

Abstract
This study aimed to investigate the role of necroptosis in the neuroprotection of hydrogen in a mouse model of cerebral ischemia/reperfusion (I/R) injury. C57BL mice were randomly divided into sham group, I/R group, hydrogen/oxygen group (HO), nitrogen/oxygen group (NO). Middle cerebral artery occlusion (MCAO) for 1 hour followed by reperfusion was introduced to animals which were allowed to inhale 66.7% hydrogen/33.3% oxygen for 90 minutes since the beginning of reperfusion. Mice in NO group inhaled 66.7% nitrogen/33.3% oxygen. 24 hours after MCAO, brain infarction, brain water content and neurological function were evaluated. The protein expression of mixed lineage kinase domain like protein (MLKL) was detected at 3, 6, 12, 24 and 72 hours after reperfusion in HO group and the protein and mRNA expression of MLKL at 24 hours after MCAO in four groups. Hydrogen inhalation significantly reduced infarct volume, attenuated brain edema and improved neurobehavioral deficit in MCAO mice. The MLKL expression increased after MCAO and peaked at 6–24 hours after reperfusion. However, hydrogen inhalation had no significant effect on the MLKL expression at transcriptional and translational levels after MCAO. This study indicates high concentration hydrogen improves mouse neurological outcome after cerebral I/R injury independent of anti-necroptosis.
Keywords: high concentration hydrogen; necroptosis, ischemia/reperfusion, mixed lineage kinase domain like protein, neurological function
INTRODUCTION
Stroke is caused by a poor blood flow to the brain and ischemic stroke is a major type of stroke in clinical practice.1 Stroke has been the second most common cause of death following ischemic heart disease, and accounts for 9% of all deaths worldwide.2 Moreover, it has high disability and recurrence rate, increasing the economic burdens to the family and the society. However, the thrombolytic therapy as the only approved treatment for ischemic stroke is limited due to the short time window and the efficacy of other therapies has not been confirmed in clinical trials so far, which is partially ascribed to the incomplete understanding of pathogenesis of stroke.
It has been confirmed that the pathogenesis of stroke is closely related to the activation excitotoxic glutamatergic signaling, ionic imbalance, and excess production of reactive oxygen species (ROS).3,4,5,6 In recent years, increasing studies focus on the role of programmed cell death (PCD) in the pathogenesis of stroke. It has been confirmed that apoptosis and autophagy are the major modes of PCD, and traditionally necrosis is regarded as a deranged or accidental cell demise that is a passive process caused by overwhelming stress.7 In recent years, it has been revealed that necrotic cell death, at least in part, can be a well regulated and orchestrated event as apoptosis, which is termed “necroptosis”.8 Currently, studies have indicated that necroptosis play an important role in the pathogenesis of ischemic stroke, hemorrhagic stroke, and cerebral hypoxia/ischemia injury.9,10,11
Hydrogen has been used as a physiologically inert gas in deep diving for the prevention of nitrogen narcosis.12 However, numerous studies have confirmed the anti-oxidative, anti-inflammatory and anti-apoptotic capabilities of hydrogen in a variety of animal models and clinical trials since Ohsawa et al.13 reported that hydrogen inhalation could protect the brain against cerebral ischemia/reperfusion (I/R) injury by selectively neutralizing hydroxyl radicals and peroxynitrite. In most studies, the concentration of hydrogen is usually no more than 4% due to safety concerns. Recently, our group employed high concentration hydrogen (HCH) (67% hydrogen and 33% oxygen) in the treatment of several diseases in animal models, and its protective effects were confirmed.14,15,16,17 This mixed gas is produced using an AMS-H-01 hydrogen/oxygen nebulizer (Asclepius, Shanghai, China), which can produce hydrogen and oxygen by electrolyzing water.
This study was undertaken to investigate whether HCH protected the brain against I/R injury via anti-necroptosis in a mouse model.
