

Abstract
Background
The prevention and correction of vitamin D deficiency requires a precise depiction of the current situation and identification of risk factors in each region. The present study attempted to determine these entities using a systematic review and meta-analysis in Iran.
Methods
Articles published online in Persian and English between 2000 and November 1, 2016, were reviewed. This was carried out using national databases such as SID, IranMedex, Magiran, and IranDoc and international databases such as PubMed, Google Scholar, and Scopus. The heterogeneity index among the studies was determined using the Cochran (Q) and I2 test. Based on the heterogeneity results, the random-effect model was applied to estimate the prevalence of vitamin D deficiency. In addition, meta-regression analysis was used to determine heterogeneity-suspected factors, and the Egger test was applied to identify publication bias.
Results
The meta-analysis of 48 studies identified 18531 individuals with vitamin D deficiency. According to the random-effect model, the prevalence of vitamin D deficiency among male, female, and pregnant women was estimated to be 45.64% (95% CI: 29.63 to 61.65), 61.90% (95% CI: 48.85 to 74.96), and 60.45% (95% CI: 23.73 to 97.16), respectively. The results of the meta-regression analysis indicated that the prevalence of vitamin D deficiency was significantly different in various geographical regions (β=4.4; P=0.023).
Conclusion
The results obtained showed a significant prevalence of vitamin D deficiency among the Iranian population, a condition to be addressed by appropriate planning.
Keywords: Vitamin D deficiency, Meta-analysis, Iran
What’s Known
Vitamin D status varies among different societies. Research shows a high prevalence of vitamin D deficiency, between 30% and 93%, during the past 2 decades. Sporadic studies in Iran have indicated high rates of vitamin D deficiency among various age groups
What’s New
We estimated the pooled prevalence of vitamin D deficiency in Iran. Prevalence was high among pregnant women and children nationwide. Age of the population studied affected the prevalence of vitamin D deficiency. Findings have implications for public health.
Introduction
Among the deficiencies of all micronutrients, vitamin D deficiency is currently considered a pandemic.1 According to the global estimations, more than 1 billion people are known to suffer from vitamin D deficiency, a matter of considerable importance in the 21st century.2-3
Vitamin D has a significant role in the health, survival, and fertility of humans.4-5 Several studies have emphasized its role in preventing diseases such as heart diseases, malignancies, inflammatory bowel diseases, multiple sclerosis, rheumatoid arthritis, type 1 diabetes, immune disorders, and infectious diseases.6-8 Vitamin D leads to an increase in the absorption of phosphorus and calcium through intestines and their reduced excretion through kidneys, while improving ontogenesis.6 Hence, its deficiency is among the main factors in metabolic bone disorders, leading to skeletal abnormalities, short stature, and delayed growth in children and osteomalacia, osteoporosis, and pathologic fractures among adults.2,9
The main source of vitamin D for humans is the exposure of the skin to sunlight and to a lower extent, the diet particularly vitamin D-containing dairy products.10 Theoretically speaking, although vitamin D deficiency is not expected in regions with intense sunlight, there are large numbers of reports indicating the high prevalence of vitamin D deficiency in countries with intense sunlight.11 This could be due to the various factors such as geographical locations, types of clothing, skin colors, and diets lacking in sufficient vitamin D.12
Vitamin D status varies among different societies. Various studies have shown a high prevalence of vitamin D deficiency in countries with intense sunlight such as China, Turkey, India, Iran, and Saudi Arabia, with an estimated prevalence between 30% and 93% over the past 2 decades.13 According to another study, 40%–100% of European and American elderly males and females who live a normal life and are not cared for in elderly care centers suffer from vitamin D deficiency.14 Also, more than 50% of menopausal women who have undergone treatments for osteoporosis have insufficient amounts of 25-hydroxy vitamin D.15
Numerous studies in Iran have indicated a high prevalence of vitamin D deficiency among various age groups, including students from Isfahan Province (at Lat: 32° 39 N), young women in Uremia Province (at Lat: 37° 32 N), and the general population in Tehran Province (at Lat: 36° 21 N).16
A study in Tehran during 2004 showed severe, moderate, and mild prevalence rates of vitamin D deficiency of 9.5%, 57.6%, and 14.2%, correspondingly.17 In a comprehensive study from several bone health centers in 2001, the rates of moderate to severe vitamin D deficiency in the urban population among the age groups of below 50, 50–60 years, and above 60 years were 7.2%, 45.47%, and 44.2% among males and 54.2%, 41.2%, and 37.5% among females.13
Decrease in vitamin D is globally considered a major health problem.2 On the other hand, the prevention and correction of the current situation is feasible provided that proper decisions are arrived at, especially with respect to high-risk groups. This in turn requires a precise depiction of the current situation, identification of risk-factor determinants, and development of the data collection process from specific populations in each region.
With a view to providing a basis for future efforts aimed at addressing the consequences of vitamin D deficiency, we conducted the present study via a systematic review and meta-analysis to estimate the prevalence of vitamin D deficiency in the general population of Iran apropos age, sex, and regional subgroups.
Methods
Literature search: Articles published in national and international journals were searched using studies published online from 2000 to November 1, 2016. This was conducted by employing relevant keywords in national databases such as SID, IranMedex, Magiran, and IranDoc and international databases such as PubMed, Google Scholar, and Scopus. The search strategy for the articles was generally based on the keywords of vitamin D, 25-hydroxy vitamin D, deficiency, prevalence, vitamin D deficiency, 25(OH) D, frequency, Iran, and their Persian equivalents. The search was carried out independently by 2 of the researchers (November 1–15, 2015). Also, the references of the published studies were consulted to increase the sensitivity and selection of a higher number of investigations. The assessment of the research was made randomly by 1 of the researchers to ensure that none of the studies was omitted. Also, the hard copies were searched in order to access the articles which were not published online, and appropriate research centers and experts were consulted in regard to the unpublished investigations.
Selection criteria and quality assessment: The full text or the abstract of all researches, records, and reports from advanced searches were extracted. The unrelated and duplicated studies were omitted by screening the title, abstract, and full text of the articles, leading to the subsequent selection of the related articles. Also, according to the most published guidelines, vitamin D deficiency was defined as serum 25(OH) D below 20 ng/mL (<50 nmol/L). To prevent bias due to transverse and longitudinal publication, the researchers tried to screen, identify, and omit the duplicated studies. Having determined the related studies based on titles and contents, the researchers employed the checklist used in previous studies to evaluate the quality of the records.18 This checklist by checking the STROBE checklist content19 comprises questions on 12 items, covering various aspects of methodology such as those determining proper sample size, study type, sampling type, and research populations. Furthermore, the method of data collection, method of defining the variables, method of studying the samples, tools of data collection, statistical tests, and research objectives were considered to ascertain that the results obtained were compatible with the objectives. The meta-analysis required 1 point for each question in addition to any studies that achieved at least 8 points.18
Data extraction: Data for each research were extracted based on the title, corresponding author, year of conducting the study, type of study, sampling method, sample size, language of the article, general prevalence of vitamin D deficiency, prevalence of vitamin D deficiency based on gender, prevalence of vitamin D deficiency based on specific groups (i.e., pregnant women, children [age≤18 y], and patients [diabetes type 2, metabolic syndrome, depression, and dialysis]), and geographical regions. (These categories were based on the number of the studies published in each region. If the number of the studies conducted in each region exceeded 1, they were separately categorized for meta-analysis by geographic regions; otherwise, the study was placed in another category.) The data extracted were entered in a Microsoft Excel spreadsheet.
Inclusion criteria: The aspects to be considered for the selection of materials included all Persian and English studies, which after the evaluation process and achieving the required score, reported the sample size, general prevalence of vitamin D deficiency, and prevalence of vitamin D deficiency based on gender. (Vitamin D deficiency was defined as 25(OH) D<20 ng/mL or <50 nmol/L).
