

Abstract
The aim of this study was to evaluate the timed sit-to-stand (STS) test performances of healthy young adults and to investigate the relationship of timed STS tests with 6-minute walk test (6MWT). A cross-sectional study was performed. A total of 40 healthy volunteers (mean age: 21.7 ± 1.2 years) were evaluated with 10, 30, and 60 seconds STS tests and 6MWT. Fatigue and shortness of breath were rated using Borg category-ratio scale (CR10) before and after each test. Weekly energy expenditures of volunteers were calculated using International Physical Activity Questionnaire. 30 and 60 seconds STS tests were moderately (r = 0.611 and r = 0.647, respectively) (P < .001) and 10 seconds STS test was weakly (r = 0.344) (P = .028) correlated with 6MWT. Among correlations of each STS test with 6MWT, none of them was statistically stronger to one another (P > .05). Borg fatigue scores after 10, 30, and 60 seconds STS tests were weakly correlated with fatigue score after 6MWT (r = 0.321, r = 0.378, and r = 0.405, respectively) (P < .05). Weekly energy expenditure (MET-min/week) was moderately correlated with 10, 30, and 60 seconds STS tests and 6MWT (r = 0.533, r = 0.598, r = 0.598, and r = 0.547, respectively) (P < .001). Considering the statistically significant relationship between timed STS tests and 6MWT, any of the timed STS tests may be used for a quick and alternative measurement of physical performance and functional capacity in healthy young adults.
Keywords: functional capacity, physical activity, sit-to-stand test, 6-minute walk test, young adults
1. Introduction
Functional capacity is the ability to perform activities of daily living that require sustained aerobic metabolism. The integrated efforts and health of the pulmonary, cardiovascular, and skeletal muscle systems dictate an individual's functional capacity.[1] For assessing functional capacity, cardiopulmonary exercise tests are commonly used to measure maximal oxygen consumption (VO2max) directly.[2] But, since most of the daily activities do not require maximal effort, the term of functional capacity is also used to express an individual's capacity to perform submaximal activities.[1] Therefore, physical performance tests like the 6-minute walk test (6MWT), shuttle walk test and timed get up and go test may also be used for assessing the functional capacity.[3]
The 6MWT is easy to apply and does not require any special equipment, therefore it is widely used in clinical practice.[4] Although, the 6MWT was first designed for using in older individuals or rehabilitation patients, it is now recognized for broader ability to predict functional capacity in all individuals. To date, the 6MWT was found to be correlated with the mobility related function, standing balance, and walk speed.[5]
The sit-to-stand (STS) test is a measure of mobility related function[5] and physical performance,[6] and it has been generally used to assess older population.[7] There are several options for assessing STS performance, including those does not require timing and those that are dependent on timing.[7] In the studies that investigate the relationship between the timed STS tests and physical performance parameters, correlations of the number of repetitions in STS test with the maximum walking speed[8] in 10 seconds STS (10sSTS) test and with the 6MWT distance in 60 seconds STS (60sSTS) test[9] have been reported.
It is not only the older patients who have diseases that might affect their functional capacity. Young patients with these kinds of diseases should also be tested and compared to healthy youngsters. Therefore, normative data on the functional capacity of the healthy individuals for all age spans is needed. The 6MWT is already validated for young people and it is the most common test for assessing the functional capacity in clinical setting but, it has troublesome logistical requirements such as 30 meter corridor and time constraints (total test time of 20–25 minutes) and occasionally it may be difficult to test the individuals with severely limited mobility with the 6MWT.
Since both the 6MWT and STS tests are considered physical performance tests, it is hypothesized that the STS tests may be correlated with the 6MWT and therefore a useful alternative for assessing the functional capacity of young adults, especially as a substitute test for patients with the limited functional capacity. Since the individual physical features, especially body height, may affect STS test results, the demographic data is also included in the correlation analyses. Additionally, the relationship between the participants’ amount of physical activity participation and their physical performance on these tests was investigated to help control for the effect of physical activity participation or sedentary behavior on test results. Finally, to investigate whether the STS tests are as physically demanding as the 6MWT, correlation between the fatigue levels after each STS test and the fatigue level after 6MWT was analyzed. Thus, aim of this study was to evaluate the STS test performance of young adults by studying the STS tests and their correlations with the 6MWT, while also studying the impact of physical activity participation on these performance measures.
