

Abstract
Background
Reducing the reading time of capsule endoscopy films is of high priority for gastroenterologists. We report a prospective multicenter evaluation of an “express view” reading mode (Intromedic capsule system).
Methods
Eighty-three patients with obscure gastrointestinal bleeding were prospectively included in 10 centers. All patients underwent small-bowel capsule endoscopy (Intromedic, Seoul, Republic of Korea). Films were read in standard mode, then a second reading was performed in express view mode at a second center. For each lesion, the precise location, nature, and relevance were collected. A consensus reading and review were done by three experts, and considered to be the gold standard.
Results
The mean reading time of capsule films was 39.7 minutes (11 – 180 minutes) and 19.7 minutes (4 – 40 minutes) by standard and express view mode, respectively ( P < 1 × 10 – 4 ). The consensus review identified a significant lesion in 44/83 patients (53.0 %). Standard reading and express view reading had a 93.3 % and 82.2 % sensitivity, respectively (NS). Consensus review identified 70 significant images from which standard reading and express view reading detected 58 (82.9 %) and 55 (78.6 %), respectively. The informatics algorithm detected 66/70 images (94.3 %) thus missing four small-bowel angiodysplasia.
Conclusion
The express view algorithm allows an important shortening of Intromedic capsule film reading time with a high sensitivity.
Introduction
Capsule endoscopy is the first choice small-bowel examination for most gastroenterologists worldwide in patients presenting with obscure (overt or occult) gastrointestinal bleeding (OGIB), because of simple use, low risk, and high sensitivity compared to all other small-bowel imaging modalities 1 2 . Capsule endoscopy is a very sensitive examination for the detection of small-bowel lesions, as assessed by long-term follow-up of patients after negative capsule endoscopy: only 10 % of patients present with ongoing bleeding related to a missed small-bowel lesion 3 . The main limitation of capsule endoscopy is the substantial time needed for capsule reading by highly qualified medical personnel. Most series 4 5 6 , report a mean reading time of 50 to 60 minutes. In addition, the focus and attention to detail that are necessary to efficiently read a film are difficult to maintain during the whole reading 4 7 . For this reason, attempts have been made to transfer capsule reading to nurses or other similarly qualified personnel, with relatively satisfying results 8 9 . Informatics approaches to solving the reading time dilemma have also been proposed, with variable results. This approach needs clinical evaluation and validation 10 11 .
Nowadays, very few informatics algorithms for accelerated reading have been validated, although almost all capsule systems propose such informatics tools. This includes the SBI (small-bowel blood indicator, Given Imaging/Medtronic), that proved to be of poor sensitivity and specificity 12 13 , and the Quick-view algorithm that was validated through a retrospective blinded double-reading trial published in 2012 14 . Since that study, very few evaluations of informatics reading algorithms have been published, and no prospective evaluation 15 . Developing such complex algorithms requires specifically large image databases that have been produced through international collaborations 16 . The Intromedic company recently proposed a new informatics algorithm named “express view” to reduce the reading time of small-bowel capsule films by skipping repetitive and non-significant small-bowel images on the film. To the best of our knowledge, this algorithm has never been evaluated. We thus performed a prospective, multicenter evaluation of the express view algorithm in unselected films from 10 French gastroenterology centers, with the aim of evaluating the sensitivity and specificity of an express view reading compared to the previous standard reading of the capsule film.
Materials and methods
Small-bowel capsule endoscopy and population
The study includes 83 small-bowel capsule films from 83 consecutive unselected patients included prospectively in one of 10 experienced French centers belonging to the French Society of Digestive Endoscopy (SFED). The indication for capsule endoscopy was obscure (overt or occult) bleeding in all cases, with negative bidirectional endoscopy in all cases. The capsule endoscopy (Mirocam, Intromedic, Seoul, Republic of Korea) procedure was performed in each center following the usual local procedures including preparation and prokinetics in some centers: as the main objective of the study was the reading time, and as each capsule film was read in both standard mode and express view mode, being its own control, differences in preparation quality or small-bowel transit time could not modify the results. Characteristics of the Intromedic capsule system are: a resolution of 320 × 320, a field of view of 170° and a frame rate of 3 images per second. Each capsule film was read initially by one experienced local reader (standard or initial reading). Information on patient characteristics, indication for capsule, findings according to the SFED classification of relevance 17 , and reading time, were recorded prospectively. All observed lesions were described in the reports in terms of nature, location, and relevance. All 83 films were registered on the same hard disk, and then dispatched to the different centers for express view analysis.
