

Abstract
Background
There are several studies regarding the predictors or risk factors of unintended pregnancy, but only a small number of studies have been carried out concerning the socio-economic factors influencing the unintended pregnancy rate. This study aimed to determine the socioeconomic inequality of unintended pregnancy in Tehran, Iran, as a developing country.
Methods
In this hospital based cross-sectional study, 5152 deliveries from 103 hospitals in Tehran (the capital of Iran) were included in the analysis in July 2015. Socioeconomic status (SES) was measured through an asset-based method and principal component analysis was carried out to calculate the household SES. The concentration index and curve was used to measure SES inequality in unintended pregnancy, and then decomposed into its determinants. The data was analyzed by statistical Stata software.
Results
The Wagstaff normalized concentration index of unintended pregnancy (− 0.108 (95% Confidence Interval (CI) = − 0.119 ~ − 0.054)) endorses that unintended pregnancy is more concentrated among poorer mothers. The results showed that SES accounted for 27% of unintended pregnancy inequality, followed by the mother’s nationality (19%), father’s age (16%), mother’s age (10%), father’s education level (7%) and Body Mass Index (BMI) groups (5%).
Conclusion
Unintended pregnancy is unequally distributed among Iranian women and is more concentrated among poor women. Economic status had the most positive contribution, explaining 27% of inequality in unintended pregnancy.
Keywords: Unintended pregnancy, Socioeconomic inequality, Concentration index, Decomposition, Iran
Background
Unintended pregnancy is a major public health concern, being defined as a mistimed, unplanned or unwanted pregnancy at the time of conception [1]. Roughly, 213 million pregnancies took place globally in 2012, with 85% of all pregnancies occurring in developing or less developed countries, 56% of which occurred in Asia [2]. A proportion of all pregnancies are unintended or unplanned. In 2012, the worldwide rate of unintended pregnancy was 53 cases per 1000 women aged 15 to 44 years old. Bases on the data reported in 2012, 40% of pregnancies were unintended, a rate which has not significant decreased in recent decades (in 1995 and 2008 it was 43 and 42%, respectively) [2, 3]. In the United State, it was reported that 49% of pregnancies in 2006 and 48% in 2001 were unintended [4]. In another study conducted in United States, it was reported that 45% of pregnancies in 2011 and 51% in 2008 were unintended [5].
Based on a meta-analysis study in Iran, the unwanted pregnancy rate is 30.6% [6]. Even with the government’s efforts regarding family planning, nearly 55.4% of women at reproductive age use contraceptive methods [7].
A large number of studies have been conducted to detect the unintended pregnancy rate, its predictors and outcomes. For example, several studies have suggested that unintended pregnancies have some adverse health, socioeconomic and psychological outcomes for both women and their children [8–12]; however, only a small number of studies have been carried out concerning socio-economic factors influencing the unintended pregnancy rate.
The social determinants of health have an important impact on unintended pregnancy. In some studies [13–15], it has been shown that lower educational attainment is strongly associated with unplanned pregnancy. Controversially, Hamdela et al. [16] attested that there is no association between maternal education and unintended pregnancy. On the other hand, previous studies have suggested that unemployment has a significant association with unintended pregnancy [17, 18]. Goossens et al. [14] concluded that less-planned pregnancies were associated with lower socio-economic status. Briefly, there is some evidence that unintended pregnancy is associated with SES.
To the best of our knowledge, there has been no study quantitatively examining the impact of socio-economic inequality on unintended pregnancy. In the current study, we want to clarify the socioeconomic inequality in unintended pregnancy in Tehran, the capital of Iran, by means of a concentration index (CI) decomposition approach. This method helps to identify the major predictors of socioeconomic inequalities in unintended pregnancy in societies, which will be important for health policy makers. Therefore, this study aimed to determine the socioeconomic inequality in unintended pregnancy in Tehran, Iran, as a developing country.
Methods
Design, setting, and patients
In this hospital based cross-sectional study, 5152 mothers in labor who were referred to the Obstetrics and Gynecology Wards of 103 hospitals (affiliated with Tehran, Beheshti, and Iran’s Universities of Medical Sciences) in Tehran province (Capital of Iran) were included in the analysis.
We included all women in the defined period (between 6th to 21st July, 2015) in this study, regardless of the type of delivery (natural or cesarean section), the pregnancy outcome (live birth, stillbirth, or spontaneous abortion), type of hospitals (private or governmental), gravidity (nulliparous or multiparous), and singleton or twin. All women who gave informed consent were included in the study. The required data was gathered from medical centers with obstetrics and gynecology wards. The sampling process was performed for two weeks and the data was collected by 103 trained midwives or nurses. More detail about methodology was reported elsewhere [19–24].
