

Abstract
Hidden barriers to visit a medical facility especially for young busy workers have been neglected in the aging society. The aim of this cross-sectional study is to analyze demographics of patients who had visited the first known convenient clinic located inside a railway station, which is adjusted to the lifestyle of working generations.
We analyzed de-identified data of patients who had visited the department of internal medicine of a clinic, which is located inside a railway station building and offers primary care with after-hours accessibility in Tokyo, between August 2013 and June 2016. Data were collected on patients’ sex, age, time of visit, waiting time, presence or absence of an appointment, diagnosis, and patients’ addresses using the electronic health and billing records.
Overall, 28,001 patients visited 87,126 times. Number of visits increased in winter season compared with the other seasons. Sixty-one percent were women and the median age of all patients was 38 years (range, 0–102). The number of visits on Mondays was the highest in a week and the most frequent visiting time was between 6 and 7 p.m. The number of visits of working generations (from 15 to 65 years old) and men increased after 6 p.m. and on weekends. The 3 most common diagnoses were upper respiratory tract infection (22,457), allergic rhinitis (20,916), and hypertension (4869). The number of individuals who were referred to other medical institutions was 1022 (1.2%). The median waiting time was 748 seconds (range, 2–5344). The number of visits from within 2-, 5-, and 10-mile radius from our clinic was 41,696 (50.6%), 63,190 (76.7%), and 75,015 (91.1%), respectively, and patients’ addresses were mainly located along the railway network.
The locational and temporal convenience of our clinic has attracted the unmet medical demands especially for young workers who have difficulty in visiting conventional medical institutions.
Keywords: after-hours accessibility, convenient care clinic, Japan, railway network, retail clinic
1. Introduction
In developed countries, many modern urban dwellers put a high value on convenience in their daily life, and a demand for “convenient care” options is growing in the medical field as well. For example, in the United States, a new type of clinic, the so-called retail clinic, has been emerging as insurance coverage is expanded under the Patient Protection and Affordable Care Act of 2010 because of limited access to conventional primary care. Retail clinics are typically located in a pharmacy or supermarket and usually operate with extended hours and during weekends with shorter waiting time and lower cost as compared with a conventional physician's office or emergency department. Indeed, between 2006 and 2016, the number of retail clinics in the United States increased 10-fold from roughly 200 clinics to nearly 2000, and retail clinics have accounted for almost 16 million annual visits in the recent years.[1–3] Such rapid expansion of retail clinics indicates that they fulfilled unmet needs that are lacking in the traditional medical provision system.[4]
In Japan, an exactly similar type of operation as in the retail clinics in the United States is currently not available due to legislative regulations. Japan has achieved a universal health care coverage since 1961, and patients can access to any medical facility they want. However, Japan has the most aging society globally with 25.9% of the total population being 65 years and older in 2014, and this number will continually increase in the coming decades. Since these elderly populations account for 49% of visits in conventional outpatient clinics,[5] the health care system adapted to the requirement of the elderly. With this circumstance, a hidden barrier to visit a medical facility especially for young busy workers might exist because they would need to be absent from their work to see a doctor in the usual primary care service, except in emergency service, due to its unavailability during evenings and weekends.
Another characteristic to be noted is that Japan's annual number of doctor consultations per person was one of the highest among countries joining the Organization for Economic Co-operation and Development (OECD), while the number of practicing physicians per population was below the international average. As a result, annual consultations per doctor were the second highest following Korea: 5963 in Japan, while the OECD average was 2277, and the US average was 1644 in 2013.[6] These health system characteristics were reflected in a recent survey that showed that 27.4% of Japanese patients were dissatisfied with the long waiting time.[7] These inconveniences have often resulted in delays or interruptions of the visit and an increase in emergency department visits.
