

Abstract
Objective
To present a measure of effective workplace organizational policies, programs and practices that focuses on working conditions and organizational facilitators of worker safety, health and wellbeing: the Workplace Integrated Safety and Health (WISH) Assessment.
Methods
Development of this assessment used an iterative process involving a modified Delphi method, extensive literature reviews, and systematic cognitive testing.
Results
The assessment measures six core constructs identified as central to best practices for protecting and promoting worker safety, health and wellbeing: leadership commitment; participation; policies, programs and practices that foster supportive working conditions; comprehensive and collaborative strategies; adherence to federal and state regulations and ethical norms; and data-driven change.
Conclusions
The WISH Assessment holds promise as a tool that may inform organizational priority setting and guide research around causal pathways influencing implementation and outcomes related to these approaches.
INTRODUCTION
Efforts to protect and promote the safety, health, and wellbeing of workers have increasingly focused on integrating the complex and dynamic systems of the work organization and work environment.1–3 The National Institute for Occupational Safety and Health (NIOSH) applies this integrated approach in the Total Worker Health® (TWH) initiative by attending to “policies, programs, and practices that integrate protection from work-related safety and health hazards with promotion of injury and illness prevention efforts to advance worker well-being.”4 NIOSH has defined best practices as a set of essential elements for TWH that prioritizes a hazard-free work environment and recognizes the significant role of job-related factors in workers’ health and wellbeing.5,6
Increasingly, others have also emphasized the importance of improvements in working conditions as central to best practice recommendations.7–15 For example, the Robert Wood Johnson Foundation’s efforts have focused on building a culture of health in the workplace.16 Continuous improvement systems have relied on employee participation as a means of shaping positive working conditions.17–19 In Great Britain, continuous improvement processes are employed through a set of “management standards” that assess and address stressors in the workplace, including demands, control, support, relationships, role, and organizational change.20 Researchers have reported benefits to this integrated systems approach, including reductions in pain and occupational injury and disability rates;21–26 strengthened health and safety programs;27,28 improvements in health behaviors;29–38 enhanced rates of employee participation in programs;39 and reduced costs.28
Assessment of the extent to which a workplace adheres to best practice recommendations related to an integrated systems approach is important for several reasons. Understanding relationships between working conditions and worker safety and health outcomes can inform priority-setting and decision making for researchers, policy-makers, and employers alike, and may motivate employer actions to improve workplace conditions.40 In turn, identifying the impact of worker health and safety on business-related outcomes, such as worker performance, productivity, and turnover, may help to demonstrate the importance of protecting and promoting worker health for the bottom line.41 Baseline data with follow up assessments can also provide a means for tracking improvements in working conditions and related health outcomes over time. An important part of the process for evaluating workplace adherence to recommendations and understanding its relationship to worker and business outcomes is the creation of assessment tools that effectively capture implementation of best practice recommendations.
In 2013, the Harvard T.H. Chan School of Public Health Center for Work, Health and Wellbeing published a set of “Indicators of Integration” that were designed to assess the extent to which an organization has implemented an approach integrating occupational safety and health with worksite health promotion.1 This instrument assessed four domains: organizational leadership and commitment; collaboration between health protection and worksite health promotion; supportive organizational policies and practices (including accountability and training, management and employee engagement, benefits and incentives to support workplace health promotion and protection, integrated evaluation and surveillance); and comprehensive program content. The instrument was validated in two samples,42,43 and has played as useful role in the evolving dialogue around integrated approaches to worker safety, health and wellbeing.44,45 There is a need, however, for building on this work toward assessment of more conceptually grounded and practical constructs that measure the implementation of systems approaches focusing on improving working conditions as a means of protecting and promoting worker safety, health and wellbeing.
This manuscript describes an improved measure that reflects the Center’s conceptual model, which articulates the central role of working conditions in shaping health and safety outcomes as well as enterprise outcomes such as absenteeism and turnover (Figure 1).2 Working conditions, placed centrally in the model as core determinants of worker health and safety, encompass the physical environment and the organization of work (i.e., psycho-social factors, job design and demands, health and safety climate). The model highlights the potential interactions across systems, guiding exploration of the shared effects of the physical environment and the organization of work. Working conditions serve as a pathway from enterprise and workforce characteristics and effective policies, programs, and practices, to worker safety and health outcomes, as well as to more proximal outcomes such as health-related behaviors. Effective policies, programs, and practices may also contribute to improvements in enterprise outcomes such as turnover and health care costs. Feedback loops underscore the complexity of the system of inter-relationships across multiple dimensions, and highlight the potential synergy of intervention effects.
Figure 1.
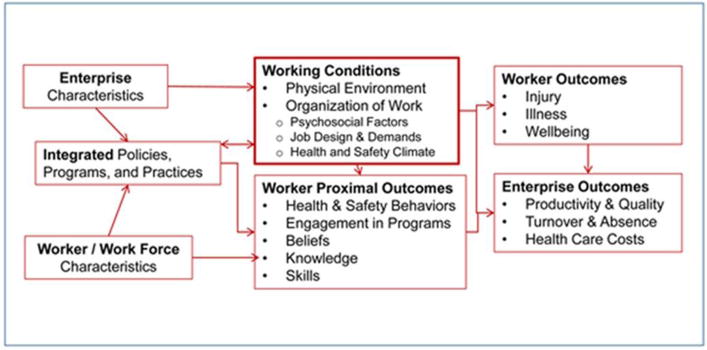
Systems level conceptual model centered around working conditions.
The purpose of this paper is to present a new measure of effective workplace organizational policies, programs and practices that focuses on working conditions as well as organizational facilitators of worker safety, health and wellbeing: the Workplace Integrated Safety and Health (WISH) Assessment. The objective of the WISH Assessment is to evaluate the extent to which workplaces implement effective comprehensive approaches to protect and promote worker health, safety and wellbeing. The policies, programs and practices encompassed by these approaches include both those designed to prevent work-related injuries and illnesses, and those designed to enhance overall workforce health and wellbeing.
Like the Indicators of Integration, this assessment is designed to be completed at the organizational level by employer representatives, such as directors of human resources, occupational safety, or employee health. These representatives are likely to be knowledgeable of organizational priorities, as well as policies, programs and practices related to workplace safety and health. Moreover, these representatives are in the position to influence the cultural and structural re-alignment necessary for integrated approaches. These organizational assessments are increasingly being used by policymakers, organizational leadership, and health and safety committees to guide goal setting and decision making. Organizational assessments such as this one may additionally complement worker surveys that can effectively capture employee practices as well as their perceptions of working conditions.
The WISH Assessment differs from the Indicators of Integration in two important ways: it embraces an increased focus on the central role of working conditions (as illustrated in Figure 1), and it expands assessment of best practice systems approaches to include a broader definition of protecting and promoting worker safety, health and wellbeing. This paper also describes the methods used to develop this instrument.
METHODS
Investigators from the Harvard Chan School Center for Work, Health and Wellbeing, a TWH Center for Excellence representing multiple institutions in the Boston area, developed the WISH Assessment.46 This instrument measures workplace-level implementation of policies, programs and practices that protect and promote worker safety, health and wellbeing. Accordingly, the intended respondents are organizational representatives who are knowledgeable about existing policies, programs and practices at workplaces, such as executives at small businesses, or directors of human resources or safety departments. Development of the WISH Assessment relied on an iterative process involving a modified Delphi method, extensive literature reviews, and systematic cognitive testing.