Variable definition
Unintended pregnancy was selected as a dichotomous outcome variable, i.e. whether each of the interviewed mothers had experienced an unplanned pregnancy or not. However, and most importantly, the socioeconomic status (SES) of participants was measured using an asset based approach. In fact, there are three approaches to measure socioeconomic status: income, expenditure, and assets. Income estimation is the direct method for measurement of socioeconomic status, but as researchers usually have no access to the people’s true income, especially in developing countries, the income method is not normally suggested. The expenditure method is also not suggested as a favored method, as modern human life entails a plethora of expenditure items, ranging from health, food, housing, education, to recreational expenditures. To put it better, this enaction of this method consumes a vast amount of both time and resources. However, economists have suggested that the possession of household assets can be used as a proxy for income and expenditure as a socioeconomic measure. In the present study, to assess the SES via the asset-based method, the pregnant women were asked about whether they possessed certain assets, including a laptop, freezer, dish washing machine, vacuum cleaner, handicraft carpet, private cars, three-dimensional TV, side by side refrigerator, smart phone, a microwave, the number of rooms in their house, and the area of their residence per meter. Principal Component Analysis (PCA) was used to determine a household’s economic status, based on their possession of the above-mentioned assets [25].
Among the determinant variables, BMI values were categorized into different BMI groups, as previously described [26]: underweight (BMI < =19.9), normal (BMI = 20–24.9) overweight (BMI = 25–29.9) obese (BMI = 30–39.9) and morbidly obese (BMI > =40).
Statistical analysis
Inequality in unintended pregnancy was explored through the use of a Concentration Index (CI) [27]. As a CI is a decomposable index, it is widely when measuring inequality in health [28]. The CI was calculated as twice the covariance of a health variable and the fractional rank of a socioeconomic variable divided by the mean of a health-related variable, as follows:
| 1 |
Where yi denotes the health variable (i.e. unintended pregnancy) of i th individual, μ indicates its mean and Ri denotes the fractional rank of i th individual in terms of the index of their socio-economic status. CI values can vary between −1 and + 1; the negative and positive values indicated that inequality is disproportionally concentrated in either the poor or the rich (pro-rich and pro poor inequality), respectively, as well the value being zero in the case of no inequality [27]. Since, in this study, unintended pregnancy is a dichotomous variable, a normalization of the CI was needed to calculate inequality properly [29]. Wagstaff has suggested that the index could be normalized as follow [30]:
| 2 |
Therefore, in this study we used Wagstaff’s normalized concentration index (WCI) to measure and decompose unintended pregnancy inequality.
Decomposition approach
To reveal the contribution of each explanatory variable to the measured health inequality (i.e. unintended pregnancy inequality), a CI decomposition approach was used. According to Wagstaff, van Doorslaer and Watanabe [31], we applied a linear regression model linking unintended pregnancy (y) to a set of k determinants (xk):
| 3 |
Where is a set of k determinant variables for the i th individual, βk signifies the coefficient, and εi is an error term. Given the association of yi and in eq. (3), CI for (y) can be represented as:
| 4 |
Where is μ the mean of y, is the mean of xk, Ck is the normalized concentration index for xk (defined exactly like the CI for unintended pregnancy), is the elasticity of unintended pregnancy with explanatory variables, and GCε is the generalized CI for εi (residual component). More details pertaining to the CI decomposition method have been provided elsewhere [27, 31]. The first step in conducting the decomposition analysis is running an appropriate regression model for calculating the coefficients (βk) of the explanatory variables. Taking account of the dichotomous nature of unintended pregnancy in this study, and following Yiengprugsawan et al., a Generalized Linear Model (GLM) (with a binomial family and identity link) [32] was used for decomposing unintended pregnancy inequality. The pros of GLM, when compared to other regression models, is that it leads to valid coefficient estimates that do not differ by choice of reference group ( [33]). Data analysis was carried out using Stata statistical software (Stata version 13.0; Stata Corp LP, College Station, TX Stata).
Results
We analyzed 5152 deliveries in July 2015. Of these 20% were unintended pregnancy (n = 1021). 40.02 and 35.50% of mothers and fathers had a diploma, respectively. Based on the BMI categories, most of the mothers (43.25%) had a normal weight (BMIs were in the range of 20–24.9). Most of the mothers and fathers were aged 20–39 and 30–39, respectively. Fortunately, most of the mothers didn’t have a history of abortion (80%) or miscarriage (99%). The results show that 42.08% of the studied mothers had been pregnant at least four times (Table 1).
