

Abstract
Introduction: Rural populations, particularly in Africa, suffer worse health outcomes from poor health services access. Community health workers (CHWs) effectively improve health outcomes, but the best means for CHWs reaching rural populations is unknown. Since Zambia is predominantly Christian, this study explored the use of CHWs through churches as an existing community structure for promoting preventive health behaviors, specifically rotavirus vaccine uptake. Methods: A noncontrolled cross-sectional study of 32 churches receiving a packaged intervention of diarrhea prevention and treatment messaging was conducted with repeated time points of data collection over 13 months (2013-2014) in the Kafue District of Zambia. Two churches were selected for each of the 17 catchment areas, and CHWs were identified and trained in the intervention of promoting 4 key messages related to diarrhea prevention and treatment: hand washing with soap, exclusive breast-feeding, rotavirus vaccination, and treating diarrhea with oral rehydration solution and zinc. The intervention was conducted within existing church’s women’s groups, and data was collected on attendance and the distribution of Rota Cards for tracking rotavirus immunizations. Results: Nineteen (59%) churches completed the study, and CHWs delivered health messages at a total of 890 women’s group meetings. The overall reach of the intervention was to 37.0% of church-attending women, and the efficacy was 67.7% (317 of 468 Rota Cards collected at health centers). Discussion: Implementing community health programs is often expensive and unsustainable, but the reach and efficacy levels achieved through existing structures like churches are encouraging in resource-constrained countries. Churches can be effective channels for delivering health prevention strategies to often difficult-to-reach rural populations. Further research is needed to investigate the impact of the intervention on health outcomes.
Keywords: rural health, rotavirus, vaccination, community health, church, diarrhea, Zambia, global health
Introduction
Rural populations worldwide have less health care access and worse health outcomes than urban populations, with rural Africa suffering most from these disparities.1 Sixty percent of Zambia’s population lives in rural areas, which have worse maternal and infant mortality rates than urban areas partly due to Zambia’s geography, climate, and economy—all of which prevent health care from reaching rural populations.1-4 The rural population of Africa is expected to continue growing for the next 20 years, and unequal distribution of health care resources in Zambia and across Africa needs to be addressed.1,2
Specifically, rural Zambians have less access to safe water, fewer use improved drinking water sources, and sanitation facilities are often absent.4 All these contribute to an environment of increased diarrhea from unsafe drinking water and poor sanitation. Diarrhea is the third leading cause of child mortality in Zambia, leading to an estimated 15 000 deaths per year, a third of which are due to rotavirus infection.5
Rotavirus is the most common cause of severe acute gastroenteritis in infants and young children globally, leading to 500 000 deaths per year and 5% of under-5 children’s deaths.6-8 Impoverished rural households are at highest risk for child mortality.3 In an effort to curb this risk, rotavirus vaccines with clinical efficacy and safety have been introduced in 19 countries in Africa in the past 3 years, including in Zambia.6,7,9
Community health workers (CHWs) are trained community members who are recognized and supported by the health system.10 They are effective means for promoting health messages and improving immunization rates, but more research is needed to assess their effectiveness in delivering prevention information, particularly in sub-Saharan Africa.11-13 Eighty-seven percent of Zambia is Christian, and church is a large part of rural Zambian culture, yet the role of CHWs in church structures is understudied.14 One randomized controlled trial in North Carolina attempted to evaluate the role of CHWs in rural African American churches, but it was of poor quality and was underpowered.15,16 Churches are a valuable existing structure for CHWs to tap into as a means of spreading prevention messages, specifically regarding diarrheal disease and rotavirus vaccination.17-19
In conjunction with the Centre for Infectious Disease Research in Zambia’s (CIDRZ) efforts to pilot the national rollout of rotavirus vaccination in Zambia, a strategy was developed for CHWs to deliver health messages regarding diarrhea and rotavirus vaccination within women’s groups at Christian churches in a rural district of Zambia. While previous work has been done in African American churches, this approach was novel as it was set in rural Zambia and could potentially influence CHW policies and practices in the future. This study sought to evaluate the reach and efficacy of this novel community health outreach strategy within a rural community.
Methods
Ethics Statement
This work was part of the Ministry of Health’s approved implementation program. No specific ethical review was sought. Based on the government’s approval of the project, a waiver was obtained from the University of Zambia Bioethics Committee.
