

Abstract
Although many experts have attempted communication about radiation risk, fears about radiation exposure stemming from the Fukushima Daiichi Nuclear Power Plant accident remain deeply rooted. The characteristics of the anxiety vary with social background, which makes it difficult to alleviate with one approach. Our ultimate goal is therefore to create risk-communication materials tailored to various groups with differing social backgrounds. Towards that end, the purpose of the present study was to clarify potential factors associated with radiation-related anxieties within these groups. After obtaining informed consent, we conducted focus group interviews (FGIs) with Fukushima residents from various social groups, including evacuees, emergency responders, government personnel, medical staff, and decontamination workers. We obtained narrative comments specifically related to the following two themes: (i) lessons learned (at work or home) in light of one’s position in society, and (ii) health issues. After transcribing the comments, we examined potential factors associated with radiation-related anxieties using both quantitative and qualitative study methods simultaneously, using the KH Coder software and the Steps for Coding and Theorization (SCAT) method respectively. FGIs were undertaken with 141 persons. Categories, words and storylines extracted in this study might indicate potential anxieties that are unique to each group, but our analysis also suggested that some anxieties were common to all groups. We expect to continue the analyses and, ultimately, to establish group-tailored risk-communication materials for achieving our final goal of adapting and better managing risk-communication efforts to help people deal more effectively with the scientific, technological and societal changes that came about after the disaster.
Keywords: radiation-related anxiety, narrative, group-tailored risk communication, social background, Fukushima Daiichi Nuclear Power Plant accident
INTRODUCTION
Many specialists have done their best to conduct effective radiation risk communication, aimed at residents and persons who dealt with disaster response, over the past 6 years since the Fukushima Daiichi Nuclear Power Plant (FDNPP) accident. Basic knowledge about radiation was offered, the present situation with regard to radioactive exposure and contamination was explained, and information concerning measures for dose reduction was disseminated. However, not all anxieties related to the radiation disaster have yet been resolved [1, 2].
From our experience in the field of radiation risk communication, it is not uncommon to encounter persons who harbor deep-rooted anxieties about the disaster [3]. According to a study concerned with the determinants of the choice made regarding whether to return to one’s hometown after the FDNPP accident, convenience and compensation were mentioned as factors that outweighed radiation exposure considerations [4, 5].
We suggest that the characteristics of people’s anxieties vary with their social background, and that this heterogeneity renders it difficult to carry out effective risk communication. Even if we continued providing well-intentioned conventional radiation-risk communication to the masses, it would be difficult to accommodate individual needs and unlikely that anxieties rooted in the disaster would be assuaged. For that reason, we focused on narrative comments obtained during the focus group interviews (FGIs), expecting to find evidence of group dynamics [6, 7] that would allow us to tailor risk communication in such a way as to target specific characteristics shared by particular groups.
The purpose of this research was to analyze factors potentially related to anxieties observed among persons with a diversity of social backgrounds and to design risk-communication materials incorporating measures that would deal with the characteristic factors underlying those anxieties. We propose to add such materials to conventional risk-communication tools. The ultimate aim of our work is to establish a group-tailored radiation-risk-communication approach that better addresses the needs of each unique social-background group.
MATERIALS AND METHODS
We summarize the framework of the data analysis in Fig. 1.
Fig. 1.

Framework for the data analysis.
Data collection
Data were drawn from the FGIs conducted among people who come from various social backgrounds who had been either a resident affected by the FDNPP accident, or involved in the subsequent disaster response. We conducted the FGIs from May 2016 to April 2017. After obtaining informed consent, we analysed the FGI responses for groups of people defined by having the same social background, each group consisting of 3–7 persons. In the FGIs, we presented the participants with two topics related to the FDNPP accident on 2011: (i) lessons learned (at work or home), in light of their position in society, and (ii) their health issues. To avoid influencing comments from participants, interviewers asked open-ended questions. All interviews were recorded electronically.
Data transcription
Recorded interviews were systemically transcribed into text with the RECAIUS™ Speech Transcribing Editor cloud service [8].
Data analysis
The data were subjected to two analysis methods: (i) KH Coder and (ii) Steps for Coding and Theorization (SCAT).