Analysis: Stata software was used to analyze the data. The standard deviation (SD) of the general prevalence of vitamin D deficiency, prevalence of vitamin D deficiency based on gender, prevalence of vitamin D deficiency based on specific groups, and prevalence of vitamin D deficiency based on geographical regions in each study was calculated via the binomial distribution formula. Ultimately, the heterogeneity index among the studies was determined using the Cochran (Q) and I2 test. Based on the heterogeneity results, the random-effect model was employed to estimate the general prevalence of vitamin D deficiency and the prevalence of vitamin D deficiency based on gender, in Iran. The point estimation of the general prevalence of vitamin D deficiency and the prevalence of vitamin D deficiency based on gender was calculated at a confidence interval (CI) of 95% in forest plots. Moreover, the Egger test was carried out to assess the publication bias and considering the significance level below 0.01 as a criterion for judgment. Also, meta-regression analysis was conducted to investigate the heterogeneity-related factors.
Results
Through an initial search, 2598 papers were found from national and international databases and after limiting the search strategy and omitting the duplicates, due to the overlap of the databases, 706 records were included in this study. Having screened the titles and abstracts, 539 reports were found to be nonrelevant. The full text of the remaining 167 articles was studied, of which 117 reports were unrelated. Furthermore, 3 articles found through studying the references were added to our search list. Subsequently, by evaluating the quality of the articles and considering the inclusion and exclusion criteria, we omitted 5 articles and subjected 48 articles to the meta-analysis process (figure 1).
Figure 1.
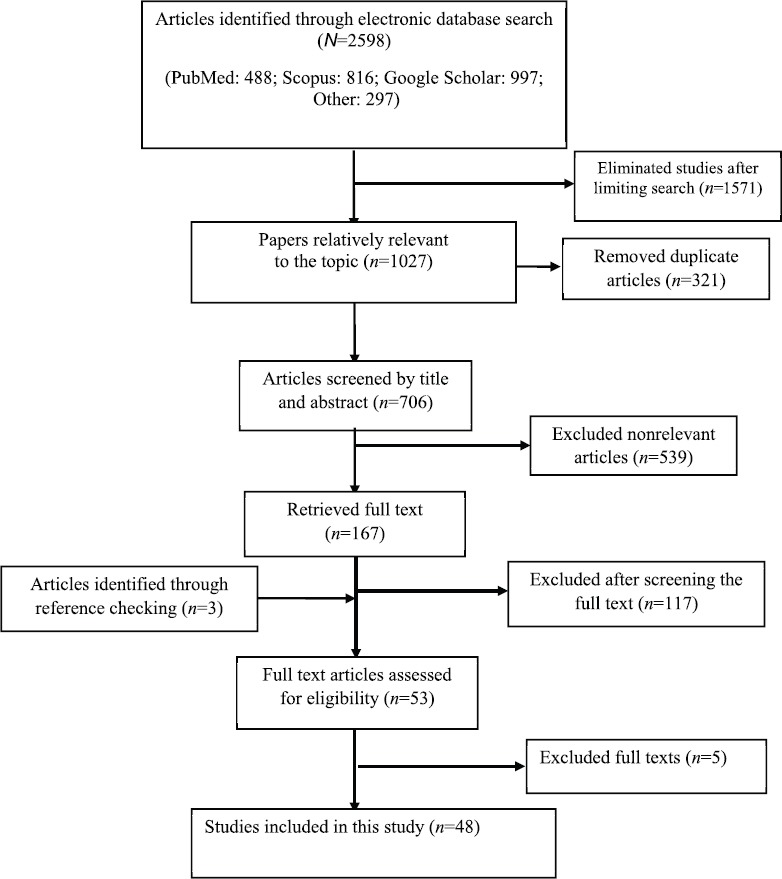
Flowchart of literature search showing the final 48 studies entered into this systematic review and meta-analysis.
The research type in all of the records included in the study was cross-sectional, and 33 of the 48 studies were selected randomly. The searched studies comprised 7 studies on pregnant women, 15 on children aged less than 18 years, 14 on patients (diagnosed with type 2 diabetes, metabolic syndrome, dialysis patients, etc.), and 12 on the general population above 18 years old with the exclusion of pregnant women, children, and patients (table 1).
Table 1.
Characteristics of the primary studies included in the present meta-analysis
| Id | First author | Publication year | Target population | Sample size | Prevalence of vitamin D deficiency | ||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Male | Female | Total | Female | Male | ||||
| 1 | Shahla20 | 2005 | General population | 162 | - | 162 | 82.1 | 82.1 | - |
| 2 | Salak21 | 2007 | Children | 513 | 271 | 242 | 26 | 12.26 | 13.74 |
| 3 | Heidarpour22 | 2006 | Children | 318 | 153 | 165 | 46.2 | 72.1 | 18.3 |
| 4 | Hatami23 | 2014 | Pregnant women | 100 | - | 100 | 76 | 76 | - |
| 5 | Rostami24 | 2015 | Pregnant women | 1581 | - | 1581 | 84.4 | 84.4 | - |
| 6 | Banakdaran25 | 2015 | General population | 902 | 380 | 522 | 79.3 | 45.89 | 33.5 |
| 7 | Karimi26 | 2014 | Children | 216 | - | 216 | 96 | 96 | - |
| 8 | Shakiba27 | 2008 | General population | 82 | 41 | 41 | 91.5 | - | - |
| 9 | Talaei28 | 2011 | Children | 420 | 200 | 220 | 84 | 99.1 | 66.5 |
| 10 | Asadi29 | 2015 | Pregnant women | 186 | - | 186 | 74.4 | 74.4 | - |
| 11 | Rahimi30 | 2005 | General population | 252 | - | 252 | 64.2 | 64.2 | - |
| 12 | Ghanei31 | 2014 | Children | 124 | 59 | 65 | 81 | 100 | 61 |
| 13 | Azizi32 | 2000 | General population | 1172 | 490 | 682 | 78.63 | 91 | 60 |
| 14 | Akhlaghi33 | 2015 | Pregnant women | 190 | - | 190 | 85.3 | 85.3 | |
| 15 | Khalaji34 | 2013 | Children | 1111 | 573 | 538 | 91.7 | 94.8 | 88.8 |
