

Abstract
Under the concept of meridian channels that belongs to traditional Chinese medicine, BIOCERAMIC Resonance (BR) has already been applied to many clinical medical research projects with functions mimicking of traditional acupuncture. Forty-five patients were recruited with chronic sleep disorders; 36 patients were given, applied to the device with BIOCERAMIC material and sound rhythm on chest skin surface; 9 patients were included as controls. All study participants completed a sleep pattern and quality of life questionnaire (assessment on psychological and physical causes of sleep disturbances), which was repeated before, during and after treatment. Electroencephalograph (EEG) recordings were analyzed before, during and after treatment. Functional MRI (fMRI) was also used for demonstration of BR effect for another 8 candidates. During the first 3 days of treatment, sleep quality improved in all 36 patients especially to psychological reasons; in 91.7% (33/36) treatment was associated with an elevation in the beta spectrum of the EEG (at 15–27 Hz). The result of fMRI found corresponding cerebral and cerebellar areas of activation and deactivation. BIOCERAMIC Resonance can improve sleep disorder due to psychological causes, with transient alter brain wave activity and functional activation on specific locations of brain.
Keywords: EEG, BIOCERAMIC, Sound rhythm, Sleep disturbance, fMRI
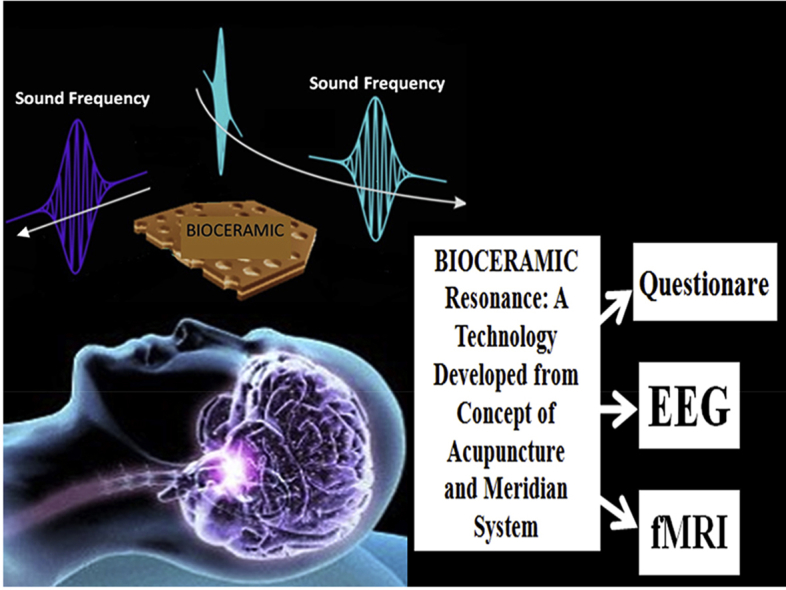
Graphical abstract
BIOCERAMIC Resonance is a new technology of using concept of acupuncture from traditional Chinese medicine. No past study is reported for a similar non-invasive and convenience therapy for sleep disturbance. Our study was approach by using questionaire, EEG and fMRI to evaluate the possible effect of BIOCERAMIC Resonance on sleep disturbance and brain physiology.
1. Introduction
The rationale to conduct this research is due to our clinical observation and impression of beneficial effect on sleep quality, when our candidates were received BIOCERAMIC treatment. Thus, we were decided to perform a study to assess the possible improvement of sleep disorder by BIOCERAMIC Resonance.