KH Coder
Transcribed data were first subjected to quantitative text mining analysis using KH Coder, a software program developed by K. Higuchi at Ritsumeikan University in Japan. This program consists of R programming language, with the ‘ChaSen’ language-morphology-analysis system as the backend program. KH Coder produces a list of words ordered according to their frequencies and interrelationships [9].
We focused on the top 30–40% of words most frequently used in responses to the FGI. We reviewed all sentences containing those key words to examine usage of the words, and we eliminated sentences in which the word was used inappropriately or was unrelated to the topic discussed. We then categorized the FGI responses into clusters of major topics based on the key words. Specifically, within the KH Coder software, we used the ‘hierarchical cluster analysis mode’ in which distance between words is given by the Jaccard index, and the binding rule is Word’s method. In order to categorize the contents, assisted by the ‘co-occurrence network mode’, we then visualized the spatial distribution of each key word in two dimensions by using the ‘multidimensional analysis mode’. Finally, we categorized the FGI response contents into clusters, named them according to their primary topic, subcategorized the primary topic, and listed the detailed contents corresponding to each topic. The second and third authors performed the KH Coder analysis; the first author compared and compounded the results for summarizing them.
SCAT
The SCAT method was applied for qualitative analysis to identify important but low-frequency words and content among the FGI responses. SCAT was developed as a qualitative data-analysis method by T. Otani at Nagoya University in Japan. In this analysis, we chose words and sentences that the interviewer and analyzer deemed to be noteworthy, and we applied them to decontextualization and theorization steps. In the decontextualization step, we extracted from the FGI responses key words from phrases that were chosen by the interviewer and analyzer, and we paraphrased them by using appropriate professional terms not used in the original response. In the theorization step, we replaced the terms with conceptualized terms. Finally, we transformed these key words from phrases into short ‘storyline’ based on the emerging themes, which is analogous to spinning threads from the conceptualized terms obtained in the first step [10, 11]. Every author took part in the SCAT analysis.
Ethical considerations
This study was conducted in collaboration with the study group members of the Health Effects of Radiation organized by Ministry of the Environment, Japan. Permission to receive data from the FGI was granted (No. 2573) by the ethical review boards at Fukushima Medical University.
RESULTS
FGIs
The number of interviewees was 141 (90 males, 51 females). The social groups of the interviewees comprised residents, evacuees, firefighters, university public communication officers, medical staff who dealt with hospital evacuations, medical staff who dealt with medical support for the radiation disaster, decontamination workers, and mothers with small children. The distribution of participants according to social group is shown in Table 1.
Table 1.
Distribution
| Social background of the interviewee | Number in the group | Number of interviewees |
|---|---|---|
| Administrative officers who dealt with disaster management | 3 | 11 |
| Decontamination workers | 7 | 33 |
| Evacuees | 7 | 34 |
| Firefighters | 5 | 26 |
| Medical staff who dealt with hospital evacuation | 1 | 6 |
| Medical staff who dealt with radiation disaster support | 1 | 4 |
| Parents with small children | 2 | 6 |
| Teachers who worked in elementary and junior high schools | 2 | 6 |
| University public communication officers | 3 | 15 |
| Total | 31 | 141 |
KH Coder analysis
We illustrate the analysis with a summary of the responses from evacuees in Table 2 and show the list of anxieties classified into categories in Table 3.
Table 2.