MATERIALS AND METHODS
Animals and grouping
The whole study was approved by the Animal Care and Use Committee of Shanghai Jiao Tong University School of Medicine, Shanghai, China (No. A2015-011). Male C57BL/6 mice weighing 20–25 g (n = 130) were purchased from the Experimental Animal Center of Shanghai Jiao Tong University School of Medicine. One hundred of them were randomly divided into four groups: sham operation group, middle cerebral artery occlusion (MCAO)/reperfusion (I/R) group, I/R + nitrogen/oxygen (NO) group and I/R + hydrogen/oxygen (HO) group (n = 25 per group). The rest of them were used to evaluate protein expression at different time points after reperfusion.
MCAO model establishment
Mice were anesthetized by intraperitoneal injection of ketamine (80 mg/kg) and xylazine (10 mg/kg). A middle line incision was made at the neck, and the carotid artery was separated carefully. Then, a monofilament suture (Doccol, Sharon, MA, USA) was inserted into the internal carotid artery (ICA). Rectal temperature was maintained at 37.0°C during and after surgery with a temperature controlled heating pad. The regional cerebral blood flow (rCBF) was monitored using laser Doppler flowmetry (moor VMS-LDF2, Moor Instruments, Axminster, UK). Animals whose blood flow did not reduce to 20% were excluded. The monofilament suture was removed 1 hour for reperfusion.
Treatments
In sham group, mice were anesthetized, and a midline incision was made at the neck. The carotid artery was separated without occlusion. In I/R group, the left internal carotid artery was occluded, followed by reperfusion 1 hour later. In HO group, the I/R mice were exposed to HCH for 90 minutes since the beginning of reperfusion. In brief, mice were placed in a closed plastic box (28 cm × 18 cm × 14 cm), which was flushed with 67% hydrogen and 33% oxygen at a rate of 3,000 mL/min. The AMS-H-01 hydrogen/oxygen nebulizer (Asclepius) was used, which was designed to electrolyze water to produce HCH. During the HCH exposure, the hydrogen concentration in the box was monitored with a hydrogen detector (MD2XP-3140; New Cosmos, Osaka, Japan). In NO group, the mice were exposed to 67% nitrogen and 33% oxygen.
Detection of infarct volume by 2,3,5-triphenyltetrazolium hydrochloride (TTC) staining
After 24-hour reperfusion, the brain was collected, sectioned coronally at 1-mm interval, and stained with TTC at 37°C for 20 minutes. Then, brain sections were fixed in 4% paraformaldehyde and photographed with a digital camera (Canon IXUS175, Tokyo, Japan). The images were obtained for the measurement of infarct volume with Image-Pro software18 and Swanson's method.19 The infarct percentage was used for the evaluation of infarction.
Detection of brain water content
Mice were anesthetized intraperitoneally and the brain was quickly collected. The right hemisphere, left hemisphere, cerebellum, and brain stem were separated. The brain tissues were weighed immediately as wet weight, and then placed in an oven (WS70-1) at 65°C. Dry weight was obtained 48 hours later. The brain water content of each part was calculated as follow: wet to dry (W/D) ratio = [(wet weight − dry weight)/wet weight] × 100%.20
Neurological scoring
At 24-hour after reperfusion, neurological function was scored in a blind manner as previously described.21 The scores were divided into five grades with the minimum score of 0, and the maximum score of 4 (severest deficit). Menzies neurological score are as following: 0, No apparent deficits; 1, contralateral forelimb flexion; 2, Decreased grip of the contralateral forelimb while tail pulled; 3, Spontaneous movement in all directions or contralateral circling only if pulled by tail; 4, Spontaneous contralateral circling.21
Real-time PCR
After 24-hour reperfusion, the total RNA was extracted from the brain using TRIzol reagent (Invitrogen, Carlsbad, CA, USA) according to manufacturer's instructions and then processed for reverse-transcription into cDNA in a 20-μL mixture containing 1 μg of total RNA using FastQuant RT Kit with gDNase (Tiangen, Beijing, China). The mRNA expression of mixed lineage kinase domain like protein (MLKL) was detected using Power SYBR Green PCR Master Mix (Thermo Fisher Scientific, Hemel Hempstead, UK), and GAPDH served as an internal reference. The primers used for PCR were as follows: MLKL, 5'-CTG AGG GAA CTG CTG GAT AGA G-3'(forward) and 5'-CGA GGA AAC TGG AGC TGC TGA T-3'(reverse); GAPDH, 5'-CCT CGT CCC GTA GAC AAA ATG GT-3'(forward) and 5'-TTG AGG TCA ATG AAG GGG TCG T-3'(reverse). The mRNA expression was analyzed using the 2-ΔΔCT method. All experiments were carried out in triplicate.
