caucasian (43%), over half resided in a single-parent household (56.7%), and the median family income levels was $20,000–$29,999.
Table 1.
Adolescent descriptive statistics and outcome data at last assessment
| Non-maltreated adolescents (n = 185) |
Maltreated adolescents (n = 319) |
Full sample (n = 504) |
|
|---|---|---|---|
| Average age at last assessment (SD) | 18.22 (1.02) | 18.25 (1.18) | 18.24 (1.12) |
| Ethnic-racial composition | |||
| African American | 44.3% | 49.1% | 47.3% |
| White/Caucasian | 49.2% | 40.3% | 43.5% |
| American Indian or Alaska native | 0% | .6% | .4% |
| Asian or Pacific Islander | 0% | 0% | 0% |
| Latino | .5% | .9% | .8% |
| Biracial | 5.4% | 8.8% | 7.6% |
| Other | .5% | .3% | .4% |
| Median household income | $30,000–$39,999 | $20,000–$29,999 | $20,000–$29,999 |
| Household composition | |||
| One parent household | 48.9% | 61% | 56.7% |
| Two parent household | 49.5% | 37% | 41.6% |
| Other | 1.6% | 2% | 1.7% |
| Average sexual risk-taking (Variance) | 1.64 (3.02) | 2.23 (4.86) | 2.01 (4.26) |
Measures
Maltreatment status
Participants’ histories of maltreatment were assessed using administrative CPS case records. For the current study, maltreatment status was coded “1” if any maltreatment was substantiated prior to age 18 and “0” if no maltreatment had been substantiated. Due to limitations with latent class sizes, we did not run the following analyses by sub-type of maltreatment.
Substance use
Indicators of adolescent substance use were created using items adapted from the Monitoring the Future national survey questionnaires [29]. The use of specific substances were coded “1” if a related item was endorsed and “0” if no item was endorsed. Four indicators of substance use within the year prior to last assessment were created using 1 item assessing alcohol use (“had a drink”), 1 item problematic alcohol use (“got drunk”), 1 item tobacco use (“smoked cigarettes”), and 1 item cannabis use (“used marijuana or hashish”). Participants also responded on a 0 (“never”) to 9 (“12th grade”) scale to questions assessing the first time they had used each of these substances. Four indicators of substance use initiation were created by recoding responses to “0” if the item had never occurred, “1” if participants reported first use between kindergarten and 8th grade, and “2” if participants reported first use between 9th and 12th grade.
Sexual risk-taking
Items from the Sexual Attitudes and Activities Questionnaire [30] were used to measure adolescents sexual risk-taking that had occurred in the past year prior to their final assessment. Items were rated on a 0 (“none, never”) to 5 (“more than 10 partners”) scale. Responses to three items capturing the number of sexual intercourse partners in the past year, the number of partners with whom a one night stand had occurred, and the number of partners with whom sex while under the influence of alcohol or drugs had occurred were summed to create a final sexual risk-taking score (α = .71).
Data analysis plan
Latent class analysis was conducted with Mplus (version 7.4) to examine the structure underlying the 8 categorical indicators of substance use (2 [last year use and initiation] × 4 [alcohol use, problematic alcohol use, tobacco use, and cannabis use]). This involved fitting multiple models with an increasing number of classes until the optimal model for interpretation was identified. Model fit was compared using the Akaike information criterion (AIC), Bayesian information Criterion (BIC), sample size adjusted BIC (SABIC), Lo-Mendell-Rubin Adjusted Likelihood Ratio Test (LMRT), Bootstrap Likelihood Ratio Test (BLRT), and entropy. Lower values for the AIC, BIC, and SABIC are preferred, and indicate an improvement between models in terms of balancing fit and parsimony. The LMRT and BLRT are likelihood ratio tests that, when significant, indicate a model with k number of classes is preferred to a model with k – 1 number of classes. Entropy values range from 0 to 1, where values closer to 1 indicate less classification error [31]. Models that contained classes with less than 5% of the sample were considered inadequate, regardless of the statistical fit of the model. Missing data on the substance use indicators was handled using maximum-likelihood estimation with robust standard errors.