Sleep disorder, such as disrupted and restricted sleep, is a common problem for many people worldwide. Sleep disorder may be related to disturbances of the autonomic nervous system, can affect mental and physical wellbeing and the ability to work and interact in social relationships.1, 2 Insomnia may be a symptom of other diseases, but untreated insomnia can lead to psychological distress, it may also cause clinical conditions of anxiety and depression.3 Sleep disorder may also be a risk factor for cardiovascular disease and increased mortality.4 In Asian countries, insomnia is one of the most prevalent health disorders, reported by 21.4% of the total population in Japan,5 17% of the population in Korea,6 and more than 25% of the Taiwanese adult population.7 Difficulty of initiating sleep is the most common type of insomnia (14.6%), followed by early morning awakening (13.9%) and difficulty maintaining sleep (13.4%).7 The prevalence of use of any drug treatment for sleep disorders (including antidepressants, mood stabilizers, and anxiolytic-hypnotic drugs) has increased to more than 12.0% of the population in Taiwan for the past decade.8 The overuse of anxiolytic, hypnotic and sedative medications leads to side effects that cause public health problems.9, 10
Alternative treatments for insomnia in Chinese populations include Chinese herbs and acupuncture, whereas in Western countries psychological and behavioral approaches are more likely to be used.11, 12 Stimulation of acupuncture points or meridian channels, is a form of complementary medicine, includes several procedures to stimulate defined anatomical points. Although usually associated with the use of needles, acupuncture techniques can also include the use of magnets, low-power lasers, heat, ultrasound, manual pressure and electrical stimulation (electro-acupuncture). The application of BIOCERAMIC material includes an unexplained phenomenon of biological effect can be transmitted by sound wave and light propagation.7 In the past, we had conducted preclinical and clinical studies on the properties and applications of LED emitted light to pass through BIOCERAMIC material, including change of skin's electricity conductance properties, when applied to traditional acupuncture points.13, 14, 15 We have previously undertaken preclinical and clinical studies which have shown that the application of BIOCERAMIC materials promotes the microcirculation in patients13 and upregulates calcium-dependent nitric oxide and calmodulin in cell lines in vitro16 through calcium-dependent nitric oxide synthase.16, 17 In a series of recent clinical studies, we found the application of BIOCERAMIC materials reduced neck muscle stiffness, relieved musculoskeletal disorders, and improved the recovery of resting cardiac and respiratory rates following exercise.18, 19 The application of BIOCERAMIC materials has been shown to increase parasympathetic activity.20, 21
About BIOCERAMIC material, it is produce a weak energy field with no ionized radiation, which is enhanced and propagated through sound wave. BICOERAMIC material was proven to have weakening effects on hydrogen bonds and can alter the characteristics of liquid water.22, 23, 24 Furthermore, significant findings of the effects of BIOCERAMIC in different cell experiments, animal experiments and human trials, particularly in the promotion of microcirculation, were also found and reproduced.16 Based on Wang's deduction, the energy of a twelfth frequency is the sum of the energies of the eleven harmonic frequencies.21, 25 According to series of publications by Wang et al, the harmonic rhythmic sound frequencies of the heartbeat are the main frequency components of the propagated pressure wave and correspond to the twelve meridian channels of TCM. Acupuncture points and meridian channels are thought to be closely related to microcirculation.16, 21 BIOCERAMIC Resonance is the technology of combining sound waves using specific frequency beats in conjunction with our proprietary BIOCERAMIC material which offers a new kind of clinical application on traditional Chinese medicine.21 Described in our previous publication, candidates received BIOCERAMIC Resonance with rhythmic sound set at different tempo output that designed for resonance with aforementioned harmonic rhythmic sound frequencies of the heartbeat that corresponding to three dimension standing waves that what we believed as twelve meridian channels of TCM.14, 15, 21, 26 During the rhythmic sound tempo being resonance with the specific standing wave arise from harmonic rhythmic sound frequency of heartbeat, it intensify the energy propagation of energy field of BIOCERAMIC. Under operation BIOCERAMIC Resonance, candidates may experience “Propagated Sensation along Meridians” (PSM), our results seem to suggest that BIOCERAMIC Resonance stimulates the twelve main meridian channels according to TCM.14, 15, 21, 26
Our previous publication has already proven that the BIOCERAMIC Resonance device can facilitate microcirculation and elicited ‘propagated sensation along meridians’ (PSM), under the concept of traditional Chinese medicine (TCM). Beside, candidates with insomnia, migraine, anxiety, benign facial tremor, low back pain, muscular paralysis, lower leg edema and poor wound healing of lower extremity, were clinical improved.14, 15, 21, 26 The purpose of this study is to find the possibility of clinical benefit of BIOCERAMIC Resonance on sleep disturbance, assess by questionnaire, EEG and fMRI.
2. Methods
2.1. Characteristics and use of BIOCERAMIC Resonance (BIOCERAMIC material with sound rhythm)
The BIOCERAMIC powder used in this study (obtained from the Bioenergy Laboratory, Bioenergy Development Ltd, Taoyuan, Taiwan) was composed of microscopic particles produced from several types of elemental oxides. BIOCERAMIC powder13, 14, 15, 16, 17, 18, 19, 20, 21 was used as 10% of a mixture with silicone rubber (Bioenergy Development Ltd, Taoyuan, Taiwan)to produce a membrane with a sponge-like density, capable of sound transmission. To choose the suitable frequency for our experiment, we reviewed previous articles and studies on the effects of different frequencies. A study by G. Rasmussen found that sound rhythm from 1 to 20 Bps are the most effective.27 We selected 10 Bps (mean value of 1–20 Bps) as the first sound rhythmic setting to prove our BIOCERAMIC Resonance device for this study to investigate the effects on patients with poor sleep quality.