Western blot assay
At 3, 6, 12, 24 and 72 hours after reperfusion, mice were sacrificed, and the brain was collected. The left cerebral hemisphere was processed for the detection of MLKL protein expression by western blot assay. In brief, brain tissues were homogenized in RIPA buffer (P1003B, Beyotime,wuhan, China) containing protease inhibitor cocktail (P8340, Sigma, St. Louis, MO, USA), and then sonicated on ice. After centrifugation, the supernatant was collected for western blot assay. An aliquot of 20 mg protein from each sample was separated by SDS-PAGE and then transferred onto a nitrocellulose membrane. The membrane was blocked with 5% nonfat milk in PBST for 2 hours (pH 7.4) and then incubated with primary antibodies against MLKL (1:1,000; ab194699, Abcam, Shanghai, China) or β-actin (1:5,000; C16678, Anbo Biotechnology, San Francisco, CA, USA) at 4°C overnight. After incubation with secondary antibody for 2 hours at room temperature, visualization was done with a chemiluminescence apparatus (ImageQuant LAS 4000mini, GE Healthcare, Lafayette, CO, USA). The optical density (OD) was measured with Image-Pro software, and the OD of MLKL was normalized to that of β-actin as the relative protein expression of MLKL.
Statistical analysis
Data are expressed as the mean ± standard error (SEM), and statistical analysis was performed using GraphPad Prism software (GraphPad Software, La Jolla, CA, USA). Comparisons were done among groups by using one-way analysis of variance (ANOVA) followed by Turkey test. A value of P < 0.05 was considered statistically significant.
RESULTS
Infarct ratio
To ensure success and stability of surgery, a laser Doppler flowmeter was used to monitor the CBF (Figure 1A). After 1-hour ischemia and 24-hour reperfusion, TTC staining was performed and infarct volume was determined. Results showed the infarct ratio was 39.51 ± 5.30% in I/R group, 20.21 ± 4.43% in HO group and 34.83 ± 3.53% in NO group, and no infarction was observed in sham group (Figure 1B). The infarct ratio in HO group was significantly lower than in I/R group and NO group (P < 0.001; Figure 1B), but there was no marked difference between NO group and I/R group.
Figure 1.

High concentration hydrogen (HCH) reduces infarct ratio in mice with cerebral ischemia/reperfusion (I/R) injury.
Note: (A) Monitoring of cerebral blood flow (CBF); (B) 2,3,5-triphenyltetrazolium hydrochloride (TTC) staining of brain sections and quantification of infarct ratio (n = 8 per group). After 1-hour ischemia and 24-hour reperfusion, TTC staining and determination of infarct ratio were done in mice. Results showed 90-minute HCH inhalation since the beginning of reperfusion significantly reduced infarct ratio in mice with I/R injury, but the neurological function and infarct ratio were comparable between I/R group and I/R + nitrogen/oxygen (NO) group. Data are expressed as the mean ± SEM, and analyzed by one-way analysis of variance followed by Turkey test. ###P < 0.001, vs. I/R group. HO: I/R + hydrogen/oxygen group; min: minute(s).
Brain edema
Cerebral I/R caused a significant increase in the brain water content in I/R group as compared to sham group (81.36 ± 1.29% vs. 78.27 ± 0.38%, P < 0.001; Figure 2A). However, HCH treatment markedly reduced the brain water content after cerebral I/R injury (79.31 ± 0.69% vs. 81.36 ± 1.29%, P < 0.01; Figure 2A), but there was no significant difference between NO group and I/R group (81.36 ± 1.29% vs. 82.19 ± 0.74%, P > 0.05; Figure 2A).
Figure 2.