Table 1.
Summary statistics about unintended pregnancy and its determinants in Iran, (2015)
| Variable | |||
|---|---|---|---|
| n | % | ||
| Unintended pregnancy | Yes | 1021 | 19.82 |
| No | 4131 | 80.18 | |
| Scio-economic status | Poorest | 1063 | 20.63 |
| Poorer | 1048 | 20.34 | |
| Middle | 1006 | 19.53 | |
| Richer | 1018 | 19.76 | |
| Richest | 1017 | 19.74 | |
| Mother’s education level | Illiterate | 204 | 3.95 |
| under Diploma | 1219 | 23.67 | |
| Diploma | 2062 | 40.02 | |
| Academic | 1667 | 32.36 | |
| Father’s education level | Illiterate | 164 | 3.18 |
| under Diploma | 1534 | 29.77 | |
| Diploma | 1828 | 35.50 | |
| Academic | 1626 | 31.55 | |
| BMI category | Underweight | 550 | 10.68 |
| Normal | 2228 | 43.25 | |
| Overweight | 1623 | 31.50 | |
| Obese | 535 | 10.38 | |
| Morbidly obese | 216 | 4.19 | |
| Mother’s age | <=19 | 180 | 3.49 |
| 20–29 | 2414 | 46.86 | |
| 30–39 | 2375 | 46.10 | |
| > = 40 | 183 | 3.55 | |
| Father’s age | <=19 | 4 | 0.08 |
| 20–29 | 1237 | 24.01 | |
| 30–39 | 3089 | 59.96 | |
| > = 40 | 822 | 15.95 | |
| Mother’s nationality | Iranian | 4788 | 92.93 |
| Non- Iranian | 364 | 7.07 | |
| History of abortion | Have | 1033 | 20.05 |
| Not have | 4119 | 79.95 | |
| History of miscarriage | Have | 39 | 0.75 |
| Not have | 5113 | 99.25 | |
| Number of pregnancy | 0 | 1520 | 29.50 |
| 1–3 | 1464 | 28.42 | |
| > = 4 | 2168 | 42.08 | |
Figure 1 illustrates the concentration curve of unintended pregnancy. As Fig. 1 depicts, the concentration curve of unintended pregnancy lay above the line of equality. This means that unintended pregnancy was more concentrated among the poorer participants. To be exact, this reveals that there is an unequal disfavoring of the poor in unintended pregnancy in Iran. Besides, the WCI value of unintended pregnancy (− 0.108 (95% CI = − 0.119 ~ − 0.054)) endorses that unintended pregnancy is more concentrated among poorer mothers (Table 2).
Fig. 1.
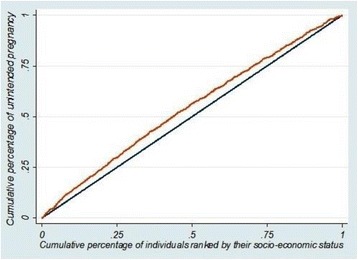
Concentration curve of unintended pregnancy in Iran (2015)
Table 2.
Wagstaff normalized concentration index (WCI) (95% confidence interval, standard error and P-value) for unintended pregnancy in Iran
| Unintended pregnancy | WCI value | Std. Err. | 95% Conf. interval for CI | P-value |
| −0.108 | 0.020 | − 0.119 ~ − 0.054 | < 0.001 |
The decomposition of unintended pregnancy is shown in Table 3. The WCIs of the determinant variables show that a number of features were concentrated among study participants with a lower socioeconomic status, such as the mother and father having a low educational level, being underweight, overweight or obese, aged < 29 years, and having experienced a larger number of pregnancies and deliveries. As the table shows, SES (about 27%) accounted for most of the unintended pregnancy inequality. If the value of the contribution of variable X were x and positive (negative), then, if the variable were to be equally distributed across the different socioeconomic groups, the unintended pregnancy inequality would decrease (increase) by x%. So, if socioeconomic resources were equally distributed across different SES groups, then inequality in unintended pregnancy in Iran would decrease by up to 27%. Mother nationality (19%), father’s age (16%), mother’s age (10%), Father’s education level (7%) and BMI groups (5%) followed in terms of the importance of their contribution to unintended pregnancy inequality in Iran. Table 3 also displays the residual components. The overall WCI of unintended pregnancy was − 0.108. The observed component of the overall WCI was − 0.085. This component shows that the determinants included in the current model were able to explain 79% of the measured inequality in unintended pregnancy in Iran. The rest of the inequality was due to residual (20.93%) components.