To solve these problems and improve convenience in medical visits in Japan, we have focused on an extensive railway network in the metropolitan Tokyo area. Tokyo and the surrounding areas have more than 30 million population with a highly dense and connected railway system as globally unparalleled.[8] In the past, train stations were considered to be just a place to pass through; however, additional services have begun to emerge recently. Since 2000, commercial facilities such as clothing stores, restaurants, and bookstores were opened in Ekinaka, which means “inside a station” in Japanese, focusing on its convenience to effectively utilize a person's short spare time and ability to attract various busy commuters.[9] Since 2007, we have established the first known Ekinaka convenient clinic adjusted to the lifestyle of working generations in Tachikawa station, which is one of the largest transport hub stations in Tokyo. Tachikawa station accounts for 160,000 passengers daily and is the fifth largest station among the East Japan Railway Company, except in the stations of the Yamanote Loop Line at the center of Tokyo.[10] Our clinic operates with extended hours and on Saturdays so that patients can easily visit us. In this study, we investigated the characteristics of patients visiting this new kind of Ekinaka convenient clinic characterized by locational and temporal convenience.
2. Methods
Our clinic, “Navitas Clinic Tachikawa,” is located inside the building of the Tachikawa station, where 3 independent railway routes connect together, and within 1-minute-walk distance from the nearest ticket gate. Tachikawa station is the gateway to Tachikawa City with the population of 180,000 and about 30 minutes to the central Tokyo area by an express train. The clinic opens from 9 a.m. to 1 p.m. and from 3 p.m. to 9 p.m. on weekdays, and from 10 a.m. to 5 p.m. on Saturdays. Usually, 2 physicians operate the department of internal medicine. We obtained de-identified data of patients who had visited the department of internal medicine in our clinic between August 2013 and June 2016 using the electronic health and billing records. We retrospectively extracted data on patients’ sex, age, time of visit, waiting time, presence, or absence of an appointment, diagnoses, and patients’ addresses. This study was approved by the institutional review board of Teikyo University, Tokyo, Japan.
Data on other medical services, such as immunization for seasonal influenza or visits to the department of dermatology or pediatrics, were not included in the analysis. Physicians exceptionally examined children or patients with skin problems only when dermatologists or pediatricians were absent and those data were included in the analysis. The data between September 6, 2015, and October 12, 2015, were not available because of the changes in the electronic health record vendors and were not included in the analysis. The referral rate to other medical institutions was counted not by each visit but by each patient. To compare the data with the conventional clinics in Japan, publicly available data was used with regard to the statistics of patients’ characteristics in conventional Japanese clinics published in 2014 by the Ministry of Health, Labour, and Welfare (MHLW).[5]
Statistical analyses were performed using the R version 3.1.2 (R foundation for Statistical Computing, Vienna, Austria). To determine the associations, a one-way analysis of variance, Tukey–Kramer test, and chi-square test were used. In all analyses, a P-value of <.05 indicates a statistical significance. Plotting of the patients’ addresses on the map was performed using the software MapInfo (Pitney Bowes Software K.K., Tokyo, Japan).
3. Results
During the study periods, 28,001 patients visited for 87,126 times. The average number of daily visits on weekdays was 109.6 and that of on Saturdays was 75.6. The median times of visit of each person were 2 and the mode was 1. Only 132 (0.47%) patients visited more than once a month on average. Men visited 33,953 times (39.0%) and the median age of all patients was 38 years (range, 0–102). Figure 1 shows the comparison of the age distribution between our clinic and other conventional Japanese clinics. The age of patients in our clinic was slightly skewed to the left (skewness was 0.69) and that in conventional clinics was skewed to the right; patients in our clinic were relatively younger than conventional clinics.
Figure 1.
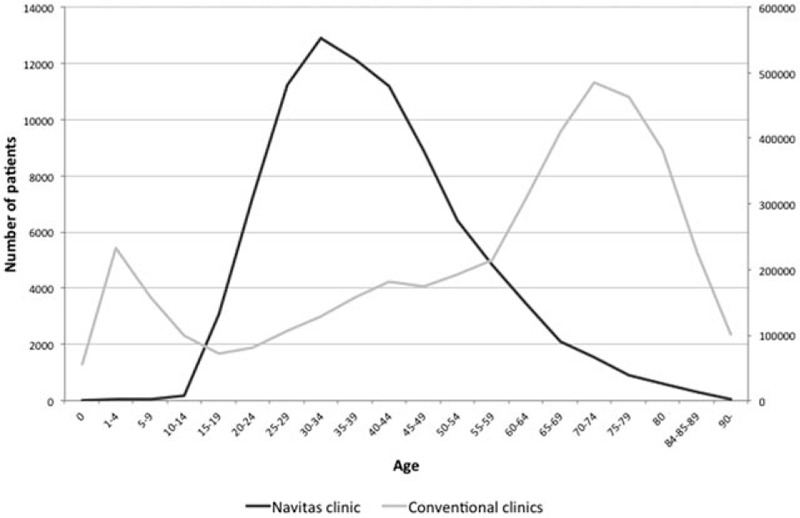
The number of patients by age groups in Navitas Clinic and conventional clinicsa in Japan. aData of conventional clinics were extracted from the Patient Survey published in 2014 by the Ministry of Health, Labour, and Welfare.