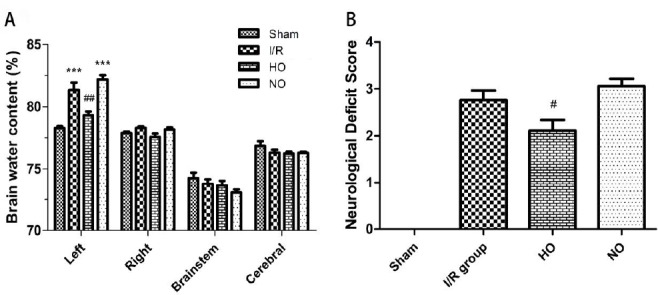
High concentration hydrogen (HCH) improves brain edema and neurological function in mice with cerebral ischemia/reperfusion (I/R) injury.
Note: (A) Brain water content as an indicator of brain edema (n = 5 per group); (B) Neurological score in different groups (n = 17-18 per group). After 1-hour ischemia and 24-hour reperfusion, the neurological function was assessed, and the brain was harvested for the quantification of water content of different brain structures. Data are expressed as the mean ± SEM, and analyzed by one-way analysis of variance followed by Turkey test. ***P < 0.001, vs. sham group; #P < 0.05, ##P < 0.01, vs. I/R group. HO: I/R + hydrogen/oxygen group; NO: I/R + nitrogen/oxygen group.
Neurological function
Cerebral I/R injury caused a significant neurological deficit in I/R group (2.77 ± 0.83). Importantly, the neurological deficit of cerebral I/R mice was markedly improved after HCH treatment (2.11 ± 0.96 vs. 2.76 ± 0.83, P < 0.05; Figure 2B), but there was no significant difference between NO group and I/R group (3.06 ± 0.66 vs. 2.76 ± 0.83, P > 0.05; Figure 2B).
Temporal change in MLKL protein expression
MLKL is a key molecule in the necrosis signaling pathway.22,23 and thus the protein expression of MLKL was detected at different time points after reperfusion, aiming to assess its temporal change. Our study showed MLKL protein expression increased after 3-hour reperfusion and then peaked at 6-24 hours, but decreased significantly after 72-hour reperfusion (Figure 3A).
Figure 3.

Mixed lineage kinase domain like protein (MLKL) protein and mRNA expression in the brain of mice with cerebral ischemia/reperfusion (I/R) injury.
Note: (A) MLKL protein expression in the brain at 3, 6, 12, 24, and 72 h after reperfusion (n = 5 per group). (B) MLKL protein and mRNA expression in the brain at 24 h after reperfusion (n = 3-5 per group). MLKL protein expression increased at 3 h after reperfusion, peaked at 6-24 h and thereafter decreased at 72 h after reperfusion. In addition, the MLKL protein and mRNA expression was comparable between I/R + hydrogen/oxygen (HO) group and I/R + nitrogen/oxygen (NO) group. *P < 0.05, **P < 0.01, ***P < 0.001, vs. sham group; #P < 0.05, vs. 3 h group. h: Hour(s).
MLKL protein and mRNA expression after cerebral I/R injury
As mentioned above, the MLKL protein expression in the injured hemisphere peaked at 6-24 hours after reperfusion. Thus, the MLKL protein and mRNA expression was further detected at 24 hours after reperfusion in different groups. Our results showed the protein and mRNA expression of MLKL increased significantly at 24 hours after reperfusion as compared to sham group, but HCH had no influence on the expression of MLKL at translational and transcriptional levels (P > 0.05; Figure 3B).
DISCUSSION
This study further confirmed that HCH could exert neuroprotective effects on cerebral I/R injury, demonstrated by the reduction in infarct ratio, decrease in brain water content and improvement of neurological function after cerebral I/R injury. In addition, cerebral I/R increased the MLKL expression in a time dependent manner: it increased at 3 hours after reperfusion, peaked at 6-24 hours, but reduced after 72-hour reperfusion. However, HCH treatment failed to inhibit the necroptosis in the mouse brain after I/R injury.