BIOCERAMIC Resonance is the device sound rhythm generator producing 10 Bps with 10% BIOCERAMIC material mixed with silicone rubber and was capable of producing BIOCERAMIC Resonance effect. The rhythmic vibration source was at about 30 cm above the skin surface of the chest and the average sound level was 50 dB.21
2.2. Patients studied
The participants we wish to collect were patients who suffer sleep disturbance, not limited to insomnia, narcolepsy, cataplexy or sleep walking & night terrors. Patients were excluded who were being medications (eg. sedative or hypotics). All patients signed informed consents to participate in this study. The study protocol was approved by the Human Subjects Ethics Committee at the Taipei Hospital (Ministry of Health and Welfare), New Taipei City, Taiwan (approval number: TH-IR-0014-0001). Because of limitation on funding resource, we allowed 45 participants in this study, who were claimed of suffering sleep disorders. There were 30 female and 15 male, with an average age of 47.4 years old (range from 25 to 68 years old), were basically suffered of insomnia. We decide the ratio of 'experimental group to control group' as '4 to 1'; thus, 36 patients underwent BIOCERAMIC with 10 Bps and 9 control subjects received sound rhythm (SR) at 10 Bps without BIOCERAMIC. They were arranged to perform sleep-quality assessment and electroencephalography (EEG) data recording. Eight male participant were received functional Magnetic Resonance Imaging (fMRI), but because of technically limitation, he was treated without and with BIOCERAMIC under circumstance of ‘pulse sequence’ sound vibration created by MRI device.
2.3. Sleep-quality assessment by questionnaire
Modification from ‘Insomnia Severity Index’ and ‘Pittsburgh Sleep Quality Index’, we developed a self-assessment questionnaire, which was found more suitable to collect data on Taiwanese citizen, to use for quantify sleep disturbance patterns in the patients studied. The initial questionnaires required information on sleep patterns (include assessment on psychological and physical causes of sleep disturbances) for the 3 days prior to the start of the study, to provide baseline sleep patterns (Table 1) prior to treatment with BIOCERAMIC Resonance with SR at 10 Bps (BR10). Experiment 1 was the completion of study questionnaires 3 days after receiving the first BR10. Experiment 2 was the completion of study questionnaires 3 days later. Experiment 3 was the completion of study questionnaires after a further 3 days. The questionnaires included the following nine questions (Table 1). Statistical analysis was done to compare the results of the study population (36 patients) with the control population (9 patients) using the Kendall rank correlation coefficient, or tau test, which is a non-parametric hypothesis test to determine the dependence of severity of sleep disturbance and response to treatment with BR10.21, 23
Table 1.
Questionnaire used for sleep quality assessment.
|
Remarks: Each question was answered as: none; occasionally; often; always.
2.4. Electroencephalography (EEG) data recording
The EEG recordings of 36 patients who received BR10 and 9 control subjects, who received plain SR at 10 Bps alone, were all performed using standard EEG scalp leads and monitoring. Candidates were told not allowed eye opening throughout the whole period of EEG recordings. EEG recordings were analyzed for three sessions for each patient: 15 min before treatment, 60 min during treatment, and 15 min after treatment. Statistical comparison of the results was performed for the two groups, the 36 patients who received BR10 and the 9 control subjects who received sound rhythm at 10 Bps alone, using Fisher's exact t-test.28, 29 The Embla 7000 digital polysomnographic recorder (Broomfield, CO, USA) and RemLogic software (Middleton, WI, USA) were used to record EEG and PSG data. The recording montage consisted of six EEG derivations (C3, C4, C4-M1, C3-M2, O1-M2, O2-M1). Signals were digitized at a rate of 1 kHz and amplified using 0.1–30 Hz analog band-pass filtering. EEGs were recorded during three time periods: 15 min before treatment, 60 min during treatment and 10 min after treatment. The EEG studies were performed in the daytime. Artifacts resulting from eye movements, blinks, muscle noise, and line noise were estimated by independent component analysis (ICA). Event-related potentials (ERPs) and event-related spectral perturbations (ERSPs) were computed using the EEGLAB MATLAB toolbox.30 In this computation method, time-frequency analysis was applied to EEG signals using the Morlettrans formation wavelet. Calculation of the individual frequency bands (delta, theta, alpha, and beta) was performed.
2.5. EEG analysis of curve patterns from 0 to 30 Hz, and of different band frequencies
The frequency spectra of the individual EEG results, in the ranges 1–4 Hz, 4–7 Hz, 7–12 Hz, 12–20 Hz, 20–25 Hz, 25–30 Hz, were analyzed for possible significant differences by comparing EEGs before, during and after BR10 treatments for the experimental and control groups.
