

Abstract
Objectives
The objective of this study was to determine which patient traits, behaviors, external tooth and/or crack characteristics correlate with the types of symptoms that teeth with visible cracks exhibit, namely pain on biting, pain due to cold stimuli, or spontaneous pain.
Methods
Dentists in the National Dental Practice-Based Research Network enrolled a convenience sample of subjects each of whom had a single, vital posterior tooth with at least one observable external crack (cracked teeth); 2,858 cracked teeth from 209 practitioners were enrolled. Data were collected at the patient-, tooth-, and crack-level. Generalized estimating equations were used to obtain significant (p<0.05) independent odds ratios (OR) associated with teeth that were painful for 10 outcomes based on types of pain and combinations thereof.
Results
Overall, 45% of cracked teeth had one or more symptoms. Pain to cold was the most common symptom, which occurred in 37% of cracked teeth. Pain on biting (16%) and spontaneous pain (11%) were less common. Sixty-five percent of symptomatic cracked teeth had only one type of symptom, of these 78% were painful only to cold. No patient-, tooth- or crack-level characteristic was significantly associated with pain to cold alone. Positive associations for various combinations of pain symptoms were present with cracks that: (1) were on molars; (2) were in occlusion; (3) had a wear facet through enamel; (4) had caries; (5) were evident on a radiograph; (6) ran in more than one direction; (7) blocked transilluminated light; (8) connected with another crack; (9) extended onto the root; (10) extended in more than one direction; or (11) were on the distal surface. Persons who were < 65 yo or who clench, grind, or press their teeth together also were more likely to have pain symptoms. Pain was less likely in teeth with stained cracks or exposed roots, or in non-Hispanic whites.
Conclusions
Although pain to cold was the most commonly noted pain associated with symptomatic cracked teeth, no patient-, tooth- or crack-level characteristic was significantly associated with pain to cold alone. Characteristics were only associated with pain on biting and/or spontaneous pain with or without pain to cold.
Clinical significance
Although often considered the most reliable diagnosis for a cracked tooth, pain on biting is not the most common symptom of a tooth with a visible crack, but rather pain to cold.
Keywords: Cracked teeth, Cracked tooth, Practice-based research, Symptoms
Introduction
Cracks in teeth, particularly posterior teeth, are a common finding. A comprehensive review on cracked teeth reported incidence rates varying between 0% - 70%, depending on the tooth type and location [1]. A recent practice-based study found that 70% of patients had at least one posterior tooth with visible fracture lines, 21% of which were symptomatic. [2]. A variety of symptoms have been attributed to cracked teeth, some of which are quite rare, such as trigeminal autonomic cephalalgia [3,4], The most commonly reported symptoms of cracked teeth are pain to cold and pain on biting [5,6,7,8]. A study of 154 symptomatic cracked teeth reported that 96% were painful on biting and 45% were sensitive to cold [9]. No clinical study to date has reported on commonalities of various factors to symptomology. Therefore, the purpose of this observational practice-based study was to correlate various patient-, tooth- and crack-level characteristics with the type of symptoms (spontaneous pain, pain on biting, pain to cold) exhibited by symptomatic cracked teeth in patients from selected practices participating in the National Dental Practice-based Research Network (National Dental Network).
Methods
A detailed description of the enrollment and data collection processes is provided in a previous publication [10]. Briefly, a convenience sample of subjects between 19 and 85 years old having a single, vital posterior tooth with at least one observable external crack (referred to in this paper as cracked teeth) was enrolled by dentists in the National Dental Practice-based Research Network [11]. Dentists were asked to enroll 20 eligible subjects, or as many as they could in eight weeks, whichever came first. The Institutional Review Board (IRB) of the lead investigators (TH & JF) reviewed and approved the study, as did the IRBs for the network’s six regions. All subjects were consented for entrance into the study.
Dentist and practice personnel were trained in data collection; data were collected at the patient-, tooth-, and crack level. Data forms are publicly available at [http://nationaldentalpbrn.org/study-results/cracked-tooth-registry.php]. Tooth vitality was confirmed, preferably with cold [12] (e.g., refrigerant, ice) although some dentists used other methods such as air, air/water spray, or electric pulp testing. Spontaneous pain information was obtained via patient report, with pain to cold determined using the aforementioned refrigerant, ice, or air/water spray, and pain on biting confirmed by having the patient occlude on a device or instrument placed on the occlusal surface of the cracked tooth. To help patients distinguish pain, i.e., a heightened response to the cold or bite assessment, from an ordinary response, dentists were asked to also perform these tests on a “normal” (e.g., contralateral) tooth. Enrollment proceeded in two phases: a pilot phase from April-July 2014, in which 183 patients were enrolled by 12 practices, and a main launch phase that occurred from October 2014-April 2015. In a previous report [10] we described 2,975 patients/cracked teeth enrolled by 209 practitioners. This current report excludes 96 cracked teeth that were partially or completely fractured (violation of eligibility criteria), and 21 patients we identified as duplicates, leaving 2,858 patients/cracks.
Symptomatic classification
Teeth were classified as symptomatic if they were sensitive to cold or had pain on biting or were spontaneously painful. Types of symptoms could be “present”, i.e., present alone or in any combination of two or three symptoms; “sole”, i.e., one symptom alone; or in “combination”, i.e., any two or three symptoms occurring together.