Following identification of the optimal latent class model, we used the modified Bolck-Croon-Hagenaars (BCH) method [32] to estimate the average level of sexual risk-taking across classes and to determine whether these associations varied as a function of adolescents’ maltreatment status. The BCH method uses posterior probabilities to classify individuals to their most likely latent class, and allows for the estimation of outcome models that include weights reflecting measurement error of the substance use latent class variable. Because of sufficient overdispersion in the sexual risk-taking count variable (i.e., variance was non-proportional to the mean), negative binomial regression models were used to estimate the associations between class membership and sexual risk-taking, and to test whether these associations were moderated by adolescents’ maltreatment status. Negative binomial regression uses a canonical link function to log transform the dependent variable, and has been shown to provide more accurate estimates when using overdispered count data [33].
Results
Model selection
Analyses of the 8 substance use items indicated a 6-class solution as the optimally fitting model. As seen in Table 2, a 6-class model had the lowest AIC, BIC, and SABIC values. Even though the LMRT indicated a 3-class solution was optimal, the BLRT indicated a 6-class solution as optimal. Classification certainty was strong across all models, indicated by high entropy values. Solutions with more than 6 classes were explored, but due to issues of sparseness (i.e., not having enough participants in each class) a 6-class model was retained.
Table 2.
Fit criteria for potential latent class models of substance use
| Class Solution | AIC | BIC | SABIC | LMRT | BLRT | Entropy |
|---|---|---|---|---|---|---|
| 1 class | 6766.82 | 6817.49 | 6779.40 | N/A | N/A | 1.00 |
| 2 class | 5458.69 | 5564.25 | 5484.90 | p < .001 | p < .001 | .89 |
| 3 class | 5169.07 | 5329.53 | 5208.92 | p < .001 | p < .001 | .89 |
| 4 class | 4974.35 | 5189.70 | 5027.82 | p < .05 | p < .001 | .94 |
| 5 class | 4874.76 | 5145.00 | 4941.86 | p = .26 | p < .001 | .92 |
| 6 class | 4787.10 | 5112.24 | 4867.83 | p = .62 | p < .001 | .93 |
AIC = Akaike Information Criterion; BIC = Bayesian Information Criterion; SABIC = Sample Size Adjusted BIC; LMRT = Lo-Mendell-Rubin Adjusted LRT; BLRT = Bootstrap Likelihood Ratio Test; N/A = Not applicable; Bold font indicates selected model.
Description of the six-class solution
Item-response probabilities used to describe the likelihood of particular responses to the substance use indicators and to label each class are presented in Table 3. Class 1 labeled “abstainers” (25% of the sample), is comprised of adolescents who largely abstained from using any substances. Class 2 (13%) labeled “polysubstance users – early initiators”, contains adolescents with high probabilities of reporting use of all substances within the last year and early initiation of all substances. Contrastingly, Class 3 (23%) labeled “polysubstance users – late initiators”, is comprised of adolescents with high probabilities of reporting use of all substances within the last year, but late initiation of all substances. Class 4 (9%) labeled “alcohol and cannabis users – late initiators”, contains adolescents who have high probabilities of endorsing last year alcohol and cannabis use and late initiation of alcohol and cannabis use. Class 5 (18%) labeled “alcohol users – late initiators”, is comprised of adolescents who had high probabilities of endorsing last year alcohol use and late initiation of alcohol use and problematic alcohol use. Lastly, Class 6 contains adolescents with high probabilities of endorsing tobacco use within the last year and was labeled “tobacco users”.
Table 3.