Delphi method and literature review
The Center’s conceptual model2 and related literature provided a guiding framework for the development of the WISH Assessment. As a starting point, we used constructs and related measures included in the Center’s published1 and validated42,43 Indicators of Integration tool. Based on an extensive review of literature, we expanded and revised the constructs captured by the instrument from four to seven. Next, we reviewed these constructs and their definitions using an iterative modified Delphi process47 with an expert review panel, including Center investigators. We reviewed the literature to identify extant items for these and similar constructs, placing a priority on the inclusion of validated measures where feasible. To ensure content validity and adequate coverage across attributes for each construct, we reviewed working drafts of the instrument with the Center’s External Advisory Board, as well as members of other TWH Centers of Excellence.48 Through repeated discussions, iterative review and revisions in six meetings over ten months, the Center members reached consensus related to a set of core domains and related measures. The working draft of the instrument was further reviewed by a survey methodologist, and prepared for cognitive testing. Following three rounds of cognitive testing and revision, as described below, Center investigators again reviewed and finalized this working version of the WISH Assessment.
Cognitive testing methods
The purpose of cognitive testing is to ensure that the items included on a survey effectively measure the intended constructs and are uniformly understood by potential respondents. The process focuses on the performance of each candidate item when used with members of the intended respondent group, and specifically assesses comprehension, information retrieval, judgment/estimation, and selection of response category.49,50 In the development of the WISH Assessment, we tested the instrument through three rounds of interviews.
Data Collection
Participants were asked to fill out the self-administered paper (N=15) or web (N=4) survey and participate in a telephone-administered qualitative interview with a trained interviewer. Participants received the survey 48 hours prior to the interview, and were encouraged to complete the survey as close to the actual interview as possible. They were not explicitly encouraged to consult with others, nor were they told not to.
The semi-structured interviews were conducted using a structured interview guide and retrospective probing techniques. The first round focused on comprehension of key attributes for each item (e.g., concepts of integration and collaborative environments) and of key words or phrases in the context of the question and instrument. Items revised following round 1 were again tested in a second round using the same approach. The focus of round 2 was to assess the adequacy of revisions in addressing the problems identified in round 1. A third round of interviews was conducted to confirm there were no additional problems due to revisions based on round 2. Across all rounds, the interviews concluded with a series of questions about the participant’s overall experience in completing the survey. For example, participants could provide general feedback on the survey content and the time required to complete the survey, and could comment on questions that didn’t fit within the survey or were duplicative. Participants were compensated with a $20 Amazon gift card for their time.
Sample
Participants were selected using purposive sampling to ensure diversity across industries and organizational roles, and included directors of human resources, occupational health, safety, and similar positions from hospitals (n=9), risk management (n=2), technology (n=2), transportation (n=2), community health center (n=1), manufacturing (n=1), laboratory research and development (n=1), and emergency response (n=1). Participants were identified through the Center for Work, Health and Wellbeing, and included attendees at a continuing education course and former collaborators on other projects. New participants were included in subsequent rounds of testing in order to ensure that revisions to items from each round adequately addressed the limitations, and that items were appropriately and uniformly interpreted among respondents.
Analysis
Following each round, feedback was summarized by item. Participant feedback was used to determine if the question wording needed modification. Each item was first considered on its own, and then assessed in terms of its fit in measuring its construct. A survey methodologist made suggested revisions which were then reviewed and discussed by the author team and interviewers to ensure that they retained substantive focus on the construct. We revised items when participants found terminology unclear or when participants’ answers did not map onto the intended construct. An item was removed if it was found to be redundant or did not adequately map onto the intended construct, and its deletion did not compromise content validity. We analyzed data across industry, and also assessed responses specific to the hospital industry, which included the most respondents.
RESULTS
Description of the constructs and measures
We identified six core constructs as central to best practices for protecting and promoting worker safety, health and wellbeing through the Delphi process and literature review. The items included in each construct with their response categories are included in Table 1. Following the Indicators of Integration, this assessment was designed to be answered by one or more persons within an organization who are likely to be familiar with the organization’s policies, programs and practices related to worker safety, health and wellbeing. Below, we present each construct, including its definition, rationale for inclusion, and sources of the items included.
Table 1.
Workplace Integrated Safety and Health (WISH) Assessment
|
Assessment Introduction: This brief survey is designed to assess the extent to which organizations effectively implement integrated approaches to worker safety, health and wellbeing. The term “integrated approaches” refers to policies, programs, and practices that aim to prevent work-related injuries and illnesses and enhance overall workforce health and wellbeing. This survey is meant to be completed by health and safety representatives, either in human resources or in safety, at the middle management level. There are no right or wrong answers–Your responses are meant to reflect your understanding of policies, practices and programs currently implemented within your organization. |
| 1. The following questions refer to leadership commitment. We define the term “leadership commitment” to mean the following: An organization’s leadership makes worker safety, health, and well-being a clear priority for the entire organization. They drive accountability and provide the necessary resources and environment to create positive working conditions. Response Categories: Please indicate how often you feel your organization or its leaders do each of the following: Not all the time, some of the time, most of the time, all of the time. |
| a. The company’s leadership, such as senior leaders and middle managers, communicate their commitment to a work environment that supports employee safety, health, and wellbeing. |
| b. The organization allocates enough resources such as enough workers and money to implement policies or programs to protect and promote worker safety and health. |
| c. Our company’s leadership, such as senior leaders and managers, take responsibility for ensuring a safe and healthy work environment. |
| d. Worker health and safety are part of the organization’s mission, vision or business objectives. |
| e. The importance of health and safety is communicated across all levels of the organization, both formally and informally. |
| f. The importance of health and safety is consistently reflected in actions across all levels of the organization, both formally and informally. |
| 2. The following questions refer to participation. We define the term “participation” to mean the following: Stakeholders at every level of an organization, including organized labor or other worker organizations if present, help plan and carry out efforts to protect and promote worker safety and health. Response categories: For these collaborative activities or programs, please indicate how often you believe your organization implements each: not at all, some of the time, most of the time, all of the time. |
| a. Managers and employees work together in planning, implementing, and evaluating comprehensive safety and health programs, policies, and practices for employees. |
| b. This company has a joint worker-management committee that addresses efforts to protect and promote worker safety and health. |
| c. In this organization, managers across all levels consistently seek employee involvement and feedback in decision making. |
| d. Employees are encouraged to voice concerns about working conditions without fear of retaliation. |
| e. Leadership, such as supervisors and managers, initiate discussions with employees to identify hazards or other concerns in the work environment. |
| 3. The following questions refer to policies, programs, and practices focused on positive working conditions. We define this term to mean the following: The organization enhances worker safety, health, and well-being with policies and practices that improve working conditions. Response categories: For each of the following policies or practices, please indicate the degree to which they are implemented at your company: not at all, somewhat, mostly, completely. |
| a. The workplace is routinely evaluated by staff trained to identify potential health and safety hazards. |
| b. Supervisors are responsible for identifying unsafe working conditions on their units. |
| c. Supervisors are responsible for correcting unsafe working conditions on their units. |
| d. This workplace provides a supportive environment for safe and healthy behaviors, such as a tobacco-free policy, healthy food options, or facilities for physical activity. |
| e. Organizational policies or programs are in place to support employees when they are dealing with personal or family issues. |
| f. Leadership, such as supervisors and managers, make sure that workers are able to take their entitled breaks during work (e.g. meal breaks). |
| g. Supervisors and managers make sure workers are able to take their earned times away from work such as sick time, vacation, and parental leave. |
| h. This organization ensures that policies to prevent harm to employees from abuse, harassment, discrimination, and violence are followed. |