Analysis
Overall frequencies were obtained among asymptomatic cracked teeth (no pain to cold, pain on biting, or spontaneous pain), and symptomatic cracked teeth, separately by type of symptom (pain to cold, pain on biting or spontaneous pain), and by patient-, tooth- and crack-level characteristics. Initial analyses with patient demographics and behaviors were used to inform categorization for the regression model. Associations between characteristics present in less than one percent of the patient population and type of symptoms were not examined because of difficulty modeling and imprecise estimates. In a univariable fashion, each patient-, tooth-, and crack-level characteristic was entered into a logistic regression model that used generalized estimating equations (GEE) method that adjusted for clustering of patients within the practice, implemented using PROC GENMOD in SAS with CORR=EXCH option. All characteristics with p<0.05 after adjusting only for clustering of patients within the practice were entered into a full model. This was followed with backwards elimination, again using GEE to adjust for clustering to identify independent associations with symptomology, being retained if p < 0.05, in a reduced model. The models were further refined by requiring a magnitude of association to be either greater than an odds ratio (OR) of 1.5 or less than 0.6. After fitting the final model, all interaction terms were tested for significance at the 0.05 level. All analyses were performed separately by type of symptoms. The referent group for all comparisons was the asymptomatic group.
Additional analyses were performed examining associations with patients having only one type of symptom, then for each combination of two types of symptoms, and lastly for those with all three types of symptoms. This was done to better ascertain if identified characteristics were associated with solely or primarily one type of symptom, if the magnitude of association differed for the type of symptoms, and if the magnitude of associations increased or changed with combinations of symptoms. Because power was limited for one symptom type alone and specified combination analyses, the significance level for entry into the full model and then retention in the reduced model was relaxed (increased) to 10%. Associations among patient-, tooth- and crack-level characteristics were examined, using GEE, to help explain/understand variations in associations across models (Supplemental Tables 1–3). All odds ratios (ORs) and p-values reported below were adjusted for clustering of patients within practitioner with GEE. All analyses were performed using SAS software (SAS v9.4, SAS Institute Inc., Cary NC).
Results
In all, 2,858 patients/cracks were enrolled by 209 practitioners, with a mean/median of 14.8/15 patients per practice and a range of 1 to 20; 1,561 (54%) of the teeth were asymptomatic. Figures 1– 3 show the distribution of symptom types. Pain was reported from several stimuli, referred to here as “types of pain.” Among the 1,297 symptomatic patients/teeth, pain to cold was present in 1,055 (81%), pain on biting was present in 459 (35%), and 367 (28%) exhibited spontaneous pain; 409 (35%) had more than one type of symptom.
Figure 1.
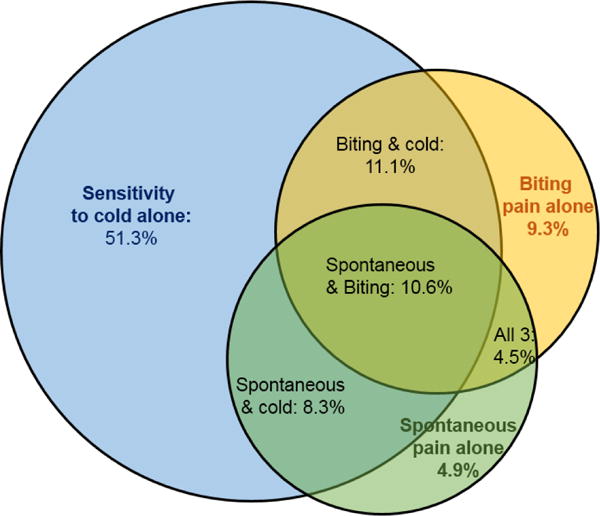
Distribution according to type and combinations of symptoms among 1,297 symptomatic teeth
Figure 3.
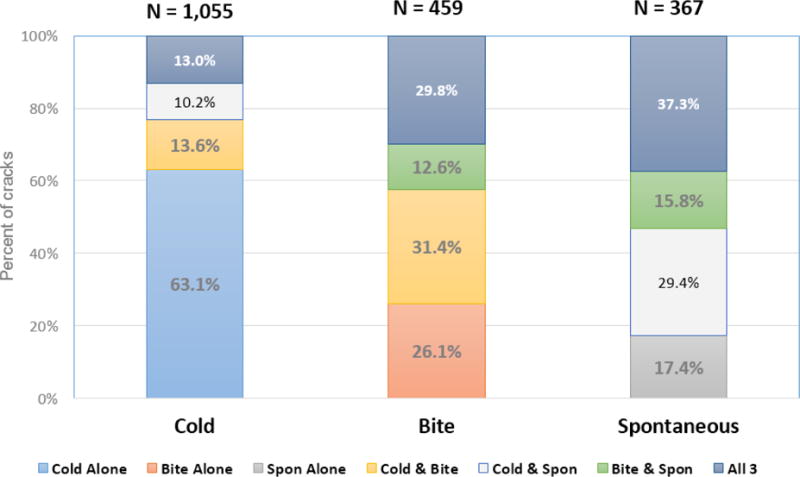
Percent of cracks with each symptom type combination within each overall type of symptom assessed
Patient-level characteristics
The mean age (SD) of the patients was 54 (12);, the median age (inter-quartile range) was 55 (46 – 62) years, with a range from 19 to 85 years. Overall, 1,813 (63%) patients were female, 2,394 (85%) were non-Hispanic white, 2,213 (77%) had some dental insurance, and 2,432 (86%) had some college education. Two-thirds of the patients (N=1,900, 66%) reported clenching, grinding, or pressing their teeth together, and 2,190 of 2,690 main launch subjects (81%) reported feeling at least some stress when queried, with over one-third reporting feeling stress at least weekly (N=1,048, 39%). (Data on stress were not obtained in the pilot phase.)