The overall median waiting time was 748 seconds (range, 2–5344). The median waiting time was 994 seconds (range, 2–5341) among the 29,622 (36.2%) patients without an appointment, and 665 seconds (range, 2–5344) among the 52,214 (63.8%) patients with an appointment. The proportion of patients who waited <15 minutes, between 15 and 30 minutes, between 30 and 60 minutes, and >60 minutes were 59.2%, 28.0%, 10.7%, and 2.1%, respectively.
Seasonal variations were observed in the number of visits (Fig. 2). The average number of monthly patients in winter seasons (December, January, and February), summer seasons (June, July, and August), and the other seasons were 2892, 2333, and 2513, respectively. More patients visited in winter seasons rather than in summer (P = .0024) and the other seasons (P = .017).
Figure 2.
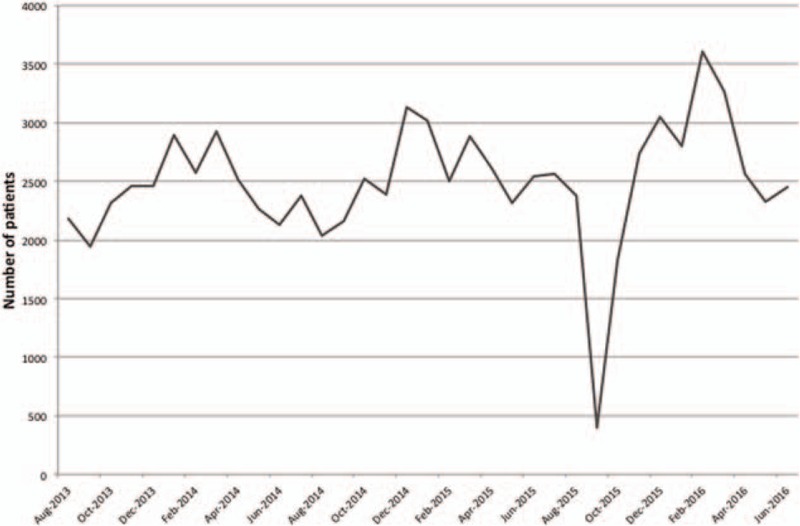
Number of monthly visits to Navitas Clinic. The data between September 6, 2015, and October 12, 2015, were not available because of the changes in the electronic health record vendors and were not included in the analysis.
Variations in the distribution of visits based on the day of the week (Fig. 3) were also observed. The number of daily visits on Mondays, Tuesdays, Wednesdays, Thursdays, Fridays, and Saturdays was 146.5 (23.3%), 110.2 (17.6%), 93.8 (14.9%), 104.8 (16.7%), 96.6 (15.4%), and 75.6 (12.0%), respectively. Of the 76,738 weekday visits and 10,722 Saturday visits, 29,159 (38.2%) and 4,794 (44.7%) were men, respectively. The proportion of men was significantly larger during Saturdays than weekdays (P < .001). Of the 81,319 visits of working generations (from 15 to 65 years old) and 5801 visits of patients <15 or >65 years old, 10,271 (12.6%) and 458 (7.9%) were on Saturdays, respectively. The proportion of Saturday visits was significantly larger among working generations compared with patients <15 or >65 years old (P < .001).
Figure 3.
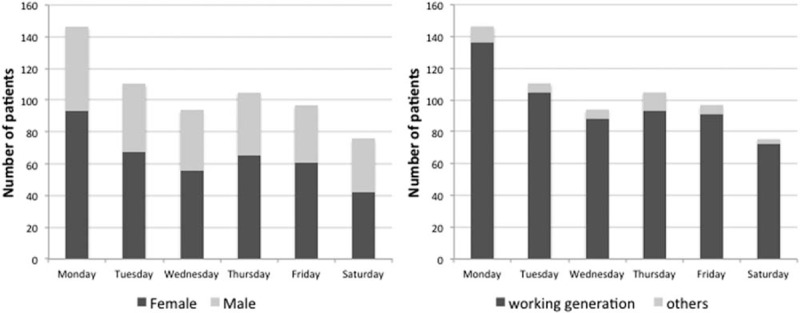
Number of daily visits to Navitas Clinic based on the day of the week. Left: The numbers of daily visits are shown for males and females. Right: The numbers of daily visits are shown for each age group.