| 16 | Ghazi35 | 2001 | General population | 172 | - | - | 54 | - | - |
| 17 | Rabbani36 | 2009 | Children | 963 | 424 | 539 | 35 | 53.6 | 11.3 |
| 18 | Saki37 | 2015 | Children | 477 | - | 81.3 | - | - | |
| 19 | Salek38 | 2008 | Pregnant women | 88 | - | 88 | 26.1 | 26.1 | - |
| 20 | Shakiba39 | 2009 | Children | 167 | - | 167 | 59.9 | 59.9 | - |
| 21 | Asadi40 | 2009 | Children | 250 | - | 250 | 59.6 | 59.6 | - |
| 22 | Zahed41 | 2015 | Dialysis | 135 | - | - | 63 | - | - |
| 23 | Banakdaran42 | 2010 | Type 2 diabetes | 119 | - | - | 26.1 | - | - |
| 24 | Paknahad43 | 2015 | Metabolic syndrome | 156 | - | - | 54.5 | - | - |
| 25 | Kaykhaei44 | 2011 | General population | 993 | 431 | 562 | 85.2 | 89 | 80.3 |
| 26 | Savaj45 | 2012 | Kidney transplantation | 113 | - | - | 45 | - | - |
| 27 | Hosseinpanah46 | 2010 | General population | 100 | - | 100 | 36 | 36 | - |
| 28 | Hosseinpanah46 | 2010 | General population | 100 | - | 100 | 31 | 31 | - |
| 29 | Ataie-Jafari47 | 2012 | Type 1 diabetes | 53 | - | - | 77 | - | - |
| 30 | Javadian48 | 2016 | Knee osteoarthritis | 92 | 20 | 72 | 69.5 | 75 | 50 |
| 31 | Larijani49 | 2016 | Children | 444 | 227 | 217 | 43.3 | 71.23 | 17.47 |
| 32 | Mirsaeid ghazi50 | 2004 | General population | 1172 | 490 | 682 | 52 | 69 | 35 |
| 33 | Saki51 | 2016 | Type 1 diabetes | 85 | 39 | 46 | 88.2 | 84.6 | 91.8 |
| 34 | Zolfaghari52 | 2016 | Degenerative diseases | 110 | 54 | 56 | 44.5 | - | - |
| 35 | Hossein-Nezhad53 | 2014 | Coronary artery diseases | 760 | 582 | 178 | 98 | - | - |
| 36 | Heidari54 | 2012 | General population | 696 | 120 | 576 | 70.1 | 70.8 | 67.5 |
| 37 | Shamsian55 | 2016 | General population | 1110 | 262 | 848 | 68.8 | - | - |
| 38 | Abbasian56 | 2016 | Pregnant women | 284 | - | 284 | 2.5 | 2.5 | - |
| 39 | Chitsaz57 | 2013 | Parkinson’s disease | 109 | 77 | 32 | 38.4 | - | |
| 40 | Heidari58 | 2016 | Type 2 diabetes | 84 | 39 | 45 | 35.72 | 13.09 | 22.62 |
| 41 | Fallahi59 | 2016 | Children | 62 | - | - | 56.5 | - | - |
| 42 | Kelishadi60 | 2016 | Children | 1095 | 569 | 526 | 40 | 39.3 | 40.7 |
| 43 | Entezari-Maleki61 | 2014 | Thromboembolism | 60 | 32 | 28 | 60 | 57.1 | 61.1 |
| 44 | Asadi62 | 2016 | Pregnant women | 186 | - | - | 74.4 | - | - |
| 45 | Sobouti63 | 2016 | Pediatric burns | 118 | 50 | 68 | 81.35 | - | - |
| 46 | Ardestani64 | 2010 | Children | 513 | 271 | 242 | 5 | 2.1 | 3.7 |
| 47 | Hejazi65 | 2015 | Asthma | 120 | - | - | 73.3 | - | - |
| 48 | Rafraf66 | 2013 | Children | 216 | 216 | - | 96 | 96 | - |
The total number of the individuals in the 48 studies subjected to the meta-analysis was 18531, which varied from 53 individuals in Ataie-Jafari’s report to 1581 subjects in Rostami’s study. The average age of the studied individuals varied from 12.6 years in Talaee’s study to 57.97 years in that of Hossein-Nezhad. The total vitamin D deficiency prevalence varied from 2.5% in Abbasian’s study to 96% in Karimi’s study (figure 2).
Figure 2.
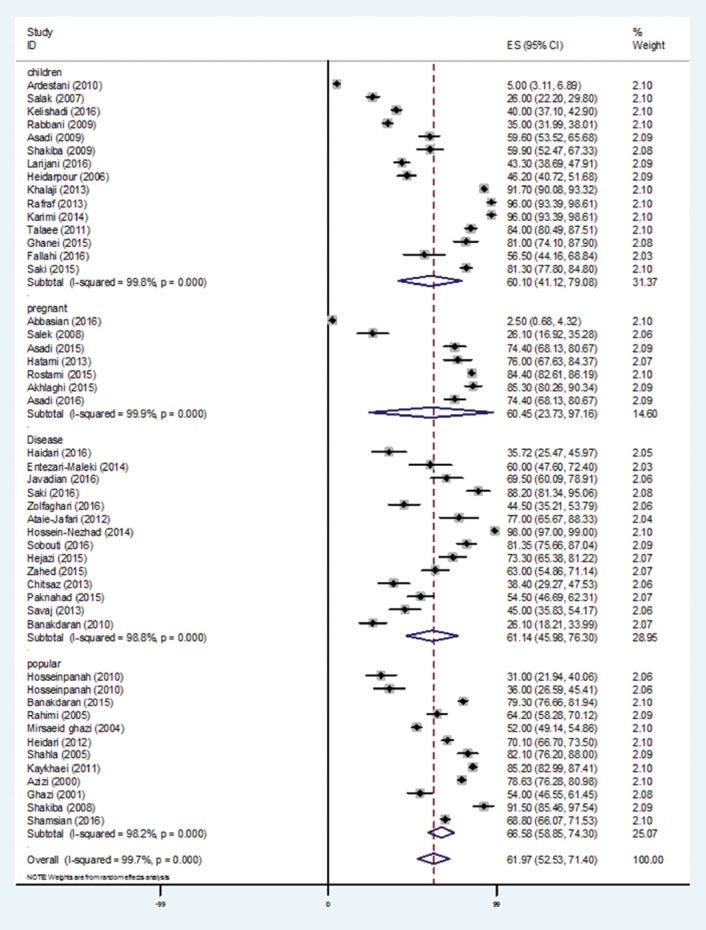
Prevalence of overall vitamin D deficiency in the Iranian population by the random-effect model for each of the 48 included studies. For each study, the estimate of prevalence and its 95% confidence interval were plotted with a box and a horizontal line.
The vitamin D deficiency prevalence was reported in 18 of 5854 studied male individuals. The vitamin D deficiency prevalence varied from 11.3% in Rabbani’s study to 82.1% in Moradzadeh’s study. According to the meta-analysis (figure 3 and table 2), the pooled prevalence of vitamin D deficiency among male Iranians was estimated to be 45.64% (95% CI: 29.63 to 61.65).
Figure 3.
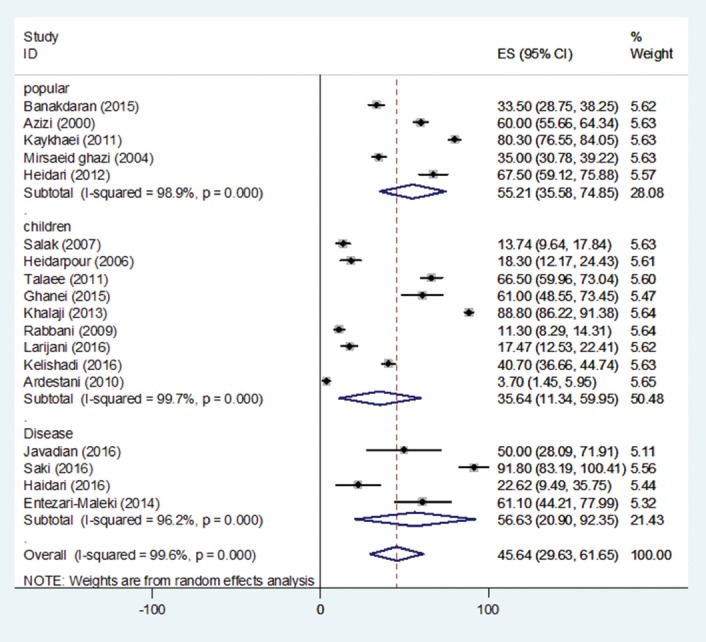
Prevalence of vitamin D deficiency among Iranian males by the random-effect model for each of the included studies. For the included studies, the estimate of prevalence and its 95% confidence interval were plotted with a box and a horizontal line.
Table 2.