Example summary of responses obtained from one of the evacuees’ FGI groups
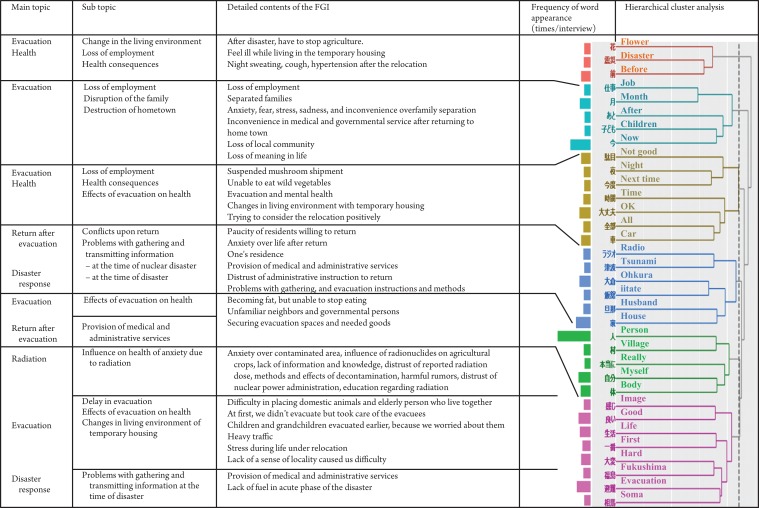 |
FGI = focus group interview. The contents of each FGI were categorized by some key words that were classified according to the hierarchical cluster analysis mode of the KH Coder software (right side of the table). We summarized the contents by primary topic, subtopic, and detailed contents corresponding to each category (left side of the table).
Table 3.
Classified categories of the interviewees’ anxieties for each social background
| Topic | Issues | Social background | ||||||
|---|---|---|---|---|---|---|---|---|
| A | B | C | D | E | F | G | ||
| Radiation | Influence on health of anxiety due to radiation | Yes | Yes | Yes | Yes | |||
| Education regarding radiation | Yes | Yes | Yes | |||||
| Distrust of nuclear power administration | Yes | Yes | ||||||
| Radiation and food safety | Yes | Yes | Yes | |||||
| Radiation effects on children | Yes | Yes | ||||||
| Anxiety over contaminated area, influence of radionuclides on agricultural crops, lack of information and knowledge, distrust of reported radiation dose, methods and effects of decontamination, harmful rumors | Yes | |||||||
| Excessive information about radiation (information overload) | Yes | |||||||
| Lack of accurate preliminary assessment of nuclear disaster, nuclear power plant (NPP) safety measures, radiation effects on families and children, social prejudice associated with having experienced the NPP accident | Yes | |||||||
| Radiation effects in decontamination work, radiation-related investigations and data reliability, trade-off between radiation risk and need for income, difficulty talking about radiation risk, environmental pollution from radionuclides | Yes | |||||||
| Collection and transmission of information concerning radiation | Yes | |||||||
| Evacuation | Loss of employment, means of communication, heavy traffic, delay of evacuation, destruction of hometown, loss of local community, changes in living environment of temporary housing, disruption of the family, loss of meaning in life | Yes | ||||||
| Work | Means of communication | Yes | Yes | |||||
| Management of evacuation centers | Yes | Yes | ||||||
| Mental health of evacuees, deep-seated radiation anxiety of residents, transmission of radiation information, health of evacuees, support for children, difficulty of radiation risk assessment, conflicts over role at work | Yes | |||||||
| Ambiguity concerning radiation effects and standards, problems with information gathering and transmitting, impact on staff responsible for nuclear disaster response, resumption of residents’ return, training of young officials, fire service in contaminated areas | Yes | |||||||
| School security and child safety, school evacuation, occupational responsibility and conflicts, responding to parents and children with radiation anxiety, measures for reducing radiation dose in schools, education about radiation at school | Yes | |||||||
| Awareness of decontamination work, lack of agreement regarding decontamination, human relations between decontamination workers and residents, consideration for affected residents pluses and minuses of NPPs | Yes | |||||||
| Transport and procurement of goods, information provision to evacuees and support givers, support for evacuees outside the prefecture and volunteer evacuees, distribution of stable iodine, improvement of infrastructure for residents | Yes | |||||||
| Work and evacuation, transfer to areas with evacuation orders lifted | Yes | |||||||
| Health | Evacuation and mental health | Yes | Yes | |||||
| Mental health accompanying the earthquake and the NPP accident | Yes | Yes | ||||||
| Effects of evacuation on health, trauma from the NPP accident, health of staff | Yes | |||||||
| Workplace environment | Yes | |||||||
| Influence on children of restricted outdoor activities | Yes | |||||||
| Health check-ups and hospital visits, dietary conditions/residential environment in workers’ dormitories | Yes | |||||||
| Mental health of staff involved in disaster response | Yes | |||||||
| Influence of restricted outdoor activity | Yes | |||||||
| Home | Verification of family safety | Yes | Yes | Yes | ||||
| Living base of staff | Yes | |||||||
| Return after evacuation | Conflicts upon return, anxiety about life after return, one’s residence, paucity of residents willing to return, provision of medical and administrative services, distrust of administrative instructions to return | Yes | ||||||
| Disaster response | Securing evacuation spaces and needed goods | Yes | Yes | |||||
| Problems with gathering and transmitting information at the time of the disaster | Yes | Yes | ||||||
| Damage to life-lines and shortage of supplies | Yes | Yes | ||||||
| Problems with gathering and transmitting information about the NPP accident, evacuation instructions and methods | Yes | |||||||
| Means of communication during the disaster, evacuation in the tsunami area, compensation for NPP accident | Yes | |||||||
A = Evacuees, B = University public communication officers, C = Firefighters, D = Elementary and middle-school teachers, E = Decontamination workers, F = Administrative staff, G = Bankers, NPP = nuclear power, plant.Yes = This group has concerns about these issues.
