

Abstract
Idiopathic pulmonary fibrosis (IPF) is a fatal lung disease characterized by the progressive and irreversible destruction of lung architecture, which causes significant deterioration in lung function and subsequent death from respiratory failure.
The pathogenesis of IPF in experimental animal models has been induced by bleomycin administration. In this study, we investigate an IPF-like mouse model induced by a double intratracheal bleomycin instillation. Standard histological assessments used for studying lung fibrosis are invasive terminal procedures. The goal of this work is to monitor lung fibrosis through noninvasive imaging techniques such as Fluorescent Molecular Tomography (FMT) and Micro-CT. These two technologies validated with histology findings could represent a revolutionary functional approach for real time non-invasive monitoring of IPF disease severity and progression. The fusion of different approaches represents a step further for understanding the IPF disease, where the molecular events occurring in a pathological condition can be observed with FMT and the subsequent anatomical changes can be monitored by Micro-CT.
Keywords: Immunology and Infection, Issue 134, Idiopathic pulmonary fibrosis (IPF), in vivo imaging, FMT, Micro-CT, lung disease, animal models, matrix metalloproteinases (MMPs), Bleomycin
Introduction
Idiopathic pulmonary fibrosis (IPF) is chronic lung disease with progressive decrease of lung functions that is unfortunately often fatal within four years of diagnosis1. The major features of IPF are extracellular matrix deposition and fibroblast proliferation, but the pathogenesis is not yet fully understood. The most supported hypothesis is that multiple cycles of lung injuries cause the destruction of alveolar epithelial cells that leads to alteration of the mesenchymal cell cycle proliferation, exaggerated accumulation of fibroblasts and myofibroblasts, and increased matrix production. Mediators involved in these processes such as matrix metalloproteinases (MMPs) have been found dysregulated in fibrosis development either in human IPF or in bleomycin-induced animal models. The uncontrolled MMP production leads to an unbalanced collagen deposition within the lung interstitium and alveolar space, mimicking abnormal wound repair1,2.
One of the main obstacles for drug discovery and development is the availability of accessible mouse models that mimic human pathogenesis and the disease phenotype. Different agents have been used to induce lung fibrosis in animal models: irradiation damage, administration of asbestos and silica, administration of fibrinogenic cytokines and bleomycin3,4; however bleomycin is the most used in mice, rats, guinea pigs, hamsters, rabbits5 or in large animals (non-human primates, horses, dogs and ruminants)6,7. Bleomycin is an antibiotic made by the bacterium Streptomyces verticillus8 and is used as an anti-cancer agent9. Pulmonary fibrosis is a common side effect of the drug and for this reason, it is used in experimental animal models to induce pulmonary fibrosis.
In bleomycin-induced lung fibrosis models, the fibrotic lesions occur 14 - 21 days after bleomycin administration. In the presented work, we used a new protocol to induce lung fibrosis in mice by double bleomycin intratracheal instillation. The bleomycin mouse model is very time consuming because new drugs need to be evaluated on established fibrotic lesions, and tested to distinguish their anti-fibrotic effects from anti-inflammatory effects.
Biochemical determination of collagen content, morphometrical and histological analysis were based on post mortem analysis, limiting the possibility to follow the pathogenesis of the disease in the same animal. Although these parameters were considered a gold standard for fibrosis evaluation, they did not provide any temporal or spatial distribution of the fibrotic lesion and preclude a way to investigate the process of disease progression.10
Recently, non-invasive imaging technologies have been applied to monitor airway remodeling, inflammation, and fibrosis progression in murine models: Magnetic Resonance Imaging (MRI), Micro Computer Tomography (Micro-CT), Fluorescence Molecular Tomography (FMT) and Bioluminescent (BLI)11,12,13,14,15,16,17,18,19,20,21. We propose a non-invasive imaging approach to monitor longitudinally lung fibrosis progression by FMT and Micro-CT at different time-points after a bleomycin challenge22.