Table 3.
Decompositions of concentration index for unintended pregnancy in Iran
| coefficient | Elasticity | normalized Ck | Absolute contribution | Percent Contribution | |
|---|---|---|---|---|---|
| SES | |||||
| The poorest | 0.018 | −0.019 | −1.000 | − 0.019 | 17.59 |
| Poorer | 0.017 | 0.016 | −0.481 | −0.008 | 7.34 |
| Middle | −0.029 | −0.029 | 0.002 | 0.000 | 0.05 |
| Richer | −0.004 | −0.004 | 0.500 | −0.002 | 1.87 |
| The richest* | – | – | – | – | – |
| Sum | 26.86 | ||||
| Mother’s education level | |||||
| Illiterate | 0.001 | 0.000 | −0.797 | 0.000 | 0.15 |
| Under diploma | −0.001 | −0.001 | − 0.518 | 0.001 | − 0.57 |
| Diploma | 0.008 | 0.016 | −0.054 | −0.001 | 0.81 |
| Academic * | – | – | – | – | – |
| Sum | 0.39 | ||||
| Father’s education level | |||||
| Illiterate | 0.006 | 0.001 | −0.739 | −0.001 | 0.64 |
| Under diploma | 0.009 | 0.014 | −0.551 | −0.007 | 6.89 |
| Diploma | 0.011 | 0.020 | 0.017 | 0.000 | −0.31 |
| Academic* | – | – | – | – | – |
| Sum | 7.22 | ||||
| BMI category | |||||
| Underweight | −0.062 | −0.031 | − 0.143 | 0.004 | −4.06 |
| Normal | −0.045 | −0.099 | 0.115 | −0.011 | 10.50 |
| Overweight | −0.092 | −0.150 | − 0.005 | 0.001 | − 0.69 |
| Obese | −0.049 | − 0.025 | −0.020 | 0.001 | −0.47 |
| Morbidly obese* | – | – | – | – | – |
| Sum | 5.28 | ||||
| Mother’s age | |||||
| <=19 | 0.017 | 0.003 | −0.350 | −0.001 | 0.97 |
| 20–29 | −0.051 | −0.120 | − 0.153 | 0.018 | −17.04 |
| 30–39 | −0.061 | − 0.142 | 0.201 | − 0.029 | 26.43 |
| > = 40* | – | – | – | – | – |
| Sum | 10.37 | ||||
| Father’s age | |||||
| <=19 | 0.04 | 0.000 | −0.607 | 0.000 | 0.11 |
| 20–29 | −0.035 | −0.042 | − 0.224 | 0.010 | −8.80 |
| 30–39 | −0.074 | − 0.223 | 0.121 | − 0.027 | 25.04 |
| > = 40* | – | – | – | – | – |
| Sum | 16.35 | ||||
| Mother’s nationality | |||||
| Iranian | −0.016 | −0.075 | 0.276 | −0.021 | 19.18 |
| Others* | – | – | – | – | – |
| History of abortion | |||||
| Yes | 0.016 | 0.016 | 0.035 | 0.001 | −0.52 |
| No* | – | – | – | – | – |
| History of miscarriage | |||||
| Yes | −0.056 | −0.002 | 0.177 | 0.000 | 0.32 |
| No* | – | – | – | – | |
| Number of pregnancy | |||||
| 0 | 0.042 | 0.062 | 0.120 | 0.007 | −6.93 |
| 1–3 | 0.011 | 0.016 | −0.038 | −0.001 | 0.56 |
| > = 4* | – | – | – | – | – |
| Sum | −6.37 | ||||
| Total observed | −0.085 | 79.07 | |||
| Residual | −0.023 | 20.93 | |||
| Total | −0.108 | 100 | |||
*denotes reference group
Discussion
The results of present study show that the concentration curve of unintended pregnancy lies above the line of equality in the concentration curve. This means that unintended pregnancy is more concentrated among the poor and there is an unequal disfavoring of the poor in unintended pregnancy in Iran. Then, in order to disclose the contribution of each independent variable to the measured unintended pregnancy inequality, a concentration index decomposition approach was used. The results showed that SES accounted for 27% of unintended pregnancy inequality, followed by mother’s nationality (19%), father’s age (16%), mother’s age (10%), father’s education level (7%) and BMI groups (5%). If the value of the contribution of variable X were x and positive (negative), then unintended pregnancy inequality would decrease (increase) by x% if the variable were to be equally distributed across different socioeconomic groups. For as much as SES accounted for 27% of the unintended pregnancy inequality, if socioeconomic resources were equally distributed across the different SES groups, inequality in unintended pregnancy could decrease by up to 27% in Iran. Also, the results showed that the determinants included in the current model were able to explain 79% of the measured inequality in unintended pregnancy in Iran. However, in this study, 21% of unintended pregnancy inequality could not be explained by the systematic variation in the determinant variables across socioeconomic groups.
