

Abstract
OBJECTIVES
This study conducted in 2016 aimed to assess the prevalence and incidence of asthma and chronic obstructive pulmonary disease (COPD) in the Eastern Mediterranean Region (EMR).
MATERIAL AND METHODS
A meta-analysis to evaluate the published research relating to asthma and COPD was conducted using data from 23 EMR Office (EMRO) countries and searching using the web of science, PubMed, SciVerse Scopus, Google scholar, and MEDLINE databases. The keywords entered were all EMRO countries (Afghanistan, Bahrain, Djibouti, Egypt, Islamic republic Iran, Iraq, Jordan, Kuwait, Lebanon, Libyan Arab Jamahiriya, Morocco, Oman, Pakistan, Palestine, Qatar, Saudi Arab, Somalia, Sudan, Syrian Arab Republic, Tunisia, the United Arab Emirates, Yemen republic, and Cyprus) and asthma OR chronic obstructive pulmonary disease (COPD) OR (chronic bronchitis). Our definition of asthma and COPD was according to the World Health Organization (WHO).
RESULTS
A total of 92 published articles were identified. The pooled prevalence of asthma and COPD was 9.38 (confidence interval [CI]: 9.20–9.55) and 5.39 (CI: 5.17–5.62), respectively. There were no articles about COPD and asthma in Bahrain and Djibouti; no articles about asthma in Jordan and Libyan Arab Jamahiriya; and no articles about COPD in Afghanistan, Iraq, Oman, Palestine, Somalia, Sudan, and Yemen republic. The highest prevalence of asthma was observed in Kuwait, and the highest prevalence of COPD was observed in Pakistan.
CONCLUSION
The EMRO countries have inadequate research and data in the areas of asthma and COPD. More efforts and relevant studies must be conducted to understand the countrywide prevalence and real burden of these diseases.
Keywords: Bronchial asthma, chronic obstructive pulmonary disease, Eastern Mediterranean Region Office
INTRODUCTION
Bronchial asthma and chronic obstructive pulmonary disease (COPD) are worldwide health problems [1,2]. Asthma is a public health problem particularly among children. According to the World Health Organization (WHO) estimation, 235 million people currently have asthma, and since asthma is under-diagnosed and under-treated, the worldwide prevalence is likely to be higher. The causes of asthma are not completely delineated. A combination of genetic predisposition with environmental exposure to house dusts mites’, cockroach, carpets pollens, active and passive tobacco smoke, and air pollution may provoke the irritation of the airways. One-hundred million more people worldwide are expected to develop asthma by 2025 [3–5].
The prevalence of asthma has increased over time and an additional 4.15 million disability-adjusted life years (DALYs) are caused by asthma [6–8]. In contrast, moderate to severe COPD was observed in 65 million people in 2005. Death due to COPD occurred in more than 3 million people, and it was the cause of 5% of all global deaths. Data on COPD prevalence, morbidity, and mortality in the high-income countries are more available. The access to collect accurate epidemiologic data on asthma and COPD in the low- and middle-income countries (LMIC) is difficult and expensive. It is known that almost 90% of COPD deaths occur in the LMIC. In the high-income countries, COPD is growing because of tobacco consumption and global demographics with many more living into the COPD age range in all countries, especially LMIC. WHO estimates that 5.4 million people died due to tobacco use in 2005. By 2030, tobacco-related deaths are predicted to grow to 8.3 million per year. The risk factors of COPD burden in the low-income countries beside tobacco use include exposure to indoor air pollution, such as the use of biomass fuels for cooking and heating and poverty [9,10]. The reduction in mortality and morbidity related to asthma and COPD particularly in the LMIC is one of the goals of WHO Global Action Plan for the Prevention and Control of non-communicable diseases. Research about bronchial asthma and COPD is one of the important instruments that each country needs to provide for accurate policy and planning on non-communicable diseases. Based on the new data, it is estimated that in 2030 COPD will become the third leading cause of death [11]. Highlighting the lack of information about asthma and COPD in the Eastern Mediterranean Region Office (EMRO) and knowing about the prevalence of asthma and COPD is very important [12]. This study conducted in 2016 aimed to assess the prevalence and incidence of asthma and COPD in the EMR.
