

Abstract
Centrally occurring salivary gland tumors are rare. Because of a considerable overlap between the clinical and histopathological features, this group of tumors often produces a diagnostic difficulty to the clinicians and oral pathologists. Acinic cell carcinoma (ACC) is an unusual, low-grade, malignant salivary gland tumor that represents approximately 2% of the salivary gland tumors with almost 90% arising in the parotid gland. The rest involve the submandibular and the minor salivary gland. ACC of the jaw is extremely rare and, to our knowledge, only 8 cases have been reported in the English literature. Herein, a case of primary intraosseous ACC of the mandible in a 31-year-old woman is presented. The present case is unique, as the central ACC has never been reported in a patient in the third decade of life. The complete surgical removal of the tumor was carried out under general anesthesia along with the extraction of teeth #31, #32, #41, and #42. The follow-up period of 1-year was uneventful.
Keywords: Carcinoma, Acinar cell, Central acinic cell carcinoma, Salivary gland neoplasms, Mandible
What’s Known
Acinic cell carcinoma of the jaw is extremely rare and, to our knowledge, only 8 cases have been reported in English literature.
What’s New
In the present case, provisional diagnose was keratocystic odontogenic tumor (KCOT); an odontogenic tumor. Central salivary gland tumors come last to mind when dealing with intraosseous swellings. The present case is one of the rarest possibilities as the provisional diagnosis was completely different to the histopathological diagnosis. Hence, this case highlights the importance of histopathology.
Introduction
Ectopic salivary gland tissues are found in various sites including centrally within maxilla and mandible. Neoplastic transformation of intraosseous salivary gland tissue is an uncommon phenomenon.1 Intraosseous acinic cell carcinoma (ACC) is extremely rare and only 8 cases have been reported so far in English literature.2 In both jaws, mandible accounts for 75% of all intraosseous salivary gland tumor cases.3 ACC occurs in all age groups with peak incidence noted in the 5th and 6th decade of life.4 Histologically, they show a uniform pattern of large cells with granular basophilic cytoplasm, often in an acinar arrangement.5 Despite apparent benign histological appearance, ACC can be invasive and occasionally metastasize. In general, management of ACC consists of complete surgical removal of the tumor. Radiotherapy is advised for recurrent, undifferentiated cases of ACC, tumors with positive margins, and tumors with cervical lymph node spread.4
Case Report
A 31-year-old woman presented to the Department of Oral Medicine NIMS Dental College, Jaipur (India) with a chief complaint of swelling on her lower front region of the jaw since 10 months. Initially, the swelling was small but it gradually increased up to the present size. Past medical and family history of the patient was non-contributory to the present swelling. Intraoral examination revealed a solitary swelling of buccal mucosa extending from #33 to #43. The color of the overlying mucosa was similar to the adjacent mucosa; vestibular obliteration was noted with relation to #42 and #43 (figure 1). The swelling was found to be tender and firm in consistency on intraoral palpation. There were no signs of paresthesia. Submandibular lymph nodes were non-palpable. Panoramic radiograph revealed a multilocular radiolucent lesion extending from #33 to #43 and the locules were separated by sclerotic margins. Occlusal derangement of #31 and #41 was noted (figure 2). Based on the clinical and radiographic examination, a provisional diagnosis of keratocystic odontogenic tumor was given with the differential diagnoses of ameloblastoma, aneurysmal bone cyst, central giant cell granuloma, and central hemangioma owing to the multilocular radiolucent pattern of the present lesion. A fine needle aspiration was done, which was non-conclusive. No incisional biopsy was taken. A complete surgical removal of the lesion was planned.
Figure 1.

Intraoral picture of the swelling reveals a bony swelling.
Figure 2.
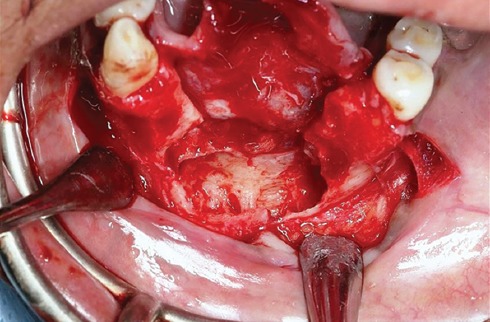
Intraoperative picture of the lesion shows surgical exposure of the lesion.
Surgical exposure was done under general anesthesia after the incision through the skin, dissection was carried out through subcutaneous tissues, platysma, deep fascia, and finally the pterygomassetric sling with periosteum was divided to approach the inferior border of the mandible and soft bone was removed till the inferior border of the mandible. Teeth #31, #32, #41, and #42 were extracted (figure 3). Resected specimen was sent to the Department of Oral and Maxillofacial Pathology for histopathological evaluation. Histopathological examination of hematoxylin and eosin stained sections revealed an encapsulated tissue (figure 4) composed of numerous serous acinar cells with abundant granular basophilic cytoplasm and round darkly stained eccentrically placed nucleus with multiple vacuolated cyst-like spaces (figure 5). The stroma was fibrovascular. Based on histopathological features, a final diagnosis of primary intraosseous microcystic ACC was given. One year follow-up period of the patient was uneventful. An informed consent from the patient was obtained for the publication of the case.
