

Abstract
Purpose
This study aimed to develop and examine the acceptability, feasibility and usability of a text messaging, or Short Message Service (SMS), system for improving the receipt of survivorship care for adolescent and young adult (AYA) survivors of childhood cancer.
Methods
Researchers developed and refined the text messaging system based on qualitative data from AYA survivors in an iterative 3-stage process. In stage 1, a focus group (n=4) addressed acceptability; in stage 2, key informant interviews (n=10) following a 6-week trial addressed feasibility; and in stage 3, key informant interviews (n=23) following a 6-week trial addressed usability. Qualitative data were analyzed using a constant comparative analytic approach exploring in-depth themes.
Results
The final system includes programmed reminders to schedule and attend late effects screening appointments, tailored suggestions for community resources for cancer survivors, and messages prompting participant feedback regarding the appointments and resources. Participants found the text messaging system an acceptable form of communication, the screening reminders and feedback prompts feasible for improving the receipt of survivorship care, and the tailored suggestions for community resources usable for connecting survivors to relevant services. Participants suggested supplementing survivorship care visits and forming AYA survivor social networks as future implementations for the text messaging system.
Conclusions
The text messaging system may assist AYA survivors by coordinating late effects screening appointments, facilitating a partnership with the survivorship care team, and connecting survivors with relevant community resources.
Implications for Cancer Survivors
The text messaging system has the potential to improve the receipt of survivorship care.
Keywords: Survivorship, adolescent and young adult, SMS, mobile device, text message, late effects
Background
Improvements in the rate of long-term survival of childhood cancer to over 83% has resulted in a growing population of adolescent and young adult (AYA) survivors at serious risk of late effects from treatment [1]. It is estimated that 65% of childhood cancer survivors will experience at least one chronic or late-occurring effect, and about 30% will experience a life-threatening late effect [2]. Late effects from cancer therapy include a variety of physical, psychological and social conditions in excess when compared to age-matched norms as they age into adulthood [3–7]. As a result, the Institute of Medicine (IOM) has recommended that childhood cancer survivors receive life long risk-based survivorship care for surveillance, prevention and treatment of late effects [8]. This recommended survivorship care consists of clinic visits where the provider reviews a patient’s past cancer treatment history, a physical exam and other diagnostic evaluations based on cancer treatment exposures that may include imaging procedures, laboratory evaluations or referrals to other specialty providers.
Despite these clinical guidelines, the majority of cancer survivors do not receive cancer-related care addressing prior cancer history and personal risks for late effects [9, 10]. Moreover, as risks for late effects increase with time since diagnosis, the proportion of survivors receiving medical attention decreases [9]. Several publications from the Childhood Cancer Survivor Study, the largest cohort of long-term childhood cancer survivors, have demonstrated that regular, risk-based screening for late effects is needed for early diagnosis to reduce future morbidity and mortality as survivors age. This is because there are late effects, that may be asymptomatic at early stages, such as cardiac dysfunction due to anthracycline exposure, so early detection and treatment is needed to minimize long-term morbidity and mortality [11–13]. Therefore, it is critical to encourage early adoption of late effects screening practices in AYA survivors. However, in order to receive recommended care, AYA survivors face several barriers: (1) health care system barriers such as a fragmented health care system and high health care costs; (2) provider barriers such as a lack of knowledge or comfort providing care for AYA survivors; and (3) patient barriers such as a lack of knowledge of late effects and beneficial health behaviors [14–18]. In summary, these barriers to care for AYAs are unique when compared to very young childhood cancer survivors or older adult survivors due to their age-specific psychosocial and logistical barriers to care. The AYA survivor wishes to move on with life after their cancer diagnosis, has competing life responsibilities including balancing competing demands of work and children, and not perceiving the need for a visit due to lack of symptoms [19]. To overcome these barriers, there is a need for an age-appropriate and innovative approach to improve the receipt of survivorship care in AYA survivor populations.
Mobile technology with Short Message Service (SMS) capabilities, also known as text messaging, is emerging as an innovative approach for sending both appointment reminders and health related messages in non-cancer populations [20–22]. For example, there have been increasing literature demonstrating the effects of text messaging interventions through self-care management and improving compliance rates. Positive effects on the self-management of diabetes have been shown when patients can send text messages to their provider regarding their glucose levels and later receive a follow up message with feedback specific to their needs, resulting in improved HBA1c levels [23]. Additionally, increased adherence and improved viral suppression in adults have also been demonstrated when patients can receive weekly text message reminders notifying them of their next antiretroviral treatment [24–26]. Similarly, immunizations rates in infants and adolescents rise in low-income populations when parents receive reminders regarding their child’s next appointment and education materials through a text messaging system [27, 28]. In a study, which tested the effectiveness of a mobile phone, based messaging intervention system called, Advanced Symptom Management System (ASyMS), participants who had recently undergone chemotherapy found its effects useful in managing their symptoms post-treatment and increased communication with their doctors when they could send text messaging reports about any adverse symptoms they were experiencing [29]. Text messaging is ubiquitous and the use of mobile phones cuts across demographics more so than home computers and internet access [30, 31]. An ever increasing number of AYAs in the United States carry mobile phones, with 68% of 12–13 year olds, 83% of 14–17 year olds, and 97% of 18–24 year olds owning a cell phone [30, 31]. The most recent Pew report claims that “teens represent the cutting edge of mobile connectivity” making a text messaging based intervention especially appropriate for this age group [30, 31]. To our knowledge, a text messaging intervention study has not been previously conducted in AYA childhood cancer survivor populations.
In this pilot study, we developed and investigated the use of a text messaging system to facilitate receipt of survivorship care for AYA survivors of childhood cancer. The objectives were to: (1) develop the text messaging system for sending programmed late effects screening reminders and tailored suggestions for community resources; (2) examine the acceptability, feasibility, and usability of the text messaging system for AYA survivors; and (3) refine the text messaging system using the qualitative data collected for use in a future intervention study.
Methods
Study participants
English-speaking AYA survivors of childhood cancer from the greater Los Angeles area were recruited from the UCLA Pediatric Hematology/Oncology Survivorship Database in person at clinic appointments, via email or via mail. Inclusion criteria for this study were: between the ages of 15–39 years at the time of study participation (the National Cancer Institute’s definition of an AYA) as this is the age group when transitioning to adult centered care often results in lack of survivorship follow-up care; off cancer therapy >1 year, and having a cell phone with text messaging capability and personal use [32]. A convenience sample was employed for the cost and time considerations of the pilot study. Each participant completed a questionnaire that asked about age, gender, race, age at diagnosis, type of cancer, cancer treatment, cell phone ownership, education level, annual income, and insurance information.