2.6. Functional Magnetic Resonance Imaging (fMRI) demonstrates difference of control and experimental groups
All brain imaging was conducted with a 3.0 T MRI system (United Imaging 3.0 T TX; Shanghai, China). After localizing images in three planes, 1-weighted images were acquired for anatomical reference. Transverse blood oxygenation level-dependent BOLD MRI images were obtained using gradient-echo planar imaging (EPI). The corresponding Imaging parameters were as follows: repetition time (TR) 3000 ms, echo time (TE) = 35 ms, matrix size = 96 × 96, reconstructed matrix size = 128 × 128, flip angle = 90°, field of view 230 × 230 mm, number of slices = 24, with 5-mm thickness and no gaps. All analyses were performed with SPM8 software (Statistical Parametric Mapping, http://www.fil.ion.ucl.ac.uk/spm/). Voxel-based individual task-related activation was evaluated.31, 32 There were 8 candidates (male: 6; female: 2; average age: 22.4 years old) received fMRI without BIOCERAMIC silicon sheet placement who were able to hear the sound of ‘BOLD’ pulse sequence for 5 min, as control group. Experimental group of the same candidates, who were received fMRI after the control study, with additional placement of a silicon sheet (mixed with 10% BIOCERAMIC material) for treatment at skin portion of bilateral temporal regions. The effect of BIOCERAMIC Resonance was produced from combing BIOCERAMIC silicon sheet the sound of ‘BOLD’ pulse sequence for another 5 min.
3. Results
3.1. Result of sleep quality assessment by questionnaire
Table 2 shows the Kendall tau rank correlation test analysis of questionnaire data, which shows a significant improvement (p < 0.05) for the group of patients who had the greatest adverse sleep scores (worst sleep quality). The study findings were significant for improvement in the responses to Q1, Q2, Q3, Q4, Q5 and Q7 (p < 0.05); but not for responses to Q6 (physical pain or discomfort that interferes with sleep), Q8 (snoring, difficulty breathing or choking), and Q9 (limb numbness and discomfort preventing sleep) (p > 0.05). These findings may indicate that questionnaire questions Q1–Q5 and Q7 may reflect sleep disorders due to psychological causes that are more likely to be modified by BR10. However, questionnaire questions Q6, Q8 and Q9 reflect sleep disorders due to physical causes that are not modified by treatment with BR10.
Table 2.
Changes in sleep quality assessment questionnaire results during the study.
| Question number | tau-c | p value |
|---|---|---|
| Q1 | −0.210 | 0.003** |
| Q2 | −0.170 | 0.016* |
| Q3 | −0.169 | 0.016* |
| Q4 | −0.165 | 0.022* |
| Q5 | −0.191 | 0.004** |
| Q6 | −0.105 | 0.139 |
| Q7 | −0.182 | 0.006** |
| Q8 | −0.043 | 0.510 |
| Q9 | −0.084 | 0.222 |
3.2. Comparison of EEG data from the control group and the BR10 treated group
As an example of the findings in a non-treated control subject, Fig. 1a–c shows the EEG signals, channel locations, and power spectrum of an example of a control group candidate, which show no change before, during and after control treatment with plain SR at 10 Bps. In contrast, Fig. 1d–f shows specific changes during BR10 when compared with those before treatment. During the first 3 days of treatment, sleep quality improved in all 36 patients; in 91.7% (33/36) of experimental group, the BR treatment was associated with an elevation in the beta spectrum of the EEG (at 15–27 Hz) (the lower row in Fig. 1e). However, there is 0% of control group was associated with this EEG finding. By statistical comparison using Fisher's exact test, the 15–27 Hz elevation resulted in a significant increment (p < 0.05) of beta EEG signals during the BR10 treatments; this was not significant for the control group.
Fig. 1.

(a–f): Electroencephalograph (EEG) signal recordings for control group before (a), during (b) and after (c) the instrument operation with sound rhythm at 10 Bps; and for experimental group before (d), during (e) and after (f) BR10. Note: Elevations of EEG frequency within the range 15–27 Hz (∗) in channels 3–6 was recorded during instrument operation with BR10.
3.3. Comparison of areas of activation and deactivation by fMRI
By comparing the result of the candidates received 3 T fMRI without and with BIOCERAMIC Resonance, it showed an fMRI signal increase in areas (with total voxels of 2808), include left cerebellum, left inferior temporal gyrus and left insula lobe, etc (Fig. 2a and Table 3). There is also fMRI signal decrease in the following area: right superior frontal gyrus (Fig. 2b and Table 3).
Fig. 2.

a–b. Obvious fMRI signal increase in the areas of left cerebellum, left inferior temporal gyrus and left insula lobe (left, a); and minimal fMRI signal decrease was noticed in the right superior frontal gyrus (right b).