Parameter estimates for the six class model of adolescent substance use (n = 504)
| Overall sample | “Abstainers” | “Polysubstance users – early initiators” | “Polysubstance users – late initiators” | “Alcohol and cannabis users – late initiators” | “Alcohol users – late initiators” | “Tobacco users” | |
|---|---|---|---|---|---|---|---|
|
| |||||||
| Latent class membership probabilities
|
|||||||
| .25 | .13 | .23 | .09 | .18 | .12 | ||
| Indicators | Item-response probabilities | ||||||
|
| |||||||
| Drink last yr. | .62 | .02 | .95 | .92 | 1.00 | .90 | .13 |
| Drunk last yr. | .28 | .01 | .68 | .51 | .28 | .23 | .02 |
| Tobacco last yr. | .43 | .00 | .90 | .82 | .02 | .24 | .65 |
| Cannabis last yr. | .42 | .00 | .76 | .80 | .89 | .00 | .42 |
| First drink | |||||||
| Never | .36 | .95 | .01 | .02 | .02 | .04 | .96 |
| k–8th grade | .21 | .00 | .99 | .14 | .26 | .11 | .01 |
| 9th–12th grade | .43 | .05 | .00 | .84 | .72 | .85 | .03 |
| First drunk | |||||||
| Never | .48 | 1.00 | .03 | .09 | .20 | .38 | .98 |
| k–8th grade | .12 | .00 | .75 | .00 | .04 | .05 | .02 |
| 9th–12th grade | .40 | .00 | .22 | .91 | .76 | .57 | .00 |
| First tobacco | |||||||
| Never | .50 | .99 | .00 | .00 | .93 | .68 | .37 |
| k–8th grade | .26 | .01 | .86 | .39 | .07 | .11 | .25 |
| 9th–12th grade | .24 | .00 | .14 | .61 | .00 | .21 | .38 |
| First cannabis | |||||||
| Never | .50 | .96 | .07 | .02 | .02 | 1.00 | .57 |
| k–8th grade | .20 | .00 | .78 | .25 | .25 | .00 | .09 |
| 9th–12th grade | .30 | .04 | .15 | .73 | .73 | .00 | .34 |
Item-response probabilities indicate proportions of individuals in a particular class endorsing a given item. Latent class membership probabilities indicate the proportion of participants in each class. To assist with interpretation, probabilities ≥ .50 are bolded.
Sexual risk-taking as a function of class membership and maltreatment status
Following the identification of the optimally fitting latent class model, a “main effects only” model was tested examining the associations between substance use classes and sexual risk-taking. Parameter estimates representing the slopes of the relationships between substance use classes and sexual risk-taking are presented in Table 4, using abstainers as the reference. Analyses revealed main effects for the polysubstance users – early initiators (M = 3.02), polysubstance users – late initiators (M = 3.07), alcohol and cannabis users – late initiators (M = 2.20), and tobacco users (M = 1.95), who all reported significantly more sexual risk-taking within the last year on average than abstainers (M = .97). Alcohol users – late initiators also reported more sexual risk-taking than abstainers (M = 1.28), although this difference was not statistically significant (see Table 4).
Table 4.
Negative binomial regression parameter estimates representing associations between substance use class membership and sexual risk-taking among female adolescents with and without histories of maltreatment, using abstainers (class 1) as reference
| Main Effects Only
|
Main Effects + Interactions
|
|||||
|---|---|---|---|---|---|---|
| EXP(B) | SE(B) | 95% CI | EXP(B) | SE(B) | 95% CI | |
| Polysubstance users – early initiators | 3.11*** | .18 | [2.33, 4.15] | 2.56*** | .24 | [1.72, 3.82] |
| Polysubstance users – late initiators | 3.16*** | .16 | [2.42, 4.13] | 2.03** | .24 | [1.36, 3.04] |
| Alcohol and cannabis users – late initiators | 2.26*** | .19 | [1.65, 3.11] | 1.71* | .27 | [1.10, 2.64] |
| Alcohol users – late initiators | 1.31 | .20 | [.95, 1.81] | .85 | .27 | [.54, 1.32] |
| Tobacco users | 2.01** | .21 | [1.42, 2.85] | .76 | .55 | [.31, 1.89] |
| Polysubstance users – early initiators X maltreatment | 1.50 | .34 | [.87, 2.61] | |||
| Polysubstance users – late initiators X maltreatment | 2.10* | .33 | [1.23, 3.59] | |||
| Alcohol and cannabis users – late initiators X maltreatment | 1.71 | .38 | [.92, 3.16] | |||
| Alcohol users – late initiators X maltreatment | 2.31* | .38 | [1.23, 4.34] | |||
| Tobacco users X maltreatment | 4.01* | .60 | [1.48, 10.85] | |||
SE = standard error; CI = confidence interval.