Pooled estimation of the vitamin D deficiency prevalence obtained from the present meta-analysis
| Variables | Included studies | Sample size (n) | Pooled prevalence (%) | 95% confidence interval | Heterogeneity (I2-%) |
|---|---|---|---|---|---|
| Vitamin D deficiency (total) | 48 | 18531 | 61.97 | 52.53-71.40 | 99.7 |
| Vitamin D deficiency (males) | 18 | 5854 | 45.64 | 29.63-61.65 | 99.6 |
| Vitamin D deficiency (females) | 32 | 10868 | 61.90 | 48.85-74.96 | 99.9 |
The vitamin D deficiency prevalence was reported in 32 of 10868 Iranian women. The vitamin D deficiency prevalence varied from 2.1% in Ardestani’s study to 100% in Ghanei’s report (table 1). According to the meta-analysis, the pooled prevalence of vitamin D deficiency among female Iranians was estimated to be 61.90% (95% CI: 48.85 to 74.96) (figure 4 and table 2).
Figure 4.
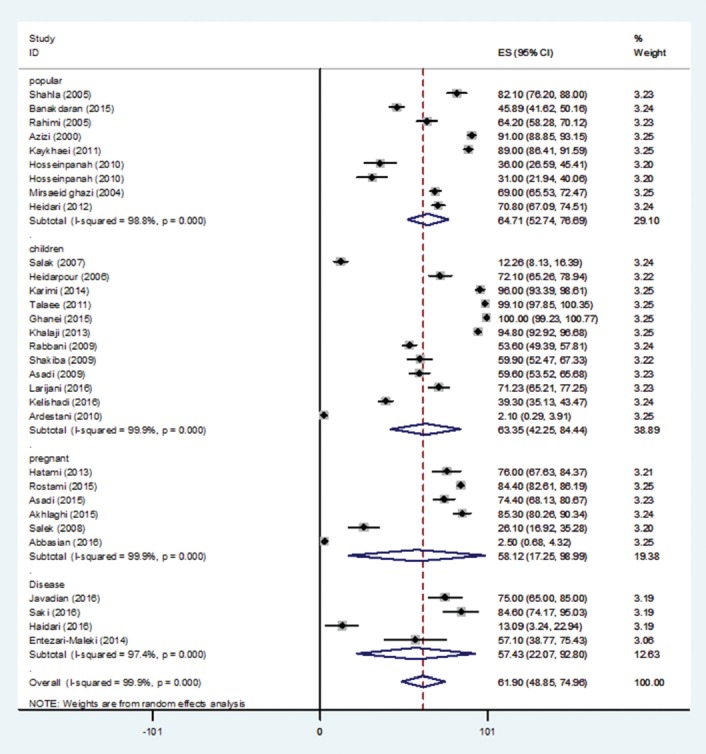
Prevalence of vitamin D deficiency among Iranian females by the random-effect model for each of the included studies. For the included studies, the estimate of prevalence and its 95% confidence interval were plotted with a box and a horizontal line.
The vitamin D deficiency prevalence was reported in 7 of 2615 studies concerning pregnant women. The vitamin D deficiency prevalence varied from 2.5% in Abbasian’s study to 85.3% in Akhlaghi’s study. Considering the presence of heterogeneity, based on the random-effect model, the pooled prevalence of vitamin D deficiency among Iranian pregnant women was estimated to be 60.45% (95% CI: 23.73 to 97.16). The vitamin D deficiency prevalence was reported in 15 studies, conducted on 6889 children. The vitamin D deficiency prevalence varied from 5% in Ardestani’s study to 96% in Rafraf’s study. According to the meta-analysis, the pooled prevalence of vitamin D deficiency in Iranian children was estimated to be 60.10% (95% CI: 41.12 to 79.08) (table 3).
Table 3.
Prevalence of vitamin D deficiency by sub-group analysis
| Subgroup | Included studies | Sample size (n) | Pooled prevalence (%) | 95% confidence interval | Heterogeneity (I2-%) |
|---|---|---|---|---|---|
| Specific group | |||||
| Pregnant women | 7 | 2615 | 60.45 | 23.73-97.16 | 99.9 |
| Children* | 15 | 6889 | 60.10 | 41.12-79.08 | 99.8 |
| Disease** | 14 | 2114 | 61.14 | 45.98-76.30 | 98.8 |
| General population (age>18 y) (with the exclusion of pregnant women, children, and patients) | |||||
| Total | 12 | 6913 | 66.58 | 58.85-74.30 | 98.2 |
| Male | 5 | 1911 | 55.21 | 35.58-74.85 | 98.2 |
| Female | 9 | 3638 | 64.71 | 52.74-76.69 | 98.9 |
Age≤18,
Group diseases included: diabetes type 2 (1 study), metabolic syndrome (1 study), depression (1 study), and dialysis (1 study)
The results of the meta-regression analysis suggested that the vitamin D deficiency prevalence was not significantly different based on the mean age (β=-0.1; P=0.795), publication year (β=0.8; P=0.337), and population group (β=1.3; P=0.700); nonetheless, the geographical region was recognized as a source of heterogeneity (β=4.4; P=0.023) (figure 5).
Figure 5.
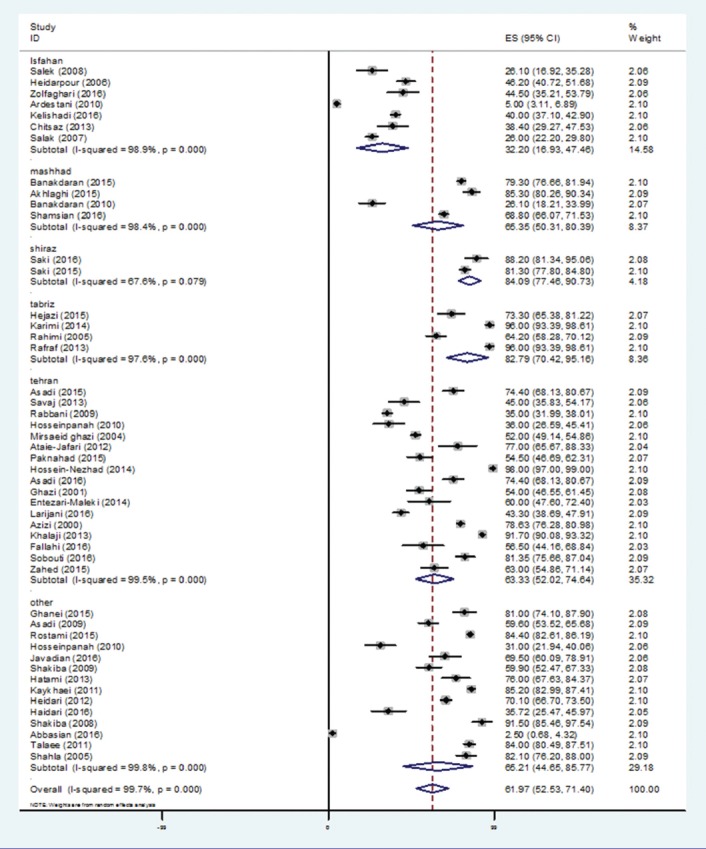
Prevalence of vitamin D deficiency in the geographical regions of Iran by the random-effect model for each of the included studies. For the included studies, the estimate of prevalence and its 95% confidence interval were plotted with a box and a horizontal line.
Also, according to the Egger test, no bias was found in regard to publication assessment (β=-6.8; P=0.153).
Discussion
In the published records on the prevalence of vitamin D deficiency in Iran’s population, the prevalence rate varied from 2.5% to 98% in various studies and regions. The vitamin D deficiency prevalence was significantly different based on geographical regions, where a high rate of the vitamin D deficiency prevalence was observed in pregnant women.