Figure 4 shows the number of weekday visits by the time of the day throughout the study periods. Many patients visited at 10 a.m. and 3 p.m., the time when consultation starts; 8903 (11.6%) and 8302 (10.9%), respectively. However, the most popular visiting time was between 6 and 7 p.m. with 11,520 (15.1%) patients. Approximately, one-third (35.5%) of weekday visits occurred after 6 p.m., when other physicians’ offices are typically closed. Adding weekend visits to that proportion, 43.4% of our clinic visits occurred when other physician's offices are likely to be closed. Among the 49,270 visits before 6 p.m. and 27,108 visits after 6 p.m., 17,668 (35.9%) and 11,491 (42.4%) were men, respectively. The proportion of men significantly increased after 6 p.m. compared with before 6 p.m. (P < .001). Among the 71,048 visits of working generations and 5343 visits of patients <15 or >65 years old, 26,732 (37.6%) and 376 (7.0%) were after 6 p.m., respectively. The proportion of visits after 6 p.m. was significantly higher among working generations compared with patients <15 or >65 years old (P < .001).
Figure 4.
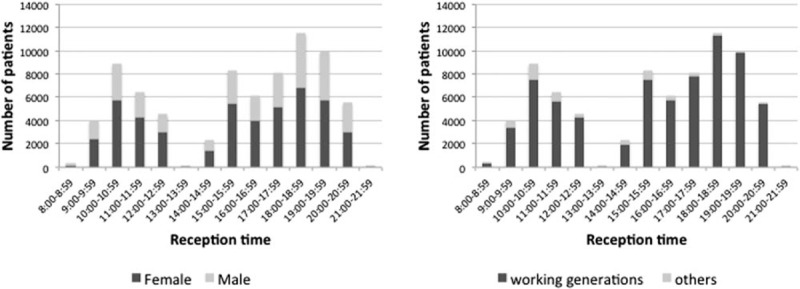
Number of weekday visits to Navitas Clinic based on the time of the day. Left: The numbers of weekday visits are shown for males and females. Right: The numbers of weekday visits are shown for each age group.
Common diagnoses included upper respiratory tract infection (22,358), allergic rhinitis (20,916), hypertension (4869), dyslipidemia (3901), gastroenteritis (3532), asthma (3497), sleep apnea syndrome (2386), pharyngitis (2230), iron deficiency anemia (2166), and acute gastritis (1875). The number of individuals who were referred to other medical institutions was 1022 (1.2%).
Figure 5 shows geographical plots of residence of patients (n = 82,381), the locations of our clinic, and the surrounding railway network. The number of visits came within 2-, 5-, and 10-mile radius from our clinic was 41,696 (50.6%), 63,190 (76.7%), and 75,015 (91.1%), respectively. Their addresses were mainly located along the railway network.
Figure 5.