p < .05,
p < .01,
p < .001
Next, we added interaction terms for substance use class membership by maltreatment status, which significantly improved the overall fit of the model; that is, maltreatment status moderated the associations between substance use class membership and sexual risk-taking (χ2[6] = 21.14, p < .01). As seen in Table 4, associations for polysubstance users – late initiators, alcohol users – late initiators, and tobacco users were moderated by maltreatment status; that is, the slopes representing the relationships between membership in these classes and sexual risk-taking differed significantly for adolescents with and without histories of maltreatment. As seen in Figure 1, adolescent polysubstance users – late initiators, alcohol users – late initiators, and tobacco users with histories of maltreatment reported significantly higher levels of sexual risk-taking than their non-maltreated counterparts.
Figure 1.
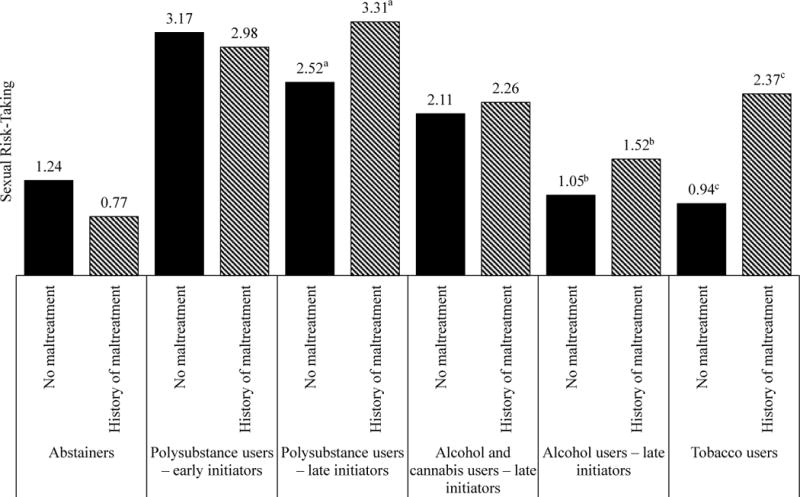
Estimated mean count of sexual risk-taking over the last year conditioned on class membership and maltreatment status. Matching subscripts denote significant differences in sexual risk-taking.
Discussion
This study contributes to a growing body of evidence indicating that a great deal of heterogeneity exists within adolescent substance use [9,34,35]. Using latent class analysis, six classes of female adolescents were identified based on response patterns to indicators of substance use spanning dimensions of type and initiation. Classes were labeled abstainers, polysubstance users – early initiators, polysubstance users – late initiators, alcohol and cannabis users – late initiators, alcohol users – late initiators, and tobacco users, reflecting the patterns of substance use that best characterized each group. These classes align with past research on latent classes of adolescent substance use [9–11] and build upon these studies by demonstrating how an over looked yet important dimension of substance use, initiation, can be used to model latent classes of adolescent substance use. Moreover, these findings indicate that substance use initiation may be a differentiating factor within groups of polysubstance users, suggesting that predictors and outcomes related to class membership should be further investigated in these two groups.