Many pathways are involved in the establishment and development of fibrosis, and not much is known. Only a deeper understanding of these processes could translate to more drug targets that may transfer into the clinic. The ability to longitudinally monitor MMP activation by fluorescence molecular tomography coupled to the detection of lung parenchymal changes by Micro-CT might be used in the future to access the clinical response to treatment.
Protocol
All animal experiments described herein were approved by the intramural animal-welfare committee for animal experimentation of Chiesi Farmaceutici and ERASMUS MC under protocol number: EMC 3349 (138-14-07) complying with the European Directive 2010/63 UE, Italian D.Lgs 26/2014 and the revised "Guide for the Care and Use of Laboratory Animals"23.
NOTE: Prior to use, female inbred C57Bl/6 (7-8 weeks old) mice were acclimatized for at least 7 days to the local vivarium conditions (room temperature: 20-24 °C; relative humidity: 40-70%; 12-h light-dark cycle), having free access to standard rodent chow and softened tap water.
1. Intratracheal Treatment of Mice with Bleomycin
Prepare the equipment for the intra-tracheal instillation12,13,14.
Put the mice in the anesthetic chamber connected to an isoflurane vaporizer set at 2.5% mixed with oxygen. Check for depth of anesthesia by the lack of a toe-pinch response. The effect of the anesthesia occurred after 3-5 min.
Position the anesthetized mouse on the intubation platform, hanging it by its incisors placed on the wire.
Turn on the laryngoscope, take a pair of blunt ended forceps and use either the forceps or laryngoscope's tip to gently open the mouth.
Pull out the tongue and hold it to the side with forceps. Place the laryngoscope blade towards the back of the mouth until the opening of the trachea is visualized and keep the laryngoscope in place.
- With the other hand, insert the delivery tube connected to the end of the PE tubing into the trachea, rotating the three-way valve. Deliver 50 µL of bleomycin (0.020 µg/mouse). After instillation, quickly remove the tube from the trachea to prevent suffocation. Hold the mice upright for a few seconds.
- Administer bleomycin intratracheally at day 0 and repeat at day 4 (Figure 1).
Remove the mouse from the intubation platform and monitor the mouse for 30 min (the time needed to fully recover from anesthesia).
Perform in vivo imaging of the mice lungs by FMT and Micro-CT after double bleomycin instillation at day 7, 14, and 21.
2. In vivo Imaging by Fluorescence Molecular Tomography
NOTE: Beforehand, prepare a fresh stock solution of 6 nmol/mL of MMP sensitive fluorescent substrate 680 in saline solution (0.9% sodium chloride), and store protected from the light at 4 °C before use. It is stable for up to 6 months at 4 °C. Allow MMP imaging agent to equilibrate to room temperature before injecting into animals.
- Probe injection
- Prepare the equipment for intravenous injection of the MMP probe solution. Pre-warm water at 50 °C to heat the mouse tail.
- To firmly grasp the mouse scruff, take it by the tail and allow it to grip the cage lid. Holding the mice across the animal's shoulders, put the tail in a warm water beaker, for 4 to maximum 8 s thermal injury to prevent thermal injury to the tail skin. Check the veins swelling for easier visualization and needle insertion.
- During the injection procedure, put the mice into a plastic restrainer to keep it steady and pull the tail through a special hole in the back. Find the two caudal veins on either side of the tail; not the artery on the underside of the tail.
- Insert the needle (26G) of the 1 mL syringe into the vein. If the needle is correctly placed, injection will be easy and the probe solution will flow into the vessel.
- Inject the MMP probe solution at 10 mL/kg.
- Discard the needle. NOTE: The optimal imaging time point is 24 h after the MMP probe injection because it is the time required by the probe to be activated. If longitudinal studies are performed, the optimal re-injection time is 7 days, which allows for the complete clearance of the agent from the mouse.
- FMT imaging NOTE: Before starting, always remove the fur on and around the areas of the animal that are to be imaged, in this case the chest, to avoid scattering and absorbance in tissue.
- To anesthetize the mouse, put it in anesthetic chamber and turn the isoflurane dial to 2.5% for induction and 2% for maintenance.