Study Design
This was a 3 stage cross-sectional pilot study in collaboration of UCLA’s Center for Embedded Network Sensing (CENS). Established in 2002, the CENS is a research enterprise led by UCLA and in partnership with five other Southern California universities. With the collaborative efforts of faculty, staff and students across a spectrum of fields such as Computer Science, Electrical Engineering, Urban Planning, Statistics and Education, the CENS project aims to explore the fundamental properties of embedded networked sensing systems to develop new technologies and investigating their role in health care and other systems education properties (http://auvac.org/people-organizations/view/386). The CENS role for this study was to develop a SMS platform to facilitate receipt of survivorship care. The SMS platform initially developed by CENS was evaluated for use by cancer survivors through a 3-stage process in which they provided qualitative data collected from a focus group and key information interviews to provide recommended revisions to the initial SMS platform. An overview of the 3–stage pilot study is shown in figure 1.
Figure 1.
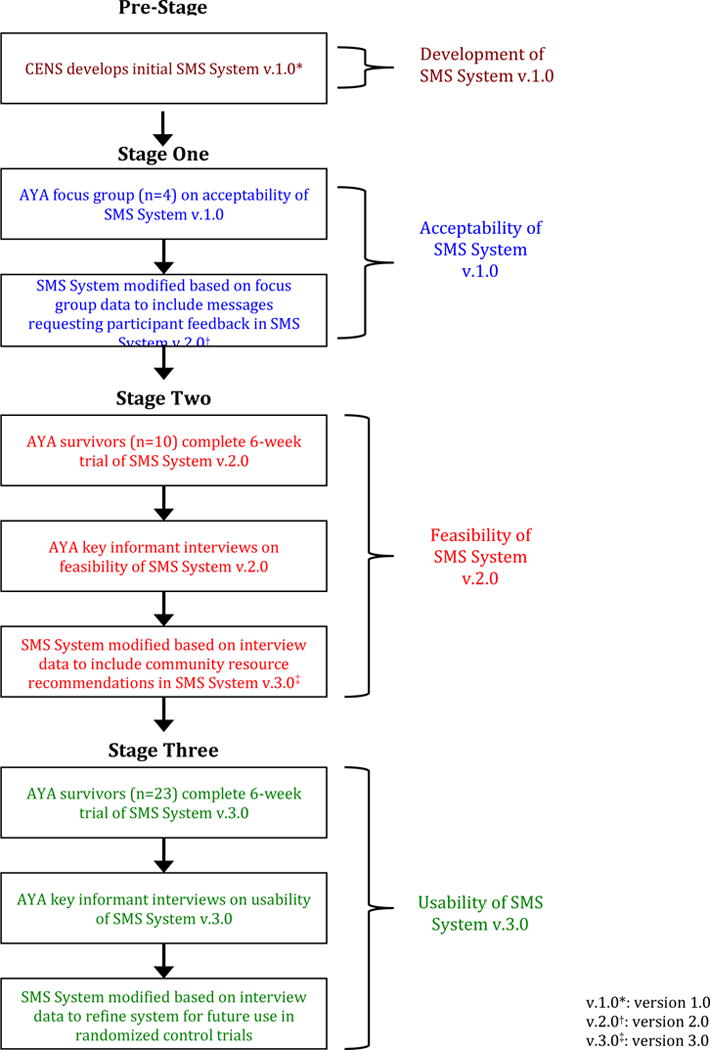
Flowchart outlining the 3-stage pilot study to develop the text messaging system.
Ethical Approval
The UCLA Institutional Review Board approved the study protocol and informed consent was obtained for each subject. Participants received a $40 gift card to offset potential text messaging costs.
Pre-Stage Development
SMS System version 1.0 design
CENS designed a 2-way text messaging system capable of sending programmed messages from the survivorship provider and managing response data from the participant. The system has a web interface for simple participant enrollment and monitoring of provider-guided text messages and participant responses. CENS built the text messaging system using existing open source software including the RapidSMS web framework, which was integrated with both a structured query language database and basic data visualization for users. The text messaging system was programmed in Python using the Django Framework. Python is a dynamic and strongly-typed programming language, while Django is a web framework that is written in Python that implements a standard three-tier web application architecture: database, user interface and the logic that mediates collecting and displaying data to the user. The basic function of SMS System version 1.0 (v.1.0) was to send programmed reminders to schedule and attend late effects screening appointments.
The survivorship care provider manages the text messaging system through the web interface (Patient Task Manager). Through this interface, the provider can enroll participants and input any late effects screening they recommend based on therapeutic exposures and Children’s Oncology Group survivorship guidelines [33]. Figure 2 shows the Processes tab, under which providers enroll new participants in the Patients column and input late effects screenings’ needed in the Scheduled column. Each late effects screening recommendation is defined as a “process” in the system. For example, if etoposide was part of a survivor’s past chemotherapy, he or she would be asked to schedule a complete blood count (CBC) to monitor for therapy-related leukemia. This CBC recommendation would be labeled as a “process.” The provider can schedule multiple late effects screening recommendations, or “processes,” for a single participant.
Figure 2.
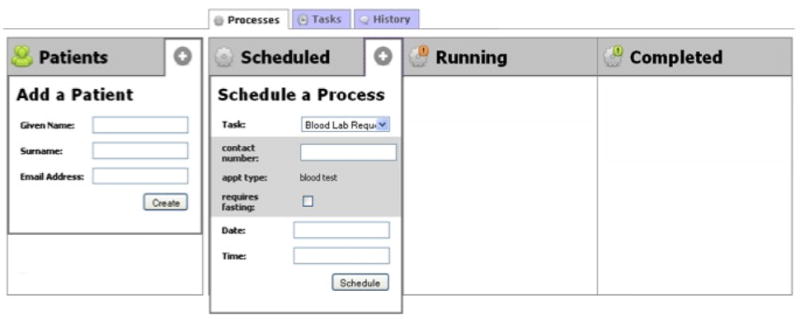
SMS Interface Processes Tab To enroll participants, providers input first name, surname, and email address. To input a late effects screening recommendation, the provider selects the appropriate item from the drop down task menu under ‘Schedule a Process,’ and enters the contact number for the referral. If the appointment has already been scheduled, the provider can input date and time. The provider can also select fasting requirements if necessary.