Vis-à-vis various geographical regions, the prevalence of vitamin D deficiency was significantly different in our study, which was consistent with other studies. Also, it has been reported that individuals in northern America have a higher rate of vitamin D than those in Africa and Europe.17,32,67-72
The high prevalence of vitamin D deficiency in the Iranian population and the different prevalence rates in various regions of Iran may be due to various factors such as the amount of skin pigments, low dietary vitamin D intakes, and genetic factors such as special vitamin D receptor polymorphisms. Vitamin D deficiency may also result from low calcium intakes, involved in the vitamin D catabolism.38,73
The findings of this research showed a significant difference in the vitamin D deficiency prevalence between various age groups. This was in agreement with the results of systematic review analyses carried out in Asia and Africa in regard to age and region.74 The main reason for the higher vitamin D deficiency prevalence in ages above 18 years is the lesser exposure to sunlight due to various reasons such as increasing industrialization, spending more time at home, and the clothing that may result in reduced vitamin D synthesis.26 On the other hand, vitamin D deficiency among Iranian adults might be due to lower dietary vitamin D intakes. Unlike certain foods consumed by adolescents lacking sufficient amounts of vitamin D, foods such as fish oil, egg yolks, and certain types of fish and seafood are valuable sources of vitamin D. In general, according to present national reports, the vitamin D content is low in the Iranian diet.75-77
Among the articles included in the present study, some studies showed no significant impact of age on the prevalence of vitamin D deficiency, which may be due to the limited age range studied, such as those focusing on a particular age, one age subgroup, or the age range of different subjects. On the other hand, no comprehensive research has been conducted to compare the level of vitamin D deficiency in children, adolescents, adults, and the elderly.
Our findings, similar to the studies carried out in Asia, showed that females had a higher prevalence of vitamin D deficiency than males. This may be explained in terms of cultural aspects and social obligations in women such as women’s preference to wear particular clothing outdoors, which prevents darkening of their skins, and skin diseases due to direct exposure to sunlight.78 Studies have clearly demonstrated women’s clothing as an independent risk factor for vitamin D deficiency among women.72,79 Accordingly, the prevalence of vitamin D deficiency is higher in countries with intense sunlight such as Saudi Arabia, United Arab Emirates, Jordan, Turkey, and Lebanon, where women’s clothing covers most parts of the body and prevents the exposure of the skin to sunlight.69,72,80-83 The higher prevalence of vitamin D deficiency among pregnant women in the foregoing countries may be related to living in apartments and the other aforementioned factors.38,84 It seems that the thresholds of vitamin D and calcium intake for changing the serum level of these micronutrients are necessary for providing adequate levels, especially for mothers and infants, and the current determined needed amounts (i.e., 400 units for vitamin D and 800 mg per day for calcium) are far lower than the needed thresholds for significant serum changes.84
In short, considering the vitamin D deficiency prevalence in both genders and also the considerable prevalence in females, despite sufficient amounts of sunlight in all seasons in Iran and other Asian countries80,85 and the adequate exposure to sunlight as indicated by some studies, there seems to be additional reasons to account for vitamin D deficiency. These may include the types of clothing, impacts of other factors such as lifestyle, dietary habits, skin pigmentations, air pollution, and inadequate vitamin D intakes, or even the disorders in the vitamin D metabolism in both genders.17,86 Another hypothesis for the prevalence of vitamin deficiency in Asia, compared to other regions, is the increase in the vitamin D catabolism. Although this vitamin is widely available and cheap, various social and cultural factors such as modern lifestyle and the fear of harmful effects of sunlight on skin account for not benefitting from adequate amounts of vitamin D.39,87
Considering all these, vitamin D deficiency is deemed a health problem and its significance grows by the increasing average age of populations and changing lifestyles. Given the process of industrialization in Iran and its young population, paying due attention to this important problem is of high priority. Hence, not only should the Iranian government make efforts to apply efficient interventions to reduce the prevalence of vitamin D deficiency, but also the country’s healthcare system should be controlled and managed through targeted and accurate planning. This can be achieved by improving the healthcare system, promoting comprehensive measures such as verbal communications, and updating the community’s awareness.
Last but not least are the limitations of this study, which are imposed by the writing styles of various authors, their inaccessibility, and having no response. Although all the 19 studies used in this research had gained the required score for entering the analysis, some fundamental properties such as the prevalence rate based on the main findings concerning subgroups have not been considered (table 1) or the prevalence rates have not been mentioned directly, which was calculated by the authors based on the data available from the studies. Also, it must be kept in mind that the best method of vitamin D assessment is the enzyme-linked immunosorbent assay (ELISA) and high performance liquid chromatography (HPLC). The high prevalence of vitamin D deficiency in our meta-analysis study may be due to different evaluation methods (17 studies using the ELISA method, 23 studies employing the method of radioimmunoassay [RIA], 6 studies utilizing the chemiluminescence method, and 2 studies drawing upon the HPLC method). Therefore, our findings should be interpreted with caution.
Although estimating the vitamin D deficiency prevalence based on cross-sectional studies is not error-free, the main advantage of this research is the accurate evaluation of the prevalence of vitamin D deficiency using a systematic review and meta-analysis, based on demographic groups in Iran.
Acknowledgement
This study was approved and financed by the Health Policy Research Center of Shiraz University of Medical Sciences, Iran, with number (95-01-62-13532).
Conflict of Interest: None declared.
References
- 1.Holick MF, Chen TC. Vitamin D deficiency: A worldwide problem with health consequences. Am J Clin Nutr. 2008;87:1080S–6S. doi: 10.1093/ajcn/87.4.1080S. [DOI] [PubMed] [Google Scholar]