- Initialize the data acquisition software and open a new study in the database for the experiment.
- Before starting the imaging with FMT, transfer the mouse into the imaging cassette. Place the anesthetized mouse in the middle of imaging cassette to optimally use the field of view of the FMT. Keep the mice flat, secure and gently compressed against both windows of the imaging cassette. Adjust the height by knobs on the cassette, and then slide it into the docking station.
- Click on subject in the scanning window and click preview to see the live image.
- Draw the scan region sufficiently large so that tissue surrounding the anticipated area of fluorescence is captured. Including a total of 25 scan points guarantees the lung region will be totally scanned.
- Once the ROI is drawn, first click add to reconstruction queue and then click Scan to image the mouse. Make sure that the correct laser at 680 nm is selected.
- When the image acquisition is completed, place the mouse back into its cage. Be sure it fully recovers from anesthesia.
- Quantify the picomoles of fluorescence in the Analysis window of the analysis software using the ROI tool and reduce the ROI around 700-800 mm3 on the signal coming from the lung region. Be careful to exclude the liver signal. Copy the ROI on the other subjects to have them similar in dimension and adjust their position in each animal image.
- Export images as jpg files.
3. In Vivo Imaging by Micro-CT
CAUTION: Before starting, always remove any metal jewelry or metal objects near the imaging area, to avoid scattering of x-rays.
NOTE: Radiation-induced lung fibrosis is a common finding during radiation induced lung injury24. Neither Micro-CT derived indices nor histological findings associated with lung fibrosis were present in saline treated control mice on day 21 subjected to four Micro-CT imaging sessions, indicating that the X-ray dose delivered to the animals during Micro-CT examinations was not sufficient to affect the findings.
Turn on the Micro-CT by pressing the green power button and launch the software to warm up the x-ray source. Use the small bore and the animal bed for mice imaging.
Create the database by clicking on New database for a new one and build the browser based on number of mice in the experiment, or click connecting to existing database to save the data to a previously created one.
Before starting the scanning, select the acquisition parameters in the software control window: X-ray tube voltage, 90 kV; CT X-ray tube current, 160 µA; Live X-ray tube current, 80 µA; FOV, 36 mm; No gating technique; Scan technique, High resolution 4 min.
Anesthetize the mice by inhalation of 3% isoflurane and place them on the bed inserted into the bore with a nose cone providing a constant supply of anesthetic. Immobilize the paws of the mice with tape on the bed to allow the chest to be exposed.
Slide the instrument door and turn on the Live Mode to see the mouse position in real time by pressing the capture button. Move the animal bed to align the chest with the field of view (FOV) using buttons directly located on the CT instrument. Center the scan on the mouse; if not adjust the position with left and right arrows located on the CT instrument.
Confirm optimal bed position by rotating the gantry by selecting 90° and clicking Set. Make sure that the region to image is fully inside the FOV.
Do not apply any gating technique and start the scan by clicking the CT Scan button. Click yes to the message that informs that the x-ray source will be turned on. NOTE: Once the x-rays are turned on, the orange lamp on top of the instrument will be illuminated and the sliding door will be impossible to open for the safety of the operator. Once the scan is finished, a new window of the 2D Viewer software appears showing the transaxial, coronal, and sagittal slice of the reconstruction.
Check the image quality and be sure not to have blurred images from movements due to the low level of anesthesia. If necessary, repeat the scan.
Place the animals back into the cage and be sure they fully recover from anesthesia.
4. Bronchoalveolar Lavage
Anesthetize animals with 3% isoflurane and sacrifice by bleeding from the abdominal aorta.
Use scissors to expose the thoracic cage and neck. Then expose the trachea and make a small incision to allow the BAL procedure to be performed with a 21-gauge lavage tube attached to a 1 mL syringe without the needle. Pay attention not to cut through the trachea.