| i. This organization has trainings for workers and managers across all levels to prevent harm to employees from abuse, harassment, discrimination, and violence. |
| j. This workplace provides support to employees who are returning to work after time off due to work-related health conditions. |
| k. This workplace provides support to employees who are returning to work after time off due to non-work related health conditions. |
| l. This organization takes proactive measures to make sure that the employee’s workload is reasonable, for example, that employees can usually complete their assigned job tasks within their shift. |
| m. Employees have the resources such as equipment and training do their jobs safely and well. |
| n. All employees in this organization receive paid leave, including sick leave. |
| 4. The following questions refer to comprehensive and collaborative strategies. We define this term to mean the following: Employees from across the organization work together to develop comprehensive health and safety initiatives. Response categories: For the following collaborative or comprehensive policies, programs, or practices, please indicate the degree to which your company implements each: not at all, somewhat, mostly, completely. |
| a. This company has a comprehensive approach to promote and protect worker safety and health. This includes collaborative efforts across departments as well as education and programs for individuals and policies about the work environment. |
| b. This company has a comprehensive approach to worker wellbeing. This includes collaboration across departments in efforts to prevent work-related illness and injury and to promote worker health. |
| c. This company coordinates policies, programs, and practices for worker health safety, and wellbeing across departments. |
| d. Managers are held accountable for implementing best practices to protect worker safety, health, and wellbeing, for example through their performance reviews. |
| e. Managers are given resources, such as equipment and trainings, for implementing best practices to protect and promote worker safety, health, and wellbeing. |
| f. This company prioritizes protection and promotion of worker safety and health when selecting vendors and subcontractors. |
| 5. The following questions refer to adherence. We define the term “adherence” to mean the following: The organization adheres to federal and state regulations, as well as ethical norms, that advance worker safety, health, and well-being. Response categories: For each of the following statements, please indicate the degree to which you believe your company adheres to or prioritizes standards and regulations: not at all, somewhate, mostly, completely. |
| a. This organization complies with standards for legal conduct. |
| b. In this organization, people show sincere respect for others’ ideas, values, beliefs |
| c. This workplace complies with regulations aimed at eliminating or minimizing potential exposures to recognized hazards. |
| d. This company ensures that safeguards regarding worker confidentiality, privacy and non-retaliation protections are followed. |
| e. The wages for the lowest-paid employees in this organization seem to be enough to cover basic living expenses such as housing and food. |
| 6. The following questions refer to data-driven change. We define this term to mean the following: Regular evaluation guides an organization’s priority setting, decision making, and continuous improvement of worker safety, health, and well-being initiatives. Response categories: Please indicate the degree to which your company does each of the following: not at all, somewhat,mostly, completely. |
| a. The effects of policies and programs to promote worker safety and health are measured using data from multiple sources, such as injury data, employee feedback, and absence records |
| b. Data from multiple sources on health, safety, and wellbeing are integrated and presented to leadership on a regular basis. |
| c. Evaluations of policies, programs and practices to protect and promote worker health are used to improve future efforts. |
| d. Integrated data on employee safety and health outcomes are coordinated across all relevant departments. |
Leadership Commitment, defined as: “Leadership makes worker safety, health, and well-being a clear priority for the entire organization. They drive accountability and provide the necessary resources and environment to create positive working conditions.” This construct was included in our Indicators of Integration; items in the WISH Assessment were adapted from this prior measure, as well as from other sources.1,41,51,52 Organizational leadership has been linked to an array of worker safety, health and wellbeing outcomes,53,54 including organizational safety climate,55,56 job-related wellbeing,57,58 workplace injuries,59,60 and health behaviors.61,62 This element recognizes that top management is ultimately responsible for setting priorities that define worker and worksite safety and health as part of the organization’s vision and mission.14,16 Leadership roles include providing the resources needed for implementing best practices related to worker safety, health and wellbeing; establishing accountability for implementation of relevant policies and practices; and effectively communicating these priorities through formal and informal channels.51,52
Participation, defined as: “Stakeholders at every level of an organization, including labor unions or other worker organizations if present, help plan and carry out efforts to protect and promote worker safety and health.” Many organizations have mechanisms in place to engage employees and managers in decision making and planning. These mechanisms may be used in planning and implementing integrated policies and programs, for example through joint worker-management committees that combine efforts to protect and promote worker safety, health and wellbeing.7,63,64 Employee participation in decision-making facilitates a broader organizational culture of health, safety and wellbeing. Participation also includes encouraging employees to identify and report threats to safety and health, without fear of retaliation and with the expectation that their concerns will be addressed. Items included were adapted from the Indicators of Integration1 and a self-assessment checklist from the Center for the Promotion of Health in the New England Workplace.65
Policies, programs and practices that foster supportive working conditions, defined as: “The organization enhances worker safety, health, and well-being with policies and practices that improve working conditions.” These policies, programs and practices are central to the conceptual model presented in Figure 1. Items include measures of the physical work environment and the organization of work (i.e., psychosocial factors, job tasks, demands, and resources), and are drawn from multiple sources.1,41,66–69 The focus on working conditions is based on principles of prevention articulated in a hierarchy of controls framework, which has been applied within TWH.10,70 Eliminating or reducing recognized hazards, whether in the physical work environment or the organizational environment, provides the most effective means of reducing exposure to potential for hazards on the job. Policies and processes to protect workers from physical hazards include routine inspections of the work environment, with mechanisms in place for correction of identified hazards, as well as policies that support safe and healthy behaviors, such as tobacco control policies. A supportive work organization includes safeguards against job strain, work overload, and harassment,7,71–74 as well as supports for workers as they address work-life balance, return to work after an illness or injury, and take entitled breaks, including meal breaks as well as sick and vacation time.75,76
Comprehensive and collaborative strategies, defined as: “Employees from across the organization work together to develop comprehensive health and safety initiatives.” Measures were adapted from our Indicators of Integration1 and also relied on recent recommendations from the American College of Occupational and Environmental Medicine.41 Although efforts to protect and promote worker safety and health have traditionally functioned independently, this construct acknowledges the benefits derived from collaboration across departments within an organization to protect and promote worker safety and health, both through policies about the work environment as well as education for workers. These efforts carry through into the selection of subcontractors and vendors, recognizing their impact on working conditions.
Adherence, defined as: “The organization adheres to federal and state regulations, as well as ethical norms, that advance worker safety, health, and well-being.” The importance of this construct has been recognized by multiple organizations, whose contributions and metrics were incorporated in the measures included here.7,77–79 Employers have a legal obligation to provide a safe and healthy work environment.7,68 There is also significant agreement that any system that includes health and safety metrics must include safeguards for employee confidentiality and privacy.7,41
Data-driven change, defined as: “Regular evaluation guides an organization’s priority setting, decision making, and continuous improvement of worker safety, health, and well-being initiatives.” Building health metrics into corporate reporting underscores the importance of worker health and safety as a business priority.16,80 Feedback to leadership based on evaluation and monitoring of integrated programs, policies and practices can provide a basis for ongoing quality improvement. An integrated system that reports outcomes related both to occupational health as well as health behaviors and other health and wellbeing indicators can point to shared root causes within the conditions of work.1,14
Cognitive testing results
We tested the WISH Assessment in three rounds of cognitive testing with a total of 19 participants. (See Appendix 1 for changes made to the items across the three rounds of testing.) On average, participants completed the self-administered survey in about 10–15 minutes, and the cognitive interviews took an average of 45 minutes. In the first round of cognitive testing, three participants completed a web version of the survey, and five, a paper-and-pencil version. Because we found no differences in concerns raised, the second round used only a paper survey, whereas the third included web respondents to confirm no differences in the final instrument. Changes made to the survey items were based on input from multiple respondents over the three rounds of interviews, and did not rely specifically on input from any one individual.