- 2.Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266–81. doi: 10.1056/NEJMra070553. [DOI] [PubMed] [Google Scholar]
- 3.Heaney RP, Dowell MS, Hale CA, Bendich A. Calcium absorption varies within the reference range for serum 25-hydroxyvitamin D. J Am Coll Nutr. 2003;22:142–6. doi: 10.1080/07315724.2003.10719287. [DOI] [PubMed] [Google Scholar]
- 4.Hagenau T, Vest R, Gissel TN, Poulsen CS, Erlandsen M, Mosekilde L, et al. Global vitamin D levels in relation to age, gender, skin pigmentation and latitude: An ecologic meta-regression analysis. Osteoporos Int. 2009;20:133–40. doi: 10.1007/s00198-008-0626-y. [DOI] [PubMed] [Google Scholar]
- 5.Hashemipour S, Lalooha F, Zahir Mirdamadi S, Ziaee A, Dabaghi Ghaleh T. Effect of vitamin D administration in vitamin D-deficient pregnant women on maternal and neonatal serum calcium and vitamin D concentrations: A randomised clinical trial. Br J Nutr. 2013;110:1611–6. doi: 10.1017/S0007114513001244. [DOI] [PubMed] [Google Scholar]
- 6.Holick MF. Vitamin D: Importance in the prevention of cancers, type 1 diabetes, heart disease, and osteoporosis. Am J Clin Nutr. 2004;79:362–71. doi: 10.1093/ajcn/79.3.362. [DOI] [PubMed] [Google Scholar]
- 7.Holick MF. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am J Clin Nutr. 2004;80:1678S–88S. doi: 10.1093/ajcn/80.6.1678S. [DOI] [PubMed] [Google Scholar]
- 8.Ziaee A, Hashemipoor S, Karimzadeh T, Jalalpoor A, Javadi A. Relation of Vitamin D3 Level with metabolic Syndrome Indices among Patients with Diabetes and Non-Diabetic Individuals. Journal of Ardabil University of Medical Sciences. 2012;12:149–56. [Persian] [Google Scholar]
- 9.Hickey L, Gordon CM. Vitamin D deficiency: New perspectives on an old disease. Curr Opin Endocrinol Diabetes. 2004;11:18–25. [Google Scholar]
- 10.Molla AM, Al Badawi M, Hammoud MS, Molla AM, Shukkur M, Thalib L, et al. Vitamin D status of mothers and their neonates in Kuwait. Pediatr Int. 2005;47:649–52. doi: 10.1111/j.1442-200x.2005.02141.x. [DOI] [PubMed] [Google Scholar]
- 11.Moussavi M, Heidarpour R, Aminorroaya A, Pournaghshband Z, Amini M. Prevalence of vitamin D deficiency in Isfahani high school students in 2004. Horm Res. 2005;64:144–8. doi: 10.1159/000088588. [DOI] [PubMed] [Google Scholar]
- 12.Lips P. Vitamin D status and nutrition in Europe and Asia. J Steroid Biochem Mol Biol. 2007;103:620–5. doi: 10.1016/j.jsbmb.2006.12.076. [DOI] [PubMed] [Google Scholar]
- 13.Heshmat R, Mohammad K, Majdzadeh S, Forouzanfar M, Bahrami A, Ranjbar Omrani G. Vitamin D deficiency in Iran: A multi-center study among different urban areas. Iran J Public Health. 2008;37:128–35. [Persian] [Google Scholar]
- 14.Holick MF, Siris ES, Binkley N, Beard MK, Khan A, Katzer JT, et al. Prevalence of Vitamin D inadequacy among postmenopausal North American women receiving osteoporosis therapy. J Clin Endocrinol Metab. 2005;90:3215–24. doi: 10.1210/jc.2004-2364. [DOI] [PubMed] [Google Scholar]
- 15.Sullivan SS, Rosen CJ, Halteman WA, Chen TC, Holick MF. Adolescent girls in Maine are at risk for vitamin D insufficiency. J Am Diet Assoc. 2005;105:971–4. doi: 10.1016/j.jada.2005.03.002. [DOI] [PubMed] [Google Scholar]
- 16.Salek M, Hashemipour M, Aminorroaya A, Gheiratmand A, Kelishadi R, Ardestani PM, et al. Vitamin D deficiency among pregnant women and their newborns in Isfahan, Iran. Exp Clin Endocrinol Diabetes. 2008;116:352–6. doi: 10.1055/s-2008-1042403. [DOI] [PubMed] [Google Scholar]
- 17.Hashemipour S, Larijani B, Adibi H, Javadi E, Sedaghat M, Pajouhi M, et al. Vitamin D deficiency and causative factors in the population of Tehran. BMC Public Health. 2004;4:38. doi: 10.1186/1471-2458-4-38. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Akbari M, Moosazadeh M, Tabrizi R, Khatibi SR, Khodadost M, Heydari ST, et al. Estimation of iron deficiency anemia in Iranian children and adolescents: A systematic review and meta-analysis. Hematology. 2017;22:231–9. doi: 10.1080/10245332.2016.1240933. [DOI] [PubMed] [Google Scholar]
- 19.Vandenbroucke JP, von Elm E, Altman DG, Gotzsche PC, Mulrow CD, Pocock SJ, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Epidemiology. 2007;18:805–35. doi: 10.1097/EDE.0b013e3181577511. [DOI] [PubMed] [Google Scholar]
- 20.Shahla A, Charehsaz S, Talebi R, Azad E. Vitamin D deficiency in women 40-15 years in Urmia city. J Urmia Univ Med Sci. 2005;16:80–83. [Persian] [Google Scholar]
- 21.Salek M, Rafati H, Hashemipour M, Ardestani PM, Nezhadnik H, Amini M, et al. Is Vitamin D Deficiency Prevalent in Healthy 6-year-old Children in Isfahan City? Journal of Isfahan Medical School. 2007;25:95–103. [Persian] [Google Scholar]
- 22.Heidarpour R, Moussavi M, Âminorroaya A, Pournaghshband Z, Âmini M. The prevalence of vitamin D deficiency is Isfahani students. Journal of Mazandaran University of Medical Sciences. 2006;16:88–95. [Persian] [Google Scholar]
- 23.Hatami G, Ahmadi S, Motamed N, Eghbali SS, Amirani S. 25-OH Vitamin D serum level in pregnant women in Bushehr-2012. ISMJ. 2014;16:410–8. [Persion] [Google Scholar]
- 24.Rostami M, Ramezani Tehrani F, Simbar M, Hosein Panah F, Alavi Majd SH. Prevalence of Vitamin D deficiency and related factors Among Pregnant Women referred to Masjed Soleimam health centers in 2014. The Iranian Journal of Obstetrics, Gynecology and Infertility. 2015;18:1–10. [Persian] [Google Scholar]
- 25.Bonakdaran S, Ghayour-Mobarhan M, Fakhraee F. Assessment of 25 hydroxyvitamin D level and its correlation with metabolic syndrome in Mashhad. Medical Journal of Mashhad University of Medical Sciences. 2015;58:88–95. [Persian] [Google Scholar]
- 26.Karimi- Hasanabad S, Rafraf M, Asghari-Jafarabadi M. Prevalence of vitamin d deficiency and its relationship with body mass index and waist circumference in female adolescents 17-14 years, Boukan. Iranian Journal of Diabetes and Lipid Disorders. 2014;14:55–62. [Persian] [Google Scholar]
- 27.Shakiba M, Rafiei P. Prevalence of vitamin D deficiency among medical staff in Shahid Sadoughi Hospital in Yazd, Iran. Toloo-E-Behdasht. 2009;7:22–30. [Persian] [Google Scholar]
- 28.Talaei A, Yadegari N, Rafee M, Rezvanfar M. Vitamin D Deficiency and Its Cut-off Point among young teenagers. Journal of Birjand University of Medical Sciences. 2011;18:210–6. [Persian] [Google Scholar]
- 29.Asadi M, Saeidifard F, Qorbani M, Adabi K. Vitamin D deficiency and mode of delivery: A study in Tehran Women General Hospital. Tehran University Medical Journal TUMS Publications. 2015;73:442–6. [Persian] [Google Scholar]
- 30.Rahimi A, Zarghami N, Seddighi A, Alani B, Dostzadeh A. Prevalence of vitamin D deficiency and other possible risk factors in reproductive age women in Tabriz. Medical Journal of Tabriz University of Medical Scienced and Health Services. 2006;27:7–11. [Persian] [Google Scholar]