To perform the BAL, fill the 1 mL syringe without a needle with 0.6 mL of sterile solution [10x Hank's balanced salt solution (HBSS); 100 mM ethylenediaminetetraacetic acid (EDTA); 1 mM 4-(2-hydroxy-ethyl)-1-piperazineethansulphonic acid (HEPES); distilled water].
Insert the lavage tube into the incision in the trachea and slowly inject and withdraw the solution 3 times, pausing on the third withdrawal to allow optimum collection of the BALF for subsequent analysis.
5. Histology and Histomorphometry
Expose and remove lungs, inflating them with a cannula through the trachea by gentle infusion with 0.6 mL of 10% neutral-buffered formalin and store the samples at room temperature for 24 h.
Dehydrate samples through different passages in increasing concentrations of alcohol solutions (60% ethanol for 1 h, 70% ethanol for 1 h, 90% ethanol for 1 h, 95% ethanol for 2 h, and 100% ethanol for 2 h) using an automatic tissue processor.
Place specimens in xylene for 2 h to make them translucent. At the end of dehydration, infiltrate samples in paraffin at 60 °C for 3 h and embed them in the automated processor.
Obtain 5 µm thick serial sections using a rotary microtome.
Deparaffinize and rehydrate slides in descending grades of ethanol and stain with Masson's Trichrome using an automatic tissue processor.
Manually focus on lung slices, scanning at 20X magnification using a slide scanner and capture digital images of entire lung sections using the viewing software with a resolution of 451 nm/pixel.
- Morphologically assess fibrotic lung injury by semi-quantitative and quantitative parameters as follows:
Representative Results
Spontaneous resolution of the lung fibrosis lesions observed three weeks after single bleomycin administration and moderate structural changes highlight the limits of this model. Only preventive treatment could be performed due to the narrow therapeutic window that does not represent clinical practice17.
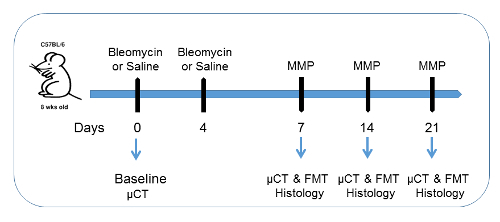
Here, we demonstrate that our protocol of double bleomycin intratracheal instillation is able to develop long lasting lung fibrosis in mice18. The experimental design is shown in Figure 119,20,21. The goal of this study is to look at lung fibrosis progression in mice with noninvasive imaging technologies. Bleomycin was intratracheally administered twice (at day 0 and 4; 1 mg/kg of bleomycin in 50 µL on each occasion). Twelve mice for each group were intratracheally challenged with the same volume of vehicle only at the same time as the bleomycin group to use as a control. For the assessment of fibrosis, a semi-quantitative histological analysis was done based on the Ashcroft scoring system.10
In the present work, we assessed lung fibrosis development in bleomycin-induced mouse model by using Micro-CT and FMT technologies in combination with classical histology. The noninvasive nature of imaging technologies represents real value for preclinical evaluation of lung fibrosis progression and the agreement found with the histology is an excellent step. Micro-CT imaging could play an important role in the quantification of lung parenchymal changes due to fibrotic lesions longitudinally.
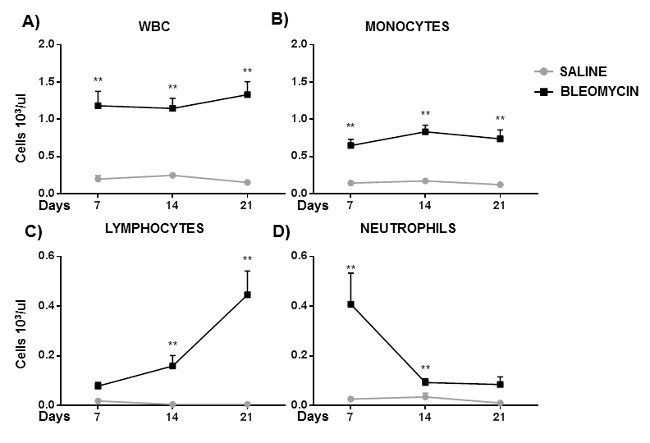
Histology pictures of the bleomycin treated group showed a pronounced pattern of fibrosis starting from day 7, mainly as single fibrotic masses, and progressed at day 14 to confluent conglomerates of substitutive collagen and remained unaltered until day 21 (Figures 2A-2C). Bleomycin treatment induced lung inflammation (Figure 3A), where the number of WBC was significantly higher in BALF of bleomycin treated mice at 7, 14, and 21 days compare to vehicle group. Interestingly, the lymphocyte and monocyte fractions were also increased at each time of sampling (Figures 3B-3C); in contrast, a significant increase of the neutrophil fraction has been observed at day 7 (Figure 3D).