Findings also draw attention to the intersection of substance use and sexual risk-taking, and suggest a need for targeted intervention that considers both of these related behaviors together. Consistent with prior evidence that more severe patterns of adolescent substance use are more strongly related to sexual risk-taking [10,11], both early and late initiated polysubstance use were associated with the highest levels of sexual risk-taking on average. These findings suggest that more severe patterns of female adolescent substance use may serve as a marker for additional sexual health needs, and that sexual risk-taking prevention efforts targeting female adolescent substance users may have significant implications for addressing sexual health disparities within this population. However, as demonstrated by our findings, there is variability in the association between substance use and sexual risk-taking that interventions should consider when determining which behaviors to target.
In addition to targeting more severe patterns of substance use, our findings suggest a need for sexual risk-taking prevention efforts to be trauma-informed. Specifically, we found that late initiated polysubstance use, late initiated alcohol use, and tobacco use are more strongly related to sexual risk-taking for female adolescents with histories of maltreatment. Notably, the moderating effect of maltreatment status on the link between tobacco use and sexual risk-taking was especially strong. By providing evidence that female adolescent tobacco users are at inordinate risk for participating in sexual risk-taking when a history of maltreatment is present, our study extends prior evidence supporting a positive relationship between tobacco use and sexual risk-taking among female adolescents [5,22,23], indicates a need for further research into tobacco related sexual health disparities among female adolescents who have been maltreated, and draws attention to an opportunity for targeting maltreated female adolescent tobacco users in our sexual risk-taking prevention efforts.
Our findings also suggest that timing may matter in understanding the relationships between substance use and sexual risk-taking among maltreated female adolescents. Maltreatment status was a significant moderator of the late initiated polysubstance use and sexual risk-taking link, but did not moderate the association between early initiated polysubstance use and sexual risk-taking. We suspect these findings may have been influenced by the timing of maltreatment experienced by participants in this particular study. Studies have shown that maltreatment increases the risk of adolescent substance use when it occurs across childhood and adolescence or in adolescence alone [36,37]. Thus, the initial recruitment of adolescents with substantiated incidences of maltreatment within the previous 12-months at baseline may explain why a significant interaction term was obtained for late initiated and not early initiated polysubstance use. This would suggest that maltreatment occurring in adolescence may serve as a risk marker to distinguish early initiated polysubstance use from late initiated polysubstance use.
Limitations and Future Directions
Several limitations should be considered when interpreting our findings. First, we are limited in our generalizability of findings, and additional research will be needed to determine if these patterns and associations are replicated among male adolescents. Second, only victims with substantiated cases were included in the maltreatment condition, which may influence our findings and limit generalizability. Third, even though it is important to understand the associations between patterns of substance use and sexual risk-taking, our decision to examine their concurrent associations limits the ability to conclude a casual inference. If we are to truly understand these associations, longitudinal person-centered research will be needed to determine the role patterns of substance use play in the development and maintenance of sexual risk-taking over time. Lastly, person-centered research should consider the role other dimensions of maltreatment (e.g., severity, timing) and substance use (e.g., dependency) have on this complex relationship.
Implications for Practice
Effective strategies to reduce female adolescents’ sexual risk-taking have the potential to improve overall public health by decreasing rates of STIs and unwanted pregnancies within a high-risk population. By demonstrating strong relationships between patterns of substance use and sexual risk-taking, our findings contribute to a growing body of evidence suggesting that the primary prevention of substance use may be an effective strategy for promoting sexual health among female adolescents [3,10,11]. Even though these relationships were particularly robust across female adolescents, our findings also point to the need for secondary prevention of polysubstance use, alcohol use, and tobacco use for maltreated female adolescents that addresses sexual risk-taking. Despite evidence that interventions can be effective when targeting more than one risk behavior [38] and that substance use and sexual risk-taking are related [22], few interventions explicitly target this intersection [39]. More research is therefore needed to identify factors that explain the relationships between polysubstance use, alcohol use, and tobacco use among maltreated female adolescents’ to fully inform the development of more targeted prevention strategies for this at-risk population.