2. Methods
2.1. Study population
Among 57 volunteers aged between 18 and 25, 40 volunteers (20 females, 20 males; mean age: 21.7 ± 1.2 years) were found eligible and included in this cross-sectional study. A university notice board was used to recruit the volunteers who are students in the school of physiotherapy and rehabilitation. In order to collect a homogeneous sample in terms of physical performance and to eliminate the factors that might lead to an impaired performance on physical tests, exclusion criteria were determined as; history of regular sports participation or current participation in sports activities, smoking, recent hospitalization, the presence of diagnosed chronic diseases that can affect exercise capacity, diagnosed visual and/or vestibular disorders and pathologies, and pain in the lower extremities that can affect mobilization abilities (traumas, fractures, etc.). The aim of the study and testing methods were explained to the participants in advance and written informed consent was obtained before testing. This study was approved by the Research Ethics Committee of a university hospital and conducted according to the Declaration of Helsinki. The Study was conducted in the Physiotherapy and Rehabilitation Division of a university.
2.2. Sit-to-stand tests
STS tests were carried out according to Bohannon's 2012 guideline.[7] A standard (45 cm) chair with no arm rests was used for testing. Each participant was asked to come forward on the chair seat until his/her feet are flat on the floor then instructed to stand up all the way until his/her knee and hip are fully extended and sit down while upper limbs were folded across the chest. Then, participants were instructed to perform this maneuver as fast as possible for 10, 30, or 60 seconds according to the test type. When the time of the test had elapsed, the participant was instructed to stop and the number of completed STS repetitions was recorded.
2.3. Six-minute walk test
The 6MWT was applied according to the “American Thoracic Society” guideline.[4] Before testing, participants were placed on a chair at the beginning of a 30-meter corridor to rest for at least 10 minutes. Participants were informed about testing with standardized phrases. Every minute, researcher encouraged subjects to continue walking and informed them of the time elapsed. After the test, participants’ walking distance was measured and recorded.
2.4. Fatigue and shortness of breath
Fatigue and shortness of breath were assessed with Borg Scale (category-ratio scale; CR10). Participants were asked to mark their level of fatigue and shortness of breath on the Borg Scale (0 point: none, 10 point: maximum) before and immediately after each STS test and the 6MWT. For fatigue and shortness of breath, the anchors were 0 for no fatigue/shortness of breath and 10 for maximum fatigue/shortness of breath.[10]
2.5. Physical activity participation
Physical activity levels of participants were assessed with “The International Physical Activity Questionnaire—Short Form (IPAQ-SF) (2004).” The IPAQ-SF includes 7 questions divided into frequency, intensity, and duration of participation in physical activities at low (walking), moderate and vigorous levels, and total physical activity per week. The data collected are reported as continuous data [expressed as metabolic equivalent (MET-min/week)] and as a categorical score [divided into low (<600 MET-min/week), moderate (600–3000 MET-min/week), and high (>3000 MET-min/week) activity level].[11]
2.6. Procedure
All participants performed the 6MWT and the STS tests (10sSTS, 30sSTS, and 60sSTS tests) consecutively on the same day. The order of the 6MWT and STS tests and the order of the STS subtests were determined by a random draw. A 30 minute rest period was given between the 6MWT and the STS tests. Five minute intervals were given between each STS test. Fatigue and shortness of breath were rated using the Borg Scale before and immediately after each test.
2.7. Analysis
In the literature, moderate-to-strong correlations (r = 0.410 to 0.780)[7,9,12] were reported for the relationship between STS tests and the various physical performance measures. Considering this, to achieve at least a moderate correlation with the correlation coefficient of 0.450 in this study, it is calculated that the minimum number of 36 individuals[13] were needed to detect this correlation with the study power of 80% and the confidence level of 95%.