Tooth-level characteristics
Overall, the majority of cracked teeth were molars (N=2,332; 82%), with more than half in the mandibular arch (N=1,675, 59%). Most of the external cracks, 92%, were on a tooth with a restoration: 71% of cracked teeth had one restoration, 19% had two restorations and 2% had 3-4 restorations. Virtually all study teeth had an opposing tooth (N=2,793, 98%); most were opposed by a natural or restored tooth (N=2,612, 91%). Twenty-two percent (N=638) had root exposure, and 24% (N=676) presented with at least one wear facet through enamel. A lesser percentage of subject teeth had caries present (N=302, 11%) or a non-carious cervical lesion (NCCL) (N=254, 9%). Only 53 (2%) had evidence of a crack on a radiograph. Removable partial denture abutment teeth (N=20, 0.7%) and fixed partial denture abutment teeth (N=3, 0.1%) were too rare to assess by type of symptom.
Crack-level characteristics
The majority of cracked teeth had a crack that was stained (N=2,319; 81%), connected with a restoration (N=2,095; 73%), was detectable with an explorer (N=1,980; 69%), blocked transilluminated light (N=1,862; 65%) and/or ran in a vertical direction (N=2,674; 94%). Tooth surfaces with cracks were distributed in a narrow range, from 44% (N=1,267) that involved the occlusal surface to 51% (N=1,463) involving the lingual surface; 1,028 (36%) had a crack that involved two or more surfaces.
Types of symptoms
(Table: Odds ratios (OR), 95% confidence Intervals (CI), and p-values from final modes for all outcomes.)
Table.
Odds ratios (OR), 95% confidence Intervals (CI), and p-values from final models for all outcomes.
| Overall categories of symptom type (not mutually exclusive) | Each type alone | Combinations of 2 types of symptoms | All 3 symptoms | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Cold | Biting | Spontaneous | Cold | Biting | Spontaneous | Cold and bite | Cold and spontaneous | Bite and spontaneous | Cold, Bite, & Spontaneous | |
| (N=1,055) | (N=459) | (N=367) | (N=666) | (N=120) | (N=64) | (N = 144) | (N = 180) | (N=58) | (N = 137) | |
| Characteristic 2 | OR (95% CI) |
OR (95% CI) |
OR (95% CI) |
OR (95% CI) |
OR (95% CI) |
OR (95% CI) |
OR (95% CI) |
OR (95% CI) |
OR (95% CI) |
OR (95% CI) |
| Patient level | ||||||||||
| Non-Hispanic White race | w | x | w | w | 0.52 * (0.33 - 0.82) |
0.58 * (0.38 - 0.89) |
||||
| Age less than 65 years | w | 1.72 *** (1.29 - 2.28) |
x | w | 2.25 ** (1.13 - 4.49) |
w | 2.33 ** (1.26 - 4.31) |
|||
| Clench, grind, OR press teeth together | w | 1.53 *** (1.25 - 1.89) |
w | 1.61 * (1.07 - 2.43) |
1.68 † (0.96 - 2.97) |
1.62 *** (1.26 - 2.07) |
x | x | x | |
| Tooth level | ||||||||||
| Molar | 1.60 *** (1.23 - 1.93) |
2.41 *** (1.74 - 3.32) |
2.32 *** (1.68 - 3.21) |
x | 2.81 *** (1.32 - 5.99) |
2.20 *** (1.49 - 3.25) |
1.93 ** (1.16 - 3.20) |
3.63 *** (1.55 - 8.53) |
2.50 *** (1.44 - 4.36) |
|
| In occlusion w/opposing tooth | 2.50 † (0.83 - 7.57) |
|||||||||
| Wear facet through enamel | x | w | x | 1.60 † (1.02 - 2.53) |
x | |||||
| Exposed roots | x | w | 0.35 ** (0.15 - 0.82) |
0.62 * (0.40 - 0.95) |
||||||
| Caries present | w | x | 1.79 ** (1.30 - 2.46) |
2.87 ** (1.90 - 4.32) |
||||||
| NCCL present | 0.55 ** (0.34 - 0.88) |
0.33 * (0.10 - 1.05) |
x | |||||||
| Evidence of crack(s) on radiograph | 2.53 * (1.24 - 5.17) |
2.70 ** (1.44 - 5.05) |
2.79 † (1.14 - 6.81) |
4.88 * (2.31 - 10.31) |
||||||
| Crack level | ||||||||||
| Stained | 0.50 *** (0.37 - 0.69) |
0.56 ** (0.42 - 0.76) |
0.31 ** (0.17 - 0.55) |
0.60 * (0.42 - 0.87) |
0.33 ** (0.18 - 0.60) |
0.49 * (0.30 - 0.79) |
||||
| Blocks transilluminated light | w | 1.59 *** (1.21 - 2.08) |
w | w | 2.34 * (1.19 - 4.61) |
2.09 *** (1.40 - 3.12) |
||||
| Connects with another crack | 1.75 * (1.11 - 2.77) |
|||||||||
| Extends to root | w | 2.02 * (1.25 - 3.25) |
||||||||
| More than 1 direction | 1.59 ** (1.15 - 2.19) |
x | ||||||||
| Distal surface | w | 1.59 *** (1.28 - 1.98) |
w | x | 1.60 * (1.05 - 2.43) |
1.86 * (1.19 - 2.92) |
w | 1.85 * (1.18 - 2.90) |
1.61 * (1.10 - 2.34) |
|
Variables with P<0.05 after adjusting for clustering were entered in a model. Backwards elimination was used retaining if p<0.05 for all but ALONE outcomes, which were retained if p<0.10 (because of limited power)
All models were further reduced by excluding 0.6 < OR < 1.5 (weak associations)
x indicates was entered in full model, but not retained because p>0.05 or p>0.10
w: not retained because 0.6 < OR < 1.5
:P<0.001,
P<0.01,
P<0.05,
P<0.10
NCCL: Non-carious cervical lesion.