Unintended pregnancy is one of the most worrying public health issues and an extremely important worldwide reproductive health concern, leading to a considerable socioeconomic burden on both persons and wider communities [34]. There are several studies regarding the predictors or risk factors of unintended pregnancy [15, 35–38] as well as studies that explore the relationship between socioeconomic inequality and unintended pregnancy [39, 40], but such studies used traditional modes of analysis, such as logistic regression and odds ratio, whereas the concentration index and concentration curve methodology has been recommended specifically for the measurement of economic inequality in health outcomes [27, 30–33, 41]. Also, in previous studies of a similar nature [39], only educational level was used as an indicator of socioeconomic position, whereas the measure of household wealth can be assessed through multiple channels, such as “income level”, “consumption or expenditure data” and “asset-based data”. In this study we used the asset-based method as it is more appropriate for the study of developing countries. The asset-based technique is a fast and uncomplicated approach for collecting economic status data. This is because the collection of data requires little time [42, 43] and also because the asset based method is a more stable measure of economic status than consumption expenditure when considering factors such as economic shock or change [43].
No previous study has addressed the question of unintended pregnancy inequality through an approach comparable to the present study. Based on our results, we can state that unintended pregnancy was more concentrated among the poor and that SES accounted for 27% of unintended pregnancy inequality. This result has been confirmed by other published studies. Font-Ribera et al. [39] have shown that there is socioeconomic inequality in unintended pregnancy in Barcelona, Spain, and that unintended pregnancy is more concentrated among women in low socioeconomic positions. As previously stated, educational level was used as an indicator of socioeconomic position in Font-Ribera et al’s study, in which they demonstrated that women with an elementary education had higher odds of experiencing unintended pregnancies (7.22 times) than those with an university education.
The results of Lawrence Ikamari et al’s [44] study indicate that education level is not related with the incidence of unintended pregnancy. However, after adjusting their confounder variables (education, wealth index, employment status, ethnicity, household size and residence), household wealth index was significantly associated with unintended pregnancy, with women from medium (odds ratio = 0.66) and rich households (odds ratio = 0.51) being less likely to experience an unintended pregnancy than from those poor households. Employed women were also less likely to experience unintended pregnancy than unemployed women. In our study, the mother’s education exhibited no meaningful contribution to unintended pregnancy inequality. Finer and Zolna’s study [4] revealed that women with a low education level had the maximum unintended pregnancy rate, and that, in the case of economic status, the unintended pregnancy rate among deprived women was more than five times the rate for women in the highest income level. Therefore, our finding is consistent with other studies that report the association between economic status and a higher risk of unintended pregnancy [4, 39, 44].
Strengths and limitations of this study
In this study we measured economic status using an asset-based method, which is quick, simple and precise compared to other methods. Instead of using traditional analysis, for the first time, we used concentration index and concentration curve analysis to measure economic inequality and then decomposed the measured inequality. This is a cross sectional study with a self-administered questionnaire, therefore a causal interpretation of result should regarded with caution. Also, due to the cross sectional design, some biases may have been induced.
Conclusion
In conclusion, unintended pregnancy is unequally distributed among the Iranian women and is more concentrated among poor women. Economic status has the most positive contribution, explaining 27% of inequality in unintended pregnancy.
Acknowledgments
Funding
The study was funded by Royan Institute.
Availability of data and materials
The dataset used and/or analysed is available to be provided upon request.
Abbreviations
- BMI
Body mass index
- CI
Concentration Index
- CI
Confidence interval
- GLM
Generalized Linear Model
- PCA
Principal Component Analysis
- SES
Socioeconomic status
- WCI
Wagstaff normalized concentration index
Authors contributions
AAH, MS and ROS designed the study. MS and ROS were involved in data collection. AAH, EKM, MAR, SM and MAR participated in statistical analysis. All authors drafted the manuscript. Critical revision was done by AAH, MS, SM, EKM, MAR and ROS. The final version of manuscript was read and approved by all the authors.