Table 3.
Comparison of fMRI imaging signal changes in cerebral and cerebellar regions between two groups.
| Regions | x | y | z | t-value |
|---|---|---|---|---|
| Experimental–control groups(activation) | ||||
| Left temporal pole | −45 | 3 | 15 | 7.68 |
| Left parahippocampal gyrus | −15 | −36 | −12 | 7.48 |
| Left rolandic operculum | −42 | −12 | 18 | 7.09 |
| Left inferior frontal gyrus | −51 | 24 | 15 | 5.46 |
| Left precentral gyrus | −51 | 3 | 21 | 5.40 |
| Left hippocampus | −18 | −15 | −18 | 5.29 |
| Left middle frontal gyrus | −33 | 48 | 3 | 5.24 |
| Left insula | −33 | 9 | 12 | 4.99 |
| Left thalamus | −3 | −27 | 6 | 4.99 |
| Left cerebellum | −51 | −63 | −9 | 4.89 |
| Left gyrus insula | −30 | 18 | 12 | 4.49 |
| Control–experimental groups(deactivation) | ||||
| Middle temporal gyrus | 51 | −57 | 21 | 4.62 |
4. Discussion
The results of this study have shown that in patients with sleep disorders, treatment with BR produced a significant improvement in sleep quality during the first 3 days after treatment, compared with non-treated controls. The improvement was more pronounced in subjects with more severe sleep disorders and in patients with psychological, rather than physical, causes of sleep disorder and the effects was cumulative.
In this study, during the procedure of BR, there was no significant change in average amplitude of the electroencephalography (EEG) for different frequency bands, including 1–4 Hz, 4–7 Hz, 7–12 Hz, 12–20 Hz, 20–25 Hz, and 25–30 Hz. The correlation between sleep quality and EEG bands of theta (4–7 Hz) and delta (1–4 Hz) frequencies, were not found to be significantly changed; these findings on delta and alpha EEG not able to explain sleep quality improvement by previous concept.33 However, there were a high percentage of subjects (91.7%) with increased EEG potentials between 15–27 Hz (beta-1 frequency band). This finding may be explained by the fact that this study was designed to determine EEG data before, during and after the operation of BR during the daytime, and not during sleep, and so BR may not have an instant effect on delta and alpha EEG frequencies. A case study of using fMRI for assessment of BR also demonstrate areas of activation and deactivation of different cerebral and cerebellar zones. Among the limitations of this study, the small study size and the use of a single study center may have introduced some possible of study bias, so it is clear that further larger multicenter studies are required. A further reason for including a larger study population in future studies would be that this would allow for more detailed analysis of the effects of BR on the sub-types of chronic sleep disorder and, in particular, those due to psychological causes. We also recommend that future studies be performed during sleep time rather than daytime. Also, in this study, the data analysis did not control for patient medication, such as antipsychotic or anti-depressant drugs, which may affect the EEG findings. A common use for EEG evaluation is in the diagnosis and monitoring of treatment for epilepsy, but none of our cases suffered from epilepsy.34 Finally, the beneficial effects of treatment with acupuncture, including electro-acupuncture, may be explained by ‘placebo effect’ for patients who know they are being treated. In this study, patients were aware that they were being treated with a form of acupuncture, and so we recommend that future double-blind controlled studies be performed. In previous studies where acupuncture has been performed in different anatomical sites, there were complex changes in delta and alpha rhythms of the EEG, as well as significant changes of beta-2 and gamma frequency bands observed in specific electrode sites.35, 36 Similar effects also demonstrated by activation and deactivation of different cerebral and cerebellar anatomical zones.31, 32 Some studies have shown increased EEG potentials in different frequency bands during states of meditation.37, 38, 39 Some recent alternative treatments for sleep disorder have been described, including neuromodulation with transcranial direct current stimulation (tDCS),40 and transcranial magnetic stimulation (TMS).41, 42 The tDCS treatment had been shown to increase beta power during and after stimulation.43 TMS had shown consistently evoked beta-band oscillations (13–20 Hz) in the parietal cortex.44, 45 This study has shown some new findings in this important and common clinical problem of sleep disorders, with the finding of short-term EEG elevation between 15–27 Hz and areas of activation and deactivation in cerebral and cerebellar regions. Those data may reflect a beneficial outcome following BR, or possibly a manifestation of other neurological effects. Some limitations of this study are including (i) relationships between daytime EEG spectrum changes and fMRI pattern finding with the nighttime sleep improvement has not able to discuss.