Cracked teeth with one type of symptom (N=850, 66% of symptomatic):
666 ONLY sensitive to cold (63% of all those sensitive to cold; 78% of those with one type of pain)
120 ONLY pain on biting (26% of all those with pain on biting; 14% of those with one type of pain)
64 ONLY had spontaneous pain (17% of all those with spontaneous pain; 8% of those with one type of pain)
Cracked teeth with two types of symptoms (N=310, 24% of symptomatic):
144 had pain to cold and pain on biting (46% of those with two types of pain),
108 had pain to cold and spontaneous pain (35% of those with two types of pain),
58 had pain on biting and spontaneous pain (19% of those with two types of pain),
Cracked teeth with all three types of symptoms (N=137, 11% of symptomatic teeth).
Because of the numerous associations examined, namely, patient-, tooth- and crack-level for 10 outcomes overall (descriptive) statistics are described below. Univariable associations adjusted only for clustering within practice are presented in Supplemental Tables 4–7 for each type of symptom for patient-, tooth- and crack-level characteristics, respectively. The associations described below are from the 10 final models that represent independent associations presented in the Table.
Independent associations ( Table)
To ascertain if associations would be affected by how crack-level characteristics were analyzed, the analysis was repeated placing cracks into the following categories: all cracks exhibited the characteristic; at least one crack exhibited the characteristic; no cracks exhibited the characteristic. There was no change to the final, reduced model (results not shown). All possible 2-way interactions were entered and none were found significant, indicating that an additive model is sufficient. The independent associations with each type of symptom from the final models are presented in the Table. The following characteristics and types of symptoms associated with those characteristics presented below represent a 1.50 increased odds of one or more type of symptoms, or inversely with ORs < 0.60.
Pain to cold
A crack being on a molar was the only characteristic at the patient-, tooth-, or crack-level, that was associated with pain to cold overall (biting or spontaneous pain or both were also present for some) with a 60% increased odds (OR=1.60); no characteristic was associated with pain to cold alone.
Pain on biting
A crack being present on a molar tooth and pain on biting was the most consistent association observed, as was the presence of pain on biting overall (OR=2.41), pain on biting alone (OR=2.81), pain on biting combined with pain to cold (OR=2.20), with spontaneous pain (OR=3.63), and with all three types of pain (OR=2.50). Age less than 65 years was associated with pain on biting alone (OR=2.25), with all 3 types of symptoms being present (OR=2.33), and weaker association with pain on biting overall (OR=1.72). Clenching, grinding, or pressing one’s teeth together were associated with pain on biting overall (OR=1.53), pain on biting alone (OR=1.61), and pain on biting combined with pain to cold (OR=1.62). Evidence of crack(s) on a radiograph was associated with pain on biting overall (OR=2.53) and with pain to cold and pain on biting in combination (OR=2.79). Blocking transilluminated light was associated with pain on biting and spontaneous pain in combination (OR=2.34) and when all three types of symptoms were present (OR=2.09). Cracks that extended in more than one direction were significantly associated with pain on biting overall (OR=1.6). The presence of a NCCL on a cracked tooth was inversely associated with pain on biting overall (OR=0.55) and with pain on biting alone (OR=0.33). Staining was inversely associated with pain on biting (OR=0.50), with pain to cold and pain on biting combined (OR=0.60), with pain on biting and spontaneous pain combined (OR=0.33) and with all 3 types of pain combined (OR=0.49).
In summary, patient age less than 65 years, a crack being on a molar, evidence of crack(s) on a radiograph, and a crack blocking transilluminated light were associated with an over two-fold increased odds of pain on biting overall, alone, or in combination with another type of symptom, and NCCL occurrence and staining were inversely associated.
Spontaneous pain
A crack being on a molar tooth was associated with spontaneous pain overall (OR=2.32), when combined with pain on biting (OR=3.63), and with all 3 types of symptoms being present (OR=2.50). Also similar to findings with pain on biting, evidence of crack(s) on a radiograph was associated with spontaneous pain overall (OR=2.70) and with pain to cold and spontaneous pain in combination (OR=4.88). Staining was inversely associated with spontaneous pain overall (OR=0.56), alone (OR=0.31), with pain on biting and spontaneous pain combined (OR=0.33), and with all 3 types of symptoms combined (OR=0.49). The presence of caries on a cracked tooth was associated with spontaneous pain and pain to cold in combination (OR=2.87) and moderately associated with spontaneous pain overall (OR=1.79).
In summary, crack presence on a molar, evidence of crack(s) on radiograph, and presence of caries were associated with an over two-fold increased odds of spontaneous pain overall, alone, or in combination with another type of symptom, and staining was inversely associated.