Ethics approval and consent to participate
The study was approved by Ethical Committee of Royan Institute (Ethical code: EC/92/1097) in 2015 and was performed in accordance with Helsinki Declaration ethical codes. Informed consent was obtained from all participants.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Footnotes
Esmaeil Khedmati Morasae is part-funded by the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care North West Coast (NIHR CLAHRC NWC). The views expressed are those of the authors and not necessarily those of the NHS, NIHR or Department of Health.
Contributor Information
Reza Omani-Samani, Email: r.samani@gmail.com.
Mostafa Amini Rarani, Email: mostafaaminirarani@gmail.com.
Mahdi Sepidarkish, Email: mahdi.sepidarkish@gmail.com.
Esmaeil Khedmati Morasae, Email: E.Khedmati-Morasae@liverpool.ac.uk.
Saman Maroufizadeh, Email: saman.maroufizadeh@gmail.com.
Amir Almasi-Hashiani, Email: amiralmasi2007@gmail.com.
References
- 1.Trussell J, Vaughan B. Contraceptive failure, method-related discontinuation and resumption of use: results from the 1995 National Survey of family growth. Fam Plan Perspect. 1999;31:64–93. doi: 10.2307/2991641. [DOI] [PubMed] [Google Scholar]
- 2.Sedgh G, Singh S, Hussain R. Intended and unintended pregnancies worldwide in 2012 and recent trends. Stud Fam Plan. 2014;45(3):301–314. doi: 10.1111/j.1728-4465.2014.00393.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Singh S, Sedgh G, Hussain R. Unintended pregnancy: worldwide levels, trends, and outcomes. Stud Fam Plan. 2010;41(4):241–250. doi: 10.1111/j.1728-4465.2010.00250.x. [DOI] [PubMed] [Google Scholar]
- 4.Finer LB, Zolna MR. Unintended pregnancy in the United States: incidence and disparities, 2006. Contraception. 2011;84(5):478–485. doi: 10.1016/j.contraception.2011.07.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Finer LB, Zolna MR. Declines in unintended pregnancy in the United States, 2008–2011. N Engl J Med. 2016;374(9):843–852. doi: 10.1056/NEJMsa1506575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Moosazadeh M, Nekoei-moghadam M, Emrani Z, Amiresmaili M. Prevalence of unwanted pregnancy in Iran: a systematic review and meta-analysis. Int J Health Plann Manag. 2014;29(3):e277–ee90. doi: 10.1002/hpm.2184. [DOI] [PubMed] [Google Scholar]
- 7.Sadat-Hashemi SM, Ghorbani R, Majdabadi HA, Farahani FK. Factors associated with contraceptive use in Tehran, Iran. Eur J Contracept Reprod Health Care. 2007;12(2):148–153. doi: 10.1080/13625180601143462. [DOI] [PubMed] [Google Scholar]
- 8.Marston C, Cleland J. Do unintended pregnancies carried to term lead to adverse outcomes for mother and child? An assessment in five developing countries. Popul Stud. 2003;57(1):77–93. doi: 10.1080/0032472032000061749. [DOI] [PubMed] [Google Scholar]
- 9.Hardee K, Eggleston E, Wong EL. Irwanto, hull TH. Unintended pregnancy and women's psychological well-being in Indonesia. J Biosoc Sci. 2004;36(5):617–626. doi: 10.1017/S0021932003006321. [DOI] [PubMed] [Google Scholar]
- 10.Gipson JD, Koenig MA, Hindin MJ. The effects of unintended pregnancy on infant, child, and parental health: a review of the literature. Stud Fam Plan. 2008;39(1):18–38. doi: 10.1111/j.1728-4465.2008.00148.x. [DOI] [PubMed] [Google Scholar]
- 11.Trussell J. The cost of unintended pregnancy in the United States. Contraception. 2007;75(3):168–170. doi: 10.1016/j.contraception.2006.11.009. [DOI] [PubMed] [Google Scholar]
- 12.Tsui AO, McDonald-Mosley R, Burke AE. Family planning and the burden of unintended pregnancies. Epidemiol Rev. 2010;32(1):152–174. doi: 10.1093/epirev/mxq012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wellings K, Jones KG, Mercer CH, Tanton C, Clifton S, Datta J, et al. The prevalence of unplanned pregnancy and associated factors in Britain: findings from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3) Lancet (London, England) 2013;382(9907):1807–1816. doi: 10.1016/S0140-6736(13)62071-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Goossens J, Van Den Branden Y, Van der Sluys L, Delbaere I, Van Hecke A, Verhaeghe S, et al. The prevalence of unplanned pregnancy ending in birth, associated factors, and health outcomes. Hum Reprod. 2016;31(12):2821–2833. doi: 10.1093/humrep/dew266. [DOI] [PubMed] [Google Scholar]
