

Abstract
Background:
Global photographs (GPs) have been widely used to grade the severity in female pattern hair loss (FPHL). However, existing classifications for FPHL are not useful in the evaluation of early FPHL. Although there are some variations in early FPHL, even to a mild degree, all types of early FPHL are included in just one category. Therefore, the authors have devised a grading system for early FPHL with five levels focusing on the changes revealed by the surface reflected light of flash generated on GPs.
Aims:
This study aims to examine the possibility of evaluating the treatment course of early FPHL using the grading system based on changes in hair surface reflection patterns.
Subjects and Methods:
Retrospective chart review of 114 early FPHL patients was performed. GPs of these patients were classified into five grades. Photographs of the lowest and the highest grades of each patient were selected and paired. First, the relevance between the value of FPHL-severity index (FPHL-SI) and grades of all the selected photos was analyzed. Next three volunteers graded the paired photographs and chose the milder degree, and then, the concordance rate among author's and volunteers' evaluations were analyzed.
Results:
The value of FPHL-SI and incidence rate of hair diameter diversity tended to rise along with increasing of GP grade. Concordance rate of grading among author and more than two volunteers was 57%. The concordance rate of course evaluation between author and two volunteers was 97%.
Conclusion:
The new classification can finely classify the grade of early FPHL and can be used for treatment course evaluation.
Key words: Female pattern hair loss, global photograph, surface reflection light
INTRODUCTION
For patients with female pattern hair loss (FPHL) and global photographs (GPs) are probably the single most important and reliable means of evaluation.[1] Although there are some variations in the manifestations of early FPHL, all types of early FPHL are included as just one category in existing classifications because of difficulty to objectively evaluate various patterns in early FPHL.[2,3,4,5,6,7]
Therefore, the authors have developed a grading system for early FPHL with five levels focusing on the changes revealed by the surface reflected flashlight of GPs [Figure 1] and examined whether treatment courses can be assessed using it.
Figure 1.
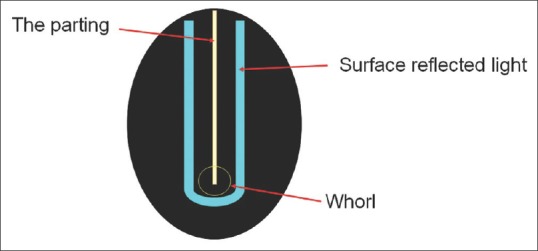
Surface reflected light. Surface reflected light is light which hits the hair and reflects on the surface of the cuticle and appears as shining white. It runs parallel keeping a constant distance from the parting and becomes U shape at the whorl
SUBJECTS AND METHODS
Authors conducted a retrospective chart review of women who first visited the author's clinic from July 2012 to November 2016 and were diagnosed as having early FPHL. The diagnosis of early FPHL was determined by history, physical examination findings, blood test findings, scope images, and GPs. Regarding GPs, we took photographs using the same procedure every time. Patients were instructed not to apply any styling agent before attending the clinic. They were asked to sit with their face up so that their parietal region and whorl were in the front and center of the photograph [Figure 2]. The whole head was photographed by a digital camera (Finepix F30®) with built-in flash.
Figure 2.

Shooting method. Patients sat with their face up so that their parietal region and whorl are in center of the photograph
Inclusion of early FPHL patients in this study was dependent on fulfilling all of the following criteria; more than 6 months follow-up period, access to all the data necessary for this study, and GPs with almost the same background brightness. A total of 114 early FPHL women were included in this study.
All GPs taken during the treatment course were sorted into five grades based on the shape of the surface reflected light [Figure 3]. We obtained a permission of usage of data including photograph from each patient whose data was used in this study.
Figure 3.
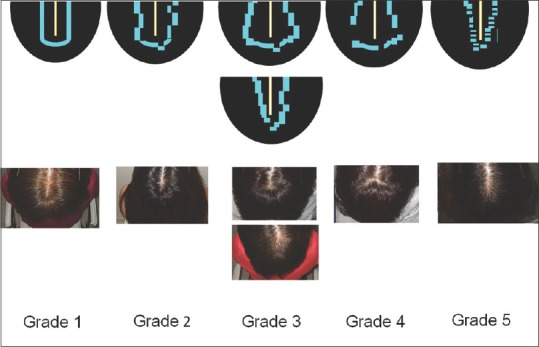
Grading system of early female pattern hair loss using global photographs. The patterns of the surface reflected light band differ from each other. Grade 1 is the ideal condition and grade 5 is the condition which is close to obvious hair loss
Grade 1
From the parietal/midscalp region to the whorl, the surface reflected light band is clearly present and runs parallel with the parting and curves in a U shape without deviation or has a deviation within one width of the surface reflected light band (regarded as almost normal).