MATERIAL AND METHODS
A meta-analysis was conducted to evaluate published data related to asthma and COPD by identifying relevant papers from 23 EMRO countries. The literature search was performed using the web of science, PubMed, SciVerse, Scopus, Google scholar, and MEDLINE databases, searching for articles published in the English language for 1996–2016. Keywords entered into the above mentioned search engines were all the EMRO countries (Afghanistan, Bahrain, Djibouti, Egypt, Islamic republic Iran, Iraq, Jordan, Kuwait, Lebanon, Libyan Arab Jamahiriya, Morocco, Oman, Pakistan, Palestine, Qatar, Saudi Arab, Somalia, Sudan, Syrian Arab Republic, Tunisia, the United Arab Emirates, Yemen republic, and Cyprus) and asthma OR Chronic Obstructive Pulmonary Disease (COPD) OR (chronic bronchitis). Our definition of asthma and COPD was according to the WHO [11]. Articles were reviewed and cross-checked independently by two reviewers. Any disagreements were resolved by consensus of all reviewers. The total number of original research and review articles published from the EMRO countries about COPD and asthma was 92. The inclusion of the published articles for the study was based on the following criteria: design of the study: descriptive or cross-sectional studies; prevalence of asthma among 13–14-year-olds; and COPD among the general population. The exclusion criteria for the selection were as follows: randomized control trials and intervention studies. To evaluate the articles, the quality of the selected articles was verified using the Strobe guidelines; the articles were excluded if they were not good enough [13].
After screening the available studies and selecting studies that met the inclusion criteria, the prevalence rate of COPD or Asthma was extracted from each of them as the main outcome under study. To combine these outcomes, we first assessed the heterogeneity among the reported outcomes using the I-square index. Since this index represents a high value of heterogeneity among these countries, a random effect methodology was applied for pooling the prevalence rates. Using this approach and considering the inverse variance as the weight of each study, the pooled prevalence rate in addition to 95% confidence interval (CI) was calculated and represented using the Forest plot. The data analysis was performed using the STATA (IC 13, STATA Corp LP, TX, USA). Since the heterogeneity among the included studies was high, a considerable random effects model was used for pooling the data. This study was approved by Ethics Committee of the Shahid Behehti Medical Sciences University, Tehran, Iran.
RESULTS
The literature search covered the period of 1996–2016. There were no published documents about COPD and asthma in Bahrain and Djibouti; no published documents about asthma in Jordan and Libyan Arab Jamahiriya; and no data were available on COPD from Afghanistan, Iraq, Oman, Palestine, Somalia, Sudan, and Yemen republic (Figure 1).
Figure 1.

Summarizing the number of studies reviewed for 23 countries
Figure 1 shows a summary of the number of studies reviewed for 23 countries.
Figure 2 is a forest plot analysis, which shows the pooled prevalence of asthma in the Eastern Mediterranean countries. The prevalence of asthma in the Eastern Mediterranean countries was 9.38 (CI: 9.20–9.55) among children aged 13–14 years.
Figure 2.

Forest plot analysis of asthma in the Eastern Mediterranean countries
Figure 3 is a forest plot analysis, which shows the pooled prevalence of COPD. The prevalence of COPD was 5.39 (CI: 5.17–5.62) in the general population.
Figure 3.

Forest plot analysis of prevalence of COPD in the Eastern Mediterranean countries
Figure 4 shows the prevalence of asthma in the Eastern Mediterranean countries. The prevalence of asthma was more in Kuwait, Qatar, and Saudi Arabia than in other countries.
Figure 4.