Topics related to radiation were not the main issues among the anxieties. There exists other various topics including evacuation, work, health, home, return after evacuation, and disaster response.
Evacuees is one of the FGI groups whose responses are illustrated in Table 2. We considered that they were interested in the effect of ‘evacuation’, particularly in regard to ‘health’ consequences, two of the main topics. During the acute phase of the disaster, they had ‘anxiety about contaminated area’, ‘influence of radionuclides on agricultural crops’ and ‘lack of information and knowledge’, as seen in see the sixth row in the column describing the detailed contents of the FGI responses. However, in the current situation, they have ‘anxiety about life after return’, shown in the fourth row in the column describing subtopics and detailed contents. Especially in the acute phase of the disaster, respondents mentioned that ‘lifesaving and maintenance of basic necessities for living’ and ‘health literacy including radiation health effects and protection’ should be provided (seventh subtopic). Currently, however, they expressed a need for ‘information for decision-making about whether to return to their home town or not’ in the situation of ‘paucity of residents willing to return’ and ‘provision of medical and administrative services’, which are the highest priorities for them, as seen in the fourth row of the column describing the detailed contents of the FGI.
Table 3 consists of the main topics, subtopics, and some parts of the detailed contents of the FGI responses given in Table 2. For example, the topic ‘evacuation’ in Table 3 contains the subtopics of ‘loss of employment’, ‘means of communication’, ‘heavy traffic’, ‘delay of evacuation’, ‘destruction of hometown’, ‘loss of local community’, ‘changes in living environment of temporary housing’, ‘disruption of the family’ and ‘loss of meaning in life’. All of these phrases are contained among the contents of the evacuation category in Table 2, which were derived from the evacuees’ FGI responses. With the same analysis method, we analyzed other groups’ FGI responses and derived the results presented in Table 3.
University public communication officers (social background B in Table 3) were interested in ‘correct knowledge about radiation and its effects’ and ‘how to transmit accurate radiation information’. They felt anxiety over the current situation in the form of ‘conflicts over role at work’ because of ‘excessive information about radiation (information overload).
The group of firefighters (social background C in Table 3) was interested in ‘resumption of residents’ return’ at work. To continue the ‘fire service in contaminated area’, they felt anxiety about ‘training young officers’.
SCAT
In addition to the KH Coder analysis, the database was subjected to the SCAT analysis. Key words or sentences were subjectively chosen by the researchers and analyzers and applied to the SCAT procedures as described above. Then, storylines from theoretical qualitative analysis were extracted from each FGI.
As an example, the following is an analysis of a response taken from a university public communication officer:
Despite being in a situation where she was affiliated with public institutions and had easy access to information on radiation, she felt strongly concerned about her family’s disorientation and radiation anxiety during the initial period of confusion. Anxiety in this context arose about the reliability of information, the ‘divergence between revealed information and reality’, ‘the loss of confidence in government authorities’ and ‘concern over how to survive in an ambiguous situation’. Moreover, she reacted anxiously and vigilantly to radiation issues ‘from the perspective of a mother’.