When a provider inputs a late effects screening recommendation, or “process,” the system will automatically send an “appointment request” text message to the participant detailing the screening needed and phone number for the office or lab, prompting them to schedule the appropriate appointment. Participants respond to the “appointment request” text message with the time and date of the appointment he or she has scheduled. Integrating this response, the system programs an “appointment reminder” message to be sent 2 days before, the day before, and the morning of the participant’s appointment detailing the type of appointment and the time and date with any specific requirements (i.e. fasting). Participants can opt out of receiving messages at any time by replying “STOP”. Moving on to the History Tab, shown in Figure 3, the provider can view the messages sent to and from the participant, detailing if the survivor scheduled the appointment or did not.
Figure 3.
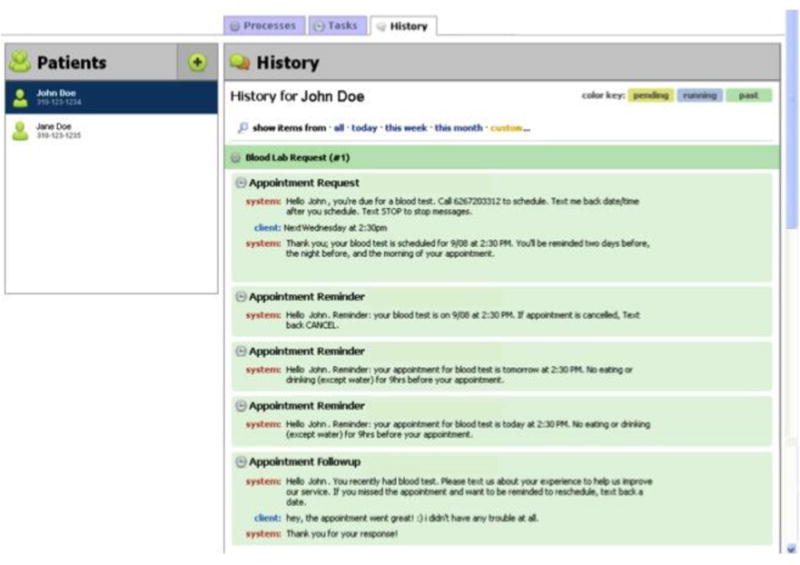
SMS Interface History Tab Providers can view a record of the conversation between the system (provider) and the client (participant) under the History tab. Each text message is time-stamped for appropriate archival of participant-provider communication.
Stage One
SMS System version 1.0: AYA focus group
A focus group of four AYA survivors (n=4) was conducted to provide in-depth qualitative data on the acceptability of SMS System v.1.0 for sending programmed reminders to schedule and attend late effects screening appointments and recommendations for system improvements. A survivorship research assistant (RA) guided the discussion with open-ended questions. Major themes that were identified from the qualitative data informed the modification of the text messaging system to develop SMS System version 2.0 (v.2.0).
Stage Two
SMS System version 2.0: AYA key informant interviews
Ten AYA survivors (n=10) participated in a 6-week trial of SMS System v.2.0 that was developed from changes received by focus group participants in stage 1. After using the text messaging system for 6 weeks, participants completed key informant interviews with the RA to provide in-depth qualitative data on the feasibility of SMS System v.2.0 to improve the completion of late effects screening(s) and recommendations for system improvements. Themes extracted from the qualitative data informed the modification of the SMS system to develop SMS System version 3.0 (v.3.0).
Stage Three
SMS System version 3.0: AYA key informant interviews
Twenty-three AYA survivors (n=23) participated in a 6-week trial of SMS System v.3.0. After using the text messaging system for 6 weeks, participants completed key informant interviews with the RA to provide in-depth qualitative data on the usability of SMS System v.3.0 to assist in reaching personal survivorship health behavior goals.
Qualitative analysis used for the 3 stages
The focus group and key informant interviews were audiotaped and transcribed verbatim. Qualitative analysis of the transcriptions was conducted using the grounded theory approach developed by Glaser and Strauss which uses inductive reasoning [34]. Using this approach in the study, inductive reasoning began with data collection from the survivor’s healthcare experience and then through a coding procedure, the data was compared to one another. Through this process, key theories and themes were made. Transcript data for each of the 3 stages of data collection were reviewed separately and codes were then categorized and refined through a constant comparative method, from which themes were identified. Quotes from the text were then extracted for each theme [35, 36]. Two coders (RAs) independently coded the transcripts and then met to review the codes and themes with each other and the first author to discuss any disagreements and resolve differences. There was 90% agreement between the coders in both the focus group and key informant interview transcript analysis. Transcripts were loaded into NVIVO 10 (QSR International) to assist with systematic coding and text management [37].
Results
Stage One
Acceptability of SMS System v.1.0
Sample characteristics of focus group in stage 1
Two male and 2 female cancer survivors (n=4), aged 20–35 and diagnosed between ages 2–19, participated in the focus group. All participants received chemotherapy and 3 received radiation therapy. Three participants had insurance coverage and all had at least some college education. All participants had copies of their medical records, treatment summary, and a survivorship care plan, indicating they were highly engaged survivors. All participants had a mobile device with text messaging capabilities, and 3 of the 4 participants had unlimited text messaging plans.
Thematic analysis of focus group
Two key themes emerged as positive attributes of SMS System v.1.0 from the focus group in stage 1:
Acceptable method for communicating reminders to schedule and attend late effects screening appointments
The AYA focus group participants preferred text message reminders to automated phone calls, the traditional method of appointment reminders in clinical settings. Participants felt that viewing and responding to text messages was more convenient than listening to automated phone call reminders. The participants reported that receiving reminders by text message created a sense of urgency to schedule appointments because it is a rapid form of communication, difficult to ignore as it automatically notifies the individual regardless of location or access to the Internet, and it is short in length making it quick to read.