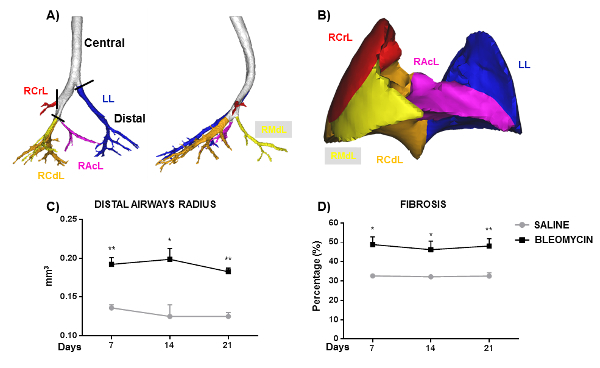
In this study, Micro-CT was used to monitor the lung parenchyma changes longitudinally. Progressive anatomical changes of the lung architecture at different time points of observation from baseline are clearly seen in Micro-CT projections (Figures 4A-4B). The airway radius in the distal part of the bronchial tree (Figures 5A and 5C)19,20,21 and total lung fibrosis percentage (Figures 5B and 5D) could quantify fibrosis progression. The fibrosis percentage quantification in bleomycin treatment group at day 7 (Figure 5D) was slightly overestimated if compared to histology scoring. This could be explained by a dual reaction of inflammation and fibrosis onset, making it hard to distinguish between the two symptoms. The airway radius and the percentage of fibrosis were selected from image processing of the Micro-CT projections for the quantification of the lung parenchymal changes (Figures 5C-5D)19,20,21. These Micro-CT parameters are very well in agreement with histological findings as shown in Figures 2A/2C.
Micro-CT imaging directly reflected the pathologic and therapeutic changes of lung parenchyma and FMT technology provided quantitative information more related to protein expression liked to IPF. For this study, we chose an MMP probe based on its relevance to IPF and we found specific MMPs activation in bleomycin treated mice (Figure 6)18. The role of MMPs has been investigated by injecting either vehicle or bleomycin treated mice with MMP activable fluorescent probes at selected time points. Twenty-four hours after injection, the mice were imaged by FMT revealing that fibrotic mice can activate the specific MMP fluorescent probe in vivo (Figures 6A-6D)18 and ex vivo (Figure 6E)18.
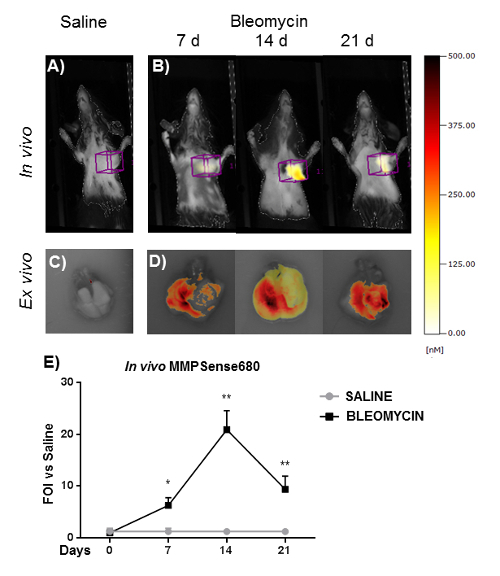
Figure 1: Experimental set up for bleomycin-induced mouse lung fibrosis. C57BL/6 female mice had either saline or bleomycin instilled intratracheally on two occasions, day 0 and 4. Mice were imaged by a Micro-CT scanner at baseline (day 0), 7, 14, and 21 days. Groups of 12 mice were sacrificed at 7, 14, and 21 days and their lungs were assessed for collagen deposition to correlate histological results with images obtained by µCT. This figure has been modified from the published article21. Please click here to view a larger version of this figure.