Stroke may trigger a variety of biochemical and molecular mechanisms leading to the neurological dysfunction including the activation excitotoxic glutamatergic signaling, ionic imbalance, and excess production of ROS. In recent years, hydrogen was found to be a potent antioxidant and has been widely used in the treatment of diseases in animal models and clinical trials.24 As compared to other available antioxidants, hydrogen has some advantages: it may not disturb metabolic redox reactions or affect ROS because it mainly reacts with highly toxic ROS hydroxyl radicals and peroxynitrite; it has favorable distribution characteristics and can penetrate biomembranes and diffuse through barriers into cellular components; its metabolite (water) is not harmful to cells. Although the neuroprotective effects of hydrogen gas have been confirmed in some animal models and even in clinical trials, the concentration of hydrogen gas used is no higher than 4% due to safety concerns. In recent years, a new hydrogen generator which can produce 66.7% hydrogen and 33.3% oxygen by electrolyzing water was developed by the Asclepius Company. With a specific technique, it may avoid the risk for explosion of hydrogen at this high concentration. The protective effects of HCH (66.7% hydrogen and 33.3% oxygen) were also revealed in our previous studies.15,16 However, the neuroprotective effects of HCH on stroke are still unclear. Our results showed HCH inhalation for 90 minutes since the beginning of reperfusion could also exert neuroprotection against cerebral I/R injury (reductions in infarct ratio and brain water content, and improvement of neurological function), which were consistent with findings from MCAO rats treated with HCH inhalation for 2 hours. However, the specific mechanism underlying the protective effects of HCH remains to be elucidated.
It has been confirmed that PCD plays a crucial role in the pathogenesis of stroke, and regulation of PCD is promising for the treatment of stroke. Necroptosis is a new mode of PCD and also closely related to the pathogenesis of ischemic stroke, hemorrhagic stroke and cerebral hypoxia/ischemia, and inhibition of necroptosis has also been found to be neuroprotective in several animal models.10,25,26,27 Receptor-interacting protein 1 (RIP1), RIP3 and MLKL are the key molecules in the necroptosis signaling pathways and have been used as markers of necroptosis.28 Pseudokinase MLKL is a substrate of RIP3 and may serve as a major executioner of necroptosis.22,23 In this study, MLKL was employed as a marker of necroptosis. Although the role of necroptosis in stroke has been widely investigated, the temporal change in necroptosis is poorly understood. Our results showed the necroptosis increased at 3 hours after reperfusion, peaked at 6-24 hours, but decreased after 72-hour reperfusion. This indicates necroptosis is an early mechanism of cell death after ischemic stroke, and early treatment targeting necroptosis might be neuroprotective. However, post-occlusion HCH treatment failed to inhibit necroptosis in MCAO mice. This suggests that the neuroprotection of HCH seems to be independent of anti-necroptosis. Our group showed HCH inhalation could attenuate I/R injury in a rat model via inhibiting apoptosis, oxidative stress and inflammation,15 and anti-autophagy is also involved in the neuroprotection of hydrogen gas (1.3%) in C57BL/6J mice with global cerebral ischemia.29 In respect of PCD, whether anti-apoptosis (and anti-autophagy) plays a major role in the neuroprotective effects of HCH is needed to be further investigated.
There were still limitations in this study.First, the MLKL expression immediately after ischemia was not detected; second, it is necessary to use Nec-1 to inhibit necroptosis and then investigate the role of necroptosis in the neuroprotection of HCH; third, whether HCH initiated during ischemia is also neuroprotective and its neuroprotection has involvement of anti-necroptosis are needed to be further investigated. It has been confirmed that cells may undergo necroptosis as an alternative means of cell death under conditions where caspases fail to be activated,30 and there is also interaction between necroptosis and autophagy.31 Thus, the specific roles of different PCD in the neuroprotection of HCH are warranted further investigation.
Footnotes
Conflicts of interest
The authors declare that there is no conflict of interest in this paper.
Financial support
This study was supported by the National Natural Science Foundation of China, No. 81772015 to WWL and No. 81371316 to XJS.
Research ethics
The study protocol was approved by the Animal Care and Use Committee of Shanghai Jiao Tong University School of Medicine, Shanghai, China (No. A2015-011).
Data sharing statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Plagiarism check
Checked twice by iThenticate.
Peer review
Externally peer reviewed.
Funding: This study was supported by the National Natural Science Foundation of China, No. 81772015 to WWL and No. 81371316 to XJS.