Figure 3.
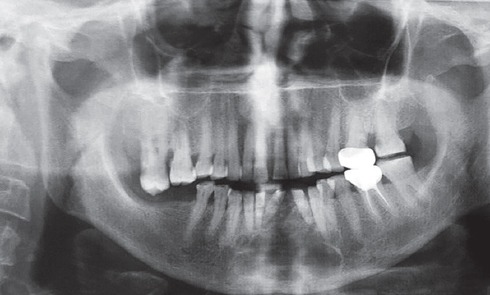
Panoramic radiograph reveals a multilocular radiolucent lesion of anterior mandible.
Figure 4.
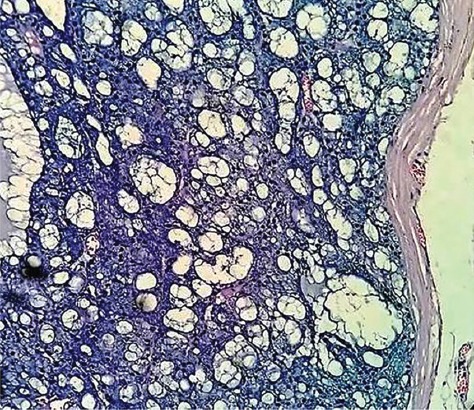
Photomicrograph reveals a well encapsulated tissue with numerous serous and acinar cells with prominent microcystic areas (Hematoxylin and Eosin stain, ×10).
Figure 5.
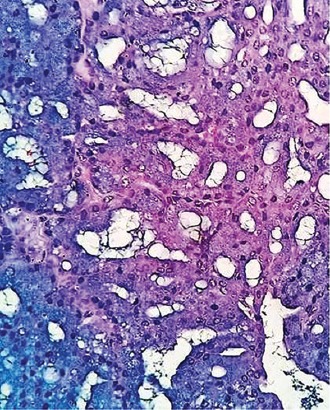
High power view shows serous acinar cells with abundant granular basophilic cytoplasm and round darkly stained eccentrically placed nucleus with multiple vacuolated cyst-like spaces (Hematoxylin and Eosin stain, ×40).
Discussion
The world health organization (WHO) described ACC as a malignant epithelial neoplasm of the salivary glands in which at least few neoplastic cells show serous acinar cell differentiation characterized by cytoplasmic zymogen secretory granules.4 Salivary ductal cells can also be a component of this neoplasm that most often occurs in the parotid gland and presents at a relatively younger age than other salivary gland tumors.6 This malignant tumor shows a female predilection.1 Godwin et al. described ACC as an entity for the first time over 50 years ago.5 The terms “acinar” and “serous” refer to the histological resemblance of tumor cells to the secretory parenchymatous cells of the parotid, found to be grouped in grape-like clusters and hence given the Latin name “acinus”.6
Primary intraosseous salivary gland neoplasms of the jaws are unusual. Central ACC of the jaw is an extremely rare neoplasm and exhaustive literature review could reveal only 8 such cases.1,3 Mandible is the most common site for intraosseous salivary gland neoplasm, accounting for 75% of all cases.3,6 Similar to the present case, Flood et al.7 reported a case of ACC in the mandible. Two theories for the central salivary gland neoplasms have been proposed; one suggests a neoplastic transformation in developmentally entrapped salivary gland tissue in the bone and the other suggests a metaplasia of epithelial lining of an odontogenic cyst.6 The present case belonged to the first category.
ACC may be found in all age groups, including children, with peak incidence noted within the 5th and 6th decades of life and that slow-growing swelling and pain may be the presenting symptoms.8,9 The present case was associated with a 31-year-old lady; however, pain was not an associated symptom in this case. Hiremath et al.2 reported a case of central ACC of the mandible in a female patient. Similar to the present case, the patient was female and the involved jaw was the mandible. Radiographic features of central ACC may mimic benign odontogenic tumors, central hemangioma, and giant cell granuloma.10 Histopathological examination is required for the final diagnosis. Hara et al.8 reported a case of mandibular ACC which was provisionally diagnosed as an odontogenic tumor and on the basis of histopathological features it was diagnosed as ACC. The present case was diagnosed provisionally as keratocystic odontogenic tumor (KCOT) and histopathological examination revealed the diagnosis of ACC. Primary intraoral ACCs usually present a diagnostic challenge to pathologists because of their great radiological and cytological similarities with benign tumors and with normal acinar component of the salivary gland, respectively.6 Radiographically, they mimic benign odontogenic lesions (i.e. ameloblastoma and KCOT). Histological differential diagnoses include clear cell carcinoma, Warthin’s tumor, mucoepidermoid carcinoma, and oncocytoma.11
Histopathologically, ACCs are defined by serous and acinar cell differentiation.8 However, several histological patterns are recognized including acinar, intercalated ductal, vacuolated, clear and non-specific glandular and solid-lobular, microcystic, papillary-cystic and follicular growth patterns.9 The present case was diagnosed as microcystic form.