Figure 2: Histological analysis time course of bleomycin induced lung fibrosis in mice. (A) Quantification of lung fibrosis by Ashcroft score either vehicle or bleomycin treated mice at different time points. The experiment was repeated three times and each point represents the mean ± SEM of 12 animals. Statistical analysis has been performed by ANOVA followed by Tukey's test. *p< 0.05; **p< 0.01. (B) Ashcroft score frequency distribution allocated in mild, moderate, and severe subcategories. (C) Representative histology of Masson's Trichome stained mouse lung sections for intratracheally double instilled bleomycin or saline treated mice at 7, 14, and 21 days post treatment (magnification 10X, scale bar 200 µm). Please click here to view a larger version of this figure.
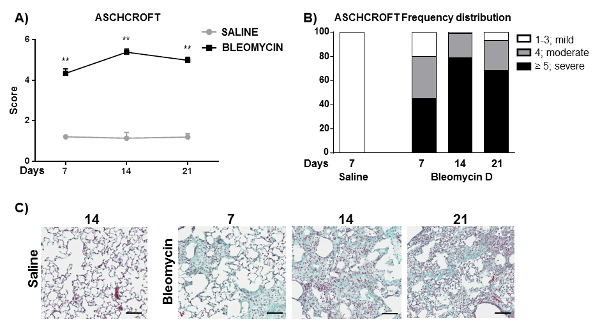
Figure 3: Cellular infiltration time course into the BALF of bleomycin induced lung fibrosis in mice. The (A) number of WBC, (B) Monocytes, (C) Lymphocytes, and (D) Neutrophils. Cells found in BALF were expressed as number of cells*103/µL. The experiment was repeated three times and each point represents the mean ± SEM of 9 animals. Statistical analysis has been performed by ANOVA followed by Dunnett's test. *p< 0.05; **p< 0.01. Please click here to view a larger version of this figure.
Figure 4: Longitudinal Micro-CT imaging projections of bleomycin-induced lung fibrosis and vehicle treated mice. (A) Micro-CT, bleomycin treated mouse and (B) Micro-CT, saline treated mouse Please click here to view a larger version of this figure.

Figure 5: Airways, fibrosis lung lobes quantification and segmentation based on repeated Micro-CT imaging. (A) Airways were divided into a central and distal part. (B) The distal part of the airways is the intrapulmonary tract used to identify and split into lung lobes as: Right Cranial Lobe (RCrL), Right Middle Lobe (RMdL), Right Caudal Lobe (RCdL), Right Accessory Lobe (RAcL), and Left Lung (LL). (C) Airway radius and (D) total lung fibrosis quantification either vehicle or bleomycin treated mice at different time points. Each point represents the mean ± SEM of 5 animals, for a total of 30 mice. Statistical analysis has been performed by ANOVA followed by Dunnett's test. *p< 0.05; **p< 0.01. This figure has been modified from the published article21. Please click here to view a larger version of this figure.
Figure. 6. Time course of fluorescence signal measured by FMT inbleomycin induced lung fibrosis mice. In vivo (A and B) and ex vivo (C and D) FMT representative images of mice injected with MMP probe treated with vehicle or with bleomycin. (E) The total amount of lung fluorescence signal was automatically calculated by FMT image software. The experiment was repeated three times and each point represents the mean ± standard deviation of 9 animals. Statistical analysis has been performed by ANOVA followed by Dunnett's test. *p< 0.05; **p< 0.01. This figure has been modified from the published article18. Please click here to view a larger version of this figure.