- 31.Ghanei L, Jalilolghadr S, Javadi M, Ghorbani A, Khoeiniha M. Epidemiology of vitamin D deficiency among 10-18 years old population of Minoodar district, Qazvin (2010) J Qazvin Univ Med Sci. 2015;18:24–32. [Persian] [Google Scholar]
- 32.Azizi F, Rais Zadeh F, Ghazi A. Vitamin D deficiency in a group of Tehran population. Research in Medicine. 2000;4:291–303. [Persian] [Google Scholar]
- 33.Akhlaghi F, Vakili R, Khorasani E. Evaluation of umbilical cord vitamin D level and maternal factors effective on it in three hospitals of Emam Reza, Ghaem & Omol Banin during 2013-2014. Iranian Journal of Obstetrics, Gynecology and Infertility. 2015;17:1–7. [Persian] [Google Scholar]
- 34.Khalaji N, Asadzadeh S, Neyestani T, Hajifaraji M, Omidvar N, Shariatzadeh N, et al. High prevalence of vitamin D deficiency in school age children in Tehran 2008: A red alert. Iranian Journal of Nutrition Sciences & Food Technology. 2013;7:389–98. doi: 10.1017/S1368980011000188. [Persian] [DOI] [PubMed] [Google Scholar]
- 35.Ghazi AA. Serum 25 (OH) vitamin D in healthy people in Tehran. J Med Counc Iran. 2001;19:197–202. [Persian] [Google Scholar]
- 36.Rabbani A, Alavian SM, Motlagh ME, Ashtiani MT, Ardalan G, Salavati A, et al. Vitamin D insufficiency among children and adolescents living in Tehran, Iran. J Trop Pediatr. 2009;55:189–91. doi: 10.1093/tropej/fmn078. [DOI] [PubMed] [Google Scholar]
- 37.Saki F, Dabbaghmanesh MH, Omrani GR, Bakhshayeshkaram M. Vitamin D deficiency and its associated risk factors in children and adolescents in southern Iran. Public Health Nutr. 2015:1–6. doi: 10.1017/S1368980015001925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Salek M, Hashemipour M, Aminorroaya A, Gheiratmand A, Kelishadi R, Ardestani PM, et al. Vitamin D deficiency among pregnant women and their newborns in Isfahan, Iran. Exp Clin Endocrinol Diabetes. 2008;116:352–6. doi: 10.1055/s-2008-1042403. [DOI] [PubMed] [Google Scholar]
- 39.Shakiba M, Nafei Z, Lotfi MH, Shajari A. Prevalence of vitamin D deficiency among female students in secondary guidance school in Yazd City. Acta Med Iran. 2009;47:209–14. [Google Scholar]
- 40.Jamali Z. Prevalence of Vitamin D Deficiency in female students in Rafsanjan city [dissertation] [Mashhad]: Payame Noor University; 2009. [Google Scholar]
- 41.Zahed N, Chehraza S. The Evaluation of prevalence of 25 _hydroxy vitamin D in hemodialysis patient. Med J Mashhad Univ Med Sci. 2015;57:879–83. [Persian] [Google Scholar]
- 42.Bonakdaran S, Varasteh A, Khaajeh-Dalouie M. Serum 25 hydroxy vitamin D3 and laboratory risk markers of cardiovascular diseases in type 2 diabetic patients. Iranian Journal of Endocrinology and Metabolism. 2010;11:504–9. [Persian] [Google Scholar]
- 43.Paknahad Z, Ahmadivasmehjani A, Maracy MR. Association of Serum 25-hydroxyvitamin D concentration and Markers of Metabolic Syndrome in adult women. Health System Research. 2015;11:317–26. [Persian] [Google Scholar]
- 44.Kaykhaei MA, Hashemi M, Narouie B, Shikhzadeh A, Rashidi H, Moulaei N, et al. High prevalence of vitamin D deficiency in Zahedan, southeast Iran. Ann Nutr Metab. 2011;58:37–41. doi: 10.1159/000323749. [DOI] [PubMed] [Google Scholar]
- 45.Savaj S, Ghods FJ. Vitamin D, parathyroid hormone, and bone mineral density status in kidney transplant recipients. Iran J Kidney Dis. 2012;6:295–9. [PubMed] [Google Scholar]
- 46.Hosseinpanah F, Pour SH, Heibatollahi M, Moghbel N, Asefzade S, Azizi F. The effects of air pollution on vitamin D status in healthy women: A cross sectional study. BMC Public Health. 2010;10:519. doi: 10.1186/1471-2458-10-519. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Ataie-Jafari A, Rahmat AB, Abbasi F, Cheong Loke S, Qorbani M, Larijani B. Vitamin D status and associated factors in recent-onset type 1 diabetic children in Iran. J Diabetes Metab Disord. 2012;11:12. doi: 10.1186/2251-6581-11-12. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Javadian Y, Adabi M, Heidari B, Babaei M, Firouzjahi A, Ghahhari BY, et al. Quadriceps Muscle Strength Correlates With Serum Vitamin D and Knee Pain in Knee Osteoarthritis. Clin J Pain. 2017;33:67–70. doi: 10.1097/AJP.0000000000000358. [DOI] [PubMed] [Google Scholar]
- 49.Larijani B, Hossein-Nezhad A, Feizabad E, Maghbooli Z, Adibi H, Ramezani M, et al. Vitamin D deficiency, bone turnover markers and causative factors among adolescents: A cross-sectional study. J Diabetes Metab Disord. 2016;15:46. doi: 10.1186/s40200-016-0266-2. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Mirsaeid Ghazi AA, Rais Zadeh F, Pezeshk P, Azizi F. Seasonal variation of serum 25 hydroxy D3 in residents of Tehran. J Endocrinol Invest. 2004;27:676–9. doi: 10.1007/BF03347502. [DOI] [PubMed] [Google Scholar]
- 51.Saki F, Omrani GR, Pouralborz Y, Dabbaghmanesh MH. Vitamin D deficiency and the associated factors in children with type 1 diabetes mellitus in southern Iran. Int J Diabetes Dev Ctries. 2016:1–7. [Google Scholar]
- 52.Zolfaghari F, Faridmoayer A, Soleymani B, Taji M, Mahabadi M. A Survey of Vitamin D Status in Patients with Degenerative Diseases of the Spine. Asian Spine J. 2016;10:834–42. doi: 10.4184/asj.2016.10.5.834. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Hossein-Nezhad A, Eshaghi SM, Maghbooli Z, Mirzaei K, Shirzad M, Curletto B, et al. The role of vitamin D deficiency and vitamin d receptor genotypes on the degree of collateralization in patients with suspected coronary artery disease. Biomed Res Int. 2014;2014:304250. doi: 10.1155/2014/304250. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Heidari B, Haji Mirghassemi MB. Seasonal variations in serum vitamin D according to age and sex. Caspian J Intern Med. 2012;3:535–40. [ PMC Free Article] [PMC free article] [PubMed] [Google Scholar]
- 55.Shamsian AA, Rezaee SA, Rajabiian M, Moghaddam HT, Saeidi M, Bahreini A. Study of the Vitamin D Levels in Patients Referred to Clinical Laboratories in Mashhad in 2015 and their Relationship with the Patients'Lipid Profiles. Electron Physician. 2016;8:2269–73. doi: 10.19082/2269. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Abbasian M, Chaman R, Amiri M, Ajami ME, Jafari-Koshki T, Rohani H, et al. Vitamin D Deficiency in Pregnant Women and Their Neonates. Glob J Health Sci. 2016;8:54008. doi: 10.5539/gjhs.v8n9p83. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Chitsaz A, Maracy M, Basiri K, Izadi Boroujeni M, Tanhaei AP, Rahimi M, et al. 25-hydroxyvitamin d and severity of Parkinson's disease. Int J Endocrinol. 2013;2013:689149. doi: 10.1155/2013/689149. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Haidari FP, Zakerkish MD, Karandish MP, Saki AP, Pooraziz SM. Association between Serum Vitamin D Level and Glycemic and Inflammatory Markers in Non-obese Patients with Type 2 Diabetes. Iran J Med Sci. 2016;41:367–73. [ PMC Free Article] [PMC free article] [PubMed] [Google Scholar]