Express view reading
For each center, one reader was in charge of capsule video analysis in express view mode, and was blinded to any information about previous diagnosis. This reader was thus in charge of the analysis of films from one other center. The readers were asked to read only in express view mode and to select all pathological images, identify their relevance, and define a final diagnosis corresponding to the most significant image in the entire (including stomach and colon) capsule film. Readers were allowed to choose their preferred image reading frame. The results of the express view reading and of the initial reading were saved on a pro forma.
Interpretation of the results (see flow chart, Fig.1 )
Fig. 1.
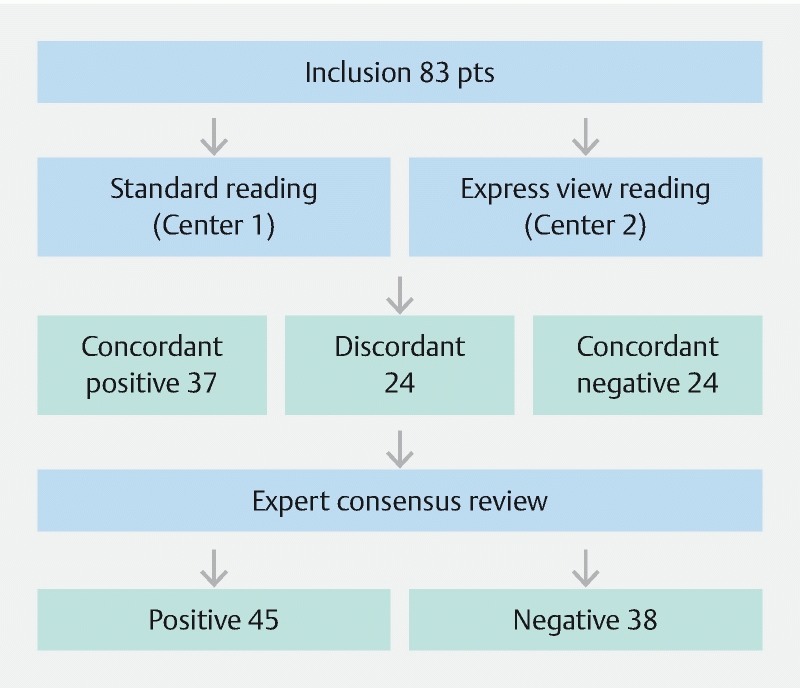
Study flow chart showing the results of standard reading and express view reading, then final results after expert consensus review.
A comparison was made for each case between the results of the initial reading and that of the express view reading. In cases with concordant (positive or negative) diagnosis between the standard and express view reading, no complementary reading was performed. In case of a discordant final diagnosis and/or different lesions observed, a secondary expert review was performed by three readers (JCS, PJ, GR), all three having experience of more than 500 capsule readings, and a consensus decision was made. The result of this consensus review was considered to be the gold standard result and compared with the results of the standard reading and of the express view reading. We performed a per patient analysis based on the main diagnosis obtained by capsule endoscopy for each patient (i. e. small-bowel tumor, angiodysplasia, ulceration, etc.). We performed a per lesion analysis by including all significant (P1 or P2) lesions according to the SFED classification 17 .
Statistical analysis
Sensitivity values were presented as a percentage (95 % confidence interval). McNemar’s test was used to compare the express view and standard reading sensitivity and specificity results using the expert review as a gold standard. We used SPSS 12.0 version software (SPSS Inc, Chicago, IL, United States) in a Windows XP (Microsoft, Seattle, WA, United States) environment. A P value < 0.05 was considered to be statistically significant.