For items with uniform interpretation, revisions were made if respondents suggested a word or phrase that would clarify the question that investigators felt retained substantive focus. In addition, some items were dropped because they revealed multiple sources of problems, were too difficult to answer, or were identified as redundant. The first round of testing led to the removal of seven items and the modifying of 24 items. The second round of cognitive testing revealed that problems with the question wording remained with 15 questions in the context of the full survey. No additional questions were removed. These specific questions were updated and re-tested among three participants.
Throughout the cognitive testing process, we found several items to have either ambiguous terminology resulting in non-uniform or restrictive interpretation, inadequate framing of key terms and constructs, or lack of knowledge or perceived ability to provide an answer, resulting in poor information retrieval or mapping to the construct. Items measuring integration or collaboration within an organization were more often identified as problematic; to address this concern, we included a description of these constructs in the survey’s introduction to frame the survey for respondents. Although there was uniform interpretation of items asking about employee’s living wage, some respondents reported they did not have knowledge to provide an accurate answer. Most other items revealed uniform interpretation and no concerns regarding information retrieval or selecting response categories.
Looking at the items by construct, we identified particular concerns with items measuring two domains: “policies, programs, and practices that foster supportive working conditions” and “adherence” to norms and regulations. To address these concerns, we revised these items by improving the description of constructs or the terms in the respective sections’ introductions, using less ambiguous wording and integrating appropriate examples as necessary. We found commonalities across the responses in the remaining four domains, and describe our specific remediation process for each of these domains:
Leadership commitment
In round 1, we found a lack of clarity for the concept of “leadership.” For example, one respondent from the health care industry reported that: “[senior leaders and middle managers] should be distinguished and not conflated because there are several layers of management.” As a result, several respondents expressed difficulty retrieving accurate information due to level-specific answers. One respondent from a laboratory research and development company noted “[…] leadership communicate their commitment to safety and health through written policies. If you were to add supervisors – people closer to the front line – it would be different.” We addressed this concern by rewriting the introduction for this domain to clearly define “leadership commitment” and remove mention of leadership levels. However, we retained the wording “[…] such as senior leaders and middle managers, […]” in two items to reflect that organizations have channels through which commitment is communicated or enforced.
Participation
The questions for collaborative participation were largely identified as clear and uniformly interpreted. However, there was lack of clarity regarding who the key stakeholders were, particularly in the introduction. In addition, respondents reported that the introduction was too wordy and had a high literacy bar. Given these concerns and the suggestion that the use of the term “culture” was too academic, so we omitted use of this term. Some respondents expressed difficulty retrieving an appropriate answer due to this lack of clear framing of items in the introduction. We addressed this concern by rewriting the introduction to emphasize the definition of “participation” in the context of an organization’s activities that ensure worker safety and health. Feedback from round 2 found that this helped frame the item set more clearly. However, the word “encourage” in “In this organizational culture, managers encourage employees to get involved in making decisions” was identified as ambiguous. This was changed to “[…] seek employee involvement and feedback […]”.
Comprehensive and collaborative strategies
The most common feedback, expressed among several participants in multiple industries, for items in this domain was difficulty with the concept of “comprehensive,” i.e., that programming should address both prevention of illness and injury and promotion of worker health and safety. To a lesser extent, respondents also found difficulty with the “collaborative” concept. For example, some respondents including those from the hospital industry and in risk management, expressed difficulty responding to an item that included both “prevent” and “enhance,” which were perceived as “two different questions within this question.” We addressed these concerns by more clearly defining the two core constructs in a revised introduction. Moreover, we revised items to retain both “prevent and promote” while more clearly framing the question in context of collaboration. For example, the item “This company has a comprehensive approach to worker wellbeing that includes efforts to prevent work-related illness and injury as well as to enhance worker health” was revised to “This company has a comprehensive approach to worker wellbeing. This includes collaboration across departments in efforts to prevent work-related illness and injury and to promote worker health.”
Data-driven change
For this domain, we found evidence of poor cueing for the concepts of integration and coordination in the context of using data to produce organizational change. For example, several respondents from the hospital industry expressed that they did not understand what was meant by “integrated” in the context of “Summary reports on integrated policies and programs are presented to leadership on a regular basis, while also protecting employee confidentiality,” or “coordinated system” in context of “Data related to employee safety and health outcomes are integrated within a coordinated system.” Remediation focused on clarifying the context and definitions for integration and coordination. First, the introduction was revised to explicitly define data-driven change. Secondly, items were reworded to clarify integration and coordination. For example, “Summary reports on integrated policies and programs are presented to leadership on a regular basis, while also protecting employee confidentiality” was revised to “Data from multiple sources on health, safety, and wellbeing are integrated and presented to leadership on a regular basis.”
Our analyses also underscored commonalities across industries even when these issues seemed industry-specific. For example, comments from several participants suggested that a product-based mission may often dominate concerns about worker safety and health. In healthcare, this may be manifested by prioritizing patient care and safety over worker health and safety, or in other industries by a focus on production or timeline goals. Across industries, there was widespread agreement that Employee Assistant Programs was the primary resource for supporting employees dealing with personal or family issues.
DISCUSSION
Effective policies, programs and practices contribute to improvements in worker health, safety and wellbeing, as well as to enterprise outcomes such as improved employee morale, reduced absence and turnover, potentially reduced healthcare costs, and improved quality of services.2,40,81–84 This manuscript presents the Workplace Integrated Safety and Health (WISH) Assessment, designed to evaluate the extent to which organizations implement best practice recommendations for an integrated, systems approach to protecting and promoting worker safety, health and wellbeing. This instrument builds on the Indicators of Integration, previously published and validated by the Center for Work, Health and Wellbeing.1,42,43 We have expanded this tool based on the conceptual model presented in Figure 1,2 which prioritizes working conditions as determinants of worker safety, health and wellbeing. In addition, the WISH Assessment is designed to measure the extent to which an organization implements best practice recommendations. These constructs have also been used to inform in the Center’s guidelines for implementing best practice integrated approaches.8
A growing range of metrics are available to assess organizational approaches to worker safety and health. The Integrated Health & Safety Index (IHS Index), created by the American College of Occupational and Environmental Medicine in collaboration with the Underwriters Laboratories, focuses on translating health and safety into value for businesses using three dimensions: economic, environmental and social standards.41 By focusing on value, this measure has the potential to bolster the business case for health and safety.41,85 The HERO Health and Well-being Best Practices Scorecard in Collaboration with Mercer is an online tool that allows employers to receive emailed feedback on their health and well-being practices.86 Similarly, the American Heart Association’s Workplace Health Achievement Index provides an on-line self-assessment scorecard that includes comparisons with other companies.87 The health metrics designed by the Vitality Institute include both a long and short form questionnaire, both with automatic scoring.88 The Center for the Promotion of Health in the New England Workplace (CPH-NEW) has developed a tool to assess organizational readiness for implementing an integrated approach11 and is developing a tool that focuses on participatory engagement of workers, with the goal of involving workers in the process of prioritizing health and safety issues and then developing and evaluating the proposed solutions.89 Other measures of the work environment, such as the Health and Safety Executive Managements Standards Indicator Tool used in the United Kingdom, are designed to be taken by workers and so can provide detailed information on conditions as they are experienced by workers, but do not capture company-level policies and programs.90 The WISH Assessment, designed to assess a company’s use of best practices for health and safety, is substantially shorter than the IHS Index and the HERO Scorecard, does not require the compilation of metrics and does not use individual employee data. In addition, in comparison to these other measures, the WISH Assessment can be used to guide organizations towards best practices and can be easily completed by organizations that might not have the resources to use the more extensive assessments.