5. Conclusions
As far as we know, this is the first clinical study with preliminary data that proving a BIOCERAMIC Resonance can objectively improving sleep disorder due to psychological causes, but not significant effective to sleep disorders due to physical causes. Beside, BIOCERAMIC Resonance can transient alter brain wave activity, conducted by questionnaire for sleep-quality assessment correlating with EEG and fMRI monitoring. BIOCERAMIC Resonance has a high potential to act as an adjuvant treatment to chemical drug on chronic sleep disturbance.
Conflict of interest
The authors have no conflict of interest to declare.
Acknowledgements
This study was supported by funded of National Natural Science Foundation of China (Grant No. 81201069) and there is no conflict of interest in the manuscript. The authors are also grateful for the assistance of Dr. Qian Feng Wang, Miss Nancy Ling and Mr. Tai Lin Ping.
Footnotes
Peer review under responsibility of The Center for Food and Biomolecules, National Taiwan University.
References
- 1.Meerlo P., Sgoifo A., Suchecki D. Restricted and disrupted sleep: effects on autonomic function, neuroendocrine stress systems and stress responsively. Sleep Med Rev. 2008;12:197–210. doi: 10.1016/j.smrv.2007.07.007. [DOI] [PubMed] [Google Scholar]
- 2.Burgess H.J., Trinder J., Kim Y., Luke D. Sleep and circadian influences on cardiac autonomic nervous system activity. Am J Physiol. 1997;273:1761–1768. doi: 10.1152/ajpheart.1997.273.4.H1761. [DOI] [PubMed] [Google Scholar]
- 3.Srisurapanont M., Likhitsathian S., Chua H.C. Clinical and sociodemographic correlates of severe insomnia in psychotropic drug-free, Asian outpatients with major depressive disorder. J Affect Disord. 2015;186:26–31. doi: 10.1016/j.jad.2015.06.032. [DOI] [PubMed] [Google Scholar]
- 4.Sofi F., Cesari F., Casini A., Macchi C., Abbate R., Gensini G.F. Insomnia and risk of cardiovascular disease: a meta-analysis. Eur J Prev Cardiol. 2014;21:57–64. doi: 10.1177/2047487312460020. [DOI] [PubMed] [Google Scholar]
- 5.Kim K., Uchiyama M., Okawa M., Liu X., Ogihara R. An epidemiological study of insomnia among the Japanese general population. Sleep. 2000;23:41–47. [PubMed] [Google Scholar]
- 6.Ohayon M.M., Hong S.C. Prevalence of insomnia and associated factors in South Korea. J Psychosom Res. 2002;53:593–600. doi: 10.1016/s0022-3999(02)00449-x. [DOI] [PubMed] [Google Scholar]
- 7.Kao C.C., Huang C.J., Wang M.Y., Tsai P.S. Insomnia: prevalence and its impact on excessive daytime sleepiness and psychological well-being in the adult Taiwanese population. Qual Life Res. 2008;17:1073–1080. doi: 10.1007/s11136-008-9383-9. [DOI] [PubMed] [Google Scholar]
- 8.Chien I.C., Bih S.H., Chou Y.J., Lin C.H., Lee W.G., Chou P. Trends in the use of psychotropic drugs in Taiwan: a population-based national health insurance study, 1997–2004. Psychiatr Serv. 2007;58:554–557. doi: 10.1176/ps.2007.58.4.554. [DOI] [PubMed] [Google Scholar]
- 9.Barker M.J., Greenwood K.M., Jackson M., Crowe S.R. Cognitive effects of long-term benzodiazepine use: a meta-analysis. CNS Drugs. 2004;18:37–48. doi: 10.2165/00023210-200418010-00004. [DOI] [PubMed] [Google Scholar]
- 10.Hollingworth S.A., Siskind D.J. Anxiolytic, hypnotic and sedative medication use in Australia. Pharmacoepidemiol Drug Saf. 2010;19:280–288. doi: 10.1002/pds.1899. [DOI] [PubMed] [Google Scholar]
- 11.Han K.H., Kim S.Y., Chung S.Y. Effect of acupuncture on patients with insomnia: study protocol for a randomized controlled trial. Trials. 2014;15:403. doi: 10.1186/1745-6215-15-403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Yeung W.F., Chung K.F., Poon M.M. Chinese herbal medicine for insomnia: a systematic review of randomized controlled trials. Sleep Med Rev. 2012;16:497–507. doi: 10.1016/j.smrv.2011.12.005. [DOI] [PubMed] [Google Scholar]