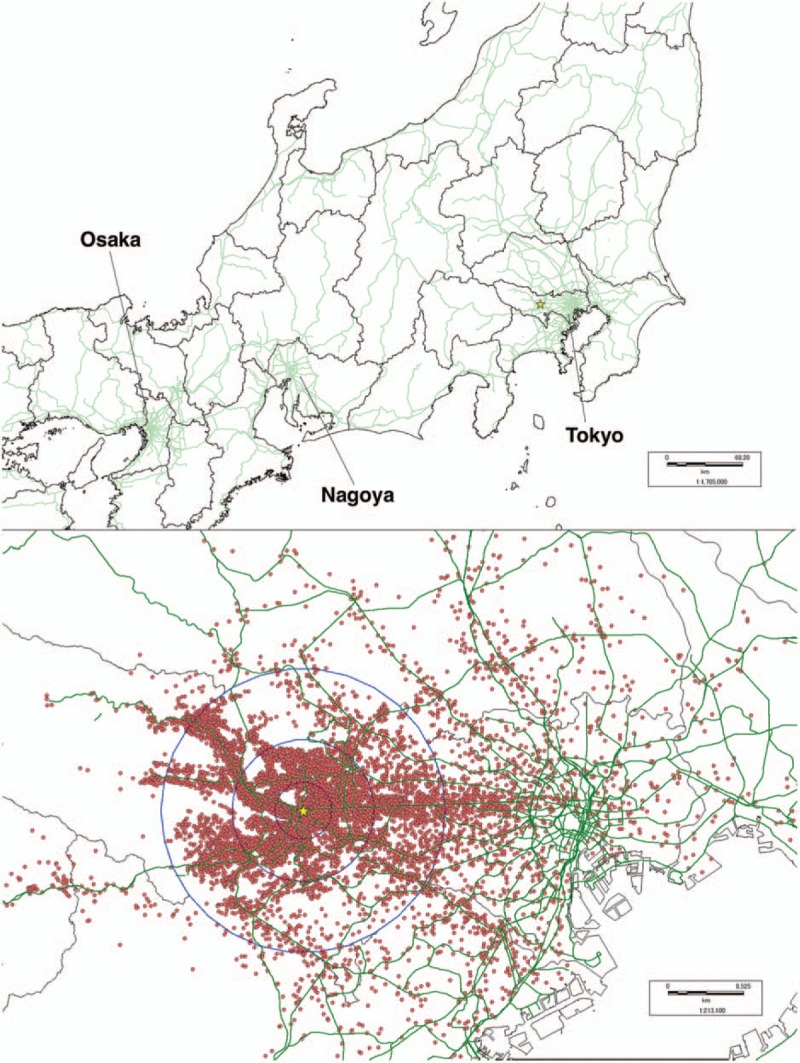
Addresses of patients and the railroad network around Navitas Clinic. Upper: Map of Tokyo and surrounding areas. Lower: Magnified map around Tachikawa City in Tokyo. The yellow star indicates the location of Navitas Clinic Tachikawa; the green lines indicate the railway network; the red points indicate patients’ addresses; the blue circles indicate 2, 5, and 10-mile radius from the clinic.
4. Discussion
Our convenient care clinic is located inside one of the largest station buildings in Tokyo, and we have provided extended hours of access that is rare in Japanese medical institutions other than an emergency department. Here, we revealed unique demographic characteristics of our patients that were different from those in conventional clinics in Japan; patients were younger, predominantly women, and visited most often between 6 and 7 p.m. These characteristics were consistent with those of the customers of other station-related non-medical commercial facilities.[11,12]
The most common diagnoses of our patients were uncomplicated common diseases such as an upper respiratory tract infection or allergic rhinitis. Admittedly, patients with such disease will be able to endure without medication; however, the quality of life and the efficacy of the work would be significantly impaired if untreated. Since the Japanese society suffers from a declining birth rate and shrinking total population, the barriers of visiting should be removed as much as possible to improve the productivity of young workers. Notably, our results showed that episodes were usually resolved within 1 or 2 visits, and referral rates to other medical institutions were quite low. This suggests that patients might have an ability to self-triage, and patients with minor symptoms were attracted to our clinic as in the context of retail clinics.[13] Further, although the usual catchment area of conventional clinics located in a residential area in Tokyo has been thought to be within 1 to 2 miles from a clinic, half of the patients of our clinic came from more than a 2-mile radius. As most of their residence was distributed along the railway network, we speculate that railway users visit our clinic on the way to work, home, or of shopping.
The proportion of patients in working generations and men significantly increased after 6 p.m. and during weekends, when the usual physician's offices are typically closed. Although the precise reason of the increase was not surveyed in this study, we suppose that these workers visited us when they are free from their work. In Japan, the proportion of regular employment of men is higher than that of women (78% and 43%, respectively, in 2014)[14] and such a disproportion of employment pattern might have been associated with the increased proportion of male patients after 6 p.m. and during weekends. These needs will also increase among women as their participation in the workforce continues to rise with an active support from the Japanese government.