Simplification of late effects screening recommendations
Focus group participants repeatedly commented on the overwhelming nature of the lengthy lists of late effects screening recommendations, typical of annual survivorship care planning visits. The text messages effectively deconstructed these lists by delivering concise information for easy comprehension and providing actionable steps to complete the screening recommendations. Coordinating late effects screening can be highly complex in a fragmented health care system with referrals to multiple community providers, often not at the cancer center providing survivorship care. Focus group participants felt the text messaging system simplified these recommendations by consolidating reminders to various providers into one platform.
I think it gets sometimes overwhelming and confusing…I have to get my skin checked, I’ve got my dermatologist, and I’ve got my mammogram, I’ve got my UCLA appointment, I went to a neurologist, so that it literally ends up being at least one doctor a week…Text messages would help in terms of a reminder like you’re actually due for this…
One key theme emerged as a proposed modification of SMS System v.1.0 from the focus group in stage 1:
Providing referrals to providers knowledgeable in cancer survivorship
Participants expressed the need for screening referrals to providers that are knowledgeable in the care of AYA survivors. The survivors discussed feeling their survivorship health care concerns were often not valued by providers. For example, if a survivorship provider refers a survivor to a cardiologist in their local community, the provider may not be aware of the specific risks the survivor faces due to previous cancer treatment as they typically care for older aged patients in their practice. As a result, the providers may not actively engage in conversations regarding strategies to maintain cardiac health with the AYA survivors.
If you’re given your care plan, [it is challenging] to find…specialists…like where do I go? And who is the best person? Who is experienced with what I have been through?
Modifications made to SMS System version 1.0
Based on the major themes identified from the focus group data recommending opportunities for survivor feedback on late effects screening appointments, CENS researchers added “appointment followup” messages to SMS System v.2.0. After a participant responds to an “appointment request” message with the time and date of the appointment he or she has scheduled, the system automatically programs an “appointment followup” message to be sent after the scheduled appointment time. The participant can respond with information regarding his or her experience, including how much knowledge the provider had in childhood cancer survivorship and whether they would return to that provider for late effects screening. The survivorship provider can view participant feedback on the web interface under the History Tab (see Figure 3).
Stage 2
Feasibility of SMS System v.2.0
Sample characteristics of SMS System v.2.0 trial participants in stage 2
Six male and 4 female cancer survivors (n=10), aged 19–38, participated in the SMS System v.2.0 trial. The ethnically diverse sample of participants was diagnosed between ages 2 and 19. All participants received chemotherapy, 9 received radiation therapy, and 5 underwent a bone marrow transplant. Participants had been diagnosed with either leukemia, lymphoma, a CNS tumor, or rhabdomyosarcoma. Nine participants had insurance coverage and all had at least some college education.
Thematic analysis of key informant interviews
One key theme emerged as a positive attribute of SMS System v.2.0 from participants in stage 2:
Encouraged active health monitoring
Participants felt the text messaging system reminders prompted them to schedule and attend their late effects screening appointments. Participants reported that the familiar language of the text messages, tailored to fit their demographic, encouraged them to schedule the appointments. For example, “you” was replaced with “u” and emoticons were used to supplement the text message. As a result, the text message reminders were interpreted favorably and perceived as friendly and “cool” despite their brevity.
It’s funny because the next appointment I had [was]…my thyroid scan, and like I missed it twice. And if I had the text thing I probably would have remembered it.
Two key themes emerged as a proposed modification of SMS System v.2.0 from participants in stage 2:
Improving text message logistics
Although participants wanted “appointment reminder” messages delivered both two days before and on the morning of an appointment, they did not want an “appointment reminder” message the night before a scheduled appointment. They indicated that reminders sent the night before an appointment could induce anxiety.
Providing resources to help reach survivorship goals
Participants discussed how the text messaging system could provide suggestions for community resources specific to individual survivorship needs. These resources could help survivors set and meet personal survivorship health behavior goals beyond scheduling and attending late effects screening appointments.
Modifications made to SMS System version 2.0
Based on the major themes identified from the key informant interviews, CENS researchers developed programmed messages to provide tailored suggestions for community survivorship resources to assist participants in reaching personal survivorship health behavior goals. In order to personalize suggestions to each participant, additional fields for age, diagnosis, and zip code were added to enrollment. Community survivorship resources were compiled from an established UCLA Cancer Survivorship community resource database and filtered by the text messaging system based on the information provided for each participant. Based on major themes regarding functional aspects of the system, CENS reduced the number of “appointment reminder” messages from 3 to 2 by removing the programmed message the night before the scheduled appointment.
Stage Three
Usability of SMS System v.3.0
Sample characteristics of SMS System v.3.0 pilot trial participants in stage 3
Twelve male and 11 female cancer survivors (n=23), aged 16–35, participated in the SMS System v.3.0 trial. The sample was ethnically diverse and included non-Hispanic White, African American, Asian Pacific Islander, Latino, multiracial, and other participants. The participants were diagnosed between ages 2 and 19. All participants received chemotherapy, 11 received radiation therapy, and 7 underwent a bone marrow transplant. Nineteen participants had insurance coverage. Fifteen participants had at least some college education, 3 had graduated high school, and 6 had not graduated high school.
Thematic analysis of key informant interviews
Three key themes emerged as positive attributes of SMS System v.3.0 from participants in stage 3:
Increased awareness of community resources for AYA survivors
Participants felt the messages increased awareness of community resources that were specific to their personal needs. For example, despite a basic familiarity with the American Cancer Society (ACS), one participant was unaware that the organization provided resources for obtaining health insurance.
Yeah, that [resource from the ACS] was really interesting because I never thought could go through that agency to find more information. So that really helped because I started thinking about what kinds of health insurance I need to consider right now [as a survivor].
Empowered AYA survivors to access community resources specific to their needs
Participants suggested that the messages empowered them to become confident consumers of community survivorship resources by actively engaging the survivor outside of the survivorship care planning visits. The system provided actionable steps to access the community survivorship resources by giving specific contact information and a brief description of the program(s). The text messaging system continued to engage the survivor by sending a “followup” message to confirm if the resource had been accessed and prompted feedback about the usefulness of the resource for the survivor.
It lit a fire under me to actually find a [local] program… I never knew all the different resources you could have or call to find out your care and I really liked that. I thought it was really good. It touched on everything that you have questions about but don’t necessarily know who to ask.
Allows AYA survivors to partner with the survivorship care team
The participants saw the text messaging system as a tool to reach their health care goals by partnering with their survivorship care team. The “followup” messages provided a valuable opportunity for participant feedback, allowing them to actively participate in the management of their survivorship care.