REFERENCES
- 1.Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart Disease and Stroke Statistics-2017 Update: A Report from the American Heart Association. Circulation. 2017;135:e146–e603. doi: 10.1161/CIR.0000000000000485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kim AS, Johnston SC. Temporal and geographic trends in the global stroke epidemic. Stroke. 2013;44:S123–S125. doi: 10.1161/STROKEAHA.111.000067. [DOI] [PubMed] [Google Scholar]
- 3.Martin HG, Wang YT. Blocking the deadly effects of the NMDA receptor in stroke. Cell. 2010;140:174–176. doi: 10.1016/j.cell.2010.01.014. [DOI] [PubMed] [Google Scholar]
- 4.Besancon E, Guo S, Lok J, Tymianski M, Lo EH. Beyond NMDA and AMPA glutamate receptors: emerging mechanisms for ionic imbalance and cell death in stroke. Trends Pharmacol Sci. 2008;29:268–275. doi: 10.1016/j.tips.2008.02.003. [DOI] [PubMed] [Google Scholar]
- 5.Shirley R, Ord EN, Work LM. Oxidative stress and the use of antioxidants in stroke. Antioxidants (Basel) 2014;3:472–501. doi: 10.3390/antiox3030472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Davis SM, Pennypacker KR. Targeting antioxidant enzyme expression as a therapeutic strategy for ischemic stroke. Neurochem Int. 2017;107:23–32. doi: 10.1016/j.neuint.2016.12.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hotchkiss RS, Strasser A, McDunn JE, Swanson PE. Cell death. N Engl J Med. 2009;361:1570–1583. doi: 10.1056/NEJMra0901217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Linkermann A, Green DR. Necroptosis. N Engl J Med. 2014;370:455–465. doi: 10.1056/NEJMra1310050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wang YZ, Wang JJ, Huang Y, et al. Tissue acidosis induces neuronal necroptosis via ASIC1a channel independent of its ionic conduction. Elife. 2015;4 doi: 10.7554/eLife.05682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zille M, Karuppagounder SS, Chen Y, et al. Neuronal death after hemorrhagic stroke in vitro and in vivo shares features of ferroptosis and necroptosis. Stroke. 2017;48:1033–1043. doi: 10.1161/STROKEAHA.116.015609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Askalan R, Gabarin N, Armstrong EA, Fang Liu Y, Couchman D, Yager JY. Mechanisms of neurodegeneration after severe hypoxic-ischemic injury in the neonatal rat brain. Brain Res. 2015;1629:94–103. doi: 10.1016/j.brainres.2015.10.020. [DOI] [PubMed] [Google Scholar]
- 12.Bjurstedt H, Severin G. The prevention of decompression sickness and nitrogen narcosis by the use of hydrogen as a substitute for nitrogen, the Arne Zetterstrom method for deep-sea diving. Mil Surg. 1948;103:107–116. [PubMed] [Google Scholar]
- 13.Ohsawa I, Ishikawa M, Takahashi K, et al. Hydrogen acts as a therapeutic antioxidant by selectively reducing cytotoxic oxygen radicals. Nat Med. 2007;13:688–694. doi: 10.1038/nm1577. [DOI] [PubMed] [Google Scholar]
- 14.Peng Z, Chen W, Wang L, et al. Inhalation of hydrogen gas ameliorates glyoxylate-induced calcium oxalate deposition and renal oxidative stress in mice. Int J Clin Exp Pathol. 2015;8:2680–2689. [PMC free article] [PubMed] [Google Scholar]
- 15.Cui J, Chen X, Zhai X, et al. Inhalation of water electrolysis-derived hydrogen ameliorates cerebral ischemia-reperfusion injury in rats - A possible new hydrogen resource for clinical use. Neuroscience. 2016;335:232–241. doi: 10.1016/j.neuroscience.2016.08.021. [DOI] [PubMed] [Google Scholar]