Stress was associated with each type of symptom when adjusted only for clustering, but in the final models, it was only significantly associated with pain to cold and spontaneous pain combination, and of marginal statistical significance with overall pain to cold (OR=1.06, P=0.06) and pain on biting (OR=1.09, P=0.06), and with pain on biting alone (OR=1.20, P=0.07) (Supplemental Table 8). As stress was not assessed during the pilot phase, thus excluding 167 patients, stress was not included in the final models presented in the Table (Odds ratios, 95% confidence Intervals, and p-values from final modes for all outcomes).
Discussion
Pain on biting is cited in the literature as the most common symptom in cracked teeth [5,8,9]. However, in the cohort of teeth followed in this study, the most prevalent symptom was pain to cold, found in 81% of the symptomatic teeth. Pain on biting was the next most common type of pain at 35%. Pain on biting alone occurred in only 4% of the cracked teeth. There are a number of considerations that may account for this variation from previous findings. First, the patient population in this study is a convenience sample of patients who attended a dental office and whose dentist judged that they would be likely to return for long-term follow-up for their cracks. It may be that a random sample of patients with cracked teeth from dental offices would produce a different distribution of the type of symptoms, as might a random sample of persons in the community at large who had not entered the dental care system. Additionally, other characteristics also present in some of the teeth could account for the widespread pain to cold, including caries, dentin hypersensitivity, and defective and/or leaking restorations[8, 13].
A variety of significant associations between types of symptoms and patient-, tooth-, and crack-level characteristics was found in the reduced model. The strongest associations (highest odds ratios) were found when there was evidence of crack(s) on a radiograph, for presence of pain on biting and spontaneous pain, or when pain to cold was combined with pain on biting or spontaneous pain. It is relatively rare to find evidence of a crack on a radiograph, because the size of the crack, the orientation of the crack relative to the x-ray beam, and the thickness of overlying dentin can all act to obscure radiographic visualization of a crack [8,13]. This is the case for our study as well, with only 53 teeth out of 2,858 showing radiographic evidence of the crack. However, it does indicate that when present, a crack evident on a radiograph is a strong correlate for pain, and this usually includes pain on biting.
The characteristic associated with the most symptom types was when the cracked tooth was a molar. This is consistent with data showing that molars are the teeth with the highest prevalence of cracks [1]. Data from a large-scale survey of general dentists showed cusp fractures in molars to be nearly four-fold greater than in premolars (79% vs 21%)[14]. Occlusal forces increase with more distal arch location [15], and so molar teeth, are subjected to greater functional and parafunctional forces compared to premolars. Guertsen [16] noted that excessive forces applied to a tooth could result in enamel and dentin fractures.
The patient-level factor with the most number of significant types of symptoms, although none surpassed the magnitude of 70% increased odds (namely, all with OR < 1.70), was patients who clench, grind, or press their teeth together. It is logical that of the types of symptoms that were significantly associated with teeth clenching, grinding, and/or pressing, three out of four involved biting (pain on biting presence, pain on biting alone, pain on biting and pain to cold in combination). Parafunctional activity is related to stress [17], which in turn is implicated as a causative factor in crack initiation and propagation [1].
Cracks located on the distal surface of teeth were significantly correlated with increased symptoms: presence of pain on biting, pain on biting alone, spontaneous pain alone, when both pain on biting and spontaneous pain were present, and when all three types of pain were present. As noted in our previous publication, it is not clear why a tooth with a crack on the distal surface would be more likely to be symptomatic compared to a tooth with cracks on other surfaces [10]. However, other studies have found correlations to cracks in the distal surface of teeth and adverse outcomes. In a smaller practice-based study of 634 teeth, Hilton et al [18] found that the highest odds ratio associating symptomatic cracked teeth to the specific cracked surfaces was when cracks were on the distal surface. Another study of cracked teeth diagnosed with reversible pulpitis and treated with a crown, found that the crack characteristic most commonly associated with a treated cracked tooth needing RCT was a crack on the distal marginal ridge (56% of the cracked teeth needing RCT) [19]. Again, the cause of this association is not clear.
The crack-level characteristic that had the next highest number of symptom types significantly associated with it was when a crack blocked transilluminated light (pain on biting presence, pain on biting and spontaneous pain, all three symptoms present). The blocking of light transilluminated through a tooth is often recommended as a method to determine that a crack penetrates into dentin; however, little evidence exists to support this contention [1]. Therefore, the increased odds of a variety of symptoms on a tooth with such a crack seems consistent with the concept that a crack to or into dentin would be more likely to stimulate a pain response. Two factors could potentially account for this. First, cracks that communicate with the oral cavity are a source of bacterial and toxin influx that can elicit pain [20, 21]. Second, dentin fluid can accumulate in the crack, where it is then subjected to dimensional change due to pressure or temperature fluctuation, increasing the rate of fluid movement through the dentin tubules and stimulating pain fibers [22]. Perhaps it is also possible that transillumination typically identifies cracks that extend all the way to the DEJ, and thus are more extensive and more likely to be associated with symptoms than those that are more confined to the tooth surface.