Results
Between February 2013 and February 2016, 83 patients with obscure/overt digestive bleeding were included (43 women, mean age 62.5 years, range 21 – 85). The 83 CE films were read in express view mode without technical issue, with a mean reading time of 18.3 minutes (range 3 – 41 minutes) versus 37.7 minutes (range 11 – 180 minutes, P < 0.0001, Student’s bilateral t test) for standard reading mode. Evaluation of landmarks in normal and express view reading modes yielded comparable mean gastric and small-bowel transit times: 50.1 and 223.1 minutes (normal mode) and 49.6 and 210.4 minutes (express view mode). The algorithm selection allowed a mean reduction in the number of images from a mean of 80 596 images (range 123 323 – 52 248) to a mean of 22 087 (5196 – 43 017) thus resulting in a mean 70 % reduction in the number of images in one complete capsule film.
Per patient analysis
From the 83 patients prospectively included, 45 (54.2 %) had a main diagnosis after consensus review of the whole series ( Fig. 1 ). The final diagnosis was angiodysplasia in 29 cases, erosion-ulcerations in 10 cases, ongoing bleeding without evidenced diagnosis in four cases and tumor in two cases. Standard reading identified 42 (sensitivity 93.3 %) of these main diagnoses and express view reading identified 37 (82.2 %) of these diagnoses ( Table 1 ). Standard reading missed one P2 gastric tumor, one P2 cecal ongoing bleeding, and one P1 gastritis. Express view reading missed four cases of small-bowel angiodysplasia (including two cases where the image was skipped by the express view algorithm, Fig. 2 ), 1 jejunal ulcer ( Fig. 3 EV1), one P2 duodenal ulcer, and 2 gastric lesions (P1 gastritis and P2 ulcer). Thus, six out of eight main diagnoses missed at express view reading were present on the express view film but missed by the readers, and two were missed because of the informatics selection.
Table 1. Sensitivity of initial reading and express view reading (95 % confidence interval) in a per patient and per lesion analysis.
| Normal reading | Express view reading | P value | |
| Per patient sensitivity | 93.3 % (0.88 – 0.98) | 82.2 % (0.74 – 0.90) | 0.388 |
| Per lesion sensitivity | 69.0 % (0.74 – 0.92) | 77.2 % (0.69 – 0.88) | 0.430 |
Fig. 2 .
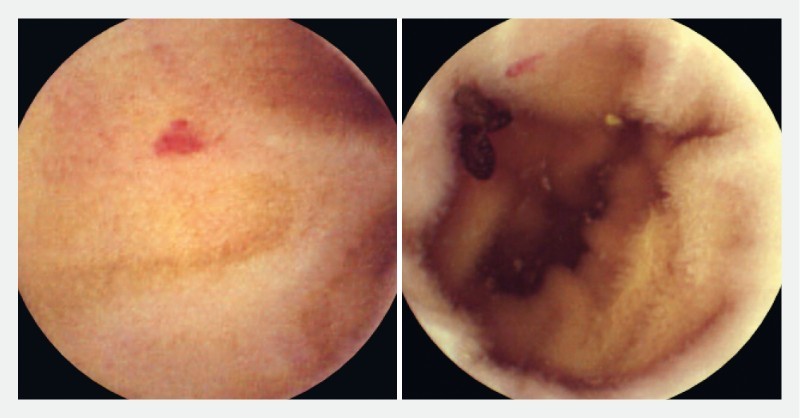
Two P2 and P1 angiodysplasias skipped by the express view algorithm, thus absent from the express view film.
Fig. 3 .