You were able to respond with what you were looking for. How you wanted to organize what was priority and least priority to you…that this is the most important thing to me right now and then once I get this done I want to do this and this.
Two key themes emerged as proposed modifications of the SMS System from participants in stage 3:
To educate AYA survivors about their individual survivorship care plan
The participants discussed how the text messaging system could supplement the survivorship care plan they received in the clinical setting. AYA survivors expressed interest in receiving specific information about their cancer diagnosis, treatment exposures, and risks for late effects through the text messaging system. AYA survivors could receive a text message detailing survivorship care planning information in an accessible and concise manner.
I thought [the text messaging system] was actually going to give me like, “oh so you are at risk of having cardiac whatever because you took…so you need to be aware of x, y, and z,” but instead it just kept sending me back to that big-binder that I had gotten one day when I spent like three hours with my…it would be a lot more accessible or a lot more useful if I was getting that information through the text. Like little bite-sized pieces of information that I would get – like everyday it would send me a new thing…
To establish an AYA survivor network
The participants saw this text messaging system as an opportunity for creating an active survivor network in their local community. AYAs would like to meet peers who understand their unique experience and may share similar interest(s). For example, if there were a local exercise program for survivors, they could potentially attend with peers they meet through the network.
Yeah cause I feel like when you’re a survivor, support isn’t necessarily what you need but more like just talking to other people. So networking…
A summary table of the focus group and key informant interview participants is below in table 1.
Table 1.
Patient demographics of all participants who participated in the 3 phases of the pilot study.
| Participant Table | |
|---|---|
| Stage One: | |
| Sample Size | n=4 |
| Males | 2 |
| Female | 2 |
| Age Range | 20–35 |
| Age of Diagnosis | 2–19 |
| Education Level | All college level educated |
| Diagnoses Types | leukemia, Lymphoma |
| Treatment Types | Chemotherapy, Surgery, Bone Marrow Transplant |
| Stage Two: | |
| Sample Size | n=10 |
| Males | 6 |
| Female | 4 |
| Age Range | 19–38 |
| Age of Diagnosis | 2–19 |
| Education level | All college level educated |
| Diagnoses Types | Leukemia. Lymphoma, Rhabdomysosarcoma |
| Treatment Types | Chemotherapy, Radiation Therapy, Surgery, Bone Marrow Transplant |
| Stage Three: | |
| Sample Size | n=23 |
| Males | 12 |
| Females | 11 |
| Age Range | 16 35 |
| Age of Diagnosis | 2–19 |
| Education Level | College, highschool and non-highschool graduates |
| Diagnoses Types | Leukemia, Lymphoma. Neuroblastoma |
| Treatment Types | Chemotherapy, Radiation Therapy. Surgery, Bone Marrow transplant |
Discussion
This 3-stage pilot study enabled CENS to develop and modify a text messaging system based on qualitative data from AYA survivors of childhood cancer. The final version, SMS System v.3.0 includes text messages delivering programmed reminders to schedule and attend late effects screening appointments, tailored suggestions for community resources for cancer survivors, and messages prompting participant feedback regarding appointments and resources. Participants found the text messaging system to be an acceptable form of communication, the screening reminders and feedback prompts feasible for improving the receipt of survivorship care, and the suggestions for community resources usable for connecting survivors to relevant services. Themes extracted from the qualitative data suggest the text messaging system has the potential to mitigate barriers in coordinating survivorship care, encourage active self-management of survivorship care, and help survivors reach personal survivorship health behavior goals beyond late effects screening.
By consolidating screening reminders to various providers into one platform, this text messaging system has the potential to help mitigate barriers posed by the fragmented health care system in the United States. For late effects screening, survivorship care providers refer patients to various specialists, often not located at the cancer center providing survivorship care, leading to difficulties coordinating care [15]. The text messaging system serves as a centralized platform for survivors to receive reminders for late effects screening appointments at various locations. Participants in this pilot study indicated feeling overwhelmed by the long lists of late effects screening recommendations. The reminders help simplify these lists by providing concise contact information for scheduling appointments, giving the survivor actionable steps in a more manageable format. Additionally, the system delivers persistent reminders to help the survivor reschedule any missed appointment to encourage the completion of late effects screening recommendations. There is a significant body of literature regarding the low uptake of recommended screening by survivors, and innovative interventions are needed to address this issue for early detection of late effects [38, 39]. By actively engaging the survivors to schedule and attend recommended late effects screening, the text messaging system may facilitate early diagnosis of late effects and ultimately improve health outcomes for AYA survivors.
Additionally, this text messaging system may promote adherence to late effects screening recommendations by supporting active self-management of survivorship care. The system reinforces recommendations by periodically sending prompts to the survivor between annual survivorship care planning visits. While little empirical evidence exists for interventions to improve adherence in the AYA survivor population due to the relative novelty of this area of study, self-management of care has been found to promote adherence in adolescents with chronic diseases [40]. Qualitative data from this study suggests that the “followup” messages prompting participant feedback empowered survivors to actively partner with their survivorship care team. It was reported that it enabled them to take more control of their care by providing feedback to their survivorship provider on their experience completing late effects screening in the community. Text messaging is a direct form of communication, able to deliver survivorship screening recommendations to the highly mobile AYA population. Participants also reported that the age-appropriate language and persistent reminders encouraged them to complete the screening recommendations. While there are multiple factors that can predict successful interventions in cancer survivors, including intervention timing, duration, and channels of delivery, it is critical to design the intervention to meet the needs of the specific population [41]. Based on the positive responses to the acceptability and age-appropriateness for AYA survivors of childhood cancer, this text messaging system shows promise for future intervention research for improving the receipt of survivorship care.
The text messaging system also has the potential to help survivors reach personal survivorship health behavior goals by connecting them to relevant community resources. There are many barriers to receipt of survivorship care including cost and insurance issues, distance to the cancer center, and fear of recurrence [42]. Community-based organizations offer low cost services to cancer survivors to help overcome these barriers, but survivors are often unaware these services are available [43]. By providing tailored suggestions for community resources, the system connects survivors directly with services they need such as assistance obtaining health insurance or joining social support and exercise groups. The text messaging system not only increases awareness, but also facilitates accessing resources by providing information about offered services and specific contact details. The messages prompting survivor feedback help ensure the community resource suggestions meet the needs of the survivor. For example, if a participant feels a community program targets an older survivor demographic after attending, the survivor can inform the provider by responding to the follow up message and receive information for another, more AYA age-appropriate program. Text messaging is also a highly accessible and scalable method for disseminating this information, as the participant does not need to be near the system administrator to get connected to resources local to them.