Discussion
Despite many research groups focusing on developing new drugs to treat IPF, at the moment only two are available for patients. There is an urgent medical need to find more effective therapies7 because only lung transplantationis able to prolong survival of 4-5 years26. The essential prerequisite for translational medicine and development of new drugs is the availability of an animal model that mimics the features of IPF and in which interventional studies are predictive of success in the clinic. However, the usefulness of the existing pulmonary fibrosis animal models is still controversial27. We develop a new mouse model of lung fibrosis that requires a double instillation of bleomycin as described in Figure 118. Imaging technologies are powerful tools to visualize disease progression, and pharmacological response to treatment. This animal model better recapitulated the human features of IPF and noninvasive technologies could create a bridge between preclinical settings and clinical practice27.
However, to obtain robust and reproducible data, some steps are crucial. The intratracheal instillation must be performed when the mice are fully anesthetized, using a standardized procedure. Micro-CT acquisition requires very accurate monitoring of the anesthesia, because the CT projections are gated by the respiratory frequency. Before imaging, check that the mice have the same depth of anesthesia. A very important step for optical imaging by FMT is depilation. Before starting, always remove the fur on and around the chest, to avoid scattering and absorbance in tissue. The probe injection needs to be corrected by the body weight of the animal.
The possibility to investigate and quantify a specific molecular read-out with anatomical changes in the same mice at different time points represents a huge step in understanding fibrosis development, an obvious advance for functional as well as pharmacological studies.
This multimodal imaging approach is a smart tool to evaluate drug efficacy, providing much more information compared to terminal assessment, translating in a more efficient drug discovery process.
Disclosures
The authors declare that they have no competing interests.
Acknowledgments
The authors would like to thank Dr. Daniela Pompilio and Roberta Ciccimarra for technical help.
References
- Wynn TA. Integrating mechanisms of pulmonary fibrosis. J. Exp. Med. 2011;208(7):1339–1350. doi: 10.1084/jem.20110551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wynn TA, Ramalingam TR. Mechanisms of fibrosis: therapeutic translation for fibrotic disease. Nat. Med. 2012;18(7):1028–1040. doi: 10.1038/nm.2807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore BB. Animal models of fibrotic lung disease. Am J Respir Cell Mol Biol. 2013;49(2):167–179. doi: 10.1165/rcmb.2013-0094TR. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ackermann M, et al. Effects of nintedanib on the microvascular architecture in a lung fibrosis model. Angiogenesis. 2017. [DOI] [PMC free article] [PubMed]
- Moore BB, Hogaboam CM. Murine models of pulmonary fibrosis. Am J Physiol Lung Cell Mol Physiol. 2008;294(2):152–160. doi: 10.1152/ajplung.00313.2007. [DOI] [PubMed] [Google Scholar]
- Organ L, et al. A novel segmental challenge model for bleomycin-induced pulmonary fibrosis in sheep. Exp Lung Res. 2015;41(3):115–134. doi: 10.3109/01902148.2014.985806. [DOI] [PubMed] [Google Scholar]
- Organ L, et al. Structural and functional correlations in a large animal model of bleomycin-induced pulmonary fibrosis. BMC Pulm Med. 2015;15:81. doi: 10.1186/s12890-015-0071-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shen B, Du L, Sanchez C, Edwards DJ, Chen M, Murrell JM. Cloning and characterization of the bleomycin biosynthetic gene cluster from Streptomyces verticillus ATCC15003. J Nat Prod. 2002;65(3):422–431. doi: 10.1021/np010550q. [DOI] [PubMed] [Google Scholar]
- Yu Z, et al. Targeted Delivery of Bleomycin: A Comprehensive Anticancer Review. Curr Cancer Drug Targets. 2016;16(6):509–521. doi: 10.2174/1568009616666151130213910. [DOI] [PubMed] [Google Scholar]