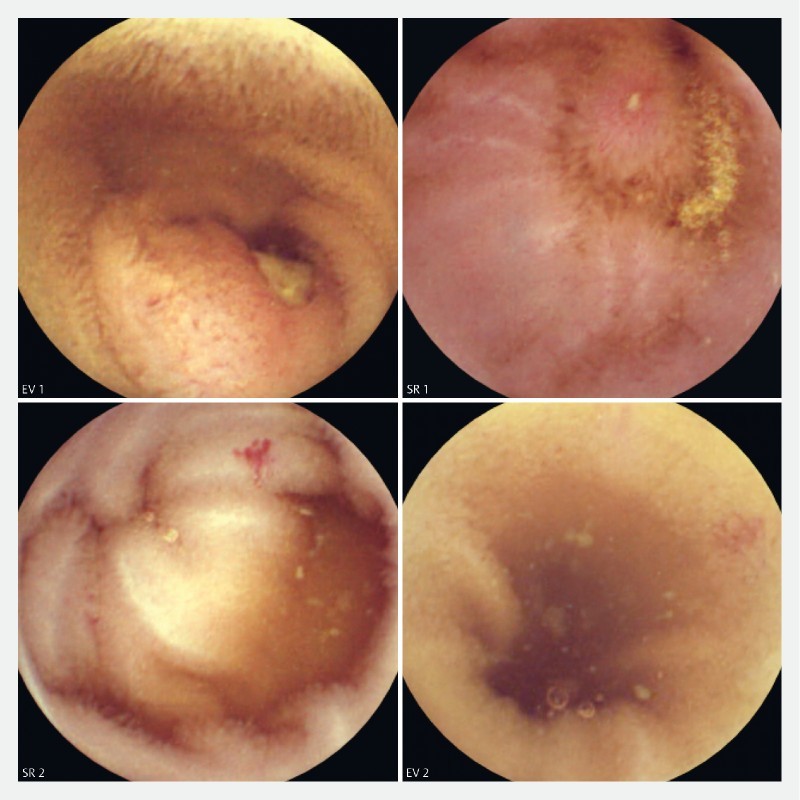
Different small-bowel diagnoses missed by the readers in express view (EV) or standard reading (SR) mode but present on the corresponding films. EV1: P2 jejunal ulceration; SR1: Aphthous P1 ulceration in the ileum; SR2: P2 angiodysplasia; EV2: P1 angiodysplasia.
Per lesion analysis
Seventy significant (P1 or P2) images were identified by the readers according to the expert review final evaluation. Standard reading (normal mode) identified 58 from these 70 images (82.9 %), compared to 55 images identified in express view mode (78.6 %, P = 0.388). On the express view film, 66/70 images were present (sensitivity of the algorithm 94.3 %). Thus, at initial reading, readers missed 12 images present on the entire capsule films (17.1 %) and express view readers missed 11 images present on the express view-selected capsule film (16.6 %, Fig. 3 ). The informatics algorithm skipped four significant images from the initial film that were all small-bowel angiodysplasia, classified as highly relevant in two cases and of uncertain/intermediate relevance in two cases. Fig. 2 shows two angiodysplasias skipped by the informatics algorithm.
Discussion
There is a high expectation of efficient algorithms allowing reading time reduction for small-bowel capsule endoscopy films, as the mean reading time proved to be significant, from 30 to 60 minutes 4 17 18 . Interestingly, numerous algorithms exist for different capsule endoscopy devices, but very few prospective blinded evaluations have been performed at the present time. One retrospective blinded multicentric evaluation validated the quick-view algorithm of the Given Imaging (now Medtronic) small-bowel capsule endoscopy device 14 . That study showed a 93 % sensitivity of the informatics algorithm for significant (P1 or P2) lesions in a setting of obscure bleeding. The present study shows that the express view informatics algorithm developed for the Intromedic device and software has a 94.2 % sensitivity for the detection of significant lesions. This sensitivity for significant lesions should be the main objective of any prospective evaluation of these algorithms, as the major consideration from the patient’s point of view is that no important diagnostic should be missed (skipped) by the selection algorithm. Thus, the express view algorithm, like the quick-view algorithm previously, seems to be a very efficient and safe selection algorithm for clinical use, although confirmative studies are needed.