The point of view ‘being a mother’ would not have been extracted without the SCAT analysis. Using this analysis, we were also able to identify other low frequency of word appearance but important information such as this.
DISCUSSION
In earlier studies, various differences in risk perception have been demonstrated between groups having different social background characteristics (e.g. country, occupation, sex and age) [12–15]. However, few studies have focused on the differences in the characteristics of radiation-related anxieties between groups with particular social backgrounds [4, 5, 16]. The results of the current study suggest that some characteristic anxieties are common to all groups, but that other characteristics of anxiety often vary according to social background. According to our results, the evacuees’ prevailing issue was ‘how to prevent adverse health effects after the evacuation’. On the other hand, we found that university public communication officers were interested in ‘offering information to promote media literacy’, and that a prevailing issue among firefighters was to ‘protect from further disaster the lives of the returnees’, which was part of their mission. The heterogeneity of these potential underlying factors makes it difficult to deal with radiation-related anxieties with the same approach for all subgroups.
We are planning to combine and compare the results from respondents with different social backgrounds to identify the primary radiation-related concerns that correspond to these individual social backgrounds. After identifying those primary concerns, we will initiate measures specifically designed to address them. Using our results, we propose to establish an advanced risk-communication style, which we call ‘group-tailored risk communication’. We therefore hope to serve as health-care supporters who can help people to better adapt and self-manage in the face of the social, physical and emotional challenges caused by the disaster [17].
There are several limitations to our research. First, we had only a limited amount of data to analyze quantitatively and qualitatively. Second, we only had data available from 4–6 years after the disaster. To overcome these limitations, we would first like to provide feedback in the form of our results to the same interviewees and to other people who belong to the same social backgrounds, to assess whether our results truly reflect their anxieties. Second, we would like to increase both the number of interviewees and the number of categories of the interviewees’ social backgrounds. Third, we would like to continue our research to examine the time trends in anxiety according to social background, especially for those anxieties identified by the qualitative SCAT analysis.
Our study suggests a new research methodology based on the comprehensive use of text-mining analysis methods, such as KH Coder and SCAT, for text data. The quantitative and qualitative analysis of results, as described here, have been used in various fields, including medicine [18, 19]. We analyzed the data not only with high-throughput quantitative methods, but also with qualitative methods for picking up rare but important patterns in the responses. These analysis methods have advantages and disadvantages. KH Coder makes it possible to analyze a large amount of quantitative information as high-throughput, but because it is based on word frequency, it may fail to detect some important low-frequency words that might be qualitatively important. We therefore attempted to pick up such rare but important information by combining KH Coder with the SCAT method.
If the human race continues at its current high standard of living, we may have no choice but to coexist with atomic power, at least for several decades. The research described herein will contribute to radiological protection and radiation risk communication for the benefit of the public as part of the nuclear energy policy in a time of peace. Furthermore, we think that our research paves the way toward a future risk-administration plan that is consistent with the public’s position. Formulating such a plan is our challenge in our mission to help the public to adapt and self-manage successfully in the face of a similar disaster [17].
CONCLUSIONS
Our lexical analysis suggested that there were differences between subgroups in terms of anxieties about radiation exposure in Fukushima. This is a methodology for establishing the advanced risk-communication style that we call ‘group-tailored risk communication’. Our primary results are included in this paper. In the future, we will attempt to apply these results by developing and using appropriate group-tailored risk communication materials, as per our ultimate goal.
ACKNOWLEDGEMENTS
The authors express thanks to the study group members and staff for their cooperation. They also thank Professor Koichi Tanigawa, Professor Aya Goto, Professor Tomoko Hatakeyama and Professor Kenneth E. Nollet for valuable advice. Results from this study were presented at the First International Symposium of the network-type Joint Usage/Research Center for Radiation Disaster Medical Science.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
FUNDING
This work was supported by Research on the Health Effects of Radiation organized by the Ministry of the Environment, Japan.