Next steps in the development of the WISH Assessment include validation of the instrument across multiple samples, and design and testing of a scoring system. We validated the Indicators of Integration in two samples and found it to have convergent validity and high internal consistency, and to express one unified factor even when slight changes were made to adapt the measure.42,43 We expect to follow a similar approach in validating this tool and assessing its dimensionality in large samples using factor analysis. Our goal is to design a scoring system that would be appropriate for both applied and research applications. As such, we expect the scoring algorithm to be simple enough for auto-calculation.
This tool may ultimately serve multiple purposes. As a research tool, it may provide a measure of workplace best practices that can be examined as determinants of worker safety and health outcomes. After being validated, the WISH Assessment may be used to explore organizational characteristics that may be associated with implementation of best practices. This instrument also responds to calls for practical tools for organizations implementing an integrated approach and focusing on working conditions.41 The Center used the Indicators of Integration as part of a larger assessment process in three small-to-medium manufacturing businesses to inform organizations’ priority setting and decision making around the integration of occupational safety and health and health promotion.91 In-person group discussions with key staff and executive leaders were used to rate each question on the scorecard, resulting in actionable steps based on identified gaps. Similarly, a validated WISH Assessment could be translated into a scorecard to be used to inform priority setting, decision making and to monitor changes over time in conditions of work and related health and safety outcomes. The Center has also applied the constructs defined in the WISH Assessment in its new best practice guidelines,8 which include suggestions for formal and informal policies and practices (Table 2).
Table 2.
Example Policies and Practices by each WISH construct.
| Construct | Formal Policies | Informal Practices |
|---|---|---|
| Leadership Commitment |
|
|
| Participation |
|
|
| Policies, Programs, and Practices Focused on Positive Working Conditions | Physical environment
|
Physical environment
|
| Comprehensive and Collaborative Strategies |
|
|
| Adherence |
|
|
| Data-driven Change |
|
|
McLellan D, Moore W, Nagler E, Sorensen G. 2017. Implementing an integrated approach: Weaving worker health, safety, and well-being into the fabric of your organization. Dana-Farber Cancer Institute: Boston, MA. http://centerforworkhealth.sph.harvard.edu/
These indicators describe policies, programs and practices within the control of a specific organization or enterprise, and are most likely to apply to organizations that employ approximately 100 or more employees. The cognitive testing conducted to refine the items included in the WISH Assessment included representatives from organizations in selected settings; the generalizability of these results may therefore be restricted to similar types of organizations. There remains a need for exploring how this measure may function in different industries and across organizations of varying size. Although the purpose of the WISH instrument is to provide a measure that might be broadly useful across industries, we also recognize that each industry faces particular challenges due to the nature of what they do; supplementary questions may be needed to address these industry-specific concerns. Although this measure has not yet been validated, we believe it is important to share it and to explore opportunities for collaboration with other researchers interested in testing its psychometric properties and across populations and settings, in order to further develop this tool. It will ultimately be important as well to develop mechanisms for scoring this instrument, taking account potential weighting across the domains included.
Conclusions
Growing evidence clearly documents the benefits to be derived from integrated systems approaches for protecting and promoting worker safety, health and wellbeing. Practical, validated measures of best practices that are supported by existing evidence and do not place an undue burden on respondents are needed to support systematic study and organizational change. In cognitive testing, we demonstrated that the items included in this instrument effectively assess the defined constructs. Our goal was to create a measure that will be broadly useful and valid across industry, and might contribute to understanding differences and similarities by industry. Thus, the general applicability of this instrument is a strength in that it would allow for comparisons across industries, if so desired by substantive research. We also recognize the potential benefits of industry-specific versions of this instrument which may use this broader instrument as a base set of measures while also expanding on areas that are unique to a given industry. This may help increase understanding of industry-specific health and safety challenges. The WISH Assessment holds promise as a tool that may inform organizational priority setting and guide research around causal pathways influencing implementation and outcomes related to these approaches.
Supplementary Material
Acknowledgments
Funding:
This work was supported by a grant from the National Institute for Occupational Safety and Health (U19 OH008861) for the Harvard T.H. Chan School of Public Health Center for Work, Health and Well-being.
Footnotes
Conflict of Interest noted: None
References
- 1.Sorensen G, McLellan D, Dennerlein J, Pronk N, Allen JD, Boden LI, Okechukwu CA, Hashimoto D, Stoddard A, Wagner GR. Integration of Health Protection and Health Promotion: Rationale, Indicators, and Metrics. J Occup Environ Med. 2013 Dec;55:S12–18. doi: 10.1097/JOM.0000000000000032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sorensen G, McLellan DL, Sabbath EL, Dennerlein JD, Nagler EM, Hurtado DA, Pronk NP, Wagner GR. Integrating Worksite Health Protection and Health Promotion: A Conceptual Model for Intervention and Research. Prev Med. 2016;91 doi: 10.1016/j.ypmed.2016.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jetha A, Kernan L, Kurowski A, Pro-Care Research T Conceptualizing the dynamics of workplace stress: a systems-based study of nursing aides. BMC Health Serv Res. 2017;17:12. doi: 10.1186/s12913-016-1955-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.National Institute for Occupational Safety and Health [NIOSH] What is Total Worker Health. Retrieved from https://www.cdc.gov/niosh/twh/totalhealth.html. Accessed January 20, 2017.
- 5.National Institute for Occupational Safety and Health. Essential Elements of Effective Workplace Programs and Policies for Improving Worker Health and Wellbeing. 2009 http://www.cdc.gov/niosh/worklife/essentials.html. Accessed July 7, 2010.
- 6.National Institute for Occupational Safety and Health. Fundamentals of total worker health approaches: essential elements for advancing worker safety, health, and well-being By Lee MP, Hudson H, Richards R, Chang CC, Chosewood LC, Schill AL, on behalf of the NIOSH Office for Total Worker Health. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health; Dec, 2016. [Google Scholar]
- 7.National Institute for Occupational Safety and Health. Essential elements of effective workplace programs and policies for improving worker health and wellbeing. http://www.cdc.gov/niosh/twh/essentials.html Accessed on 12/2/16. 2008.
- 8.McLellan D, Moore W, Nagler E, S G. Implementing an integrated approach: Weaving worker health, safety, and well-being into the fabric of your organization. Boston, MA: Dana-Farber Cancer Institute; 2017. [Google Scholar]
- 9.McLellan D, Harden E, Markkanen P, Sorensen G. SafeWell practice guidelines: An integrated approach to worker health Version 2.0. Boston, MA: Dana-Farber Cancer Institute; 2012. http://centerforworkhealth.sph.harvard.edu/sites/default/files/safewell_guidelines/SafeWellPracticeGuidelines_Complete.pdf. [Google Scholar]
- 10.National Institute for Occupational Safety and Health. Total Worker Health: Let’s Get Started. 2016 Retrieved from: https://www.cdc.gov/niosh/twh/letsgetstarted.html.