- 15.Calvert C, Baisley K, Doyle AM, Maganja K, Changalucha J, Watson-Jones D, et al. Risk factors for unplanned pregnancy among young women in Tanzania. Journal of Family Planning and Reproductive Health Care. 2013;39(4):e2. doi: 10.1136/jfprhc-2012-100389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hamdela B, Gmariam A, Tilahun T. Unwanted Pregnancy and Associated Factors among Pregnant Married Women in Hosanna Town, Southern Ethiopia. PLoS ONE. 2012;7(6):e39074. doi: 10.1371/journal.pone.0039074. [DOI] [Google Scholar]
- 17.Kibret A, Bayu HA. M M. Prevalence of Unintended Pregnancy and Associated Factors among Pregnant Women Attending Antenatal Clinics in Debre-markos Town, North West Ethiopia 2012. J Women’s Health Care. 2015;4(3):1–6. [Google Scholar]
- 18.Theme-Filha MM, Baldisserotto ML, Fraga ACSA, Ayers S, da Gama SGN, MdC L. Factors associated with unintended pregnancy in Brazil: cross-sectional results from the Birth in Brazil National Survey, 2011/2012. Reproductive Health. 2016;13(3):118. doi: 10.1186/s12978-016-0227-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sepidarkish M, Almasi-Hashiani A, Maroufizadeh S, Vesali S, Pirjani R, Samani RO. Association between previous spontaneous abortion and pre-eclampsia during a subsequent pregnancy. Int J Gynecol Obstet. 2017;136(1):83–86. doi: 10.1002/ijgo.12008. [DOI] [PubMed] [Google Scholar]
- 20.Samani RO, Almasi-Hashiani A, Vesali S, Shokri F, Cheraghi R, Torkestani F, et al. Tehran survey of potential risk factors for multiple births. International journal of fertility & sterility. 2017;11(3):220. doi: 10.22074/ijfs.2017.4700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Omani-Samani R, Sepidarkish M, Safiri S, Esmailzadeh A, Vesali S, Farzaneh F, et al. Impact of gestational weight gain on cesarean delivery risk, perinatal birth weight and gestational age in women with normal pre-pregnancy BMI. The Journal of Obstetrics and Gynecology of India. 2017:1–6. [DOI] [PMC free article] [PubMed]
- 22.Omani-Samani R, Ranjbaran M, Amini P, Esmailzadeh A, Sepidarkish M, Almasi-Hashiani A. Adverse maternal and neonatal outcomes in women with preeclampsia in Iranian women. The Journal of Maternal-Fetal & Neonatal Medicine. 2017;(just-accepted):1–13. Epub ahead of print [DOI] [PubMed]
- 23.Omani-Samani R, Mohammadi M, Almasi-Hashiani A, Maroufizadeh S. Cesarean Section and Socioeconomic Status in Tehran, Iran. Journal of Research in Health Sciences. 2017;17(4):e00394. [PubMed] [Google Scholar]
- 24.Almasi-Hashiani A, Sepidarkish M, Safiri S, Morasae EK, Shadi Y, Omani-Samani R. Understanding determinants of unequal distribution of stillbirth in Tehran, Iran: a concentration index decomposition approach. BMJ Open. 2017;7(5):e013644. doi: 10.1136/bmjopen-2016-013644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Vyas S, Kumaranayake L. Constructing socio-economic status indices: how to use principal components analysis. Health Policy Plan. 2006;21(6):459–468. doi: 10.1093/heapol/czl029. [DOI] [PubMed] [Google Scholar]
- 26.Abenhaim HA, Kinch RA, Morin L, Benjamin A, Usher R. Effect of prepregnancy body mass index categories on obstetrical and neonatal outcomes. Arch Gynecol Obstet. 2007;275(1):39–43. doi: 10.1007/s00404-006-0219-y. [DOI] [PubMed] [Google Scholar]
- 27.O'Donnell O, Van Doorslaer E, Wagstaff A, Lindelow M. Analyzing health equity using household survey data: a guide to techniques and their implementation. Washington, DC: World Bank; 2008. [Google Scholar]
- 28.Combes J-B, Gerdtham U-G, Jarl J. Equalisation of alcohol participation among socioeconomic groups over time: an analysis based on the total differential approach and longitudinal data from Sweden. Int J Equity Health. 2011;10(1):10. doi: 10.1186/1475-9276-10-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Rarani MA, Rashidian A, Khosravi A, Arab M, Abbasian E, Morasae EK. Changes in socio-economic inequality in neonatal mortality in Iran between 1995-2000 and 2005-2010: an Oaxaca decomposition analysis. International journal of health policy and management. 2017;6(4):219. doi: 10.15171/ijhpm.2016.127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wagstaff A. The bounds of the concentration index when the variable of interest is binary, with an application to immunization inequality. Health Econ. 2005;14(4):429–432. doi: 10.1002/hec.953. [DOI] [PubMed] [Google Scholar]