There were three characteristics inversely associated with symptoms: presence of NCCL, exposed roots, and stained cracks. Stain was by far the characteristic with the highest number of symptom types inversely associated with it. This is interesting in that it goes against empirically held practitioner beliefs [23, 24] that stained cracks imply the tooth is at greater risk for fracture or caries. Determination of risk relative to various external tooth characteristics is a longer-term goal of this study, but it is clear from baseline data that stained cracks are much less likely to be symptomatic, particularly for the presences of pain on biting and spontaneous pain, spontaneous pain alone, when pain on biting is found in conjunction with pain to cold or spontaneous pain, or when all three symptom types are present in the tooth. It seems likely that stained cracks are of long-standing duration [25]. Although this study’s case report form did not provide for recording if a crack stain was superficial or penetrating, a possible explanation for why cracked teeth would not be painful can be offered for both situations. If the stain is superficial in nature, then this may be because the crack does not penetrate into the dentin of the tooth and therefore does not act as a source of noxious stimuli. On the other hand, stain that does penetrate deeper into the tooth could potentially seal dentin tubule orifices, reducing fluid flow that is the source of pain on biting or pain to cold. The dentin sealing effect could also prevent bacteria and their toxins from traversing dentin tubules in a pulpward direction, thereby reducing this as a source of spontaneous pain. In this case, although the tooth may be more susceptible to fracture due to the separation that allows the stain ingress, since it is non-symptomatic, the tooth is less likely to be treated prior to a more catastrophic type of failure. Yet another explanation for this finding is that long-standing injury to the tooth that permits staining of cracks over time may promote secondary dentin formation [26], resulting in a less painful response.
The reduced likelihood of pain in cracked teeth with NCCLs and exposed roots could also have both a mechanical and a biologic explanation. The mechanical rationale may be more compelling since pain on biting is the symptom that is common to all significantly reduced pain categories: pain on biting presence, pain on biting alone in the case of NCCLs, and pain on biting plus spontaneous pain combination as well as pain on biting combined with spontaneous and pain to cold for cracked teeth with exposed roots. Both NCCLs and exposed roots could provide a mechanism for stress relief and crack mitigation in the tooth, by allowing for increased flexure of the tooth. In both cases, the occlusal forces are dissipated by increased tooth flexure, in turn minimizing further crack propagation and crack interface opening that could facilitate fluid movement or bacterial penetration.
A large amount of data was gathered on nearly 3,000 subjects in this study. As a result, relatively minor differences could be found to be statistically significant. Therefore, we moderated the statistical models used in the data analysis by requiring a magnitude of association to be either greater than an odds ratio of 1.50 or less than 0.60. We did this to reduce associations that were statistically significant but would have very little clinical meaning. We considered requiring a magnitude of OR>2.00 for retaining in the final model, as that better represents clinically meaningful differences; however, because of the varying number of patients in the regression models depending on type of symptom, greatly limiting power in some models, we judged that requiring such a magnitude would erroneously exclude some associations. We also focused our descriptions and interpretations on consistency of associations across models to reduce likelihood of Type 1 errors (falsely concluding that an association exists).
There are several differences between this current paper and our previous publication regarding the correlation of various patient-, tooth- and crack-level characteristics to pain in cracked teeth [10]. In that manuscript, analyses were on the global definition of “symptomatic,” i.e. a cracked tooth causing any type of pain. The focus in the present paper is on the type of pain as well as various combinations of types of pain. This places the emphasis on what the patient experiences rather than what the dentist observes. Importantly, the relation of the different types of pain to external crack characteristics show that cold pain alone, the most common type of pain, is not related to any specific patient, tooth or crack characteristic. This contradicts common clinical thinking and what many practitioners may have erroneously taken away from the earlier paper.
The inclusion criteria stated that an observable external crack was required for entry into the study. As a result, some cracked teeth that did not have a visible fracture line were not part of the study. However, it would not be possible to characterize a tooth sensitive to biting as a cracked tooth in the absence of objective, observable criteria. There are other clinical entities that can cause biting pain other than cracked teeth. Therefore, to ensure that the inclusion criteria was as uniform as possible, as well as to ensure that all teeth entered into the study did indeed have a crack, we instituted the requirement for visible evidence of a crack.
There are a number of limitations to this study. As mentioned previously, the study population is not a random sample. This was done for practical reasons, so participating practitioners could select patients who met inclusion criteria and were most likely to return for recall visits. Nonrandom selection could introduce bias, particularly if study patients do not mimic individuals who do not enter the dental care system, but the long-term goal of the study is to develop guidelines for those dentists and patients who do participate in regular dental care. Another potential weakness has to do with the subjective nature of specific measures used in the study; all participating personnel underwent training prior to participating, but the subjective nature of the assessments meant that there may be some variation in recorded data among the participants.
The study has several strengths including a high number of subjects from a large variety of dental practices across the U.S., which collected a large amount of data in a systematic, controlled manner.
Conclusion
This large-scale, practice-based observational study of patients with cracked teeth determined that although pain to cold was the most commonly noted pain associated with symptomatic cracked teeth, no patient-, tooth- or crack-level characteristic was significantly associated with pain to cold alone. Only when pain to cold was found in combination with pain on biting and/or spontaneous pain were characteristics associated with symptoms. Positive associations for various combinations of pain symptoms were present with cracks that: (1) were on molars; (2) in occlusion; (3) had a wear facet through enamel; (4) had caries; (5) were evident on a radiograph; (6) ran in more than one direction; (7) blocked transilluminated light; (8); connected with another crack; (9) extended onto the root; (10) extended in more than one direction; or (11) were on the distal surface. Persons who were < 65 yo or who clench, grind, or press their teeth together also were more likely to have pain symptoms. Pain symptoms were less likely in teeth with stained cracks or exposed roots, or in non-Hispanic whites. The investigators will continue to observe the teeth included in this study for several years to determine risk factors associated with adverse outcomes.