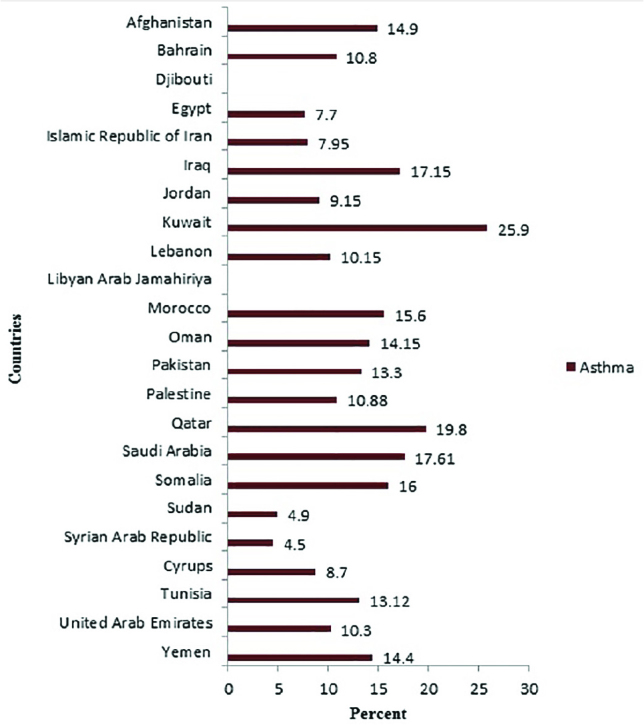
Prevalence of asthma in the Eastern Mediterranean countries
Figure 5 shows the prevalence of COPD in the Eastern Mediterranean countries. COPD was more prevalent in Pakistan, Morocco, and Lebanon than in other countries [14–27].
Figure 5.

Prevalence of COPD in the Eastern Mediterranean countries
DISCUSSION
Asthma and COPD are worldwide problems particularly in the LMIC. The prevalence of asthma and chronic respiratory diseases in the EMRO countries is rising [28]. It has been shown that the majority of problems focused on the EMRO countries due to lack of adequate document of prevalence, incidence, burden, and DALY of asthma and COPD. A study by Sweileh et al. [28] in 2014 showed that research from Arab countries was low [29].
A study on the global asthma prevalence in adults conducted by To et al. [22] in 2012 showed that the prevalence of diagnosed asthma was 4.17–4.36, clinical asthma was 4.36–4.55, and wheezing symptoms was 8.47%–8.74%. The study showed that the prevalence of asthma was 9.38 (CI: 9.20–9.55), which was higher than the global rate.
The findings showed that there were no documents about COPD and asthma in Bahrain and Djibouti. In addition, there were no data about asthma in Jordan and Libyan Arab Jamahiriya. Also, no data were available about COPD in Afghanistan, Iraq, Oman, Palestine, Somalia, Sudan, and Yemen republic. Evaluating the current available data showed that the prevalence of asthma was more in Kuwait, Qatar, and Saudi Arabia than other countries. A study by Khadadah [30] showed that the prevalence of asthma in Kuwait was 15% among adults and 18% among children (93,923 adults; 70,158 children). Lai et al. [31] showed that the prevalence of asthma was 15.5 % in Khartoum and was totally 10.8% in Sudan. Janahi et al. [17] showed that diagnosed asthma in Qatari was 19.8%. The prevalence of asthma was more than other Eastern Mediterranean countries. Sudan is a low-income country and the life expectancy among Sudanese men and women are 49.55 and 66.57 years, respectively. Asthma is more prevalent in poverty and inappropriate health condition, which could be the reason of high prevalence of asthma in Sudan and other low-income countries. Also, COPD was more prevalent in Pakistan, Morocco, and Lebanon than other Eastern Mediterranean countries. The burden of asthma could be reduced by the implementation of developed effective strategies. Most of countries in the world do not have a national asthma and COPD strategy for children and/or adults. Among the EMRO countries, only Iran, Saudi Arabia, and the United Arab Emirates have a national asthma strategy for children and adults, and only Kuwait has a national asthma strategy for children [32]. Adeloye et al. [23] in 2015 showed that the prevalence of COPD, both globally and regionally, was high and increasing. The number of studies in the EMR was low. Findings revealed that a global collaboration is needed to access the precise information to policymaking and asthma and COPD prevention programs. Our findings were in line with those of Adeloye et al. [27] and Sweileh et al. [28]. Policy makers and planners need accurate information for legislation and policy for disease prevention [33–35]. Our findings showed that the prevalence of COPD was 5.39 (CI: 5.17–5.62). Figure 4 shows weighting of COPD in WHO regions. Weighting of COPD among the EMRO countries was 4.75, and the prevalence of COPD was 13.20 (8.78–17.62) in contrast with our findings (Figure 6) [27].