- Ashcroft T, Simpson JM, Timbrell V. Simple method of estimating severity of pulmonary fibrosis on a numerical scale. J Clin Pathol. 1988;41(4):467–470. doi: 10.1136/jcp.41.4.467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stellari F, et al. In vivo imaging of the lung inflammatory response to Pseudomonas aeruginosa and its modulation by azithromycin. J Transl Med. 2015;13:251. doi: 10.1186/s12967-015-0615-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stellari F, et al. In vivo monitoring of lung inflammation in CFTR-deficient mice. J Transl Med. 2016;14(1):226. doi: 10.1186/s12967-016-0976-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stellari FF, et al. In vivo imaging of transiently transgenized mice with a bovine interleukin 8 (CXCL8) promoter/luciferase reporter construct. PloS one. 2012;7(6):39716. doi: 10.1371/journal.pone.0039716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stellari FF, et al. Enlightened Mannhemia haemolytica lung inflammation in bovinized mice. Vet Res. 2014;45:8. doi: 10.1186/1297-9716-45-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tassali N, et al. MR imaging, targeting and characterization of pulmonary fibrosis using intra-tracheal administration of gadolinium-based nanoparticles. Contrast Media Mol Imaging. 2016;11(5):396–404. doi: 10.1002/cmmi.1703. [DOI] [PubMed] [Google Scholar]
- Ma X, et al. Assessment of asthmatic inflammation using hybrid fluorescence molecular tomography-x-ray computed tomography. J Biomed Opt. 2016;21(1):15009. doi: 10.1117/1.JBO.21.1.015009. [DOI] [PubMed] [Google Scholar]
- Van de Velde G, et al. Longitudinal micro-CT provides biomarkers of lung disease that can be used to assess the effect of therapy in preclinical mouse models, and reveal compensatory changes in lung volume. Dis Model Mech. 2016;9(1):91–98. doi: 10.1242/dmm.020321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stellari FF, et al. Heterologous Matrix Metalloproteinase Gene Promoter Activity Allows In Vivo Real-time Imaging of Bleomycin-Induced Lung Fibrosis in Transiently Transgenized Mice. Front Immunol. 2017;8:199. doi: 10.3389/fimmu.2017.00199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hellbach K, et al. X-ray dark-field radiography facilitates the diagnosis of pulmonary fibrosis in a mouse model. Sci Rep. 2017;7(1):340. doi: 10.1038/s41598-017-00475-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhou Y, et al. Noninvasive imaging of experimental lung fibrosis. Am J Respir Cell Mol Biol. 2015;53(1):8–13. doi: 10.1165/rcmb.2015-0032TR. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruscitti F, et al. Longitudinal assessment of bleomycin-induced lung fibrosis by Micro-CT correlates with histological evaluation in mice. Multidiscip Respir Med. 2017;12:8. doi: 10.1186/s40248-017-0089-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stellari F, et al. Monitoring inflammation and airway remodeling by fluorescence molecular tomography in a chronic asthma model. J Transl Med. 2015;13:336. doi: 10.1186/s12967-015-0696-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guide for the Care and Use of Laboratory Animals, 8th ed. Washington DC: National Research Council; 2011. [Google Scholar]
- Meganck JA, Liu B. Dosimetry in Micro-computed Tomography: a Review of the Measurement Methods, Impacts, and Characterization of the Quantum GX Imaging System. Mol Imaging Biol. 2016. [DOI] [PMC free article] [PubMed]
- Hubner RH, et al. Standardized quantification of pulmonary fibrosis in histological samples) BioTechniques. 2008;44(4):507–514. doi: 10.2144/000112729. [DOI] [PubMed] [Google Scholar]
- King TE, Pardo A, Selman M. Idiopathic pulmonary fibrosis. Lancet. 2011;378(9807):1949–1961. doi: 10.1016/S0140-6736(11)60052-4. [DOI] [PubMed] [Google Scholar]
- De Langhe E, et al. Quantification of lung fibrosis and emphysema in mice using automated micro-computed tomography. PloS one. 2012;7(8):43123. doi: 10.1371/journal.pone.0043123. [DOI] [PMC free article] [PubMed] [Google Scholar]