REFERENCES
- 1. The National Diet of Japan, the Fukushima Nuclear Accident Independent Investigation Commission The Official Report of the Fukushima Nuclear Accident Independent Investigation Commission: Main Report, 2012. http://warp.da.ndl.go.jp/info:ndljp/pid/3856371/naiic.go.jp/en/report/ (11 June 2016, date last accessed), in Japanese.
- 2. McCurry J. Fukushima residents still struggling 2 years after disaster. Lancet 2013;381:791–2. [DOI] [PubMed] [Google Scholar]
- 3. Perko T. Importance of risk communication during and after a nuclear accident. Integr Environ Assess Manag 2011;7:388–92. [DOI] [PubMed] [Google Scholar]
- 4. Orita M, Hayashida N, Urata H et al. Determinants of the return to hometowns after the accident at Fukushima Dai-ichi nuclear power plant: a case study for the village of Kawauchi. Radiat Prot Dosimetry 2013;156:383–5. [DOI] [PubMed] [Google Scholar]
- 5. Orita M, Hayashida N, Nakayama Y et al. Bipolarization of risk perception about the health effects of radiation in residents after the accident at Fukushima Nuclear Power Plant. PLoS One 2015;10:e0129227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Barbour RS. Making sense of focus groups. Med Educ 2005;39:742–50. [DOI] [PubMed] [Google Scholar]
- 7. Rabiee F. Focus-group interview and data analysis. Proc Nutr Soc 2004;63:655–60. [DOI] [PubMed] [Google Scholar]
- 8. Shiga N. Toshiba to Introduce Voice Synthetic Cloud Service: RECAIUS, ZAIKEI NEWS; 2015. http://www.zaikeinews.com/articles/1358/20151221/toshiba-introduce-voice-synthetic-cloud-service-recaius.htm (28 January 2016, date last accessed).
- 9. Higuchi K. Analysis of free comments in a questionnaire survey: quantitative analysis by KH Coder. Shakai Chosa. 2012;8:92–6. [Google Scholar]
- 10. Otani T. ‘SCAT’ a qualitative data analysis method by four-step coding: easy startable and small scale data-applicable process of theorization. Bull Grad School Educ Hum Dev 2007;54:27–44. [Google Scholar]
- 11. Otani T. The qualitative study series: SCAT; Steps for Coding and Theorization—easy startable with explicit procedure and small scale data-applicable process of theorization. Kansei Eng 2011;10:155–60. [Google Scholar]
- 12. Slovic P, Layman M, Kraus N et al. Perceived risk, stigma, and potential economic impacts of a high-level nuclear waste repository in Nevada. Risk Anal 1991;11:683–96. [DOI] [PubMed] [Google Scholar]
- 13. Kinoshita T. Thought and technique of the risk communication In: Shibata Y. (ed). Radiation Risk Communication. Nagasaki: Nagasaki Newspaper Pubish, 2012, 7–52 (in Japanese). [Google Scholar]
- 14. Nakayachi K, Takahito S. A comparison of perceived risk of crime between lay public and expert: estimation of crime numbers by undergraduate students and police officers. Jpn J Soc Psychol 2008;24:34–44. [Google Scholar]
- 15. Tsuchiya T, Taniguchi T, Kosugi M. An analysis of the risk communication activity in Tokai, Japan. Sociotechnica 2009;6:16–25 (in Japanese). [Google Scholar]
- 16. Miyazaki M. Establishment of Risk Communication With Risk Analysis Based on Individual Total Radiological Dose Assessments in Fukushima Prefecture www.env.go.jp/chemi/rhm/reports/h2503a_4.pdf (28 January 2016, date last accessed).
- 17. Huber M, Knottnerus JA, Green L et al. How should we define health? BMJ 2011;343:d4163. [DOI] [PubMed] [Google Scholar]
- 18. Goto A, Lai AY, Yoshida K et al. Leveraging public health nurses for disaster risk communication in Fukushima City: a qualitative analysis of nurses’ written records of parenting counseling and peer discussions. BMC Health Serv Res 2014;14:129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Aomatsu M, Otani T, Tanaka A et al. Medical students’ and residents’ conceptual structure of empathy: a qualitative study. Educ Health 2013;26:4–8. [DOI] [PubMed] [Google Scholar]