- 59.Fallahi M, Afjeh A, Saneifard H, Namazi N, Kazemian M, Tabatabaee S. Comparison of Vitamin D Level in Preterm and Term Infant–Mother Pairs: A Brief Study. Iranian Journal of Neonatology. 2016;7:32–6. [Google Scholar]
- 60.Kelishadi R, Qorbani M, Motlagh ME, Heshmat R, Poursafa P, Bahreynian M. Prevalence of Vitamin D Deficiency according to Climate Conditions among a Nationally Representative Sample of Iranian Adolescents: The CASPIAN-III Study. Int J Pediatr. 2016;4:1903–10. [Google Scholar]
- 61.Entezari-Maleki T, Hajhossein Talasaz A, Salarifar M, Hadjibabaie M, Javadi MR, Bozorgi A, et al. Plasma Vitamin D Status and Its Correlation with Risk Factors of Thrombosis, P-selectin and hs-CRP Level in Patients with Venous Thromboembolism;the First Study of Iranian Population. Iran J Pharm Res. 2014;13:319–27. [ PMC Free Article] [PMC free article] [PubMed] [Google Scholar]
- 62.Asadi M, Saeidifard F, Qorbani M, Adabi K. Vitamin D deficiency and mode of delivery: A study in Tehran Women General Hospital. Tehran University Medical Journal TUMS Publications. 2015;73:442–6. [Persian] [Google Scholar]
- 63.Sobouti B, Riahi A, Fallah S, Ebrahimi M, Shafiee Sabet A, Ghavami Y. Serum 25-Hydroxyvitamin D Levels in Pediatric Burn Patients. Trauma Mon. 2016;21:e30905. doi: 10.5812/traumamon.30905. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Ardestani PM, Salek M, Keshteli AH, Nejadnik H, Amini M, Hosseini SM, et al. Vitamin D status of 6- to 7-year-old children living in Isfahan, Iran. Endokrynol Pol. 2010;61:377–82. [PubMed] [Google Scholar]
- 65.Hejazi V, Hejazi ME. Vitamin D Level in Asthmatic Patients, Tabriz City, Iran. Asian J Med Pharm Res. 2015;5:27–33. [Google Scholar]
- 66.Rafraf M, Hasanabad SK, Jafarabadi MA. Vitamin D status and its relationship with metabolic syndrome risk factors among adolescent girls in Boukan, Iran. Public Health Nutr. 2014;17:803–9. doi: 10.1017/S1368980013003340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Taha SA, Dost SM, Sedrani SH. 25-Hydroxyvitamin D and total calcium: Extraordinarily low plasma concentrations in Saudi mothers and their neonates. Pediatr Res. 1984;18:739–41. doi: 10.1203/00006450-198408000-00013. [DOI] [PubMed] [Google Scholar]
- 68.Sedrani SH. Low 25-hydroxyvitamin D and normal serum calcium concentrations in Saudi Arabia: Riyadh region. Ann Nutr Metab. 1984;28:181–5. doi: 10.1159/000176801. [DOI] [PubMed] [Google Scholar]
- 69.Sadiniya A, Larijani B, Jalaliniya S, Farzadfar F, Keshtkar A, Rezai A, et al. The trend of vitamin D deficiency prevalence in Iranian population in Islamic Republic of Iran based on province living in the period 1990-2010. Iran J Diabetes Lipid Disord. 2013;12:574–84. [Persian] [Google Scholar]
- 70.Du X, Greenfield H, Fraser DR, Ge K, Trube A, Wang Y. Vitamin D deficiency and associated factors in adolescent girls in Beijing. Am J Clin Nutr. 2001;74:494–500. doi: 10.1093/ajcn/74.4.494. [DOI] [PubMed] [Google Scholar]
- 71.Dawodu A, Agarwal M, Hossain M, Kochiyil J, Zayed R. Hypovitaminosis D and vitamin D deficiency in exclusively breast-feeding infants and their mothers in summer: A justification for vitamin D supplementation of breast-feeding infants. J Pediatr. 2003;142:169–73. doi: 10.1067/mpd.2003.63. [DOI] [PubMed] [Google Scholar]
- 72.Alagol F, Shihadeh Y, Boztepe H, Tanakol R, Yarman S, Azizlerli H, et al. Sunlight exposure and vitamin D deficiency in Turkish women. J Endocrinol Invest. 2000;23:173–7. doi: 10.1007/BF03343702. [DOI] [PubMed] [Google Scholar]
- 73.Ziaee A, Javadi A, Javadi M, Zohal M, Afaghi A. Nutritional status assessment of Minodar residence in Qazvin city, Iran: Vitamin D deficiency in sunshine country, a public health issue. Glob J Health Sci. 2012;5:174–9. doi: 10.5539/gjhs.v5n1p174. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Hilger J, Friedel A, Herr R, Rausch T, Roos F, Wahl DA, et al. A systematic review of vitamin D status in populations worldwide. Br J Nutr. 2014;111:23–45. doi: 10.1017/S0007114513001840. [DOI] [PubMed] [Google Scholar]
- 75.Brooke OG, Brown IR, Bone CD, Carter ND, Cleeve HJ, Maxwell JD, et al. Vitamin D supplements in pregnant Asian women: Effects on calcium status and fetal growth. Br Med J. 1980;280:751–4. doi: 10.1136/bmj.280.6216.751. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Maghbooli Z, Hossein-Nezhad A, Shafaei AR, Karimi F, Madani FS, Larijani B. Vitamin D status in mothers and their newborns in Iran. BMC Pregnancy Childbirth. 2007;7:1. doi: 10.1186/1471-2393-7-1. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Maxwell JD, Ang L, Brooke OG, Brown IR. Vitamin D supplements enhance weight gain and nutritional status in pregnant Asians. Br J Obstet Gynaecol. 1981;88:987–91. doi: 10.1111/j.1471-0528.1981.tb01686.x. [DOI] [PubMed] [Google Scholar]
- 78.Fuleihan GE-H. Vitamin D deficiency in the Middle East and its health consequences for children and adults. Clin Rev Bone Miner Metab. 2009;7:77–93. [Google Scholar]
- 79.Batieha A, Khader Y, Jaddou H, Hyassat D, Batieha Z, Khateeb M, et al. Vitamin D status in Jordan: Dress style and gender discrepancies. Ann Nutr Metab. 2011;58:10–8. doi: 10.1159/000323097. [DOI] [PubMed] [Google Scholar]
- 80.Sedrani SH, Elidrissy AW, El Arabi KM. Sunlight and vitamin D status in normal Saudi subjects. Am J Clin Nutr. 1983;38:129–32. doi: 10.1093/ajcn/38.1.129. [DOI] [PubMed] [Google Scholar]
- 81.Sedrani SH. Vitamin D status of Saudi men. Trop Geogr Med. 1984;36:181–7. [PubMed] [Google Scholar]
- 82.el-Sonbaty MR, Abdul-Ghaffar NU. Vitamin D deficiency in veiled Kuwaiti women. Eur J Clin Nutr. 1996;50:315–8. [PubMed] [Google Scholar]
- 83.Al-Jurayyan NA, El-Desouki ME, Al-Herbish AS, Al-Mazyad AS, Al-Qhtani MM. Nutritional rickets and osteomalacia in school children and adolescents. Saudi Med J. 2002;23:182–5. [PubMed] [Google Scholar]
- 84.Maghboli Z, Hossein Nezhad A, Shafaei A, Karimi F, Mdani FS, Larijani B. Vitamin D status in pregnant women and their newborns. Scientific Journal of Kurdistan University of Medical Sciences. 2006;11:64–73. [Persian] [Google Scholar]
- 85.Lo CW, Paris PW, Holick MF. Indian and Pakistani immigrants have the same capacity as Caucasians to produce vitamin D in response to ultraviolet irradiation. Am J Clin Nutr. 1986;44:683–5. doi: 10.1093/ajcn/44.5.683. [DOI] [PubMed] [Google Scholar]
- 86.Moradzadeh K, Keshtkar A, Hossein NA, Rajabian R, Nabipour I, Omrani G, et al. Normal values of vitamin D and prevalence of vitamin D deficiency among Iranian population. Scientific Journal of Kurdistan University of Medical Sciences. 2006;10:33–43. [Persian] [Google Scholar]
- 87.Awumey EM, Mitra DA, Hollis BW, Kumar R, Bell NH. Vitamin D metabolism is altered in Asian Indians in the southern United States: A clinical research center study. J Clin Endocrinol Metab. 1998;83:169–73. doi: 10.1210/jcem.83.1.4514. [DOI] [PubMed] [Google Scholar]