Study Setting
The study was conducted in Kafue District, a rural district in Lusaka Province. The total population is 242 754, of which 121 433 are female.20 Nearly the entire population is Christian and attends a variety of local churches.
Study Participants
All women with children younger than 5 years belonging to women’s groups in selected churches in Kafue District were targeted for this study. Two Christian churches were selected by convenience sampling in each of the 17 catchment areas, defined as the communities surrounding a health facility. Christian churches were eligible for selection if they had (a) the flexibility to hold health education sessions, (b) a CHW as a member their congregation, and (c) the ability to hold a women’s group meeting as part of a church activity.
Study Design
This study was a community-based, single-armed, open-label design to promote diarrhea prevention and treatment via women’s church groups. The 4 key messages were exclusive breast-feeding, hand washing with soap, rotavirus vaccination, and diarrhea treatment with oral rehydration solution and zinc. In the interest of sustainability, only churches with existing women’s groups were sought for participation.
Intervention
The intervention was delivered weekly, with each of the four health messages covered in a month (1 per week) and cycled monthly. A training manual and flip chart outlined the 4 key messages. Materials were designed to guide users’ communication with women’s groups and approved by the Ministry of Community Development Mother and Child Health. Rotavirus immunization card invitations (Rota Cards) were handed to mothers with infants below the age of 15 weeks (Figure 1). Mothers were encouraged to present the Rota Card to a health care provider when their infants were immunized against rotavirus. CHWs, community development assistants (CDAs), and environmental health technicians (EHTs) were trained on the field manual and flip chart. Trained CHWs facilitated health-related workshops within church’s women’s groups and documented all relevant activities. EHTs/CDAs supervised the CHWs and collected reports monthly. The project team conducted quarterly supportive supervision visits to mentor CHWs and discuss progress.
Figure 1.
Sample Rota Card.
Data Collection
A data collection tool was developed to capture weekly health education activities. Variables included the number of women attending church, the number of women attending women’s groups, the number of rotavirus vaccine-eligible infants (<15 weeks), and the number of Rota Cards distributed. When infants presented for immunization at the health facility, the provider completed and retained the Rota Card in a designated box placed at the health center, which the EHT/CDA collected monthly.
Data Analysis
The primary outcomes were reach and efficacy. Reach was defined as the extent to which the target population received the health messages. It was calculated as the average number of women attending the group sessions divided by the average number of women in the church over the period of intervention, expressed as a percentage. Efficacy was defined as the extent to which the health messages changed health behavior through the immunization of eligible babies against rotavirus. It was calculated as the total number of cards collected at the health center divided by the total number of Rota Cards distributed to women, expressed as a percentage. The analysis was disaggregated by church, and churches were included if they completed a minimum of 4 months of intervention because of how incomplete reported data was for churches with fewer than 4 months. Analysis was performed using SAS 9.3 and Microsoft Excel.
Results
Sample
Thirty-two churches were recruited and 2 declined to be part of the program (Figure 2). Nineteen churches completed at least 4 months of intervention and were included in the analysis, ranging from 6 to 13 months. A total of 64 CHWs, 15 CDAs, and 11 EHTs were recruited and trained. The project team conducted four mentoring visits over the course of the year. The characteristics of the final sample of 19 churches are outlined in Table 1.
Figure 2.