Data distribution was assessed with Kolmogorov–Smirnov and Lilliefors tests. For analyzing the relationship of STS tests with the 6MWT distance and weekly energy expenditure (MET-min/week); demographic features with the STS tests and the 6MWT; and fatigue levels after the STS tests with the fatigue level after the 6MWT, Pearson correlation analysis was used for normally distributed data and Spearman correlation analysis was used for non-normally distributed or ordinal data. Correlation coefficients of STS tests with the 6MWT were compared with each other by Zou's confidence interval (CI) approach for dependent overlapping correlations[14] using COCOR package[15]. The results were considered significant with P values < .05. “Statistical Package for the Social Science (SPSS) Version 20.0” was used for analysis (SPSS Inc., Chicago).
3. Results
Demographics and test results (weekly energy expenditure, 6MWT, 10sSTS, 30sSTS, and 60sSTS tests) and fatigue levels after each STS test and the 6MWT of participants are shown in Table 1. According to the body mass index classification of World Health Organization, 2 participants (5%) were underweight (below 18.5 kg/m2); 31 participants (78%) were normal (18.5–24.9 kg/m2), and 5 participants (17%) were preobese (25.0–29.9 kg/m2). Of these, 26 (65%) had moderate physical activity level, and 14 (35%) had high physical activity level. None of the participants had low physical activity levels. The resting Borg Scores of fatigue of the participants were “zero” before the 6MWT and STS tests. Also they did not experience shortness of breath before or after the tests. None of the participants had an experience in performing functional exercise tests. All participants had the same ethnicity.
Table 1.
Demographic data and test results of participants (n = 40).

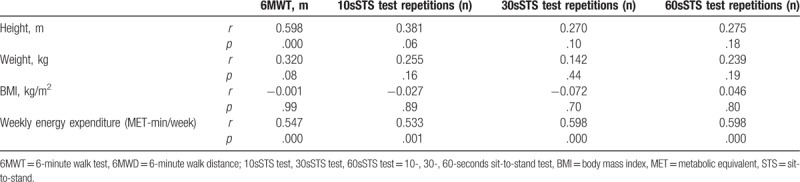
Of the demographic and physical variables of interest (age, height, weight, BMI), only body height was moderately correlated with the 6MWT. In relation to the demographic data with STS performances, no significant variation was observed. Both 6MWT and STS tests were also moderately correlated with weekly energy expenditure of participation in physical activity (Table 2).
Table 2.
Correlation of participants’ demographic data and weekly energy expenditure with 6MWT and STS test repetitions (n = 40).
6MWT distance was weakly correlated with the 10sSTS test and moderately correlated with 30sSTS and 60sSTS tests (Table 3 and Fig. 1).
Table 3.
Correlation of 6MWT with STS test repetitions and 6MWT Borg Score with STS tests Borg Scores (n = 40).

Figure 1.
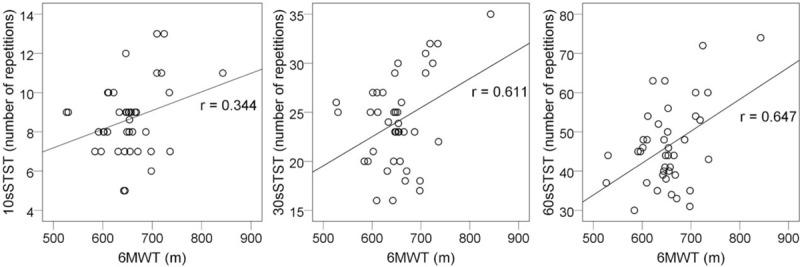
Scatter plot for the correlations of the number of repetitions in each sit-to-stand test with the maximum distance walked in 6-minute walk test. P < .05 for each plot. 6MWT = 6-minute walk test, 10sSTST = 10 seconds sit-to-stand test, 30sSTST = 30 seconds sit-to-stand test, 60sSTST = 60 seconds sit-to-stand test.