Occasional cases of dedifferentiation from a low-grade to a high-grade malignancy have been reported. These tumors are characterized by cytological pleomorphism, increased mitotic and proliferation indices, and have a worse prognosis.2-4 Attempts have been made to grade ACCs histologically; however, they have been debatable and inconsistent. Features that are often associated with more aggressive tumors include frequent mitosis, focal necrosis, neural invasion, pleomorphism, infiltration, and stromal hyalinization.12 Most of the reported central ACCs were low-grade and showed favorable prognosis. They seldom metastasize but they have a strong tendency to recur.
A literature review revealed that central ACC has been reported in women aged 84,3 67,8 and 652 years. Hence, our finding of central ACC in a 31-year-old woman is rare. Surgery is the treatment of choice for central ACC and postoperative radiotherapy may be useful for recurrent, undifferentiated cases of ACC, positive margins, and advanced tumors with cervical lymph node spread.4 The present case was treated surgically and 1-year follow-up of the patient was uneventful.
Conclusion
Central ACCs are rare lesions and show favorable prognosis. Dental surgeons should be aware of this rare entity, emphasizing the need for proper histopathological evaluation. After surgery, patients should be kept on a careful follow-up; owing to the high recurrence rate of this tumor.
Conflict of Interest: None declared.
References
- 1.Ferretti C, Coleman H, Altini M, Meer S. Intraosseous myoepithelial neoplasms of the maxilla: Diagnostic and therapeutic considerations in 5 South African patients. J Oral Maxillofac Surg. 2003;61:379–86. doi: 10.1053/joms.2003.50075. [DOI] [PubMed] [Google Scholar]
- 2.Hiremath V, Mishra N, Patil SG. Intraosseous acinic cell carcinoma. Niger J Clin Pract. 2013;16:386–8. doi: 10.4103/1119-3077.113470. [DOI] [PubMed] [Google Scholar]
- 3.Nakazawa M, Ohnishi T, Iwai S, Sakuda M. Central acinic cell carcinoma of the mandible. Report of a case. Int J Oral Maxillofac Surg. 1998;27:448–50. doi: 10.1016/s0901-5027(98)80035-0. [DOI] [PubMed] [Google Scholar]
- 4.Oliveira LR, Soave DF, da Costa JPO, Ribeiro-Silva A. Acinic cell carcinoma of parotid gland: Report of three cases and literature review. Revista Portuguesa de Estomatologia, Medicina Dentária e Cirurgia Maxilofacial. 2010;51:5–11. [Google Scholar]
- 5.Godwin JT, Foote FW, Jr, Frazell EL. Acinic cell adenocarcinoma of the parotid gland;report of twenty-seven cases. Am J Pathol. 1954;30:465–77. [ PMC Free Article] [PMC free article] [PubMed] [Google Scholar]
- 6.Barnes L, Eveson JW, Reichart P, Sidransky D. World Health Organization Classification of Tummours: Pathology and Genetics of Head and Neck Tumours. Lyon: IARC Press; 2005. [Google Scholar]
- 7.Flood TR, Maharaja BB, MacDonald DG, Giri DD. Central acinic cell carcinoma of the mandible: Report of a case. Br J Oral Maxillofac Surg. 1991;29:26–8. doi: 10.1016/0266-4356(91)90169-6. [DOI] [PubMed] [Google Scholar]
- 8.Hara I, Ozeki S, Okamura K, Toshitani K, Taniguchi K, Honda T, et al. Central acinic cell carcinoma of the mandible. Case report. J Craniomaxillofac Surg. 2003;31:378–82. doi: 10.1016/j.jcms.2003.06.001. [DOI] [PubMed] [Google Scholar]
- 9.William SG, Maynard HK, Barnet LM. “A Text book of Oral Pathology”, Tumors of the Salivary Glands. 4th ed. Philadelphia: W. B. Saunders; 2000. p. 246. [Google Scholar]
- 10.Bajpai M, Agarwal D, Bhalla A, Kumar M, Garg R, Kumar M. Multilocular unicystic ameloblastoma of mandible. Case Rep Dent. 2013;2013:835892. doi: 10.1155/2013/835892. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Prasad M, Kraus DH. Acinic cell carcinoma of the parotid gland presenting as an external auditory canal mass. Head Neck. 2004;26:85–8. doi: 10.1002/hed.10347. [DOI] [PubMed] [Google Scholar]
- 12.Buiret G, Ceruse P, Ramade A, Carrie C, Pommier P. Acinic cell carcinoma of the parotid gland with skull base invasion: Case study, managed by exclusive external 3D radiation therapy. Eur Ann Otorhinolaryngol Head Neck Dis. 2012;129:111–4. doi: 10.1016/j.anorl.2011.02.014. [DOI] [PubMed] [Google Scholar]