The secondary end point of such reading studies is the sensitivity of the reading. It is important, however, to differentiate this sensitivity from that of the informatics algorithm, as this is “operator-dependent” and represents the efficacy of the reader rather than the efficacy of the informatics algorithm or of the device itself. In the present study, the sensitivity of reading was limited in express view mode, although not significantly different from that of the standard reading. This represents real life practice: we included readers from university hospitals, general hospitals, and private practice. Although all centers had a large experience with capsule reading, differences of reading interpretation is a characteristic of multicenter studies that we observed in numerous previous studies 14 19 20 . On the other hand, image selection by an informatics algorithm may reduce the number of consecutive images of an angiodysplasia, as an example, on the express view film compared to the non-contrast film, which occurred in a few cases (not shown) in this study. However, this did not explain the lower per patient sensitivity of express mode reading in this study, as, in contrast, the per lesion sensitivity of express view reading was slightly higher (but not significantly) compared to the per lesion sensitivity of normal reading. In fact, this may actually represent the real life variability of multicenter capsule reading and argues in favor of an evolution toward automatic reading and selection by computer: this is certainly part of the future of capsule endoscopy. In this setting, the main result of such a study is the theoretical sensitivity of the informatics algorithm. The use of an expert review, considered to be the final “gold standard”, may be criticized as it represents some bias of expert judgment compared to the “real life” reading. However, we showed in previous studies that the subjectivity of capsule reading is a constant feature of multicenter studies, with a significant proportion of false positive/false negative images responsible for confusing results when evaluating the sensitivity of reading, and especially when evaluating an informatics algorithm for image selection 7 14 21 .
Is the express view algorithm now ready for clinical use? The theoretical sensitivity of more than 94 % is rather reassuring, although confirmation by an independent study would be helpful. In this setting, one could use the express view mode to make a first reading, that could be considered to be sufficient in those patients with significant findings at the end of this first reading. In those patients with a negative express view reading, a reading of the “complementary film” could be done, whenever available on the Intromedic software. On the other hand, simple patient surveillance followed by a complete reading in those with recurrent bleeding is an alternative. This approach may yield precious time saving for gastroenterologists.
Footnotes
Competing interests J.C. Saurin and G. Rhami are occasional consultants for Medtronic, Capsovision, and Intromedic.
References
- 1.Marmo R, Rotondano G, Piscopo R et al. Meta-analysis: capsule enteroscopy vs. conventional modalities in diagnosis of small bowel diseases. Aliment Pharmacol Ther. 2005;22:595–604. doi: 10.1111/j.1365-2036.2005.02625.x. [DOI] [PubMed] [Google Scholar]
- 2.Triester S L, Leighton J A, Leontiadis G I et al. A meta-analysis of the yield of capsule endoscopy compared to other diagnostic modalities in patients with obscure gastrointestinal bleeding. Am J Gastroenterol. 2005;100:2407–2418. doi: 10.1111/j.1572-0241.2005.00274.x. [DOI] [PubMed] [Google Scholar]
- 3.Lai L H, Wong G L, Chow D K et al. Long-term follow-up of patients with obscure gastrointestinal bleeding after negative capsule endoscopy. Am J Gastroenterol. 2006;101:1224–1228. doi: 10.1111/j.1572-0241.2006.00565.x. [DOI] [PubMed] [Google Scholar]
- 4.Ell C, Remke S, May A et al. The first prospective controlled trial comparing wireless capsule endoscopy with push enteroscopy in chronic gastrointestinal bleeding. Endoscopy. 2002;34:685–689. doi: 10.1055/s-2002-33446. [DOI] [PubMed] [Google Scholar]