Conclusion
The present study is one of the first to determine the specific patterns of substance use that are more strongly related to sexual risk-taking for maltreated female adolescents. By doing so, we demonstrate how a person-centered approach can facilitate our understanding of how to best leverage sexual risk-taking prevention efforts. We conclude that by considering within-person differences in adolescent substance use researchers can begin to inform the development of more targeted prevention strategies for high-risk populations.
Implications and Contributions.
This study addresses a critical gap in our understanding of substance use and sexual risk-taking among female adolescents. Findings extend past evidence linking patterns of substance use to sexual risk-taking by identifying specific patterns of use that are more strongly related to sexual risk-taking for maltreated female adolescents.
Acknowledgments
This research was supported in part by grants T32DA017629 and P50DA039898 from the National Institute on Drug Abuse (NIDA), R01HD052533 from the National Institute for Child Health and Human Development, and 5UL1TR001425-02 from the National Center for Advancing Translational Sciences.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Peter M. Rivera, Department of Marriage and Family Therapy, Seattle Pacific University
Bethany C. Bray, The Methodology Center, The Pennsylvania State University
Kate Guastaferro, The Methodology Center, The Pennsylvania State University.
Kari Kugler, Department of Biobehavioral Health, The Pennsylvania State University.
Jennie G. Noll, Department of Human Developmental and Family Studies, The Pennsylvania State University University of Cincinnati College of Medicine, Cincinnati Children’s Hospital Medical center
References
- 1.Wagner FA, Anthony JC. From first drug use to drug dependence: Developmental periods of risk for dependence upon marijuana, cocaine, and alcohol. Neuropsychopharmacology. 2002;26:479–88. doi: 10.1016/S0893-133X(01)00367-0. [DOI] [PubMed] [Google Scholar]
- 2.Center for Behavioral Health Statistics and Quality. 2015 National Survey on Drug Use and Health : Detailed tables prevalence estimates. Rockville: 2016. [Google Scholar]
- 3.Connell CM, Gilreath TD, Hansen NB. A multiprocess latent class analysis of the co-occurrence of substance use and sexual risk behavior among adolescents. J Stud Alcohol Drugs. 2009;70:943–51. doi: 10.15288/jsad.2009.70.943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Guo J, Chung I-J, Hill KG, et al. Developmental relationships between adolescent substance use and risky sexual behavior in young adulthood. J Adolesc Heal. 2002;31:354–62. doi: 10.1016/s1054-139x(02)00402-0. [DOI] [PubMed] [Google Scholar]
- 5.Somers CL, Day A, Decker L, et al. Adolescent girls in out-of-home care: Associations between substance use and sexual risk behavior. J Child Adolesc Subst Abuse. 2016;25:409–16. [Google Scholar]
- 6.Machado JR, Vinícius M, Cavellani CL, et al. Mucosal Immunity in the Female Genital Tract. HIV/AIDS. 2014:2014. [Google Scholar]
- 7.Kearney MS, Levine PB. Why is the Teen Birth Rate in the United States So High and Why Does It Matter? NBER Work Pap Ser. 2012;26:141–66. doi: 10.1257/jep.26.2.141. [DOI] [PubMed] [Google Scholar]
- 8.Hofferth SL, Reid L, Mott FL. The effects of early childbearing on schooling over time. Fam Plann Perspect. 2014;33:259–67. [PubMed] [Google Scholar]