Grade 2
From the parietal/midscalp region to the whorl, the surface reflected light band is clearly present and runs in parallel with the parting and curves in a U shape; however, it has a deviation of one or more but <2 widths of the surface reflected light band.
Grade 3
From the parietal/midscalp region to the whorl, the surface reflected light band is clear; however, it shifted sideways or to the center with a deviation of two or more widths of the surface reflected light band.
Grade 4
From the parietal/midscalp region to the whorl, the surface reflected light band attenuates and breaks for more than one width of light.
Grade 5
From the parietal/midscalp region to the whorl, the surface reflected light band is ambiguous all around. The light is no more band like and becomes column of strip-like.
Next, authors selected the GP with the highest grade (severe) and the GP with the lowest grade (mild) for each patient (n = 228). These photos were also evaluated with existing classifications. Moreover, dermoscopy findings of each grade were analyzed.
Then, authors rated the FPHL severity index (FPHL-SI) using data of the closest date to the photographs.
FPHL-SI includes four evaluation items that include the amount of hair shedding, midline hair density, hair diameter variation, and difference in the proportion of single hairs per hair follicle unit between the frontal and occipital scalp.[7] Less than 200 hairs she d per day, or negative in pull test at 0 point, and positive in pull test at 2 points.[7]
Midline hair density was assessed according to Sinclair's midline hair density scale Grade 1 where a patient complains of excessive hair shedding and loss of hair volume but has no clinically obvious reduction in hair density to 0 point, and Grade 2 which is mild but clinically apparent hair loss to point 4.[7] In the trichoscopy, image a hair diameter variation of <20% is considered point 0, and that of 20% or more is considered 5 points.[7] In addition, if there is no difference in the amount of hair included in the follicular unit between the forehead and in the occipital area, this is evaluated as point 0, if there is difference of more than 25% between them, this is assessed as point 1, and if there is difference of more than 50% then the score goes to 2 points.[7]
After rating FPHL-SI of each GP photo, we divided them into five groups by GP grades, and the average value of FPHL-SI of each group was calculated. Moreover, the relevance to GP grades and FPHL-SI value was examined statistically.
Two photos selected from each patient as described above were randomly allocated to either side of one slide. After being instructed how to grade the photographs, three volunteers (1 male, 2 females) graded the photographs of 114 cases (228 photos) and judged which photo seemed to be in milder degree in each slide. Then, the concordance rate among the author's and volunteers' evaluations was analyzed by grade evaluation and comparison of photos.
RESULTS
The mean age was 39.1 years (range, 20–55 years), and the mean age of onset was 36.0 years old (15–53 years). In 228 photos, 30 photos were graded in Grade 1, 64 photos in Grade 2, 61 photos in Grade 3, 50 photos in Grade 4, and 23 photos in Grade 5.
According to existing classifications, photos of Grade 1 were included in normal, those of Grade 2–4 were mainly included in Sinclair 1, and those of Grade 5 were mainly included in Sinclair 1 or 2 [Table 1].
Table 1.
Characteristics of each group in this classification

As for dermoscopy findings, the higher GP grade group tended to have a higher hair diameter diversity rate [Table 1]. Perifollicular pigmentation was hardly seen in Grade 1, 2, and 3 and was seen 10% in grade 4 and 5 [Table 1].
As for FPHL-SI value, the higher GP grade group tended to have a higher FPHL-SI value [Figure 4]. However, the correlation could not be statistically evaluated using the correlation coefficient because the FPHL-SI value was not normal distributed. The concordance rate for GP evaluation among two or more volunteers and author was 57%, and that between one volunteer and author was 41% [Table 2]. As for the concordance rate for photo comparisons, 97% (111/114 cases) of decisions accorded among two or more volunteers and the author, 2% (3/114 cases) of decisions accorded between one volunteer and the author, 1% of decisions (1/114 cases) did not accord [Table 2]. Representative cases are shown in Figures 5 and 6. Changes in grades along with treatment course are seen in each case.
Figure 4.
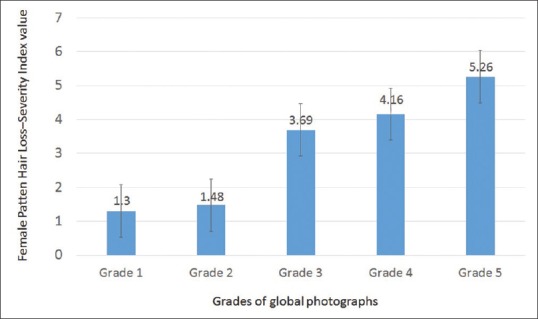
Female pattern hair loss-severity index value in each global photograph's group. The mean value and standard error of female pattern hair loss-severity index of each group are shown. The mean value of female pattern hair loss-severity index of each group increased as the global photograph grade increased
Table 2.