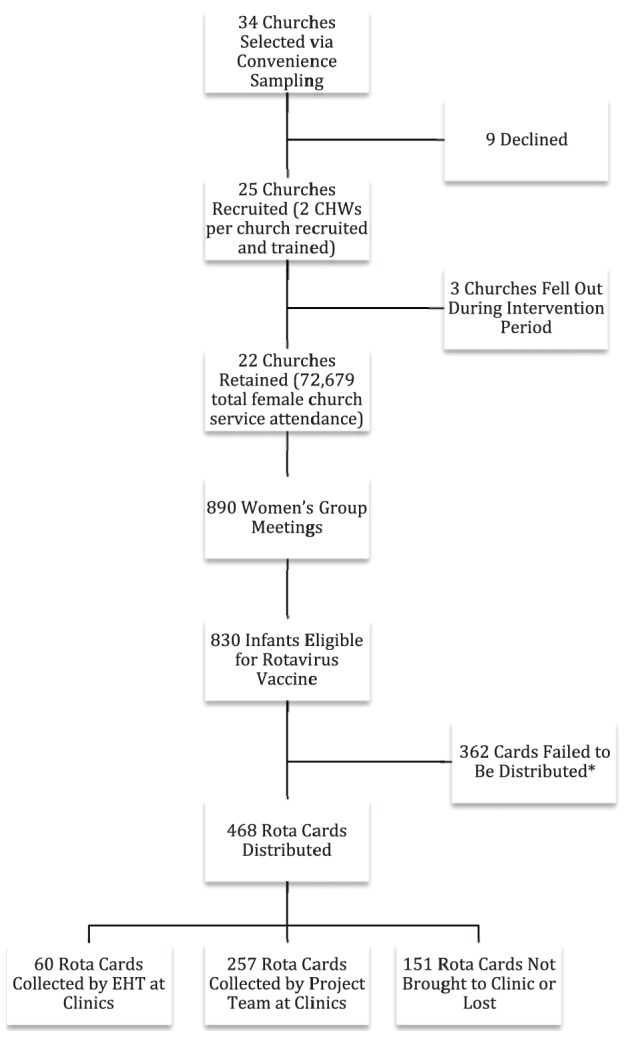
Overall flow of churches, participants, and Rota Cards.
*Almost all of this discrepancy can be explained by the likely inaccurate number of eligible babies reported by the Railway–UCZ church (357 eligible babies, 4 cards distributed). If excluded from analysis, only 9 cards failed to be distributed overall.
Table 1.
Characteristics of Included Churches.
| Catchment Area | Church | Months of Intervention | Total Women’s Groups | Average No. of Women Attending Church | Average No. of Women at Groups | Total EHT Visits | Total Eligible Babies | Total Cards Distributed | Total Cards at Clinic |
|---|---|---|---|---|---|---|---|---|---|
| Chiawa | St. Martin Catholic Church | 8 | 28 | 39.4 | 35.4 | 15 | 16 | 3 | 10 |
| Chikupi | Holy Spirit Roman Catholic | 13 | 100 | 46.3 | 25.5 | 27 | 64 | 60 | 12 |
| SDA | 9 | 48 | 64.8 | 39.0 | 22 | 52 | 42 | 9 | |
| Chinyanya | SDA | 11 | 115 | 44.2 | 17.7 | 15 | 61 | 46 | 0 |
| Chipapa | SDA | 6 | 15 | 49.0 | 20.6 | 5 | 12 | 13 | 16 |
| Chisankane | SDA | 13 | 40 | 63.3 | 40.5 | 3 | 83 | 60 | 13 |
| Kafue Estate | Upper Room–Pentecostal | 7 | 24 | 93.3 | 28.4 | 14 | 5 | 5 | 4 |
| ZAOGA–Pentecostal | 7 | 22 | 51.4 | 20.4 | 4 | 2 | 8 | 16 | |
| Kafue Mission | Grace Ministries | 13 | 62 | 46.0 | 14.8 | 15 | 3 | 1 | 18 |
| UCZ | 11 | 52 | 83.6 | 17.6 | 13 | 1 | 4 | 10 | |
| Kambale | SDA | 12 | 44 | 57.2 | 43.5 | 18 | 25 | 15 | 20 |
| St. Joseph Catholic Church | 8 | 30 | 137.8 | 58 | 9 | 8 | 31 | 10 | |
| Kazimva | UCZ | 13 | 55 | 80.3 | 10.3 | 12 | 14 | 15 | 13 |
| Mt. Makulu | UCZ | 13 | 54 | 103.2 | 24.9 | 39 | 32 | 104 | 133 |
| Mwembweshi | St. Luke Catholic Church | 7 | 25 | 66.3 | 20.8 | 8 | 24 | 12 | 10 |
| Railway | St. John Catholic Church | 7 | 52 | 534.1 | 78.9 | 2 | 33 | 18 | 0 |
| UCZ | 11 | 44 | 169.0 | 127.9 | 3 | 357 | 4 | 0 | |
| Shimabala | St. Paul’s Catholic Church | 11 | 52 | 140.4 | 63.8 | 17 | 15 | 17 | 19 |
| UCZ | 8 | 28 | 28.8 | 14.4 | 8 | 23 | 10 | 4 | |
| Total | 188 | 890 | 1898.4 | 702.4 | 251 | 830 | 468 | 317 |
Abbreviation: EHT, environmental health technician.