There are no significant differences between the correlation of 10sSTS test with the 6MWT and 30sSTS test with the 6MWT (rΔ = −0.053 [CI: −0.301 to 0.188]); 10sSTS test with the 6MWT and 60sSTS test with the 6MWT (rΔ = −0.076 [CI: −0.319 to 0.156]); 30sSTS test with the 6MWT and 60sSTS test with the 6MWT (rΔ = −0.023 [CI: −0.253 to 0.203]) indicating none of the correlations were statistically stronger to one another.
Borg scores of fatigue after each STS test were weakly correlated with the Borg score of fatigue after the 6MWT (Table 3).
4. Discussion
In the present study, 6MWT was found to be weakly correlated with 10sSTS test (P = .028) and moderately correlated with 30sSTS and 60sSTS tests (P = .000). Borg scores of fatigue after 10s-30s-60sSTS tests were weakly correlated with the Borg score of fatigue score after 6MWT (P < .05). Weekly energy expenditure was moderately correlated both with the 6MWT and all STS tests (P < .05).
Previous studies that have implemented the 6MWT in healthy adults have usually included broad age range groups. The average reported distance covered in the 6MWT was 698 ± 96 m in 20 to 40-year-old subjects[16] and 614 ± 56 m in 20 to 50-year-old subjects.[17] In a younger population (age of 16–18), the average 6MWT distance is reported 725 ± 61 m for men and 664 ± 50 m for women.[18] In an 18-year-old sample, the average 6MWT distance was reported ranging from 541 ± 109 to 561 ± 92 m.[19] The average 6MWT distance of 667 m in the present study is higher than the 18-year-old sample but similar to other studies. This may be explained by the fact that the average age in the present sample is close to 18 years; they are adults nonetheless and have a better physical performance compared to individuals in the upper age limit of adolescence.
The average 60sSTS test performance is reported 50 repetitions for men and 47 repetitions for women in 20 to 24-year-old subjects.[20] In the present study, the average 60sSTS test performance of the subjects was 45 repetitions which is similar to the results of the aforementioned study. 10sSTS and 30sSTS tests results were 8 and 24 repetitions, respectively, in the present study. According to this, it is noteworthy that as the duration of STS test increased, the number of the completed repetitions in STS test proportionally increased (Table 1). To the best of our knowledge, no clinical study is present in the literature that uses 10 or 30 seconds STS test in healthy young adults to compare with these results.
It is reported that 10sSTS test is correlated with knee extension force (r = 0.41–0.65)[8,21] and 30sSTS test is correlated with leg press strength (r = 0.71–0.78)[12] in a population over age of 60. Moreover, 10sSTS test is found to be correlated with maximum walking speed (r = 0.73)[8] and stair climbing performance (r = 0.56).[21] Ozatevli et al[9] reported a significant relationship between 60sSTS test performance and the 6MWT in chronic obstructive pulmonary disease (COPD) patients (r = 0.75) and healthy controls (r = 0.54) who are over the age of 60. These results are noteworthy since there is a difference between the correlation coefficients of healthy controls and COPD patients. But, authors state that this may be due to the limited number of healthy subjects. The results of the aforementioned studies are in consistent with the study of Bennell et al[6] which emphasizes that the timed STS tests evaluate (a) individual's ability to rise from a chair; (b) the muscle strength of trunk and lower extremities; (c) physical performance of the individual. In the present study, correlation coefficients between the STS tests and the 6MWT were moderate as in aforementioned studies. But, as Ozatevli et al states, this may be due to the relatively small sample size of the present study. Nevertheless, considering all STS tests had a statistically significant correlation with the 6MWT, it can be conjectured that the STS tests may be used to assess the functional performance in healthy young adults as well.