Another point to be noted is the quite short waiting time in our clinic compared with that in conventional Japanese hospitals. According to the patients’ behavior survey published by the MHLW in 2014, the proportions of patients who waited for <15 minutes, 15 to 30 minutes, 30 to 60 minutes, and >60 minutes in hospitals were 25%, 24.1%, 20.4%, and 24.7%, respectively.[5] Although most of our patients had an uncomplicated illness that requires only short exam time, the reservation system we have developed would have contributed to the results, that is, when making a reservation, our patients can choose from multiple ways: either through a smart phone, website, phone call (automated voice or an operator), or over the counter at the clinic. Additionally, in our clinic, the reservation time bands are divided into units of 12 minutes to reduce the waiting time as much as possible. Such punctual short waiting time would bring additional convenience to patients so that they can use their spare time on their way to work, home, or shopping, and can easily make their plans as scheduled.
Since retail clinics in the Unites States share the similar concept with our clinic to meet patients’ demands for greater convenience, it is plausible that both resulted in similar patients’ characteristics. In the previous studies with regard to retail clinics, patients were dominantly women (63.8%) and 18 to 44 years old (43%), lived within the 10-miles radius, and their visits increased during winter.[15,16] Approximately, one-third (28.9%) of weekday visits occurred after 6 p.m. when the usual physician's offices are typically closed and the proportion increased to 44.4% when weekend visits were added. More than 90% of patient's visits were mainly due to acute simple illnesses such as upper respiratory tract infections, bronchitis, urinary tract infections, etc., and the referral rate to an emergency department was low (2.3%).[17] These similarities indicate that demands for convenience among younger population are universal in developed countries.
However, several differences were noted between the retail clinics and our clinic. First, retail clinics are typically staffed by nurse practitioners or physician assistants, but our clinic is staffed by doctors. Physician organizations such as the American Academy of Pediatrics and the American Academy of Family Physicians have expressed concerns for the potential fragment of care and lower-quality care in retail clinics,[13] but such criticisms would not be applicable in our clinic.
Second, the difference in staff resulted in the difference of the disease they catered. Chronic diseases such as hypertension, dyslipidemia, and sleep apnea syndrome were higher in out clinic than in retail clinics. Furthermore, gastroenteritis and gastritis were higher in our clinic because various diseases can cause stomachache, whereas retail clinics are not designed to differentiate complicated medical conditions. On the other hand, diagnoses of sinusitis, otitis externa, otitis media, and conjunctivitis are higher in retail clinics because Japan has a universal health coverage with free access to any medical institutions, so patients would have chosen to visit an otolaryngologist or ophthalmologist before visiting our clinic when they experienced symptoms in their noses, ears, or eyes.
Third, financial incentives for patients exist only in retail clinics. Compared with the primary care physicians’ office in the United States, the medical expenses in retail clinics is inexpensive. However, there is not such a difference between our clinic and conventional Japanese clinics because official standard prices are implemented in Japan regardless of the types of operation.
Our clinic may contribute to a decrease of emergency visits to other institutions located in the surrounding areas. A previous report in the United Kingdom showed that, compared with practices without extended access, extended access of primary care services demonstrated a 26.4% relative reduction in patient-initiated emergency department visits for “minor” problems in addition to a 26.6% relative cost reduction.[18] However, retail clinics could not prove the decrease of emergency department utilization for low-acuity conditions and healthcare expenses.[19,20] Since low-acuity emergency department visits became a widespread problem in hospitals globally,[21] future studies would be needed to explore the impact of our clinic on local medical services in Japan.
This study has several limitations. First, it is an observational study in a single institution so findings cannot be widely generalized. Second, we compared the characteristics to the data of conventional clinics obtained from a nationwide survey of Japanese patients, because we could not obtain the data from other clinics in the region. For the comparison regarding waiting time, the average in outpatient department of hospitals was used because that in conventional clinics was not available. Third, the diagnoses were based on the terminology in the health insurance claim forms, and the actual medical conditions might have been different from them in some cases.
5. Conclusion
From this observational study of >87,000 patient visits, it was revealed that young workers mainly living along the railway network visit our Ekinaka clinic mostly after work because of uncomplicated illnesses. Our clinic, which is located inside a railway station building and operates with extended hours and on Saturdays, seemed to have met the unmet medical needs especially for patient populations that have been underserved by conventional medical institutions with the locational and temporal convenience. Since urbanization has made rapid strides globally[22] and constructions of railway networks are progressing further in Asia[23,24] in addition to other metropolises that has existing railway networks, such as New York, Seoul, Shanghai, Paris, and London, our Ekinaka clinic will be a new model of physicians’ office applicable to other urban cities.