Figure 6.

Overall pooled crude prevalence of COPD by WHO regions (27)
The inclusion of a descriptive and cross-sectional study into one meta-analysis may introduce heterogeneity into the results; this weakness was covered by using a random effect.
Lack of access to some of published or unpublished articles could be considered as the limitations of the study.
After the United Nation (UN) declaration for non-communicable diseases, which included chronic respiratory disease and was based on WHO prediction by 2030, COPD changed to the third leading cause of death [11]. Therefore, WHO/EMRO plans for prevention and control of non-communicable diseases, including chronic respiratory diseases. Based on the WHO data in comparison to other WHO regions, the situation of chronic respiratory diseases and COPD in the Eastern Mediterranean countries are alarming.
The findings revealed that the EMRO countries have inadequate research and data in the field of chronic respiratory diseases, including asthma and COPD. More efforts and relevant studies must be conducted to understand the countrywide prevalence and the real burden of these diseases.
Acknowledgements
The authors would like to thank Library of Shadid Beheshti University of Medical Sciences.
Footnotes
This study was presented at the 18th Annual Congress of Turkish Thoracic Society, 1–5 April 2015, Antalya, Turkey.
Ethics Committee Approval: Ethics committee approval was received for this study from the Ethics Committee of Shadid Behehti Medical Sciences University.
Informed Consent: N/A.
Peer-review: Externally peer-reviewed.
Author Contributions: Design - M.M., E.A.; Supervision - M.M., F.Z.; Resource - R.P.; Materials - R.P.; Data Collection and/or Processing - M.M., E.A., F.Z., R.P.; Analysis and/or Interpretation - M.M., E.A., F.Z.; Literature Search - E.A., R.P.; Writing - M.M., E.A., F.Z., R.P.; Critical Reviews - M.M., E.A., F.Z.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES
- 1.Wu W, Kaminski N. Chronic lung diseases. Wiley Interdiscip Rev Syst Biol Med. 2009;1:298–308. doi: 10.1002/wsbm.23. https://doi.org/10.1002/wsbm.23 [DOI] [PubMed] [Google Scholar]
- 2.Halbert R, Natoli JL, Gano A, Badamgarav E, Buist AS, Mannino DM. Global burden of COPD: systematic review and meta-analysis. Eur Respir J. 2006;28:523–32. doi: 10.1183/09031936.06.00124605. https://doi.org/10.1183/09031936.06.00124605 [DOI] [PubMed] [Google Scholar]
- 3.Behera D, Sehgal IS. Bronchial asthma-Issues for the developing world. Indian J Med Res. 2015;141:380–2. doi: 10.4103/0971-5916.159237. https://doi.org/10.4103/0971-5916.159237 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Peters SP, Ferguson G, Deniz Y, Reisner C. Uncontrolled asthma: a review of the prevalence, disease burden and options for treatment. Respir Med. 2006;100:1139–51. doi: 10.1016/j.rmed.2006.03.031. https://doi.org/10.1016/j.rmed.2006.03.031 [DOI] [PubMed] [Google Scholar]
- 5.Saeedfar K, Behmanesh M, Mortaz E, Masjedi MR. The Expression of STAT3 and STAT5A Genes in Severe Refractory Asthma. Tanaffos. 2017;16:1–8. [PMC free article] [PubMed] [Google Scholar]
- 6.Aggarwal A, Chaudhry K, Chhabra SK, et al. Prevalence and risk factors for bronchial asthma in Indian adults: a multicentre study. Indian J Chest Dis Allied Sci. 2006;48:13–22. [PubMed] [Google Scholar]
- 7.Agarwal R, Denning DW, Chakrabarti A. Estimation of the burden of chronic and allergic pulmonary aspergillosis in India. PLoS One. 2014;9:e114745. doi: 10.1371/journal.pone.0114745. https://doi.org/10.1371/journal.pone.0114745 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Reddel HK, Hurd SS, FitzGerald JM. World Asthma Day. GINA 2014: a global asthma strategy for a global problem. Int J Tuberc Lung Dis. 2014;18:505–6. doi: 10.5588/ijtld.14.0246. https://doi.org/10.5588/ijtld.14.0246 [DOI] [PubMed] [Google Scholar]