Summary of Data
The 19 churches averaged 99.9 women per church service (SD 111.8, interquartile range [IQR] 50.6) and 37.0 women per group (SD 28.7, IQR 23.0). When averaging the sample of 19 churches, the average reach was 44.6% (95% CI 35.6% to 53.5%) and the average efficacy was 182.4% (95% CI 134.4% to 350.3%). The project’s overall reach was 37.0% and efficacy was 67.7% across the 19 included churches. When evaluating all 25 churches that reported data, the overall reach was 35.0% and efficacy was 65.0%.
Discussion
The study’s overall reach and efficacy rates demonstrate that churches in developing countries can be effective conduits for delivering preventive care messages to rural populations, specifically immunization promotion. This study developed an important new methodology of tracking individual health behaviors in a low-income rural setting through the Rota Card system. Though previous literature supported CHWs as particularly effective regarding exclusive breast-feeding and immunization coverage, it was believed that one-on-one personal encounters were required through door-to-door canvasing.11,13 This study demonstrates that using existing structures within churches for group preventive health promotion can link rural mothers to new vaccines through a low-cost community initiative.
Our efficacy rates ranged from 0% to 1800%, which suggests that rural populations are dynamic between catchment areas. Rota Cards were not differentiated based on where they were distributed; it was impossible to determine if an infant’s Rota Card turned in at the health center originated from the catchment area’s closest church or not. It is common cultural practice for young mothers to relocate to the parents’ homestead and stay there around the period of delivery before moving back to their own home. Aggregate data in resource-poor rural settings may need to adapt to the flow of individuals between homes and clinics.
Environmental health technicians consistently visited churches monthly but did not routinely collect Rota Cards from health clinics. Thirteen of the 19 churches included in analysis averaged at least one EHT weekend visit per month on average, boosted through transport fee reimbursement, but only 60 of the 317 Rota Cards collected at clinics were collected by EHTs. The study team had to collect the remaining 257. While this is consistent with previous evidence of unsatisfactory record keeping in 2 rural Kenyan hospitals, it is also surprising since EHTs should be visiting health facilities regularly.21 Future efforts working with EHTs and other governmental health officials should attempt to garner more buy-in from assisting staff as well as developing electronic data capabilities.
A major strength of this study was the innovative use of Rota Cards for tracking health behaviors. It provided direct evidence that rural communities reached through church can be linked to health facilities. Second, it suggests that existing rural structures like churches can be a sustainable addition to health systems’ outreach activities in low-resource communities. In Zambia, where the doctor to population ratio is in excess of 1 to 14 000, and the nurse to population ratio is 1 to 1700, there is no other way to effectively reach the population with heath care than to capitalize on such existing structures.22
Several limitations existed in this study. First, aggregated women’s group attendance does not delineate how many unique individuals attended health sessions, so the assumption that the same cohort of women came each week underestimated reach. Second, lack of a control group led to an overestimate of efficacy since it is unclear what proportion of rotavirus vaccination behaviors were due to the CHW’s health messaging versus mothers’ initial intent to immunize their children regardless of health messaging. Third, knowledge and attitudes were not directly measured to more directly assess health-messaging efficacy. Fourth, many mothers did not remember or were confused on when to drop off Rota Cards, leading to an underestimate of efficacy. Fifth, the inability to verify the actual number of eligible babies within the church because mothers might not bring babies younger than 15 weeks to church in an attempt to protect them from infections underestimated efficacy. Sixth, some CHWs complained about not receiving any form of money for the work they were doing and the study did not offer any incentives. This could be one of the reasons that churches dropped out of the study. Finally, a large number of eligible babies did not receive Rota Cards, but this can almost entirely be explained by the likely inaccurate reporting of 357 eligible babies and only 4 cards distributed by the Railway–UCZ church (Figure 3).
Figure 3.

Reach and efficacy by church.
Future studies should examine how much knowledge is gained and how health behaviors change compared with a control group through church-based preventive health promotion. This study could be improved and extended by adding a control group, assessing baseline knowledge and attitudes about a health topic, assessing change in knowledge and attitudes after health programming, tracking individuals’ attendance and knowledge scores rather than aggregate tracking, better training CHWs for data collection, adding more quality control to limit missing data, and designing incentives to retain churches and reduce the attrition rate.