- 13.Zhang L., Chan P., Min Liu Z.M. The effect of photoluminescence of BIOCERAMIC (PLB) irradiation on middle cerebral arterial occlusion (MCAO) in rats. Evid Based Complement Altern Med. 2016:7230962. doi: 10.1155/2016/7230962. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Leung T.K., Gasbarri M., Tai C.J., Chan W.P. Application of photoluminescent bioceramic material for different chronic illnesses by selecting “trigger points” and “propagated sensation along meridians” phenomenon. Chin J Integr Med. 2015; Jul 4 doi: 10.1007/s11655-015-2285-0. [DOI] [PubMed] [Google Scholar]
- 15.Chen C.W., Tai C.J., Choy C.S., Hsu C.Y., Lin S.L., Chan W.P. Wave-induced flow in meridians demonstrated using photoluminescent bioceramic material on acupuncture points. Evid Based Complement Altern Med. 2013:739293. doi: 10.1155/2013/739293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Leung T.K., Lin Y.S., Chen Y.C. Immunomodulatory effects of far infrared ray irradiation via increasing calmodulin and nitric oxide production in RAW 264.7 macrophages. Biomed Eng Appl Basis. 2009;21:317–323. [Google Scholar]
- 17.Lin Y., Leung T., Lee C. Far infrared ray irradiation induces intracellular generation of nitric oxide in breast cancer cells. J Med Biol Eng. 2009;29:15–18. [Google Scholar]
- 18.Liau B.Y., Leung T.K., Ou M.C., Ho C.K., Lin Y.S. Inhibitory effects of far-infrared ray-emitting belts on primary dysmenorrhea. Int J Photoenergy. 2012:6. [Google Scholar]
- 19.Leung T.K., Chen C.H., Tsai S.Y., Hsiao G., Lee C.M. Effects of far infrared rays irradiated from ceramic material (BIOCERAMIC) on psychological stress-conditioned elevated heart rate, blood pressure, and oxidative stress-suppressed cardiac contractility. Chin J Physiol. 2012;55:323–330. doi: 10.4077/CJP.2012.BAA037. [DOI] [PubMed] [Google Scholar]
- 20.Leung T.K., Kuo C.H., Lee C.M., Kan N.W., Hou C.W. Physiological effects of bioceramic material: harvard step, resting metabolic rate and treadmill running assessments. Chin J Physiol. 2013;56:334–340. doi: 10.4077/CJP.2013.BAB132. [DOI] [PubMed] [Google Scholar]
- 21.Leung T.K., Chan W.P., Tai C.J., Cho T.P., Yang J.C., Lee P.T. Bioceramic resonance effect on meridian channels: a pilot study. Evid Based Complement Altern Med. 2015:769546. doi: 10.1155/2015/769546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Leung T.K., Huang P.J., Chen Y.C., Lee C.M. Physical chemical test platform for room temperature, far-infrared ray emitting ceramic materials (c-FIR) J Chin Chem Soc. 2011;58:1–6. [Google Scholar]
- 23.Leung T.K., Yang J.C., Lin Y.S. The physical, chemical and biological effects by room temperature ceramic far-infrared ray emitting material irradiated water: a pilot study. J Chin Chem Soc. 2012;59:589–597. [Google Scholar]
- 24.Leung T.K., Lin S.L., Chan W.P. The influence of ceramic far-Infrared ray (cFIR) irradiation on water hydrogen bonding and its related chemo-physical properties. Hydrol Curr Res. 2014;5:174. [Google Scholar]
- 25.Wang Y.Y.L., Hsu T.L., Jan M.Y., Wang W.K. Review: theory and applications of the harmonic analysis of arterial pressure pulse waves. J Med Biol Eng. 2010;3:125–131. [Google Scholar]
- 26.Leung T.K., Lin M.T., Chen C.A., Hsu C.Y., Lin S.L., Chen C.W. The analysis of normalized effects on meridian current level after the photoluminescent bioceramic treatment on acupuncture points. J Altern Complement Med. 2015;21:472–479. doi: 10.1089/acm.2014.0076. [DOI] [PubMed] [Google Scholar]
- 27.Rasmussen G. Human body vibration exposure and its measurement. J Acoust Soc Am. 1983;73:2229. [Google Scholar]
- 28.Maxwell L., Barrett B., Chase J., Brown R., Ewers T. Self-reported mental health predicts acute respiratory infection. WMJ. 2015;114:100–104. [PMC free article] [PubMed] [Google Scholar]
- 29.Pahk K., Rhee S., Kim S., Choe J.G. Predictive role of functional visceral fat activity assessed by preoperative F-18 FDG PET/CT for regional lymph node or distant metastasis in patients with colorectal cancer. PLoS One. 2016;11:e0148776. doi: 10.1371/journal.pone.0148776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Delorme A., Makeig S. EEGLAB: an open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J Neurosci Methods. 2004;134:9–21. doi: 10.1016/j.jneumeth.2003.10.009. [DOI] [PubMed] [Google Scholar]