- 9.Tomczyk S, Isensee B, Hanewinkel R. Latent classes of polysubstance use among adolescents-a systematic review. Drug Alcohol Depend. 2016;160:12–29. doi: 10.1016/j.drugalcdep.2015.11.035. [DOI] [PubMed] [Google Scholar]
- 10.Bohnert KM, Walton MA, Resko S, et al. Latent class analysis of substance use among adolescents presenting to urban primary care clinics. Am J Drug Alcohol Abuse. 2014;40:44–50. doi: 10.3109/00952990.2013.844821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Swartzendruber A, Sales JM, Brown JL, et al. Comparison of Substance Use Typologies as Predictors of Sexual Risk Outcomes in African American Adolescent Females. Arch Sex Behav. 2016;45:63–72. doi: 10.1007/s10508-015-0518-0. [DOI] [PubMed] [Google Scholar]
- 12.Cicchetti D, Toth S. Child maltreatment. Annu Rev Clin Psychol. 2005;1:409–38. doi: 10.1146/annurev.clinpsy.1.102803.144029. [DOI] [PubMed] [Google Scholar]
- 13.Cicchetti D. Annual Research Review: Resilient functioning in maltreated children: Past, present, and future perspectives. J Child Psychol Psychiatry. 2014;54:402–22. doi: 10.1111/j.1469-7610.2012.02608.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Norman RE, Byambaa M, De R, et al. The Long-Term Health Consequences of Child Physical Abuse, Emotional Abuse, and Neglect: A Systematic Review and Meta-Analysis. PLoS Med. 2012;9 doi: 10.1371/journal.pmed.1001349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Noll JG, Shenk CE. Teen Birth Rates in Sexually Abused and Neglected Females. Pediatrics. 2013;131:e1181–7. doi: 10.1542/peds.2012-3072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Noll JG, Haralson KJ, Butler EM, et al. Childhood maltreatment, psychological dysregulation, and risky sexual behaviors in female adolescents. J Pediatr Psychol. 2011;36:743–52. doi: 10.1093/jpepsy/jsr003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rivera PM, Gonzales-Backen MA, Yedlin J, et al. Family Violence Exposure and Sexual Risk-Taking Among Latino Emerging Adults: The Role of Posttraumatic Stress Symptomology and Acculturative Stress. J Fam Violence. 2015;30:967–76. doi: 10.1007/s10896-015-9735-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Santelli JS, Robin L, Brener ND, et al. Timing of alcohol and other drug use and sexual risk behaviors among unmarried adolescents and young adults. Fam Plann Perspect. 2001;33:200–5. [PubMed] [Google Scholar]
- 19.Shrier LA, Emans SJ, Woods ER, et al. The association of sexual risk behaviors and problem drug behaviors in high school students. J Adolesc Health. 1997;20:377–83. doi: 10.1016/S1054-139X(96)00180-2. [DOI] [PubMed] [Google Scholar]
- 20.Sussman S. The Relations of Cigarette Smoking with Risky Sexual Behavior among Teens. Sex Addict Compulsivity. 2005;12:181–99. [Google Scholar]
- 21.Duncan SC, Strycker LA, Duncan TE. Exploring associations in developmental trends of adolescent substance use and risky sexual behavior in a high-risk population. J Behav Med. 1999;22:21–34. doi: 10.1023/a:1018795417956. [DOI] [PubMed] [Google Scholar]
- 22.Zhao Y, Kim H, Peltzer J. Relationships Among Substance Use, Multiple Sexual Partners, and Condomless Sex: Differences Between Male and Female U.S. High School Adolescents. J Sch Nurs. 2016:1059840516635712. doi: 10.1177/1059840516635712. [DOI] [PubMed] [Google Scholar]
- 23.Camenga DR, Klein JD, Roy J. The Changing Risk Profile of the American Adolescent Smoker: Implications for Prevention Programs and Tobacco Interventions. J Adolesc Heal. 2006;39 doi: 10.1016/j.jadohealth.2005.10.014. [DOI] [PubMed] [Google Scholar]