In the future, as suggested by study participants, the text messaging system could be used as a tool to deliver information about cancer diagnosis, treatment, and risks for late effects from the survivorship care plan. Knowledge of cancer diagnosis and past treatment precludes an awareness for susceptibility to late effects which is necessary to engage in preventive screening [44]. A past study found no difference in knowledge of diagnosis and past treatment between participants that had attended a survivorship clinic or received a survivorship care plan and those who had not [45]. This text messaging system has the exciting potential to supplement annual survivorship care planning visits by periodically delivering manageable excerpts of information from the care plan. Providing this information via text message between annual survivorship care planning visits may help improve knowledge and ultimately encourage the completion of late effects screening recommendations.
Limitations
While another theme, which emerged from the key informant interviews regarding modifications for future implementations included: developing an AYA network, this capability was beyond the scope of this study. However, it has been well established that cancer is an isolating experience [46], and the data collected here supports the need for the development and evaluation of a text messaging system or platform to meaningfully engage and connect AYA survivors.
Although our system currently provides a rudimentary conversational interface, extending it to parse a wider variety of inputs and support more spontaneous interactions could encourage patients to further interact with it and foster stronger communication with their care provider. The development of software agents that communicate in natural language with the patient, providing resources and acting as a proxy to the caregiver through a conversational interface, is a growing area of research [47]. The conversational model for mHealth using our SMS system is appropriate for supporting survivorship care adherence by helping the patient and provider stay within a constant loop of information. The patient’s provider who uses this system, has the ability in real-time to monitor patient-system interactions and address the needs of their patients accordingly. Google, Apple and Microsoft’s recent interest in personal assistants (Google Now, Siri, and Cortana, respectively), demonstrates that the conversational model is still of interest and can have many implications within a healthcare setting. For example, conversational agents such as Siri and Google Now, have been shown to have some ability in responding to health related responses. Although findings have indicated that the performance of these agents still need further improvement, Siri and Google Now will try to promptly communicate to its user of nearby medical facilities or emergency services if the user indicates that they are experiencing some type of physical pain or psychological distress [48]. In addition, as the mHealth field continues to develop, there are future research opportunities to improve the survivorship care of AYA survivors through the use of smartphone apps as this area continues to expand, including through the continued collaborative efforts of both the computer science mHealth and survivorship focused-health services research teams [49]. As technology advances, so do the opportunities to integrate the conversational portion of our SMS system into mobile applications without major user interface and experience changes. Technology is now faster, more accessible, and has the increased capacity of performing more complex functions. A text messaging system, although simple, can serve as the basic foundation for an application that can be used across various settings and by large populations for continued research. But for our pilot study, the development of a smartphone app was beyond the scope of the study. Nonetheless, the development and pilot testing of the SMS system has allowed an opportunity for mHealth intervention research in the AYA childhood cancer survivor population.
Lastly, while this pilot study provided an exploratory analysis of the benefits and potential use for this text messaging system, the convenience sample used was small and comprised of knowledgeable survivors already engaged in survivorship care, likely not representative of the larger population of AYA survivors of childhood cancer. However, theoretical saturation was reached and the relatively small sample size allowed for in-depth analysis and exploration of qualitative data regarding the acceptability, feasibility, and usability of the system. This encouraging preliminary data allowed for refinement of the text messaging system to be tested in a future randomized control trial.
Conclusion
AYA participants in this pilot study found the text messaging system acceptable, feasible, and usable for delivering late effects screening reminders and tailored suggestions for community resources. This text messaging system offers a promising tool to encourage completion of late effects screening recommendations and supporting active self-management of care. The system also has the potential to assist survivors in reaching personal survivorship health behavior goals by connecting them to tailored community resources. In the future, this SMS system developed in the pilot study will be further tested in a randomized control trial to examine the effectiveness in improving receipt of survivorship care in AYA survivors of childhood cancer.
Acknowledgments
Supported by Administrative Supplement NOT-CA-10-026 from the National Cancer Institute and by a seed grant from UCLA’s Jonsson Cancer Center Foundation.
Footnotes
Compliance with Ethical Standards
Conflict of Interest The authors declare they have no conflict of interest.
Ethical Approval All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All procedures were reviewed and approved by the Institutional Review Board of the University of California, Los Angeles.
Informed Consent Informed consent was obtained from all individual participants included in the study.
References
- 1.Howlander N, et al. SEER Cancer Statistics Review, 1975–2010. 2013 http://seer.cancer.gov/csr/1975_2010/ Accessed July 14, 2015.
