

Abstract
Adult T-cell lymphoma/leukemia (ATLL) is a rare tumour of T-lymphocytes that is associated with human T-lymphotrophic virus type 1 (HTLV-1) infection as well as severe/refractory hypercalcaemia. Human immunodefficiency virus type 1 (HIV-1) infected individuals are at increased risk of acquiring co-infection with HTLV-1. We present the case of a 37 -year -old HIV-1 positive and antiretroviral therapy naive woman who was admitted to the ICU with delirium, a generalised maculopapular rash, severe hypercalcaemia of 4.48 mmol/L (normal < 2.7 mmol/L) and a positive HTLV-1 serology. The diagnosis of ATLL was confirmed on biopsy. Her hypercalcaemic state proved refractory to conventional therapy, but was rapidly corrected with a modified haemodialysis technique using a dialysate with a low low-calcium concentration.
INTRODUCTION
Human T-lymphotropic virus type 1 (HTLV-1), is an oncogenic virus that was first isolated and described in 1980, although it has likely been a pathogen in humans since ancient times [1]. Severe/refractory hypercalcaemia is a common presenting feature in individuals with occult adult T-cell lymphoma/leukaemia (ATLL), a malignancy of mature CD4 T-lymphocytes that invariably occurs in individuals with underlying HTLV-1 infection [2]. HTLV-1 and human immunodeficiency virus type 1 (HIV-1) are both retroviruses that infect CD4 lymphocytes and also share similar routes of transmission [3]. The prevalence of HTLV-1 infection is reportedly higher amongst HIV-1 positive than HIV-1 negative individuals [4]. According to the latest UNAIDS global update, there are 36.7 million people living with HIV around the world, with 2.1 million new infections in the year 2015 [5]. Although the prevalence of ATLL amongst individuals residing in HIV-1 seroprevalent regions such as sub-Saharan Africa is unknown, it is likely relatively higher. We present a case of severe/refractory hypercalcaemia in an adult patient with ATLL and HTLV-1/HIV-1 co-infection.
CASE REPORT
A 37-year-old HIV-1 positive, antiretroviral therapy naive woman was admitted to the ICU with a history of a generalized maculopapular rash, joint pains, pyrexia, fatigue and delirium. She had been diagnosed with HIV-1 infection in 2006 and as per local guidelines at the time was never initiated on antiretroviral therapy as her CD4+ lymphocyte count had always been >500 cells/μl at regular clinic follow up. On examination, she appeared ill with a pyrexia of 39.1°C and a generalized maculopapular rash (Fig. 1). Her knee, elbow and ankle joints were markedly swollen. She was also found to have axillary and inguinal lymphadenopathy, a 4 cm splenomegaly but no hepatomegaly. Except for features in keeping with delirium, no other abnormal neurological signs were noted. On this admission she had a CD4+ cell count of 616 cells/μl, a HIV viral load of 102 000 copies/mL and her HTLV-1 serology also tested strongly positive. Except for a markedly raised serum calcium level of 4.48 mmol/L, the rest of her laboratory work-up including full blood count, electrolytes, renal and liver function test, blood and urine culture, autoimmune screen, serum protein electrophoresis, serum angiotensin converting enzyme (S-ACE), parathyroid hormone (PTH) assay, beta-2 microglobulin, urinary Bence-Jones protein, joint fluid analysis and a nasopharangeal swab for the detection of respiratory viruses were unremarkable. A full body CAT scan showed extensive lymphadenopathy in the axillary, inguinal, pelvic and para-aortic regions. Radio-isotopic bone scanning showed increased uptake in the juxta-articular areas of the elbow and knee joints. Histology of a skin lesion biopsy showed a vasculitic infiltration of abnormal looking T cells, whilst lymph node biopsy and bone marrow aspiration and trephine specimens confirmed the diagnosis of acute ATLL. Her hypercalcaemia initially proved refractory to stepwise conventional calcium lowering therapy that included large volume saline diuresis (normal saline at 200 mL/h × 24 h, then 120 mL/h × 48h), loop diuretics (80 mg of furosemide 12h × 3 days), corticosteroids (100 mg of hydrocortisone 8h × 3 days) and intravenous bisphosphonate therapy (4 mg of zolendronic acid over 15 min × 1 dose). On the fifth day, due to a lack of improvement in the degree of hypercalcaemia and her persistent delirium, she was initiated on a modified SLED (slow low efficiency haemodialysis) regimen with a low calcium (1 mmol/L) containing dialysate. After receiving 4 h of SLED on Day 5 and the same on Day 6, her serum calcium level had corrected to within normal limits and her delirious state had dramatically improved. Upon stabilization of her condition in the ICU, she was transferred to the oncology department where chemotherapy and combination antiretroviral therapy (zidovudine/lamivudine/efavirenz) were initiated. Unfortunately she demised a month later from chemotherapy associated neutropenia and septic shock.