Soaresa and Pereira[22] investigated the reference values of the 6MWT in 20 to 80-year-old healthy adults and reported that the Borg fatigue score of 6MWT was minimum: 0—maximum: 5. In the present study, participants’ median of reported fatigue score was 4 [minimum: 1—maximum: 7] on a Borg scale after the 6MWT. Median of Borg fatigue scores after 10sSTS test, 30sSTS and 60sSTS tests were 1 [0–3]; 2 [0–4]; 5 [1–10], respectively. Borg score after the 6MWT was found to be significantly correlated with Borg scores after 10 seconds, 30 seconds, and 60sSTS tests. Although the correlations were weak, it may still be said that the physical demand of the STS tests, especially 30 seconds and 60 seconds tests, are similar to the 6MWT and this strengthens the assumption that the STS tests and the 6MWT are consistent with one another regarding the functional capacity assessment. Comparing the results of the maximum fatigue scores after the tests, it is observed that the maximum fatigue caused by the 60sSTS test (which is 10) is even higher than the maximum fatigue score after 6MWT (which is 7), indicating that the 60sSTS test is maybe more physically demanding than the 6MWT. This may be especially important for patients, because it indicates that the patients may need to rest during 60STS test.
In the present study, weekly energy expenditure was found to be correlated with both the 6MWT and 10 seconds, 30 seconds, and 60 seconds STS tests. It may be assumed that as the individual is more physically active, results of performance measures like the 6MWT or STS test will get better. This assumption is supported by Warburton et al[23] who reports the health benefits of physical activity including improvements in cardiopulmonary function. A dose–response relationship between physical activity and health benefits is reported.
As a limitation, correlation results in the present study could not be compared to a similar aged population because in the literature STS studies generally include elderly population or broad age range groups. Future studies should analyze these correlations in healthy young adults and the young individuals with diseases that may affect the functional capacity. Also, discriminatory power of the each STS test for assessing the functional capacity should be investigated extensively for these populations. Lastly, sample size of the present study was relatively small and the results may not be representative for the whole age span of young adults since the study included the volunteers aged between 18 and 25 years. Future studies with larger sample sizes and broader age groups in young adults are needed on this topic.
5. Conclusion
In this study, 10sSTS test was weakly and, 30 and 60 seconds STS tests were moderately correlated with the 6MWT. Comparative analysis of the correlations did not show a significant difference indicating none of the STS tests had an advantage over another for predicting the 6MWT. This result suggests that even a less physically demanding test like 10sSTS may provide evidence based data regarding the functional capacity.
Clinical Significance: (1) In observational or interventional studies which involve the assessment of functional capacity or physical performance of young adults, any of the timed STS tests may be used to gather related data especially when the 6MWT is not logistically possible to perform. (2) Results of the STS tests in young adults may provide a comparative data for evaluating the functional capacity of the patients with various diseases in the same age span.
Acknowledgments
The authors gratefully thank to Monica Ann Malt, MSN, RN, CPAN, Teaching English To Speakers Of Other Languages certified for her English editing support.
Footnotes
Abbreviations: 10sSTS = 10 seconds sit-to-stand, 30sSTS = 30 seconds sit-to-stand, 60sSTS = 60 seconds sit-to-stand, 6MWT = 6-minute walk test, BMI = body mass index, CI = confidence interval, COPD = chronic obstructive pulmonary disease, IPAQ-SF = International Physical Activity Questionnaire —Short Form, MET = metabolic equivalent, STS = sit-to-stand.
The authors have no funding and conflicts of interest to disclose.