- 2.Oeffinger KC, Hudson MM. Long-term complications following childhood and adolescent cancer: foundations for providing risk-based health care for survivors. CA Cancer J Clin. 2004;54(4):208–36. doi: 10.3322/canjclin.54.4.208. [DOI] [PubMed] [Google Scholar]
- 3.Zebrack BJ, Zeltzer LK, Whitton J, Mertens AC, Odom L, Berkow R, et al. Psychological outcomes in long-term survivors of childhood leukemia, Hodgkin’s disease, and non-Hodgkin’s lymphoma: a report from the Childhood Cancer Survivor Study. Pediatrics. 2002;110(1 Pt 1):42–52. doi: 10.1542/peds.110.1.42. [DOI] [PubMed] [Google Scholar]
- 4.Wenzel L, DeAlba I, Habbal R, Kluhsman BC, Fairclough D, Krebs LU, et al. Quality of life in long-term cervical cancer survivors. Gynecol Oncol. 2005;97(2):310–7. doi: 10.1016/j.ygyno.2005.01.010. [DOI] [PubMed] [Google Scholar]
- 5.Gurney JG, Krull KR, Kadan-Lottick N, Nicholson HS, Nathan PC, Zebrack B, et al. Social outcomes in the Childhood Cancer Survivor Study cohort. J Clin Oncol. 2009;27(14):2390–5. doi: 10.1200/JCO.2008.21.1458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Meadows AT, Friedman DL, Neglia JP, Mertens AC, Donaldson SS, Stovall M, et al. Second neoplasms in survivors of childhood cancer: findings from the Childhood Cancer Survivor Study cohort. J Clin Oncol. 2009;27(14):2356–62. doi: 10.1200/JCO.2008.21.1920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Friedman DL, Whitton J, Leisenring W, Mertens AC, Hammond S, Stovall M, et al. Subsequent neoplasms in 5-year survivors of childhood cancer: the Childhood Cancer Survivor Study. J Natl Cancer Inst. 2010;102(14):1083–95. doi: 10.1093/jnci/djq238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hewitt MWSL, Simone JV, editors. Childhood Cancer Survivorship: Improving Care and Quality of Life. Washington, D.C: The National Academies Press; 2003. [PubMed] [Google Scholar]
- 9.Oeffinger KC, Mertens AC, Hudson MM, Gurney JG, Casillas J, Chen H, et al. Health care of young adult survivors of childhood cancer: a report from the Childhood Cancer Survivor Study. Ann Fam Med. 2004;2(1):61–70. doi: 10.1370/afm.26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Nathan PC, Greenberg ML, Ness KK, Hudson MM, Mertens AC, Mahoney MC, et al. Medical care in long-term survivors of childhood cancer: a report from the childhood cancer survivor study. J Clin Oncol. 2008;26(27):4401–9. doi: 10.1200/JCO.2008.16.9607. doi: 26/27/4401[pii]10.1200/JCO.2008.16.9607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Armstrong GT1, Chen Y1, Yasui Y1, Leisenring W1, Gibson TM1, Mertens AC1, Stovall M1, Oeffinger KC1, Bhatia S1, Krull KR1, Nathan C1, Neglia JP1, Green DM1, Hudson MM1, Robison LL1. Reduction in Late Mortality among 5-Year Survivors of Childhood Cancer. N Engl J Med. 2016 Mar 3;374(9):833–42. doi: 10.1056/NEJMoa1510795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hudson MM1, Mulrooney DA, Bowers DC, Sklar CA, Green DM, Donaldson SS, Oeffinger KC, Neglia JP, Meadows AT, Robison LL. High-risk populations identified in Childhood Cancer Survivor Study investigations: implications for risk-based surveillance. J Clin Oncol. 2009 May 10;27(14):2405–14. doi: 10.1200/JCO.2008.21.1516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Myneni S1, Amith M1, Geng Y1, Tao C1. Towards an Ontology-driven Framework to Enable Development of Personalized mHealth Solutions for Cancer Survivors’ Engagement in Healthy Living. Stud Health Technol Inform. 2015;216:113–7. [PMC free article] [PubMed] [Google Scholar]
- 14.Pratt-Chapman M, Simon MA, Patterson A, Risendal BC, Patierno S. Survivorship Navigation Outcome Measures: A report from the ACS Patient Navigation Working Group on Survivorship Navigation. Cancer. 2011;117(15 0):3575–84. doi: 10.1002/cncr.26261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hewitt ME, Greenfield S, Stovall E, National Cancer Policy Board (U.S.) Committee on Cancer Survivorship: Improving Care and Quality of Life From cancer patient to cancer survivor lost in transition. Washington, DC: National Academies Press; 2005. [Google Scholar]
- 16.Kirchhoff AC, Lyles CR, Fluchel M, Wright J, Leisenring W. Limitations in health care access and utilization among long-term survivors of adolescent and young adult cancer. Cancer. 2012;118(23):5964–72. doi: 10.1002/cncr.27537. [DOI] [PubMed] [Google Scholar]
- 17.Suh E, Daugherty CK, Wroblewski K, Lee H, Kigin ML, Rasinski KA, et al. General internists’ preferences and knowledge about the care of adult survivors of childhood cancer: a cross-sectional survey. Ann Intern Med. 2014;160(1):11–7. doi: 10.7326/M13-1941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Zebrack BJ, Eshelman DA, Hudson MM, Mertens AC, Cotter KL, Foster BM, et al. Health care for childhood cancer survivors: insights and perspectives from a Delphi panel of young adult survivors of childhood cancer. Cancer. 2004;100(4):843–50. doi: 10.1002/cncr.20033. [DOI] [PubMed] [Google Scholar]
- 19.Smits-Seemann RR1,2, Kaul S3, Zamora ER4, Wu YP5,6, Kirchhoff AC7,5. Barriers to follow-up care among survivors of adolescent and young adult cancer. J Cancer Surviv. 2016 doi: 10.1007/s11764-016-0570-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Moskowitz DS, Young SN. Ecological momentary assessment: what it is and why it is a method of the future in clinical psychopharmacology. J Psychiatry Neurosci. 2006;31(1):13–20. [PMC free article] [PubMed] [Google Scholar]
- 21.Smyth JMSA. Ecological momentary assessment research in behavior medicine. J Happiness Stud. 2003;4:35–52. [Google Scholar]
- 22.Stone AA, Shiffman S. Capturing momentary, self-report data: a proposal for reporting guidelines. Ann Behav Med. 2002;24(3):236–43. doi: 10.1207/S15324796ABM2403_09. [DOI] [PubMed] [Google Scholar]
- 23.Fjeldsoe BS, Marshall AL, Miller YD. Behavior change interventions delivered by mobile telephone short-message service. Am J Prev Med. 2009;36(2):165–73. doi: 10.1016/j.amepre.2008.09.040. [DOI] [PubMed] [Google Scholar]
- 24.Lester R, Karanja S. Mobile phones: exceptional tools for HIV/AIDS, health, and crisis management. Lancet Infect Dis. 2008;8(12):738–9. doi: 10.1016/S1473-3099(08)70265-2. [DOI] [PubMed] [Google Scholar]