Supplementary Material
Figure 2.
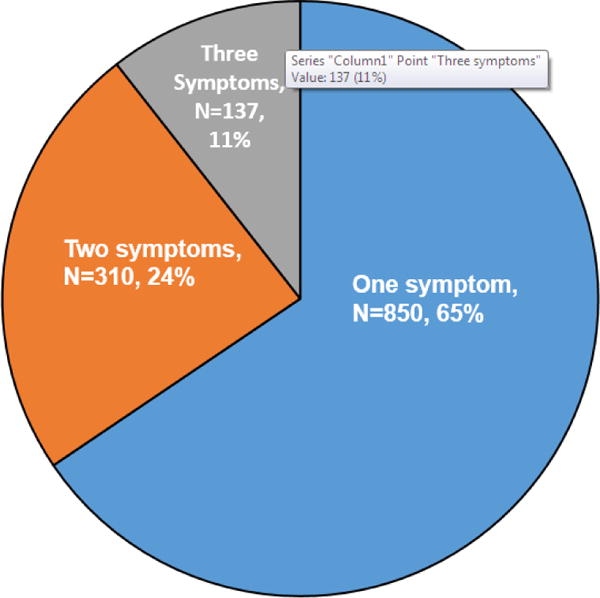
Distribution of 1,297 symptomatic cracked teeth by number of symptom types
Acknowledgments
This work was supported by NIH grant U19-DE-22516. An Internet site devoted to details about the nation’s network is located at http://NationalDentalPBRN.org. We are very grateful to the network’s Regional Coordinators who worked with network practitioners to conduct the study Midwest Region: Sarah Verville Basile, RDH, MPH, Christopher Enstad, BS; Western Region: Camille Baltuck, RDH, BS, Lisa Waiwaiole, MS, Natalia Tommasi, MA, LPC; Northeast Region: Patricia Ragusa, BA; South Atlantic Region: Deborah McEdward, RDH, BS, CCRP, Brenda Thacker AS, RDH, CCRP; South Central Region: Claudia Carcelén, MPH, Shermetria Massengale, MPH, CHES, Ellen Sowell, BA; Southwest Region: Stephanie Reyes, BA, Meredith Buchberg, MPH, Monica Castillo, MA. We are also grateful to the 12 National Network Practitioners who participated in this study as pilot practitioners: Midwest: David Louis, DDS, Timothy Langguth, DDS Western: William Reed Lytle, DDS, Don Marshall, DDS; South Atlantic: Stanley Asensio, DMD, Solomon Brotman, DDS; South Central Region: Jocelyn McClelland, DMD, James L. Sanderson Jr, DMD; Southwest: Robbie Henwood, DDS, PhD, Michael Bates, DDS; Northeast: Julie Ann Barna, DMD, MAGD; Sidney Chonowski, DMD, FAGD. We are grateful to Wendy Holder, DMD, a network practitioner in Alexander City, Alabama, and Paul Dirkes, DDS.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Thomas J. Hilton, Alumni Centennial Professor in Operative Dentistry, School of Dentistry, Oregon Health & Science University, 2730 S.W. Moody Ave., Portland, OR 97201-5042.
Ellen Funkhouser, Associate Professor, School of Medicine, University of Alabama, Birmingham, 1720 2nd Avenue South, Birmingham, AL 35294-0007.
Jack L. Ferracane, Chair, Department of Restorative Dentistry, School of Dentistry, Oregon Health & Science University, 2730 S.W. Moody Ave., Portland, OR 97201-5042.
Valeria V. Gordan, Professor, Dept of Restorative Dental Sciences, University of Florida, 1600 SW Archer Rd, Gainesville, FL 32610.
Kevin D. Huff, Private Practice, 217 W 4th St, Dover, OH 44622.
Julie Barna, Private Practice, 222 JPM Rd, Lewisburg, PA 17837.
Rahma Mungia, Assistant Professor, Department of Periodontics, School of Dentistry, University of Texas Health San Antonio, 7703 Floyd Curl Drive, MC 8258, San Antonio, TX-78229-3900.
Timothy Marker, Private Practice, 2210 Kulshan View Rd., Mount Vernon, WA 98273.
Gregg H. Gilbert, Professor and Chair, Department of Clinical and Community Sciences, School of Dentistry, University of Alabama at Birmingham, Birmingham, AL.
National Dental PBRN Collaborative Group, The National Dental PBRN Collaborative Group comprises practitioner, faculty, and staff investigators who contributed to this network activity. A list of these persons is at http://www.nationaldentalpbrn.org/collaborative-group.php.