- 16.Chen O, Cao Z, Li H, et al. High-concentration hydrogen protects mouse heart against ischemia/reperfusion injury through activation of thePI3K/Akt1 pathway. Sci Rep. 2017;7:14871. doi: 10.1038/s41598-017-14072-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Li H, Chen O, Ye Z, et al. Inhalation of high concentrations of hydrogen ameliorates liver ischemia/reperfusion injury through A2A receptor mediated PI3K-Akt pathway. Biochem Pharmacol. 2017;130:83–92. doi: 10.1016/j.bcp.2017.02.003. [DOI] [PubMed] [Google Scholar]
- 18.Huang ZX, Kang ZM, Gu GJ, et al. Therapeutic effects of hyperbaric oxygen in a rat model of endothelin-1-induced focal cerebral ischemia. Brain Res. 2007;1153:204–213. doi: 10.1016/j.brainres.2007.03.061. [DOI] [PubMed] [Google Scholar]
- 19.Swanson RA, Morton MT, Tsao-Wu G, Savalos RA, Davidson C, Sharp FR. A semiautomated method for measuring brain infarct volume. J Cereb Blood Flow Metab. 1990;10:290–293. doi: 10.1038/jcbfm.1990.47. [DOI] [PubMed] [Google Scholar]
- 20.Hu Q, Ma Q, Zhan Y, et al. Isoflurane enhanced hemorrhagic transformation by impairing antioxidant enzymes in hyperglycemic rats with middle cerebral artery occlusion. Stroke. 2011;42:1750–1756. doi: 10.1161/STROKEAHA.110.603142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Menzies SA, Hoff JT, Betz AL. Middle cerebral artery occlusion in rats: a neurological and pathological evaluation of a reproducible model. Neurosurgery. 1992;31:100. doi: 10.1227/00006123-199207000-00014. [DOI] [PubMed] [Google Scholar]
- 22.Sun L, Wang H, Wang Z, et al. Mixed lineage kinase domain-like protein mediates necrosis signaling downstream of RIP3 kinase. Cell. 2012;148:213–227. doi: 10.1016/j.cell.2011.11.031. [DOI] [PubMed] [Google Scholar]
- 23.Wang H, Sun L, Su L, et al. Mixed lineage kinase domain-like protein MLKL causes necrotic membrane disruption upon phosphorylation by RIP3. Mol Cell. 2014;54:133–146. doi: 10.1016/j.molcel.2014.03.003. [DOI] [PubMed] [Google Scholar]
- 24.Chen H, Zhang J, Hao H, et al. Hydrogen-rich water increases postharvest quality by enhancing antioxidant capacity in Hypsizygus marmoreus. AMB Express. 2017;7:221. doi: 10.1186/s13568-017-0496-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Qu Y, Shi J, Tang Y, et al. MLKL inhibition attenuates hypoxia-ischemia induced neuronal damage in developing brain. Exp Neurol. 2016;279:223–231. doi: 10.1016/j.expneurol.2016.03.011. [DOI] [PubMed] [Google Scholar]
- 26.Zhu X, Tao L, Tejima-Mandeville E, et al. Plasmalemma permeability and necrotic cell death phenotypes after intracerebral hemorrhage in mice. Stroke. 2012;43:524–531. doi: 10.1161/STROKEAHA.111.635672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Shen H, Liu C, Zhang D, et al. Role for RIP1 in mediating necroptosis in experimental intracerebral hemorrhage model both in vivo and in vitro. Cell Death Dis. 2017;8:e2641. doi: 10.1038/cddis.2017.58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wallach D, Kang TB, Dillon CP, Green DR. Programmed necrosis in inflammation: Toward identification of the effector molecules. Science. 2016;352:aaf2154. doi: 10.1126/science.aaf2154. [DOI] [PubMed] [Google Scholar]
- 29.Nagatani K, Wada K, Takeuchi S, et al. Effect of hydrogen gas on the survival rate of mice following global cerebral ischemia. Shock. 2012;37:645–652. doi: 10.1097/SHK.0b013e31824ed57c. [DOI] [PubMed] [Google Scholar]
- 30.Zhou W, Yuan J. Necroptosis in health and diseases. Semin Cell Dev Biol. 2014;35:14–23. doi: 10.1016/j.semcdb.2014.07.013. [DOI] [PubMed] [Google Scholar]
- 31.Mizumura K, Maruoka S, Gon Y, Choi AM, Hashimoto S. The role of necroptosis in pulmonary diseases. Respir Investig. 2016;54:407–412. doi: 10.1016/j.resinv.2016.03.008. [DOI] [PubMed] [Google Scholar]