- 24.Johnston LD, Malley PMO, Miech RA, et al. Monitoring the Future national survey results on drug use: 1975–2015. Overview, key findings on adolescent drug use. 2015 [Google Scholar]
- 25.Collins LM, Lanza ST. Latent class and latent transition analysis: With applications in the social, behavioral, and health sciences. John Wiley & Sons; 2010. [Google Scholar]
- 26.Tonmyr L, Thornton T, Draca J, et al. A Review of Childhood Maltreatment and Adolescent Substance Use Relationship. Curr Psychiatry Rev. 2010;6:223–34. [Google Scholar]
- 27.Noll JG, Shenk CE, Putnam KT. Childhood sexual abuse and adolescent pregnancy: A meta-analytic update. J Pediatr Psychol. 2009;34:366–78. doi: 10.1093/jpepsy/jsn098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kaufman J, Yang B-Z, Douglas-Palumberi H, et al. Social supports and serotonin transporter gene moderate depression in maltreated children. Proc Natl Acad Sci. 2004;101:17316–21. doi: 10.1073/pnas.0404376101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Johnston LD, O’Malley PM, Bachman JG, et al. Monitoring the Future: National Survey Results on Drug Use, 1975–2005. Volume 1: Secondary School Students, 2005. (NIH Publication No. 06-5883).Natl Inst Drug Abus. 2005;I:1975–2005. [Google Scholar]
- 30.Noll JG, Trickett PK, Putnam FW. A Prospective Investigation of the Impact of Childhood Sexual Abuse on the Development of Sexuality. 2003;71:575–86. doi: 10.1037/0022-006x.71.3.575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Roesch SC, Villodas M, Villodas F. Latent class/profile analysis in maltreatment research: A commentary on Nooner et al. Pears et al. and looking beyond. Child Abus Negl. 2010;34:155–60. doi: 10.1016/j.chiabu.2010.01.003. [DOI] [PubMed] [Google Scholar]
- 32.Bakk Z, Vermunt JK. Robustness of Stepwise Latent Class Modeling With Continuous Distal Outcomes. Struct Equ Model A Multidiscip J. 2016;23:20–31. [Google Scholar]
- 33.Coxe S, West SG, Aiken LS. The Analysis of Count Data: A Gentle Introduction to Poisson Regression and Its Alternatives. J Pers Assess. 2009;91:121–36. doi: 10.1080/00223890802634175. [DOI] [PubMed] [Google Scholar]
- 34.Conway KP, Vullo GC, Nichter B, et al. Prevalence and patterns of polysubstance use in a nationally representative sample of 10th Graders in the United States. J Adolesc Heal. 2013;52:716–23. doi: 10.1016/j.jadohealth.2012.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Connor JP, Gullo MJ, White A, et al. Polysubstance use: diagnostic challenges, patterns of use and health. Curr Opin Psychiatry. 2014;27:269–75. doi: 10.1097/YCO.0000000000000069. [DOI] [PubMed] [Google Scholar]
- 36.Thornberry TP, Ireland TO, Smith CA. The importance of timing: the varying impact of childhood and adolescent maltreatment on multiple problem outcomes. Dev Psychopathol. 2001;13:957–79. [PubMed] [Google Scholar]
- 37.Ireland TO, Smith CA, Thornberry TP. Developmental Issues in the Impact of Child Maltreatment on Later Delinquency and Drug Use. Criminology. 2002;40:359–99. [Google Scholar]
- 38.Hale DR, Fitzgerald-Yau N, Viner RM. A systematic review of effective interventions for reducing multiple health risk behaviors in adolescence. Am J Public Health. 2014;104:19–41. doi: 10.2105/AJPH.2014.301874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Freeman RC. Toward Development of Enhanced Preventive Interventions for HIV Sexual Risk among Alcohol-Using Populations: Confronting the ???Mere Pause from Thinking??? AIDS Behav. 2016;20:1–18. doi: 10.1007/s10461-015-1179-7. [DOI] [PubMed] [Google Scholar]