Conclusion
Churches are effective existing community structures for community health workers to use as a platform for communicating preventive health messages to rural populations in low-income countries.
Acknowledgments
We would like to appreciate the contributions of all the community health workers, environmental health technicians, and the mothers who participated in the project. We acknowledge the administrative support from Cheryl Rudd, Monde Ndana, Annie Chikombo, and Rebecca Chitundu. The authors are grateful for the support and participation of all the leadership and administrators who allowed our program in their churches.
Author Biographies
Austin Wesevich is an MD/MPH student at Washington University who interned for the Centre for Infectious Diseases Research in Zambia through a Benjamin H. Kean Travel Fellowship in Tropical Medicine from the American Society of Tropical Medicine and Hygiene.
Jenala Chipungu holds a masters degree in public health and presently serves as Research Fellow at the Centre for Infectious Disease in Zambia. She is a social and behavioural scientist with particular interest in understanding human behaviour and how to modify it for better health outcomes.
Mercy Mwale is a social worker and an assistant community coordinator at Centre for Infectious Disease Research in Zambia. Currently pursuing a bachelor’s degree in Social work and has worked for the organization for 6 years in Prevention of Mother To Child Transmission of HIV(PMTCT) and Program for Awareness and Elimination of Diarrhoea (PAED). Other projects on community work – Millennium Development Goals Initiative (MDGI), Water and Sanitation and Menstrual Hygiene Management in schools and community (WASH).
Samuel Bosomprah is a medical statistician and the head of Analysis at the Centre for Infectious Disease Research in Zambia. In his immediate previous role, he served as senior lecturer and head of Department of Biostatistics at the University of Ghana School of Public Health. Prior to joining academia, he has worked as senior statistician and M&E specialist at the Ghana Ministry of Health for 7 years.
Roma Chilengi is a physician, epidemiologist and clinical research specialist. He serves as chief scientific officer at the centre for infentious Disease Research in Zambia where he oversees all scientific work.
Footnotes
Authors’ Note: The views and conclusions expressed in this article are the authors’ own as Absolute Return for Kids (ARK) played no role in the design, collection of data, and interpretation of results.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Absolute Return for Kids (ARK), a UK-based child welfare charity.
References
- 1. Scheil-Adlung X, ed. Global evidence on inequities in rural health protection: New data on rural deficits in health coverage for 174 countries. 2015. http://www.social-protection.org/gimi/gess/ShowRessource.action?ressource.ressourceId=51297. Accessed December 4, 2015.
- 2. Population Reference Bureau. The urban-rural divide in health and development. 2015. http://www.prb.org/pdf15/urban-rural-datasheet.pdf. Accessed December 4, 2015.
- 3. Global Health Workforce Alliance, ed. Mid-level health workers for delivery of essential services. A global systematic review and country experiences: Annex 7. Zambia case study. November 2013. http://www.who.int/workforcealliance/knowledge/resources/MLHWCountryCaseStudies_annex7_Zambia.pdf. Accessed December 4, 2015.
- 4. UNICEF. Zambia. Statistics. http://www.unicef.org/infobycountry/zambia_statistics.html. Accessed September 2, 2015.