Figure 1:
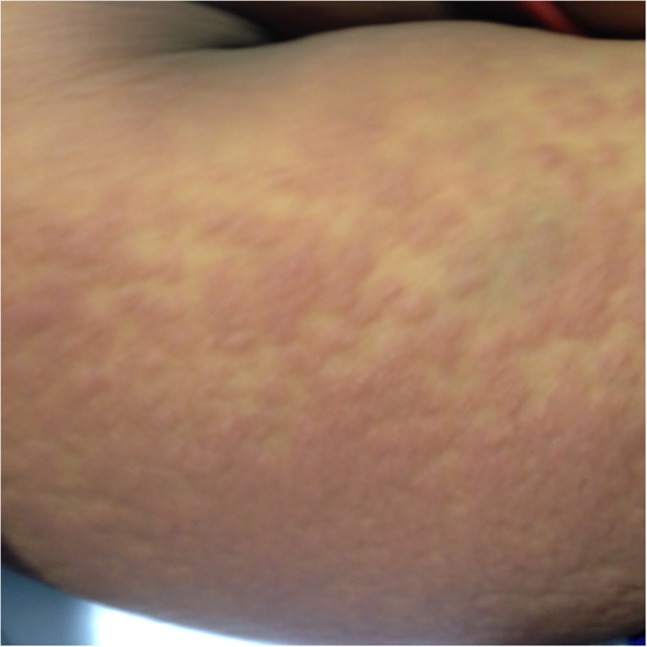
maculopapular rash on right forearm. The rash was diffuse and involved the entire body
DISCUSSION
The tetrad presentation of ATLL, HTLV-1, severe/refractory hypercalcaemia and HIV-1 is likely underreported, mostly due to the fact that HTLV-1 is seldom considered for investigation in HIV-1 infected individuals [4]. Although a handful of case series and case reports describing the presentation of HTLV-1, ATLL and hypercalcaemia have been reported in the literature [2, 6], the prevalence of this presentation in HIV co-infected individuals is not known.
Eastern and Southern African countries alone house 19 million individuals with HIV infection, which is more than half the global HIV burden [5]. Various studies have reported higher prevalence’s of HTLV-1 co-infection amongst HIV-1 positive individuals with a co-prevalence of both organisms in up to 28% of individuals with HIV infection [4, 7].
Although most individuals with HTLV-1 infection will remain asymptomatic throughout their life, it is estimated that <5% will progress to develop ATLL [8]. Severe/refractory hypercalcaemia is frequently the presenting feature in up to 70% of individuals with occult ATLL and has also been associated with early mortality [9]. The underlying mechanisms responsible for ATLL associated hypercalcaemia include an over-expression of receptor activator of nuclear factor kappa B ligand (RANKL), increase in serum macrophage colony-stimulating factor (M-CSF) levels, bony infiltration of the malignancy itself and secretion of PTH-related peptide (PTH-rP) by the tumour [10].
Similar to our finding, other case reports and patient series have shown that the stepwise implementation of conventional calcium lowering therapy including saline dieresis and the administration of furosemide, glucocorticosteroids or intravenous bisphosphonates are ineffective in correcting calcium levels [2]. In our patient, calcium levels were rapidly corrected with haemodialysis using a low calcium concentrate dialysate (1 mmol/L). This also resulted in dramatic improvement of her delirious mental state. The medical literature is rather scant with regards consensus guidelines on the use of haemodialysis in the management of refractory hypercalcaemia. Denosumab, a fully humanized monoclonal antibody has recently shown promise in the management of refractory hypercalcaemic states [11].