- 9.Bousquet J, Mantzouranis E, Cruz AA, et al. Uniform definition of asthma severity, control, and exacerbations: document presented for the World Health Organization Consultation on Severe Asthma. J Allergy Clin Immunol. 2010;126:926–38. doi: 10.1016/j.jaci.2010.07.019. https://doi.org/10.1016/j.jaci.2010.07.019 [DOI] [PubMed] [Google Scholar]
- 10.Hooper R, Burney P, Vollmer WM, et al. Risk factors for COPD spirometrically defined from the lower limit of normal in the BOLD project. Eur Respir J. 2012;39:1343–53. doi: 10.1183/09031936.00002711. https://doi.org/10.1183/09031936.00002711 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.COPD predicted to be third leading cause of death in 2030. World Health Stat. 2008. Available from: http://www.who.int/respiratory/copd/World_Health_Statistics_2008/en/
- 12.Pauwels RA, Rabe KF. Burden and clinical features of chronic obstructive pulmonary disease (COPD) The Lancet. 2004;364:613–20. doi: 10.1016/S0140-6736(04)16855-4. https://doi.org/10.1016/S0140-6736(04)16855-4 [DOI] [PubMed] [Google Scholar]
- 13.Von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology [STROBE] statement: guidelines for reporting observational studies. Gac Sanit. 2008;22:144–50. doi: 10.1157/13119325. https://doi.org/10.1157/13119325 [DOI] [PubMed] [Google Scholar]
- 14.Boutayeb A, Boutayeb S, Boutayeb W. Multi-morbidity of non communicable diseases and equity in WHO Eastern Mediterranean countries. Int J Equity Health. 2013;12:60. doi: 10.1186/1475-9276-12-60. https://doi.org/10.1186/1475-9276-12-60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sharifi H, Masjedi MR, Emami H, et al. Interim report from burden of obstructive lung disease (BOLD Study) in Tehran: prevalence and risk factors of chronic obstructive pulmonary disease. Tanaffos. 2014;13:6–13. [PMC free article] [PubMed] [Google Scholar]
- 16.Sharifi H, Masjedi MR, Emami H, et al. Burden of obstructive lung disease study in Tehran: Prevalence and risk factors of chronic obstructive pulmonary disease. Lung India. 2015;32:572–7. doi: 10.4103/0970-2113.168129. https://doi.org/10.4103/0970-2113.168129 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Janahi IA, Bener A, Bush A. Prevalence of asthma among Qatari schoolchildren: international study of asthma and allergies in childhood, Qatar. Pediatr Pulmonol. 2006;41:80–6. doi: 10.1002/ppul.20331. https://doi.org/10.1002/ppul.20331 [DOI] [PubMed] [Google Scholar]
- 18.Khafaji HA, Sulaiman K, Singh R, et al. Chronic obstructive airway disease among patients hospitalized with acute heart failure; clinical characteristics, precipitating factors, management and outcome: Observational report from the Middle East. Acute Card Care. 2015;17:55–66. doi: 10.1080/17482941.2016.1203438. https://doi.org/10.1080/17482941.2016.1203438 [DOI] [PubMed] [Google Scholar]
- 19.Daldoul H, Denguezli M, Jithoo A, et al. Prevalence of COPD and tobacco smoking in Tunisia-Results from the BOLD Study. Int J Environ Res Public Health. 2013;10:7257–71. doi: 10.3390/ijerph10127257. https://doi.org/10.3390/ijerph10127257 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Bahaj S, Moharem A, Kaid A. Prevalence of Asthma and Allergic Diseases among High School Students in Urban and Rural Communities, Yemen. The Egyptian Journal of Medical Microbiology. 2012;38:1–5. https://doi.org/10.12816/0004904. [Google Scholar]
- 21.Khelafi R, Aissanou A, Tarsift S, et al. Epidemiology of chronic obstructive pulmonary disease in Algiers. Rev Mal Respir. 2011;28:32–40. doi: 10.1016/j.rmr.2010.06.026. https://doi.org/10.1016/j.rmr.2010.06.026 [DOI] [PubMed] [Google Scholar]