- 5. Liu L, Johnson HL, Cousens S, et al. ; Child Health Epidemiology Reference Group of WHO and UNICEF. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379:2151-2161. doi: 10.1016/S0140-6736(12)60560-1. [DOI] [PubMed] [Google Scholar]
- 6. Bar-Zeev N, Kapanda L, Tate JE, et al. ; VacSurv Consortium. Effectiveness of a monovalent rotavirus vaccine in infants in Malawi after programmatic roll-out: an observational and case-control study. Lancet Infect Dis. 2015;15:422-428. doi: 10.1016/S1473-3099(14)71060-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Jiang V, Jiang B, Tate J, Parashar UD, Patel MM. Performance of rotavirus vaccines in developed and developing countries. Hum Vaccin. 2010;6:532-542. doi: 10.4161/hv.6.7.11278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Tate JE, Burton AH, Boschi-Pinto C, et al. 2008 estimate of worldwide rotavirus-associated mortality in children younger than 5 years before the introduction of universal rotavirus vaccination programmes: a systematic review and meta-analysis. Lancet Infect Dis. 2012;12(2):136-141. doi: 10.1016/S1473-3099(11)70253-5. [DOI] [PubMed] [Google Scholar]
- 9. Rudd C, Mwenda J, Chilengi R. Rotavirus landscape in Africa. Towards prevention and control: a report of the 8th African rotavirus symposium, Livingstone, Zambia. Vaccine. 2015;33:3263-3267. doi: 10.1016/j.vaccine.2015.04.002. [DOI] [PubMed] [Google Scholar]
- 10.Strengthening the performance of community health workers in primary health care. Report of a WHO Study Group. World Health Organ Tech Rep Ser. 1989;780:1-46. [PubMed] [Google Scholar]
- 11. Perry H, Zulliger R. How effective are community health workers? An overview of current evidence with recommendations for strengthening community health worker programs to accelerate progress in achieving the health-related millennium development goals. http://www.hrhresourcecenter.org/node/4754. Accessed September 16, 2015.
- 12. Gilmore B, McAuliffe E. Effectiveness of community health workers delivering preventive interventions for maternal and child health in low- and middle-income countries: a systematic review. BMC Public Health. 2013;13:847. doi: 10.1186/1471-2458-13-847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Pegurri E, Fox-Rushby JA, Damian W. The effects and costs of expanding the coverage of immunisation services in developing countries: a systematic literature review. Vaccine. 2005;23:1624-1635. doi: 10.1016/j.vaccine.2004.02.029. [DOI] [PubMed] [Google Scholar]
- 14. US Department of State. Zambia. International religious freedom report 2007. Published September 14, 2007. http://www.state.gov/j/drl/rls/irf/2007/90127.htm. Accessed September 5, 2015.
- 15. Campbell MK, James A, Hudson MA, et al. Improving multiple behaviors for colorectal cancer prevention among african american church members. Health Psychol. 2004;23:492-502. doi: 10.1037/0278-6133.23.5.492. [DOI] [PubMed] [Google Scholar]
- 16. Viswanathan M, Kraschnewski J, Nishikawa B, et al. ; RTI International-University of North Carolina Evidence-based Practice Center. Outcomes of community health worker interventions. Evid Rep Technol Assess (Full Rep). 2009;(181):1-144, A1-2, B1-14, passim. http://www.ahrq.gov/sites/default/files/wysiwyg/research/findings/evidence-based-reports/comhwork-evidence-report.pdf. Accessed December 4, 2015. [PMC free article] [PubMed] [Google Scholar]
- 17. Pengpid S, Peltzer K, Skaal L. Efficacy of a church-based lifestyle intervention programme to control high normal blood pressure and/or high normal blood glucose in church members: a randomized controlled trial in Pretoria, South Africa. BMC Public Health. 2014;14:568. doi: 10.1186/1471-2458-14-568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Lumpkins CY, Coffey CR, Daley CM, Greiner KA. Employing the church as a marketer of cancer prevention: a look at a health promotion project aimed to reduce colorectal cancer among African Americans in the Midwest. Fam Community Health. 2013;36:215-223. doi: 10.1097/FCH.0b013e31829159ed. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. DiGuiseppi CG, Thoreson SR, Clark L, et al. Church-based social marketing to motivate older adults to take balance classes for fall prevention: cluster randomized controlled trial. Prev Med. 2014;67:75-81. doi: 10.1016/j.ypmed.2014.07.004. [DOI] [PubMed] [Google Scholar]
- 20. Republic of Zambia Central Statistical Office. 2010 Census of population and housing preliminary report. 2011. http://unstats.un.org/unsd/demographic/sources/census/2010_phc/Zambia/PreliminaryReport.pdf. Accessed December 4, 2015.
- 21. Chiba Y, Oguttu MA, Nakayama T. Quantitative and qualitative verification of data quality in the childbirth registers of two rural district hospitals in western Kenya. Midwifery. 2012;28:329-339. doi: 10.1016/j.midw.2011.05.005. [DOI] [PubMed] [Google Scholar]
- 22. US President’s Emergency Plan for AIDS Relief. Zambia 2014 country operational plan executive summary. Published April 2, 2015. http://www.pepfar.gov/countries/cop/240133.htm. Accessed October 18, 2015.