- 11.University of Massachusetts Lowell. Healthy Workplace Participatory Program. https://www.uml.edu/Research/CPH-NEW/Healthy-Work-Participatory-Program/. Accessed August 16, 2017.
- 12.World Health Organization. World Health Organization. Healthy workplaces: a model for action. 2013 Available at: http://www.who.int/occupational_health/publications/healthy_workplaces_model.pdf. Accessed April 23, 2013.
- 13.University of California BLLOHP. The Whole Worker: Guidelines for Integrating Occupational Health and Safety with Workplace Wellness Programs. 2016 http://lohp.org/whole-worker/
- 14.Institute of Medicine Committee to Assess Worksite Preventive Health Program Needs for NASA Employees FaNB. Integrating employee health: A model program for NASA. Washington, DC: Institute of Medicine, National Academies Press; 2005. [Google Scholar]
- 15.International Labour Office. ILO-OSH 2001Guidelines on occupational safety and health management systems. Geneva, Switzerland: ILO; 2001. http://www.ilo.org/public/libdoc/ilo/2001/101B09_287_engl.pdf. [Google Scholar]
- 16.Quelch JA, Boudreau EC. Building a Culture of Health: A New Imperative for Business. Switzerland: Springer Nature; 2014. [Google Scholar]
- 17.Benders J, Bleijerveld H, Schouteten R. Continuous improvement, burnout and job engagement: a study in a Dutch nursing department. Int J Health Plann Manage. 2016 doi: 10.1002/hpm.2355. [DOI] [PubMed] [Google Scholar]
- 18.von Thiele Schwarz U, Augustsson H, Hasson H, Stenfors-Hayes T. Promoting employee health by integrating health protection, health promotion, and continuous improvement: a longitudinal quasi-experimental intervention study. J Occup Environ Med. 2015;57:217–225. doi: 10.1097/JOM.0000000000000344. [DOI] [PubMed] [Google Scholar]
- 19.American Society of Safety Engineers. American National Standard for Occupational Health and Safety Management Systems (ANSI Z10-2012) 2012 http://www.asse.org/assets/1/7/z10_tech_brief_2012_revised.pdf.
- 20.Cousins R, MacKay CJ, Clarke SD, Kelly C, Kelly PJ, McCaig RH. Management Standards’ work-related stress in the UK: practical development. Work & Stress. 2004;18:113–136. [Google Scholar]
- 21.Shaw WS, Robertson MM, McLellan RK, Verma S, Pransky G. A controlled case study of supervisor training to optimize response to injury in the food processing industry. Work. 2006;26:107–114. [PubMed] [Google Scholar]
- 22.Shaw WS, Robertson MM, Pransky G, McLellan RK. Employee perspectives on the role of supervisors to prevent workplace disability after injuries. J Occup Rehabil. 2003;13:129–142. doi: 10.1023/a:1024997000505. [DOI] [PubMed] [Google Scholar]
- 23.Hlobil H, Uegaki K, Staal JB, de Bruyne MC, Smid T, van Mechelen W. Substantial sick-leave costs savings due to a graded activity intervention for workers with non-specific sub-acute low back pain. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2007;16:919–924. doi: 10.1007/s00586-006-0283-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Robertson MM, Ciriello VM, Garabet AM. Office ergonomics training and a sit-stand workstation: effects on musculoskeletal and visual symptoms and performance of office workers. Appl Ergon. 2013;44:73–85. doi: 10.1016/j.apergo.2012.05.001. [DOI] [PubMed] [Google Scholar]
- 25.Pronk NP, Katz AS, Lowry M, Payfer JR. Reducing occupational sitting time and improving worker health: the Take-a-Stand Project, 2011. Prev Chronic Dis. 2012;9:E154. doi: 10.5888/pcd9.110323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tsutsumi A, Nagami M, Yoshikawa T, Kogi K, Kawakami N. Participatory intervention for workplace improvements on mental health and job performance among blue-collar workers: a cluster randomized controlled trial. J Occup Environ Med. 2009;51:554–563. doi: 10.1097/JOM.0b013e3181a24d28. [DOI] [PubMed] [Google Scholar]
- 27.LaMontagne AD, Youngstrom RA, Lewiton M, Stoddard AM, McLellan D, Wallace LM, Barbeau E, Sorensen G. Assessing and intervening on OSH programs: Effectiveness evaluation of the WellWorks-2 intervention in fifteen manufacturing worksites. Occup Environ Med. 2004;61:651–660. doi: 10.1136/oem.2003.011718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Goetzel RZ, Guindon AM, Turshen IJ, Ozminkowski RJ. Health and productivity management: establishing key performance measures, benchmarks, and best practices. J Occup Environ Med. 2001;43:10–17. doi: 10.1097/00043764-200101000-00003. [DOI] [PubMed] [Google Scholar]
- 29.Sorensen G, Barbeau E, Stoddard A, Hunt MK, Kaphingst K, Wallace L. Promoting behavior change among working-class, multi-ethnic workers: Results of the Healthy Directions Small Business Study. Am J Public Health. 2005;95:1389–1395. doi: 10.2105/AJPH.2004.038745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sorensen G, Stoddard A, LaMontagne A, Emmons K, Hunt M, Youngstrom R, McLellan D, Christiani D. A comprehensive worksite cancer prevention intervention: Behavior change results from a randomized controlled trial in manufacturing worksites (United States) Cancer Cause Control. 2002;13:493–502. doi: 10.1023/a:1016385001695. [DOI] [PubMed] [Google Scholar]
- 31.Maes S, Verhoeven C, Kittel F, Scholten H. Effects of a Dutch worksite wellness-health program: The Brabantia project. American Journal of Public Health. 1998;88:1037–1041. doi: 10.2105/ajph.88.7.1037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Sorensen G, Stoddard A, Hunt MK, Hebert JR, Ockene JK, Avrunin JS, Himmelstein J, Hammond SK. The effects of a health promotion-health protection intervention on behavior change: the WellWorks Study. Am J Public Health. 1998;88:1685–1690. doi: 10.2105/ajph.88.11.1685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Sorensen G, Barbeau EM, Stoddard AM, Hunt MK, Goldman R, Smith A, Brennan AA, Wallace L. Tools for health: the efficacy of a tailored intervention targeted for construction laborers. Cancer causes & control : CCC. 2007;18:51–59. doi: 10.1007/s10552-006-0076-9. [DOI] [PubMed] [Google Scholar]
- 34.Okechukwu CA, Krieger N, Sorensen G, Li Y, Barbeau EM. MassBuilt: effectiveness of an apprenticeship site-based smoking cessation intervention for unionized building trades workers. Cancer Causes Control. 2009;20:887–894. doi: 10.1007/s10552-009-9324-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Olson R, Anger WK, Elliot DL, Wipfli B, Gray M. A new health promotion model for lone workers: results of the Safety & Health Involvement For Truckers (SHIFT) pilot study. J Occup Environ Med. 2009;51:1233–1246. doi: 10.1097/JOM.0b013e3181c1dc7a. [DOI] [PubMed] [Google Scholar]
- 36.Elliot DL, Goldberg L, Kuehl KS, Moe EL, Breger RK, Pickering MA. The PHLAME (Promoting Healthy Lifestyles: Alternative Models’ Effects) firefighter study: outcomes of two models of behavior change. J Occup Environ Med. 2007;49:204–213. doi: 10.1097/JOM.0b013e3180329a8d. [DOI] [PubMed] [Google Scholar]