- 5.Hartmann D, Schmidt H, Bolz G et al. A prospective two-center study comparing wireless capsule endoscopy with intraoperative enteroscopy in patients with obscure GI bleeding. Gastrointest Endosc. 2005;61:826–832. doi: 10.1016/s0016-5107(05)00372-x. [DOI] [PubMed] [Google Scholar]
- 6.Lewis B S, Swain P. Capsule endoscopy in the evaluation of patients with suspected small intestinal bleeding: Results of a pilot study. Gastrointest Endosc. 2002;56:349–353. doi: 10.1016/s0016-5107(02)70037-0. [DOI] [PubMed] [Google Scholar]
- 7.Saurin J C, Delvaux M, Vahedi K et al. Clinical impact of capsule endoscopy compared to push enteroscopy: 1-year follow-up study. Endoscopy. 2005;37:318–323. doi: 10.1055/s-2005-861114. [DOI] [PubMed] [Google Scholar]
- 8.Levinthal G N, Burke C A, Santisi J M. The accuracy of an endoscopy nurse in interpreting capsule endoscopy. Am J Gastroenterol. 2003;98:2669–2671. doi: 10.1111/j.1572-0241.2003.08726.x. [DOI] [PubMed] [Google Scholar]
- 9.Riphaus A, Richter S, Vonderach M et al. Capsule endoscopy interpretation by an endoscopy nurse – a comparative trial. Z Gastroenterol. 2009;47:273–276. doi: 10.1055/s-2008-1027822. [DOI] [PubMed] [Google Scholar]
- 10.Gan T, Wu J C, Rao N N et al. A feasibility trial of computer-aided diagnosis for enteric lesions in capsule endoscopy. World J Gastroenterol. 2008;14:6929–6935. doi: 10.3748/wjg.14.6929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Iakovidis D K, Tsevas S, Polydorou A. Reduction of capsule endoscopy reading times by unsupervised image mining. Comput Med Imaging Graph. 2009;34:471–478. doi: 10.1016/j.compmedimag.2009.11.005. [DOI] [PubMed] [Google Scholar]
- 12.D’Halluin P N, Delvaux M, Lapalus M G et al. Does the “Suspected Blood Indicator” improve the detection of bleeding lesions by capsule endoscopy? Gastrointest Endosc. 2005;61:243–249. doi: 10.1016/s0016-5107(04)02587-8. [DOI] [PubMed] [Google Scholar]
- 13.Buscaglia J M, Giday S A, Kantsevoy S V et al. Performance characteristics of the suspected blood indicator feature in capsule endoscopy according to indication for study. Clin Gastroenterol Hepatol. 2008;6:298–301. doi: 10.1016/j.cgh.2007.12.029. [DOI] [PubMed] [Google Scholar]
- 14.Saurin J C, Lapalus M G, Cholet F et al. Can we shorten the small-bowel capsule reading time with the “Quick-view” image detection system? Dig Liver Dis. 2012;44:477–481. doi: 10.1016/j.dld.2011.12.021. [DOI] [PubMed] [Google Scholar]
- 15.Halling M L, Nathan T, Kjeldsen J et al. High sensitivity of quick view capsule endoscopy for detection of small bowel Crohn’s disease. J Gastroenterol Hepatol. 2014;29:992–996. doi: 10.1111/jgh.12488. [DOI] [PubMed] [Google Scholar]
- 16.Karargyris A, Koulaouzidis A. Capsule-odometer: a concept to improve accurate lesion localisation. World J Gastroenterol. 2013;19:5943–5946. doi: 10.3748/wjg.v19.i35.5943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Saurin J C, Delvaux M, Gaudin J L et al. Diagnostic value of endoscopic capsule in patients with obscure digestive bleeding: blinded comparison with video push-enteroscopy. Endoscopy. 2003;35:576–584. doi: 10.1055/s-2003-40244. [DOI] [PubMed] [Google Scholar]
- 18.Costamagna G, Shah S K, Riccioni M E et al. A prospective trial comparing small bowel radiographs and video capsule endoscopy for suspected small bowel disease. Gastroenterology. 2002;123:999–1005. doi: 10.1053/gast.2002.35988. [DOI] [PubMed] [Google Scholar]
- 19.Pioche M, Filoche B, Jacob P et al. Randomized prospective comparison of the diagnostic yield of PillCam SB2 ® and Mirocam ® videocapsules in patients with obscure digestive bleeding . Gastrointest Endosc. 2011;73:1181–1188. doi: 10.1016/j.gie.2011.02.011. [DOI] [PubMed] [Google Scholar]
- 20.Pioche M, Vanbiervliet G, Jacob P et al. Prospective randomized comparison between axial- and lateral-viewing capsule endoscopy systems in patients with obscure digestive bleeding. Endoscopy. 2013;46:479–484. doi: 10.1055/s-0033-1358832. [DOI] [PubMed] [Google Scholar]
- 21.Delvaux M, Fassler I, Gay G. Clinical usefulness of the endoscopic video capsule as the initial intestinal investigation in patients with obscure digestive bleeding: validation of a diagnostic strategy based on the patient outcome after 12 months. Endoscopy. 2004;36:1067–1073. doi: 10.1055/s-2004-826034. [DOI] [PubMed] [Google Scholar]