Concordance rate of evaluation among author and 3 volunteers
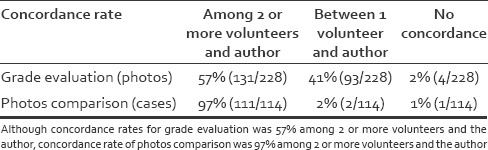
Figure 5.

Case 1: A 32-year-old woman – the surface reflected light was almost U-shaped with irregularity, so the condition was evaluated as grade 2 (a). After starting treatment, the degree of irregularity shrank (b), and the light reached parallel which means Grade 1 (c)
Figure 6.

Case 2: A 44-year-old woman – The surface reflected light was getting narrower toward the whorl which means Grade 3 (a). It began to round (b and c), and 1 year and 7 months after treatment, the condition reached Grade 1 (d)
Case 1
A 32-year-old woman – at the initial visit, the surface reflected light band was almost U-shaped but included irregularity. Hence, it was judged as grade 2 [Figure 5a]. After starting treatment, the degree of irregularity shrank [Figure 5b], and after 2.5 months, the surface reflected light reached parallel, reaching grade 1 within the normal range [Figure 5c]. Compared with the initial examination, the exposed middle scalp was narrowing at 2.5 months [Figures 5a and c].
Case 2
A 44-year-old woman – since the surface reflected light was getting narrower toward the whorl at the first visit, it was judged as grade 3 [Figure 6a]. Six months after treatment, the surface reflected light around the whorl began to round [Figure 6b]. One year after treatment, the reflected light was more clear and bright, reaching grade 2 [Figure 6c].
Further treatment was continued to achieve surface reflected light parallel at the front part. One year and 7 months after treatment, the surface reflected light around the whorl was a good U shape, and the front light became parallel to the rest. Eventually, she reached grade 1 within the normal range [Figure 6d].
DISCUSSION
Early FPHL is mild condition among all FPHL, and Olsen mentioned its feature as a slightly widened parting.[4] On the other hand, Messenger and Sinclair classifies early FPHL, which is the mildest condition, as “no clinically obvious reduction in hair density.”[5,6,7]
Because early FPHL includes various patterns even to a mild degree, the positioning of “early” in FPHL is somewhat different among experts as well.
Until now, there has not been any classifications that can accurately grade early FPHL. Because existing grading systems are based on the degree of scalp that has been exposed, this can only detect more advanced stages of FPHL. However, the authors consider that there should be an objective index of early FPHL too since women requesting early treatment against FPHL is increasing.
GPs have been used for evaluation and recording of appearance in FPHL. Olsen described, “GPs are probably the single most important and reliable end-point to use in clinical trials of women with FPHL.”[1] The therapeutic effect was assessed by appearance using the GPs, 7-point evaluation which numerically evaluates the degree of change from baseline photo (−3 = greatly decreased, −2 = moderately decreased, −1 = slightly decreased, 0 = no change, +1 = slightly increased, +2 = moderately increased, +3 = greatly increased).[8] However, the evaluation of doctors and patients does not necessarily agree.
Starting treatment at the early FPHL stage would be helpful from the viewpoint of increasing the probability of effectiveness[7] and reducing the mental and economic burden of the patient. For that purpose, there should be an objective evaluation system of early FPHL which enable not only the classification of early FPHL but also determines the effect of treatment.
Since existing FPHL classifications depend on the size of exposed scalp, GP can evaluate two-dimensionally.[2,3,5,6] On the other hand, since early FPHL includes only hair volume reduction without enlargement of exposed scalp, early FPHL requires a new index other than area of exposed scalp. Harries et al. expressed the status of early FPHL as “very individual,”[7] and the authors thought that various patterns may be caused by the three dimensional element formed by hair diameter, density of hair, and elasticity of hair that is to say thickness change.
Surface reflected light is light which hits the hair and reflects on the surface of the cuticle and appears as shining white [Figure 1].[9] The quality of the light band depends on the hair color[10] and inhomogeneity of the hair microstructure,[11] but it also depends on the volume of hair.
Therefore, the authors consider that the three-dimensional change can be capture into two dimensions by using surface reflected light as an index, the authors have devised a classification for early FPHL with five levels focusing on the changes revealed by the surface reflected light of flash generated on GPs [Figure 3].