- 37.Bertera RL. The effects of workplace health promotion on absenteeism and employment costs in a large industrial population. Am J Public Health. 1990;80:1101–1105. doi: 10.2105/ajph.80.9.1101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Bertera RL. Behavioral risk factor and illness day changes with workplace health promotion: two-year results. Am J Health Promot. 1993;7:365–373. doi: 10.4278/0890-1171-7.5.365. [DOI] [PubMed] [Google Scholar]
- 39.Hunt MK, Lederman R, Stoddard AM, LaMontagne AD, McLellan D, Combe C, Barbeau E, Sorensen G. Process evaluation of an integrated health promotion/occupational health model in WellWorks-2. Health Educ Behav. 2005;32:10–26. doi: 10.1177/1090198104264216. [DOI] [PubMed] [Google Scholar]
- 40.Pronk NP. Integrated worker health protection and promotion programs: overview and perspectives on health and economic outcomes. J Occup Environ Med. 2013;55:S30–37. doi: 10.1097/JOM.0000000000000031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Loeppke RR, Hohn T, Baase C, Bunn WB, Burton WN, Eisenberg BS, Ennis T, Fabius R, Hawkins RJ, Hudson TW, Hymel PA, Konicki D, Larson P, McLellan RK, Roberts MA, Usrey C, Wallace JA, Yarborough CM, Siuba J. Integrating health and safety in the workplace: how closely aligning health and safety strategies can yield measurable benefits. J Occup Environ Med. 2015;57:585–597. doi: 10.1097/JOM.0000000000000467. [DOI] [PubMed] [Google Scholar]
- 42.Williams J, Nelson C, Caban-Martinez AJ, Katz JN, Wagner GR, Pronk NP, Sorensen G, McLellan DL. Validation of a New Metric for Assessing the Integration of Health Protection and Health Promotion in a Sample of Small- and Medium-Sized Employer Groups. J Occup Environ Med. 2015;57:1017–1021. doi: 10.1097/JOM.0000000000000521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Williams JA, Schult TM, Nelson CC, Caban-Martinez AJ, Katz JN, Wagner GR, Pronk NP, Sorensen G, McLellan DL. Validation and Dimensionality of the Integration of Health Protection and Health Promotion Score: Evidence From the PULSE Small Business and VA Medical Center Surveys. J Occup Environ Med. 2016;58:499–504. doi: 10.1097/JOM.0000000000000732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Williams J. The Validation of a New Metric for Assessing Approaches Integrating Health Protection and Health Promotion. Abstract presented at the 1st International Symposium to Advance TOTAL WORKER HEALTH®; October 2014. [Google Scholar]
- 45.Worksafe Australia. Workplace injury and disease recording standard. Sydney: Standards Australia; 1990. [Google Scholar]
- 46.Harvard TH. Chan School of Public Health Center for Work Health and Well-being. http://centerforworkhealth.sph.harvard.edu/. Accessed December 2, 2015.
- 47.Hsu C-C, Sandford BA. The Delphi Technique: Making Sense of Consensus. Practical Assessment, Research and Evaluation. 2007;12(10):1–8. http://pareonline.net/pdf/v12n10.pdf. [Google Scholar]
- 48.National Institute for Occupational Safety and Health. NIOSH Centers of Excellence for Total Worker Health®. 2016 Available at: https://www.cdc.gov/niosh/twh/centers.html.
- 49.Willis GB. Cognitive interviewing A tool for improving questionnaire design. Thousand Oaks, CA: Sage Publications; 2005. [Google Scholar]
- 50.Willis GB, Artino AR., Jr What Do Our Respondents Think We’re Asking? Using Cognitive Interviewing to Improve Medical Education Surveys. J Grad Med Educ. 2013;5:353–356. doi: 10.4300/JGME-D-13-00154.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Centers for Disease Control and Prevention. Workplace Health Program Development Checklist. 2011 www.cdc.gov/workplacehealthpromotion/pdfs/WHPChecklist.pdf.
- 52.Center for Construction Research and Training (CPWR) Safety Culture and Climate in Construction: Bridging the Gap Between Research and Practice Workshop Report. 2014 http://www.cpwr.com/sites/default/files/publications/CPWR_Safety_Culture_Final_Report_0.pdf Accessed 3/1/2017.
- 53.Kelloway EK, Barling J. Leadership development as an intervention in occupational health psychology. Work & Stress. 2010;24:260–279. [Google Scholar]
- 54.Nyberg A, Alfredsson L, Theorell T, Westerlund H, Vahtera J, Kivimaki M. Managerial leadership and ischaemic heart disease among employees: the Swedish WOLF study. Occup Environ Med. 2009;66:51–55. doi: 10.1136/oem.2008.039362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Zohar D. Modifying supervisory practices to improve subunit safety: a leadership-based intervention model. J Appl Psychol. 2002;87:156–163. doi: 10.1037/0021-9010.87.1.156. [DOI] [PubMed] [Google Scholar]
- 56.Zohar D. The effects of leadership dimensions, safety climate, and assigned priorities on minor injuries in work groups. Journal of Organizational Behavior J Organ Behav. 2002;23:75–92. [Google Scholar]
- 57.Kuoppala J, Lamminpaa A, Liira J, Vainio H. Leadership, job well-being, and health effects–a systematic review and a meta-analysis. J Occup Environ Med. 2008;50:904–915. doi: 10.1097/JOM.0b013e31817e918d. [DOI] [PubMed] [Google Scholar]
- 58.Skakon J, Nielsen K, Borg V, Guzman J. Are leaders’ wellbeing, behaviours and style associated with the affective wellbeing of their employees? A systematic review of three decades of research. Work & Stress. 2010;24:147–139. [Google Scholar]
- 59.Kelloway EK, Mullen J, Francis L. Divergent effects of transformational and passive leadership on employee safety. J Occup Health Psychol. 2006;11:76–86. doi: 10.1037/1076-8998.11.1.76. [DOI] [PubMed] [Google Scholar]
- 60.Mullen JE, Kelloway EK. Safety leadership: A longitudinal study of the effects of transformational leadership on safety outcomes. J Occup Organ Psychol. 2009;82:253–272. [Google Scholar]
- 61.Bamberger PA, Bacharach SB. Abusive supervision and subordinate problem drinking: Taking resistance, stress and subordinate personality into account Human Relations. 2006;59:723–752. [Google Scholar]
- 62.Whiteman JA, Snyder DA, Ragland JJ. The value of leadership in implementing and maintaining a successful health promotion program in the Naval Surface Force, U.S. Pacific Fleet. Am J Health Promot. 2001;15:437–440, iii. doi: 10.4278/0890-1171-15.6.437. [DOI] [PubMed] [Google Scholar]
- 63.Punnett L, Cherniack M, Henning R, Morse T, Faghri P. A conceptual framework for integrating workplace health promotion and occupational ergonomics programs. Public Health Rep. 2009;124(Suppl 1):16–25. doi: 10.1177/00333549091244S103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Rasmussen K, Glasscock DJ, Hansen ON, Carstensen O, Jepsen JF, Nielsen KJ. Worker participation in change processes in a Danish industrial setting. Am J Ind Med. 2006;49:767–779. doi: 10.1002/ajim.20350. [DOI] [PubMed] [Google Scholar]
- 65.Center for the Promotion of Health in the New England Workplace. Readiness and Resource Self-Assessment Checklist. https://www.uml.edu/docs/Readiness%20for%20Change%20Self%20Rating%20Checklist%2010.7.15_tcm18–206143.pdf Accessed on 12/2/16. 2015. Accessed December 2, 2016.