- 22.To T, Stanojevic S, Moores G, et al. Global asthma prevalence in adults: findings from the cross-sectional world health survey. BMC Public Health. 2012;12:204. doi: 10.1186/1471-2458-12-204. https://doi.org/10.1186/1471-2458-12-204 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Adeloye D, Chan KY, Rudan I, Campbell H. An estimate of asthma prevalence in Africa: a systematic analysis. Croat Med J. 2013;54:519–31. doi: 10.3325/cmj.2013.54.519. https://doi.org/10.3325/cmj.2013.54.519 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Zachariades AG, Zachariadou T, Adamide T, et al. Prevalence of chronic obstructive pulmonary disease in Cyprus: a population-based study. COPD. 2012;9:259–67. doi: 10.3109/15412555.2011.650242. https://doi.org/10.3109/15412555.2011.650242 [DOI] [PubMed] [Google Scholar]
- 25.Lamnisos D, Moustaki M, Kolokotroni O, et al. Prevalence of asthma and allergies in children from the Greek-Cypriot and Turkish-Cypriot communities in Cyprus: a bi-communal cross-sectional study. BMC Public Health. 2013;13:585. doi: 10.1186/1471-2458-13-585. https://doi.org/10.1186/1471-2458-13-585 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Dalkan C, Galip N, Tekguc H, et al. High prevalence of allergy in North Cypriot children. Paediatr Int Child Health. 2014;34:37–42. doi: 10.1179/2046905513Y.0000000074. https://doi.org/10.1179/2046905513Y.0000000074 [DOI] [PubMed] [Google Scholar]
- 27.Adeloye D, Chua S, Lee C, et al. Global and regional estimates of COPD prevalence: Systematic review and meta-analysis. J Glob Health. 2015;5:020415. doi: 10.7189/jogh.05-020415. https://doi.org/10.7189/jogh.05.020415 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sweileh WM, Al-Jabi SW, Zyoud SH, et al. Bronchial asthma and chronic obstructive pulmonary disease: research activity in Arab countries. Multidiscip Respir Med. 2014;9:38. doi: 10.1186/2049-6958-9-38. https://doi.org/10.1186/2049-6958-9-38 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Selroos O, Kupczyk M, Kuna P, et al. National and regional asthma programmes in Europe. Eur Respir Rev. 2015;24:474–83. doi: 10.1183/16000617.00008114. https://doi.org/10.1183/16000617.00008114 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Khadadah M. The cost of asthma in Kuwait. Med Prin Pract. 2013;22:87–91. doi: 10.1159/000341154. https://doi.org/10.1159/000341154 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lai C, Beasley R, Crane J, et al. Global variation in the prevalence and severity of asthma symptoms: phase three of the International Study of Asthma and Allergies in Childhood (ISAAC) Thorax. 2009;64:476–83. doi: 10.1136/thx.2008.106609. https://doi.org/10.1136/thx.2008.106609 [DOI] [PubMed] [Google Scholar]
- 32.Al Ghobain M. The prevalence of chronic obstructive pulmonary disease in Saudi Arabia: Where do we stand? Ann Thorac Med. 2011;6:185–6. doi: 10.4103/1817-1737.84770. https://doi.org/10.4103/1817-1737.84770 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Tejano R. Re: prevalence of chronic obstructive pulmonary disease among smokers attending primary health-care clinics in Saudi Arabia. Ann Saudi Med. 2011;31:432–6. doi: 10.4103/0256-4947.77485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.El Hasnaoui A, Rashid N, Lahlou A, et al. Chronic obstructive pulmonary disease in the adult population within the Middle East and North Africa region: rationale and design of the BREATHE study. Respir Med. 2012;106:3–15. doi: 10.1016/S0954-6111(12)70010-0. https://doi.org/10.1016/S0954-6111(12)70010-0 [DOI] [PubMed] [Google Scholar]
- 35.Tageldin MA, Nafti S, Khan JA, et al. Distribution of COPD-related symptoms in the Middle East and North Africa: results of the BREATHE study. Respir Med. 2012;106:25–32. doi: 10.1016/S0954-6111(12)70012-4. https://doi.org/10.1016/S0954-6111(12)70012-4 [DOI] [PubMed] [Google Scholar]