In photographs presented in the past literature, differences in the pattern of surface reflected light were seen. For example, in the normal condition, photograph indicated by Olsen, the surface reflected light runs parallel with the parting and curves in a U shape.[3] On the other hand, in the early FPHL stage photograph of Sinclair 1, the surface reflected light is not parallel with the parting although there is no enlargement of the middle part.[5,6,7] In addition, in Sinclair's photographs of grade 2 or more, in Ludwig's classification and in Olsen's Christmas tree pattern, no clear surface reflected light can be seen.[2,3,5,6,7]
We classified the change of hair volume from normal to FPHL based on the characteristics of surface reflected light in GPs [Figures 3 and 7]. Sinclair's Grades 2–5 and Ludwig Grades I–III mainly represent obvious hair loss.[5] The grading system in this study subdivides mainly early FPHL. If the hair volume is sufficient, the surface reflected light runs parallel keeping a constant distance from the parting and becomes U shape at the whorl. This state was set as Grade 1 which is also included as the normal state [Figure 3].
Figure 7.
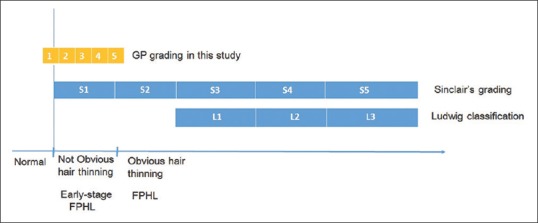
Role of the global photograph grading system. The global photograph grading system in this study subdivides mainly early female pattern hair loss
When the hair volume of a certain part decreases due to a decrease of hair diameter or density, the ridge line of the hair is deviated from the U shape, and the surface reflected light will emerge irregularly along with the deviation. The U-shaped reflected light band with irregularity was set as Grade 2 [Figure 3].
Further decrease in hair volume of a certain part, the hair ridgeline also deviates greatly from the U shape, and the surface reflected light also deviates largely out of parallel along with it. This condition was set to Grade 3 [Figure 3].
When the hair volume decreases much further, the surface reflected light becomes unclear at the part where the hair decreases, and the surface reflected light disappears. The state where the band of the surface reflected light attenuates and loses continuity was set as Grade 4 [Figure 3]. When enlargement of the parting begins to be recognized, the surface reflected light becomes difficult to be recognized. Thus, a state in which the surface reflected light band is ambiguous and difficult to trace was set to Grade 5 [Figure 3].
Apart from these grades, blurred and parallel surface reflected light band occurs, especially in aged women, because surface reflection light of each hair is found at various parts of the hair bundle in the undulating hair with aging.[12] However, since this kind of surface reflected light can be recognized, it does not affect the evaluation.
Tajima et al. reported that FPHL is likely to have a higher reduction in hair density due to an increase of telogen hair compared to androgenetic alopecia.[13] Since the hair flows in all directions at the whorl, the reduced volume of hair is easily recognized when the hair density begins to decrease.
Therefore, we took photographs of patients with upward posture due to ensure their whorl was in the center of the photograph [Figure 2].
”FPHL-SI” was proposed by Harries et al. in 2016 as a new evaluation method of FPHL severity including early FPHL.[7] This severity assessment method covers the signs of FPHL by scoring and ensures physicians objectively evaluate the patient's condition. In this study, the FPHL-SI value tended to increase as the GP grade increased, but this was not statistically significant [Figure 4]. Because the FPHL-SI value of the subjects in this study was between 0 and 11, with mostly 0 and 5, data were not normally distributed. This may have occurred because FPHL-SI was created to evaluate all grades of FPHL as numerical values and not focused on early FPHL evaluation.
Regarding dermoscopy findings, hair diameter diversity, and perifollicular pigmentation are known to be seen in patients with androgenetic alopecia.[14]
In this study, the incidence rate of hair diameter diversity was well correlated with grades rather than perifollicular pigmentation.
The greatest value of our classification is that it is easy for patients to understand the gradual changes at early FPHL stage. In the treatment of FPHL, GPs have mainly been used for recording patient's condition. However, the role of GPs in this study is a diagnostic tool, a novel application of GPs. FPHL treatment is considered as a cosmetic treatment in most countries, and it is important that patient consent is obtained for treatment course and treatment policy. If patients share recognition with doctors about the treatment course, patients, and doctors can discuss therapeutic policy constructively.