References
- 1.Lubisich E, Hilton T, Ferracane J. Cracked teeth: a review of the literature. J Esthet Restor Dent. 2010;22:158–167. doi: 10.1111/j.1708-8240.2010.00330.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hilton T, Mancl L, Coley Y, Ferracane J, Baltuck C, Peterson J, PRECEDENT NW. Initial treatment recommendations for cracked teeth in Northwest PRECEDENT. J Dent Res. 2011;91(A) abst 2387. [Google Scholar]
- 3.Türp JC, Gobetti JP. The cracked tooth syndrome: An elusive diagnosis. J Am Dent Assoc. 1996;127:1502–7. doi: 10.14219/jada.archive.1996.0060. [DOI] [PubMed] [Google Scholar]
- 4.Noma N, Shimizu K, Watanabe K, Young A, Imamura Y, Khan J. Cracked tooth syndrome mimicking trigeminal autonomic cephalalgia: a report of 4 cases. Quint Int. 2017;48:329–337. doi: 10.3290/j.qi.a37688. [DOI] [PubMed] [Google Scholar]
- 5.Cameron CE. Cracked Tooth Syndrome. J Am Dent Assoc. 1964;69:405–411. doi: 10.14219/jada.archive.1964.0108. [DOI] [PubMed] [Google Scholar]
- 6.Cameron CE. The cracked tooth syndrome: Additional findings. J Am Dent Assoc. 1976;93:971–5. doi: 10.14219/jada.archive.1976.0034. [DOI] [PubMed] [Google Scholar]
- 7.Ehrmann EH, Tyas MJ. Cracked tooth syndrome: Diagnosis, treatment and correlation between symptoms and post-extraction findings. Aust Dent J. 1990;35:105–12. doi: 10.1111/j.1834-7819.1990.tb05872.x. [DOI] [PubMed] [Google Scholar]
- 8.Banerji S, Mehta S, Millar B. The management of cracked tooth syndrome in dental practice. British Dental Journal. 2017;222:659–666. doi: 10.1038/sj.bdj.2017.398. [DOI] [PubMed] [Google Scholar]
- 9.Roh B-D, Lee Y-E. Analysis of 154 cases of teeth with cracks. Dental Traumatology. 2006;22:118–123. doi: 10.1111/j.1600-9657.2006.00347.x. [DOI] [PubMed] [Google Scholar]
- 10.Hilton TJ, Funkhouser E, Ferracane JL, Gilbert GH, Baltuck CC, Benjamin P, Louis D, Mungia R, Meyerowitz C. Correlation between symptoms and external cracked tooth characteristics: findings from the National Dental Practice-Based Research Network. JADA. 2017;148:246–256. doi: 10.1016/j.adaj.2016.12.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gilbert GH, Williams OD, Korelitz JJ, et al. Purpose, structure, and function of the United States National Dental Practice-Based Research Network. J Dent. 2013;41(11):1051–1059. doi: 10.1016/j.jdent.2013.04.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Pigg M, Nixdorf D, Nguyen R, Law A. Validity of preoperative clinical findings to identify dental pulp status: a National Dental Practice-Based Research Network Study. J Endod. 2016;42:935–942. doi: 10.1016/j.joen.2016.03.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mamoun JS, Napoletano D. Cracked tooth diagnosis and treatment: an alternative paradigm. Eur J Dent. 2015;9(2):293–303. doi: 10.4103/1305-7456.156840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fennis WMM, Kuijs RH, Kreulen CM, Roeters FJM, Creugers NHJ, Burgersdijk RCW. A survey of cusp fractures in a population of general dental practices. J Prosthodont. 2002;15:559–563. [PubMed] [Google Scholar]
- 15.Arnold M. Bruxism and the occlusion. Dent Clin North Am. 1981;25:395–407. [PubMed] [Google Scholar]
- 16.Geurtsen W. The cracked-tooth syndrome: clinical features and case reports. Int J Periodontics Restorative Dent. 1992;12(5):395–405. [PubMed] [Google Scholar]
- 17.Carra M, Huynh N, Lavigne G. Sleep bruxism: a comprehensive overview for the dental clinician interested in sleep medicine. Dent Clin N Am. 2012;56:387–413. doi: 10.1016/j.cden.2012.01.003. [DOI] [PubMed] [Google Scholar]
- 18.Hilton T, Ferracane J, Mancl L, Coley Y, Baltuck C, Lubisich E, Gilbert A, Lowder L, Barnes C, Peterson J, PRECEDENT NW. Characteristics of cracks in teeth-association with symptoms. J Dent Res. 2012;92(A) abst 671. [Google Scholar]
- 19.Krell K, Rivera E. A six year evaluation of cracked teeth diagnosed with reversible pulpitis: treatment and prognosis. J Endod. 2007;33:1405–1407. doi: 10.1016/j.joen.2007.08.015. [DOI] [PubMed] [Google Scholar]
- 20.Ricucci D, Siqueira J, Loghin S, Berman L. The cracked tooth: histopathologic and histobacteriologic aspects. J Endod. 2015;41:343–352. doi: 10.1016/j.joen.2014.09.021. [DOI] [PubMed] [Google Scholar]
- 21.Hasan S, Kuldeep S, Salati N. Cracked tooth syndrome: overview of literature. Int J Applied and Basic Med Res. 2015;5:164–168. doi: 10.4103/2229-516X.165376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Brannstrom M, Astrom A. The hydrodynamics of dentin; its possible relationship to dentinal pain. Int Dent J. 1972;2:219–227. [PubMed] [Google Scholar]
- 23.http://leeannbrady.com/restorative-dentistry/is-the-tooth-cracked, accessed July 14, 2017.
- 24.Huff K. https://www.speareducation.com/spear-review/2017/07/managing-cracked-teeth-an-enigma-wrapped-up-inside-a-riddle-asking-questions, accessed July 14, 2017.
- 25.Ratcliff S, Becker I, Quinn L. Type and incidence of cracks in posterior teeth. J Prosthet Dent. 2001;86:168–172. doi: 10.1067/mpr.2001.116578. [DOI] [PubMed] [Google Scholar]
- 26.Robertson A. Pulp survival and hard tissue formation subsequent to dental trauma. A clinical and histological study of uncomplicated crown fractures and luxation injuries. Swed Dent J Suppl. 1997;125:1–65. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.