- 31.Deng G., Hou B.L., Holodny A.I., Cassileth B.R. Functional magnetic resonance imaging (fMRI) changes and saliva production associated with acupuncture at LI-2 acupuncture point: a randomized controlled study. BMC Complement Altern Med. 2008;8:37. doi: 10.1186/1472-6882-8-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Zhang Q., Li A., Yue J., Zhang F., Sun Z., Li X. Using functional magnetic resonance imaging to explore the possible mechanism of the action of acupuncture at Dazhong (KI 4) on the functional cerebral regions of healthy volunteers. Intern Med J. 2015; Jun;45(6):669–671. doi: 10.1111/imj.12767. [DOI] [PubMed] [Google Scholar]
- 33.Perlis M.L., Kehr E.L., Smith M.T., Andrews P.J., Orff H., Giles D.E. Temporal and stagewise distribution of high frequency EEG activity in patients with primary and secondary insomnia and in good sleeper controls. J Sleep Res. 2001;10:93–104. doi: 10.1046/j.1365-2869.2001.00247.x. [DOI] [PubMed] [Google Scholar]
- 34.Suzuki S.S., Smith G.K. Spontaneous EEG spikes in the normal hippocampus. V. Effects of ether, urethane, pentobarbital, atropine, diazepam and bicuculline. Electroencephalogr Clin Neurophysiol. 1998;70:84–95. doi: 10.1016/0013-4694(88)90198-8. [DOI] [PubMed] [Google Scholar]
- 35.Yi G., Wang J., Bian H. Multi-scale order recurrence quantification analysis of EEG signals evoked by manual acupuncture in healthy subjects. Cogn Neurodyn. 2013;7:79–88. doi: 10.1007/s11571-012-9221-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Jo H.G., Jo G.H. Electroencephalogram activity induced by magnetic stimulation on heart meridian. Neurosci Lett. 2011;495:107–109. doi: 10.1016/j.neulet.2011.03.049. [DOI] [PubMed] [Google Scholar]
- 37.Takahashi T., Murata T., Hamada T. Changes in EEG and autonomic nervous activity during meditation and their association with personality traits. Int J Psychophysiol. 2005;55:199–207. doi: 10.1016/j.ijpsycho.2004.07.004. [DOI] [PubMed] [Google Scholar]
- 38.Hebert R., Lehmann D. Theta bursts: an EEG pattern in normal subjects practising the transcendental meditation technique. Electroencephalogr Clin Neurophysiol. 1977;42:397–405. doi: 10.1016/0013-4694(77)90176-6. [DOI] [PubMed] [Google Scholar]
- 39.Banquet J.P. Spectral analysis of the EEG in meditation. Electroencephalogr Clin Neurophysiol. 1973;35:143–151. doi: 10.1016/0013-4694(73)90170-3. [DOI] [PubMed] [Google Scholar]
- 40.Marshall L., Mölle M., Hallschmid M., Born J. Transcranial direct current stimulation during sleep improves declarative memory. J Neurosci. 2004;24:9985–9992. doi: 10.1523/JNEUROSCI.2725-04.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Goetz S.M., Deng Z.D. The development and modelling of devices and paradigms for transcranial magnetic stimulation. Int Rev Psychiatry. 2017;26:1–31. doi: 10.1080/09540261.2017.1305949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Nardone R., Tezzon F., Höller Y., Golaszewski S., Trinka E., Brigo F. Transcranial magnetic stimulation (TMS)/repetitive TMS in mild cognitive impairment and Alzheimer's disease. Acta Neurol Scand. 2014;129:351–366. doi: 10.1111/ane.12223. [DOI] [PubMed] [Google Scholar]
- 43.Van Dijk K.D., Møst E.I., Van Someren E.J., Berendse H.W., van der Werf Y.D. Beneficial effect of transcranial magnetic stimulation on sleep in Parkinson's disease. Mov Disord. 2009;24:878–884. doi: 10.1002/mds.22462. [DOI] [PubMed] [Google Scholar]
- 44.Mangia A.L., Pirini M., Cappello A. Transcranial direct current stimulation and power spectral parameters: at DCS/EEG co-registration study. Front Hum Neurosci. 2014:8–601. doi: 10.3389/fnhum.2014.00601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Gosseries O., Thibaut A., Boly M., Rosanova M., Massimini M., Laureys S. Assessing consciousness in coma and related states using transcranial magnetic stimulation combined with electroencephalography. Ann Fr Anesth Reanim. 2014;33:65–71. doi: 10.1016/j.annfar.2013.11.002. [DOI] [PubMed] [Google Scholar]