- 66.Occupational Safety and Health Administration. OSHA Fact Sheet: Effective Workplace Safety and Health Management Systems. https://www.osha.gov/Publications/safety-health-management-systems.pdf. Accessed on 12/2/16. 2008. Accessed February 1, 2017.
- 67.Vitality Institute. The Vitality Health Metrics Scorecard. 2016 http://thevitalityinstitute.org/projects/health-metrics-reporting/ Accessed on 12/2/16.
- 68.State of California DoIR. Guide to Developing Your Workplace Injury and Illness Prevention Program with checklists for self-inspection CS-1 revised August 2005 - Cal/OSHA Consultation Service. 2005 http://www.dir.ca.gov/dosh/dosh_publications/iipp.html. Accessed December 2, 2016.
- 69.Collins J. Assembling the Pieces: An Implementation Guide to the National Standard for Psychological Health and Safety in the Workplace. CSA Group. 2014 http://www.csagroup.org/documents/codes-and-standards/publications/SPE-Z1003-Guidebook.pdf. Accessed December 2, 2016.
- 70.Weeks JL, Wagner GR, Rest KM, Levy BS. A Public Health Approach to Preventing Occupational Diseases and Injuries. In: Levy BS, Wagner GR, Rest KM, Weeks JL, editors. Preventing Occupational Disease and Injury. Washington DC: American Public Health Association; 2005. pp. 11–17. [Google Scholar]
- 71.Karasek R, Theorell T. Healthy work: Stress, productivity, and the reconstruction of working life. New York, NY: Basic Books; 1990. [Google Scholar]
- 72.Tullar JM, Brewer S, Amick BC, 3rd, Irvin E, Mahood Q, Pompeii LA, Wang A, Van Eerd D, Gimeno D, Evanoff B. Occupational safety and health interventions to reduce musculoskeletal symptoms in the health care sector. J Occup Rehabil. 2010;20:199–219. doi: 10.1007/s10926-010-9231-y. [DOI] [PubMed] [Google Scholar]
- 73.Choi B, Schnall PL, Yang H, Dobson M, Landsbergis P, Israel L, Karasek R, Baker D. Psychosocial working conditions and active leisure-time physical activity in middle-aged us workers. Int J Occup Med Environ Health. 2010;23:239–253. doi: 10.2478/v10001-010-0029-0. [DOI] [PubMed] [Google Scholar]
- 74.Sabbath EL, Hurtado DA, Okechukwu CA, Tamers SL, Nelson C, Kim SS, Wagner G, Sorensen G. Occupational injury among hospital patient-care workers: What is the association with workplace verbal abuse? Am J Ind Med. 2014;57:222–232. doi: 10.1002/ajim.22271. [DOI] [PubMed] [Google Scholar]
- 75.Hammer LB, Sauter S. Total worker health and work-life stress. J Occup Environ Med. 2013;55:S25–29. doi: 10.1097/JOM.0000000000000043. [DOI] [PubMed] [Google Scholar]
- 76.Kelly E, Moen P, Oakes M, Okechukwu C, Davis K, Kossek E, Hanson G, Mierzwa F, Casper LM. Changing work and work-family conflict: Evidence from the Work, Family, and Health Network. Am Sociol Rev. 2014;79:485–516. doi: 10.1177/0003122414531435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Starbucks Coffee Company. Business Ethics and Compliance: Standards of Business Conduct. SKU 1111064 SOBC_ENG_v2.1_05_11.2011. [Google Scholar]
- 78.Campbell C, Kramer A, Woolman K, Staecker E, Visker J, Cox C. Effects of a brief pilot sexual harassment prevention workshop on employees’ knowledge. Workplace health & safety. 2013;61:425–428. doi: 10.1177/216507991306101002. [DOI] [PubMed] [Google Scholar]
- 79.Pronk NP. Best practice design principles of worksite health and wellness programs. ACSM’s Health & Fitness Journal. 2014;18:42–46. [Google Scholar]
- 80.Tryon K, Bolnick H, Pomeranz J, Pronk N, Y D. Investing in Prevention: A National Imperative. The Vitality Institute; 2014. Available at: http://thevitalityinstitute.org/site/wp-content/uploads/2014/06/Vitality_Recommendations2014.pdf. Accessed August 17, 2017. [Google Scholar]
- 81.Anger WK, Elliot DL, Bodner T, Olson R, Rohlman DS, Truxillo DM, Kuehl KS, Hammer L, Montgomery D. Effectiveness of Total Worker Health interventions. J Occup Health Psychol. 2015;20:226–247. doi: 10.1037/a0038340. [DOI] [PubMed] [Google Scholar]
- 82.Sorensen G, Landsbergis P, Hammer L, Amick B, Linnan L, Yancey A, Welch L, Goetzel R, Flannery K, Pratt C. Preventing Chronic Disease At the Workplace: A Workshop Report and Recommendations. Am J Public Health. 2011;101(Suppl 1):S196–207. doi: 10.2105/AJPH.2010.300075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Lamontagne AD, Keegel T, Louie AM, Ostry A, Landsbergis PA. A systematic review of the job-stress intervention evaluation literature, 1990–2005. Int J Occup Environ Health. 2007;13:268–280. doi: 10.1179/oeh.2007.13.3.268. [DOI] [PubMed] [Google Scholar]
- 84.Feltner C, Peterson K, Palmieri Weber R, Cluff L, Coker-Schwimmer E, Viswanathan M, Lohr KN. The Effectiveness of Total Worker Health Interventions: A Systematic Review for a National Institutes of Health Pathways to Prevention Workshop. Ann Intern Med. 2016;165:262–269. doi: 10.7326/M16-0626. [DOI] [PubMed] [Google Scholar]
- 85.Pronk NP. Integrated Worker Health Protection and Promotion Programs: Overview and Perspectives on Health and Economic Outcomes. Journal of occupational and environmental medicine/American College of Occupational and Environmental Medicine. 2013;55:S30–S37. doi: 10.1097/JOM.0000000000000031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Organization; HER, Mercer. The Hero Health and Well-being Best Practices Scorecard in Collaboration with Mercer Version 4. 2016 http://hero-health.org/wp-content/uploads/2016/02/HERO-Scorecard_US_form.pdf.
- 87.American Heart Association. Workplace Health Achievement Index. 2017 http://www.heart.org/HEARTORG/HealthyLiving/WorkplaceHealth/What-Is-the-Workplace-Health-Achievement-Index_UCM_481057_Article.jsp#.WbwU9oq1vq0.
- 88.Vitality Insitute. Health Metrics Reporting. 2014 http://thevitalityinstitute.org/projects/health-metrics-reporting/
- 89.Cavallari J, N S, Henning R, Fitts M, Cherniack M, Punnet L. Measuring Integration in Total Worker Health: The Center for the Promotion of Health in the New England Workplace Participatory Framework. Paper presented at: Work, Stress, and Health; Minneapolis, MN. 2017. [Google Scholar]
- 90.Executive; HaS. What are the Management Standards? 2017 http://www.hse.gov.uk/stress/standards/index.htm.
- 91.Pronk N, McLellan D, McGrail M, Olson SK, Z M, Katz JN, Wagner GR, Sorensen G. Measurement Tools for Integrated Worker Health Protection and Promotion: Lessons Learned from the SafeWell Project. J Occup Environ Med. 2016;58:651–658. doi: 10.1097/JOM.0000000000000752. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.