References
- [1].Arena R, Myers J, Williams MA, et al. Assessment of functional capacity in clinical and research settings: a scientific statement from the American Heart Association Committee on Exercise, Rehabilitation, and Prevention of the Council on Clinical Cardiology and the Council on Cardiovascular Nursing. Circulation 2007;116:329–43. [DOI] [PubMed] [Google Scholar]
- [2].Fleg JL, Pina IL, Balady GJ, et al. Assessment of functional capacity in clinical and research applications: an advisory from the Committee on Exercise, Rehabilitation, and Prevention, Council on Clinical Cardiology, American Heart Association. Circulation 2000;102:1591–7. [DOI] [PubMed] [Google Scholar]
- [3].Noonan V, Dean E. Submaximal exercise testing: clinical application and interpretation. Phys Ther 2000;80:782–807. [PubMed] [Google Scholar]
- [4].ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med 2002;166:111–7. [DOI] [PubMed] [Google Scholar]
- [5].Harada ND, Chiu V, Stewart AL. Mobility-related function in older adults: assessment with a 6-minute walk test. Arch Phys Med Rehabil 1999;80:837–41. [DOI] [PubMed] [Google Scholar]
- [6].Bennell K, Dobson F, Hinman R. Measures of physical performance assessments: Self-Paced Walk Test (SPWT), Stair Climb Test (SCT), Six-Minute Walk Test (6MWT), Chair Stand Test (CST), Timed Up & Go (TUG), Sock Test, Lift and Carry Test (LCT), and Car Task. Arthritis Care Res 2011;63(suppl 11):S350–370. [DOI] [PubMed] [Google Scholar]
- [7].Bohannon RW. Measurement of sit-to-stand among older adults. Top Geriatr Rehabil 2012;28:11–6. [Google Scholar]
- [8].Bohannon RW. Alternatives for measuring knee extension strength of the elderly at home. Clin Rehabil 1998;12:434–40. [DOI] [PubMed] [Google Scholar]
- [9].Ozatevli S, Ozden A, Itil O, et al. Comparison of the Sit-to-Stand Test with 6 min walk test in patients with chronic obstructive pulmonary disease. Resp Med 2007;101:286–93. [DOI] [PubMed] [Google Scholar]
- [10].Borg GA. Psychophysical bases of perceived exertion. Med Sci Sports Exerc 1982;14:377–81. [PubMed] [Google Scholar]
- [11].Craig CL, Marshall AL, Sjostrom M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 2003;35:1381–95. [DOI] [PubMed] [Google Scholar]
- [12].Jones CJ, Rikli RE, Beam WC. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res Q Exerc Sport 1999;70:113–9. [DOI] [PubMed] [Google Scholar]
- [13].Algina J, Olejnik S. Sample size tables for correlation analysis with applications in partial correlation and multiple regression analysis. Multivariate Behav Res 2003;38:309–23. [DOI] [PubMed] [Google Scholar]
- [14].Zou GY. Toward using confidence intervals to compare correlations. Psychol Methods 2007;12:399–413. [DOI] [PubMed] [Google Scholar]
- [15].Diedenhofen B, Musch J. Cocor: a comprehensive solution for the statistical comparison of correlations. PLoS One 2015;10:e0121945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Gibbons WJ, Fruchter N, Sloan S, et al. Reference values for a multiple repetition 6-minute walk test in healthy adults older than 20 years. J Cardiopulm Rehabil 2001;21:87–93. [DOI] [PubMed] [Google Scholar]
- [17].Chetta A, Zanini A, Pisi G, et al. Reference values for the 6-min walk test in healthy subjects 20–50 years old. Respir Med 2006;100:1573–8. [DOI] [PubMed] [Google Scholar]
- [18].Geiger R, Strasak A, Treml B, et al. Six-minute walk test in children and adolescents. J Pediatr 2007;150:395–9. [DOI] [PubMed] [Google Scholar]
- [19].Kanburoglu MK, Ozdemir FM, Ozkan S, et al. Reference values of the 6-minute walk test in healthy Turkish children and adolescents between 11 and 18 years of age. Respir Care 2014;59:1369–75. [DOI] [PubMed] [Google Scholar]
- [20].Strassmann A, Steurer-Stey C, Lana KD, et al. Population-based reference values for the 1-min sit-to-stand test. Int J Public Health 2013;58:949–53. [DOI] [PubMed] [Google Scholar]
- [21].Bohannon RW, Smith J, Hull D, et al. Deficits in lower extremity muscle and gait performance among renal transplant candidates. Arch Phys Med Rehabil 1995;76:547–51. [DOI] [PubMed] [Google Scholar]
- [22].Soaresa MR, Pereira CA. Six-minute walk test: reference values for healthy adults in Brazil. J Bras Pneumol 2011;37:576–83. [DOI] [PubMed] [Google Scholar]
- [23].Warburton DE, Nicol CW, Bredin SS. Health benefits of physical activity: the evidence. CMAJ 2006;174:801–9. [DOI] [PMC free article] [PubMed] [Google Scholar]