In conclusion, in the HIV-1 infected individual presenting to the ICU with severe/refractory hypercalcaemia, occult HTLV-1 associated ATLL must be considered as part of the differential diagnosis.
CONFLICT OF INTEREST STATEMENT
The authors’ hereby certify that this submission is not under publication consideration elsewhere, and is free of conflict of interest.
FUNDING
There is no source of funding to declare.
ETHICAL APPROVAL
Not required.
CONSENT
Informed consent was obtained from the patient to make use of patient data and photographs/images for publication purposes.
AUTHOR CONTIBUTION STATEMENTS
Laher A.E.: guarantor of the manuscript and responsible for drafting, writing, review and incorporating co-author feedback, revision, and final approval of the submission. Motara F.: contributed to the drafting, writing, review, revision and approval of the article. Moolla M.: contributed to the drafting, writing, review, revision and approval of the article. Ebrahim O.: contributed to the writing, review, revision of the article for important intellectual content, and approval of the article.
REFERENCES
- 1. Poiesz BJ, Ruscetti FW, Gazdar AF, Bunn PA, Minna JD, Gallo RC. Detection and isolation of type C retrovirus particles from fresh and cultured lymphocytes of a patient with cutaneous T-cell lymphoma. Proc Natl Acad Sci USA 1980;77:7415–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Edwards CMB, Edwards SJE, Bhumbra RP, Chowdhury TA. Severe refractory hypercalcaemia in HTLV-1 infection. J R Soc Med 2003;96:126–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Mazanderani AH, Ebrahim O. Progressive HIV infection in the presence of a raised CD4+ count: HIV/HTLV-1 co-infection. South African J HIV Med 2013;14:92–4. doi:10.7196/SAJHIVMED.904. [Google Scholar]
- 4. Nasir IA, Ahmad AE, Emeribe AU, Shehu MS, Medugu JT, Babayo A. Molecular detection and clinical implications of HTLV-1 infections among antiretroviral therapy-naïve HIV-1-infected individuals in Abuja, Nigeria. Virology 2015;6:17–23. doi:10.4137/VRT.S35331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Unaids Global AIDS Update 2016 2016. http://www.unaids.org/sites/default/files/media_asset/global-AIDS-update-2016_en.pdf (29 June 2017, date last accessed).
- 6. Naik S, Kodali S, Agheli A, Dumlao T, Singh V, Plummer K, et al. HTLV-1 adult T cell leukemia-lymphoma presenting with refractory hypercalcemia, cranial neuropathy and diagnosis by flow cytometry and cytogenetic findings. Blood 2015;110:3864. [Google Scholar]
- 7. Bessong PO, Mathomu LM. Seroprevalence of HTLV1/2, HSV1/2 and Toxoplasma gondii among chronic HIV-1 infected individuals in rural northeastern South Africa. Afr J Microbiol Res 2010;4:2587–91. [Google Scholar]
- 8. Matutes E, Catovsky D. Leukaemia, 3rd edn Oxford: Blackwell Scientific Publications, 1998. [Google Scholar]
- 9. Hagler KT, Lynch JW. Paraneoplastic manifestations of lymphoma. Clin Lymphoma 2004;5:29–36. [DOI] [PubMed] [Google Scholar]
- 10. Nosaka K, Miyamoto T, Sakai T, Mitsuya H, Suda T, Matsuoka M. Mechanism of hypercalcemia in adult T-cell leukemia: overexpression of receptor activator of nuclear factor kappaB ligand on adult T-cell leukemia cells. Blood 2002;99:634–40. doi:10.1182/blood.V99.2.634. [DOI] [PubMed] [Google Scholar]
- 11. Diel IJ, Body J-J, Stopeck AT, Vadhan-Raj S, Spencer A, Steger G, et al. The role of denosumab in the prevention of hypercalcaemia of malignancy in cancer patients with metastatic bone disease. Eur J Cancer 2015;51:1467–75. doi:10.1016/j.ejca.2015.04.017. [DOI] [PubMed] [Google Scholar]