Our classification is easy to capture any sign of hair change before obvious change occurs. In FPHL, factors influencing the change in the hair cycle, which is the disease mechanism of FPHL, are complex, so the course is not uniform, and remission and worsening may occur during course. Detecting signs of change at an early stage using this classification will make it easier to decide on the best treatment strategy and will be helpful to advance early FPHL treatment.
In conclusion, we showed the possibility of evaluating the condition and treatment course of early FPHL by a newly devised classification based on hair surface reflected light pattern of GPs in this study. The classification is understandable for patients and useful in daily clinical practice.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Olsen EA. Current and novel methods for assessing efficacy of hair growth promoters in pattern hair loss. J Am Acad Dermatol. 2003;48:253–62. doi: 10.1067/mjd.2003.81. [DOI] [PubMed] [Google Scholar]
- 2.Ludwig E. Classification of the types of androgenetic alopecia (common baldness) occurring in the female sex. Br J Dermatol. 1977;97:247–54. doi: 10.1111/j.1365-2133.1977.tb15179.x. [DOI] [PubMed] [Google Scholar]
- 3.Olsen EA. The midline part: An important physical clue to the clinical diagnosis of androgenetic alopecia in women. J Am Acad Dermatol. 1999;40:106–9. doi: 10.1016/s0190-9622(99)70539-6. [DOI] [PubMed] [Google Scholar]
- 4.Olsen EA. Female pattern hair loss. J Am Acad Dermatol. 2001;45:S70–80. doi: 10.1067/mjd.2001.117426. [DOI] [PubMed] [Google Scholar]
- 5.Biondo S, Goble D, Sinclair R. Women who present with female pattern hair loss tend to underestimate the severity of their hair loss. Br J Dermatol. 2004;150:750–2. doi: 10.1046/j.0007-0963.2003.05809.x. [DOI] [PubMed] [Google Scholar]
- 6.Messenger AG, Sinclair R. Follicular miniaturization in female pattern hair loss: Clinicopathological correlations. Br J Dermatol. 2006;155:926–30. doi: 10.1111/j.1365-2133.2006.07409.x. [DOI] [PubMed] [Google Scholar]
- 7.Harries M, Tosti A, Bergfeld W, Blume-Peytavi U, Shapiro J, Lutz G, et al. Towards a consensus on how to diagnose and quantify female pattern hair loss – The 'female pattern hair loss severity index (FPHL-SI)'. J Eur Acad Dermatol Venereol. 2016;30:667–76. doi: 10.1111/jdv.13455. [DOI] [PubMed] [Google Scholar]
- 8.Blume-Peytavi U, Hillmann K, Dietz E, Canfield D, Garcia Bartels N. A randomized, single-blind trial of 5% minoxidil foam once daily versus 2% minoxidil solution twice daily in the treatment of androgenetic alopecia in women. J Am Acad Dermatol. 2011;65:1126–3400. doi: 10.1016/j.jaad.2010.09.724. [DOI] [PubMed] [Google Scholar]
- 9.Keis K, Ramaprasad KR, Kamath YK. Studies of light scattering from ethnic hair fibers. J Cosmet Sci. 2004;55:49–63. [PubMed] [Google Scholar]
- 10.Wortmann FJ, Schulze zur Wiesche E, Bourceau B. Analyzing the laser-light reflection from human hair fibers. II. Deriving a measure of hair luster. J Cosmet Sci. 2004;55:81–93. [PubMed] [Google Scholar]
- 11.Okamoto M, Yakawa R, Mamada A, Inoue S, Nagase S, Shibuichi S, et al. Influence of internal structures of hair fiber on hair appearance. III. Generation of light-scattering factors in hair cuticles and the influence on hair shine. J Cosmet Sci. 2003;54:353–66. [PubMed] [Google Scholar]
- 12.Nagase S, Kajiura Y, Mamada A, Abe H, Shibuichi S, Satoh N, et al. Changes in structure and geometric properties of human hair by aging. J Cosmet Sci. 2009;60:637–48. [PubMed] [Google Scholar]
- 13.Tajima M, Hamada C, Arai T, Miyazawa M, Shibata R, Ishino A, et al. Characteristic features of Japanese women's hair with aging and with progressing hair loss. J Dermatol Sci. 2007;45:93–103. doi: 10.1016/j.jdermsci.2006.10.011. [DOI] [PubMed] [Google Scholar]
- 14.Deloche C, de Lacharrière O, Misciali C, Piraccini BM, Vincenzi C, Bastien P, et al. Histological features of peripilar signs associated with androgenetic alopecia. Arch Dermatol Res. 2004;295:422–8. doi: 10.1007/s00403-003-0447-y. [DOI] [PubMed] [Google Scholar]