- 31.Wagstaff A, Van Doorslaer E, Watanabe N. On decomposing the causes of health sector inequalities with an application to malnutrition inequalities in Vietnam. J Econ. 2003;112(1):207–223. doi: 10.1016/S0304-4076(02)00161-6. [DOI] [Google Scholar]
- 32.Yiengprugsawan V, Lim LL, Carmichael GA, Dear KB, Sleigh AC. Decomposing socioeconomic inequality for binary health outcomes: an improved estimation that does not vary by choice of reference group. BMC research notes. 2010;3(1):57. doi: 10.1186/1756-0500-3-57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Walsh B, Cullinan J. Decomposing socioeconomic inequalities in childhood obesity: evidence from Ireland. Economics & Human Biology. 2015;16:60–72. doi: 10.1016/j.ehb.2014.01.003. [DOI] [PubMed] [Google Scholar]
- 34.Yazdkhasti M, Pourreza A, Pirak A, Abdi F. Unintended pregnancy and its adverse social and economic consequences on health system: a narrative review article. Iranian Journal of Public Health. 2015;44(1):12–21. [PMC free article] [PubMed] [Google Scholar]
- 35.Exavery A, Kanté AM, Njozi M, Tani K, Doctor HV, Hingora A, et al. Predictors of mistimed, and unwanted pregnancies among women of childbearing age in Rufiji, Kilombero, and Ulanga districts of Tanzania. Reprod Health. 2014;11(1):63. doi: 10.1186/1742-4755-11-63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Oulman E, Kim THM, Yunis K, Tamim H. Prevalence and predictors of unintended pregnancy among women: an analysis of the Canadian maternity experiences survey. BMC Pregnancy and Childbirth. 2015;15:260. doi: 10.1186/s12884-015-0663-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Cheraghi P, Poorolajal J, Moeini B, Cheraghi Z. Predictors of unintended pregnancy among married women in Hamadan, western Iran: a case-control study. Iranian Journal of Public Health. 2013;42(8):854–859. [PMC free article] [PubMed] [Google Scholar]
- 38.Herzog AG, Mandle HB, Cahill KE, Fowler KM, Hauser WA. Predictors of unintended pregnancy in women with epilepsy. Neurology. 2017;88(8):728–733. doi: 10.1212/WNL.0000000000003637. [DOI] [PubMed] [Google Scholar]
- 39.Font-Ribera L, Pérez G, Salvador J, Borrell C. Socioeconomic inequalities in unintended pregnancy and abortion decision. Journal of Urban Health. 2008;85(1):125–135. doi: 10.1007/s11524-007-9233-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Izugbara C. Socio-demographic risk factors for unintended pregnancy among unmarried adolescent Nigerian girls. South African Family Practice. 2015;57(2):121–125. doi: 10.1080/20786190.2014.977042. [DOI] [Google Scholar]
- 41.Erreygers G, Van Ourti T. Measuring socioeconomic inequality in health, health care and health financing by means of rank-dependent indices: a recipe for good practice. J Health Econ. 2011;30(4):685–694. doi: 10.1016/j.jhealeco.2011.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Howe LD, Galobardes B, Matijasevich A, Gordon D, Johnston D, Onwujekwe O, Patel R, Webb EA, Lawlor DA, Hargreaves JR. Measuring socio-economic position for epidemiological studies in low- and middle-income countries: a methods of measurement in epidemiology paper. Int J Epidemiol. 2012;41(3):871–86. doi: 10.1093/ije/dys037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Liverpool LSO, Winter-Nelson A. Asset versus consumption poverty and poverty dynamics in the presence of multiple equilibria in rural Ethiopia. Washington DC: International Food Policy Research Institute; 2010. [Google Scholar]
- 44.Ikamari L, Izugbara C, Ochako R. Prevalence and determinants of unintended pregnancy among women in Nairobi. Kenya BMC Pregnancy and Childbirth. 2013;13:69. doi: 10.1186/1471-2393-13-69. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The dataset used and/or analysed is available to be provided upon request.