- 25.Mbuagbaw L, Bonono-Momnougui RC, Thabane L. Considerations in using text messages to improve adherence to highly active antiretroviral therapy: a qualitative study among clients in Yaounde, Cameroon. HIV AIDS (Auckl) 2012;4:45–50. doi: 10.2147/HIV.S29954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lester RT1, Ritvo P, Mills EJ, Kariri A, Karanja S, Chung MH, Jack W, Habyarimana J, Sadatsafavi M, Najafzadeh M, Marra CA, Estambale B, Ngugi E, Ball TB, Thabane L, Gelmon LJ, Kimani J, Ackers M, Plummer FA. Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): a randomised trial. Lancet. 2010 Nov 27;376(9755):1838–45. doi: 10.1016/S0140-6736(10)61997-6.9. [DOI] [PubMed] [Google Scholar]
- 27.Niederhauser V, Johnson M, Tavakoli AS. Vaccines4Kids: Assessing the impact of text message reminders on immunization rates in infants. Vaccine. 2015;33(26):2984–9. doi: 10.1016/j.vaccine.2015.04.069. [DOI] [PubMed] [Google Scholar]
- 28.Stockwell MS1, Kharbanda EO, Martinez RA, Vargas CY, Vawdrey DK, Camargo S. Effect of a text messaging intervention on influenza vaccination in an urban, low-income pediatric and adolescent population: a randomized controlled trial. JAMA. 2012 Apr 25;307(16):1702–8. doi: 10.1001/jama.2012.502. [DOI] [PubMed] [Google Scholar]
- 29.McCann L1, Maguire R, Miller M, Kearney N. Patients’ perceptions and experiences of using a mobile phone-based advanced symptom management system (ASyMS) to monitor and manage chemotherapy related toxicity. Eur J Cancer Care (Engl) 2009;18(2):156–64. doi: 10.1111/j.1365-2354.2008.00938.x. [DOI] [PubMed] [Google Scholar]
- 30.Madden MLA, Duggan M, Cortesi S, Gas U. Teens and Technology 2013. 2013 http://www.pewinternet.org/2013/03/13/teens-and-technology-2013/
- 31.Smith A. US Smartphone Use in 2015. 2015 http://www.pewinternet.org/2015/04/01/us-smartphone-use-in-2015/
- 32.Freyer DR. Transition of care for young adult survivors of childhood and adolescent cancer: rationale and approaches. J Clin Oncol. 2010 Nov 10;28(32):4810–8. doi: 10.1200/JCO.2009.23.4278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Children’s Oncology Group Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancer. 2013 http://www.survivorshipguidelines.org.
- 34.Strauss ACJ. Basics of Qualitative Research: Grounded Theory Procedures and Techniques. Newbury Park, CA: Sage; 1990. [Google Scholar]
- 35.Bradley EH, Curry LA, Devers KJ. Qualitative data analysis for health services research: developing taxonomy, themes, and theory. Health Serv Res. 2007;42(4):1758–72. doi: 10.1111/j.1475-6773.2006.00684.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Pope C, Ziebland S, Mays N. Qualitative research in health care. Analysing qualitative data. BMJ. 2000;320(7227):114–6. doi: 10.1136/bmj.320.7227.114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.QSR Vivo 8: Software for Qualitative Analysis. 8. Cambridge, MA: QSR International Pty Ltd; 2008. [Google Scholar]
- 38.Nathan PC, Ford JS, Henderson TO, Hudson MM, Emmons KM, Casillas JN, et al. Health behaviors, medical care, and interventions to promote healthy living in the Childhood Cancer Survivor Study cohort. J Clin Oncol. 2009;27(14):2363–73. doi: 10.1200/jco.2008.21.1441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Hudson MM, Ness KK, Gurney JG, et al. Clinical ascertainment of health outcomes among adults treated for childhood cancer. JAMA. 2013;309(22):2371–81. doi: 10.1001/jama.2013.6296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Butow P, Palmer S, Pai A, Goodenough B, Luckett T, King M. Review of adherence-related issues in adolescents and young adults with cancer. J Clin Oncol. 2010;28(32):4800–9. doi: 10.1200/jco.2009.22.2802. [DOI] [PubMed] [Google Scholar]
- 41.Stull VB, Snyder DC, Demark-Wahnefried W. Lifestyle interventions in cancer survivors: designing programs that meet the needs of this vulnerable and growing population. J Nutr. 2007;137(1 Suppl):243S–8S. doi: 10.1093/jn/137.1.243S. [DOI] [PubMed] [Google Scholar]
- 42.Children’s Oncology Group Nursing Discipline Clinical Practice Subcommittee/Survivorship in collaboration with the Late Effects Committee. Establishing and Enhancing Services for Childhood Cancer Survivors: Long-term Follow-up Program Resource Guide. 2007 [Google Scholar]
- 43.Gardner MH, Barnes MJ, Bopanna S, Davis CS, Cotton PB, Heron BL, et al. Barriers to the Use of Psychosocial Support Services Among Adolescent and Young Adult Survivors of Pediatric Cancer. Journal of Adolescent and Young Adult Oncology. 2014;3(3):112–6. doi: 10.1089/jayao.2013.0036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hudson MM, Tyc VL, Srivastava DK, Gattuso J, Quargnenti A, Crom DB, et al. Multi-component behavioral intervention to promote health protective behaviors in childhood cancer survivors: The Protect Study. Medical and Pediatric Oncology. 2002;39(1):2–11. doi: 10.1002/mpo.10071. [DOI] [PubMed] [Google Scholar]
- 45.Kadan-Lottick NS, Robison LL, Gurney JG, Neglia JP, Yasui Y, Hayashi R, et al. Childhood cancer survivors’ knowledge about their past diagnosis and treatment: Childhood Cancer Survivor Study. Jama. 2002;287(14):1832–9. doi: 10.1001/jama.287.14.1832. [DOI] [PubMed] [Google Scholar]
- 46.Odo R, Potter C. Understanding the needs of young adult cancer survivors: a clinical perspective. Oncology (Williston Park) 2009;23(11 Suppl Nurse Ed):23–7. 33. [PubMed] [Google Scholar]
- 47.Mazzi C, Ganguly P, Kidd M. Healthcare applications based on software agents. Studies in health technology and informatics. 2001;84(Pt 1):136–40. [PubMed] [Google Scholar]
- 48.Miner AS1, Milstein A2, Schueller S3, Hegde R4, Mangurian C5, Linos E4. Smartphone-Based Conversational Agents and Responses to Questions About Mental Health, Interpersonal Violence, and Physical Health. JAMA Intern Med. 2016 May 1;176(5):619–25. doi: 10.1001/jamainternmed.2016.0400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Wesley KM, Fizur PJ. A review of mobile applications to help adolescent and young adult cancer patients. Adolescent Health, Medicine and Therapeutics. 2015;6:141–148. doi: 10.2147/AHMT.S69209. [DOI] [PMC free article] [PubMed] [Google Scholar]