Acknowledgments
The authors wish to thank Dr. Seiya Imoto, a professor at Tokyo University, for advice on the study design and Kan Suzuki, a professor at Tokyo University, for advice on the concept of the Navitas Clinic.
Footnotes
Funding Sources: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The authors have no conflicts of interest to disclose.
References
- [1].Blue Cross and Blue Shield Association. Retail clinic visits increase despite use lagging among individually insured Americans. Available at: https://www.bcbs.com/about-us/capabilities-initiatives/health-america/health-of-america-report/retail-clinic-visits. Accessed April 17, 2017. [Google Scholar]
- [2].Zamosky L. What retail clinic growth can teach us about patient demand. Threat or opportunity: retail clinic popularity is about convenience. Med Econ 2014;91:22–4. 29–30. [PubMed] [Google Scholar]
- [3].Accenture. Number of U.S. retail health clinics will surpass 2,800 by 2017. Accenture forecasts. Available at: https://newsroom.accenture.com/news/number-of-us-retail-health-clinics-will-surpass-2800-by-2017-accenture-forecasts.htm. Accessed April 17, 2017. [Google Scholar]
- [4].Mehrotra A. The convenience revolution for treatment of low-acuity conditions. JAMA 2013;310:35–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].The Ministry of Health, Labor and Welfare. Outline of survey results. Available at: http://www.mhlw.go.jp/english/database/db-hss/dl/sps_2014_01.pdf. Accessed April 17, 2017. [Google Scholar]
- [6].OECD. Health at a Glance 2015: OECD Indicators; 2015. Available at: http://dx.doi.org/10.1787/health_glance-2015-en. Accessed April 17, 2017. [Google Scholar]
- [7].The Ministry of Health, Labor and Welfare. Outline of patient's behavior survey results (in Japanese). Available at: http://www.mhlw.go.jp/toukei/saikin/hw/jyuryo/14/dl/gaikyo-all.pdf. Accessed April 17, 2017. [Google Scholar]
- [8].Haruya Hirooka. The development of Tokyo's rail network. Available at: http://www.ejrcf.or.jp/jrtr/jrtr23/pdf/F22_Hirooka.pdf. Accessed April 17, 2017. [Google Scholar]
- [9].SPEEDA. Ekinaka and the station building: diversification strategy of East Japan Railway Company (in Japanese). Available at: https://jp.ub-speeda.com/analysis/archive/36/. Accessed April 17, 2017. [Google Scholar]
- [10].East Japan Railway Company. Number of passengers of each railway stations in 2015 (in Japanese). Available at: http://www.jreast.co.jp/passenger/index.html. Accessed April 17, 2017. [Google Scholar]
- [11].Kanto transportation advertisement council. Transit media marketing report 2009 (in Japanese). Available at: http://www.train-media.net/report/0812/report_09.pdf. Accessed April 17, 2017. [Google Scholar]
- [12].Station consumption research center. Results of the survey of station-related economics in capital area (in Japanese). Available at: http://www.jeki.co.jp/ekishoken/upload/docs/EKISUMER_vol_5.pdf. Accessed April 17, 2017. [Google Scholar]
- [13].Chang JE, Brundage SC, Chokshi DA. Convenient ambulatory care—promise, pitfalls, and policy. N Engl J Med 2015;373:382–8. [DOI] [PubMed] [Google Scholar]
- [14].The Statistics Bureau, Ministry of Internal Affairs and Communications. Characteristics of the regular and non-regular employment in these days (in Japanese). Available at: http://www.stat.go.jp/info/today/097.htm#k14. Accessed April 17, 2017. [Google Scholar]
- [15].Mehrotra A, Lave JR. Visits to retail clinics grew fourfold from 2007 to 2009, although their share of overall outpatient visits remains low. Health Aff (Millwood) 2012;31:2123–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Association of State and Territorial Health Officials. Defining the Safety Net: Retail Clinics. Available at: http://www.astho.org/Programs/Access/Primary-Care/Safety-Net-Fact-Sheets/Materials/Retail-Clinics-Fact-Sheet/. Accessed April 17, 2017. [Google Scholar]
- [17].Mehrotra A, Wang MC, Lave JR, et al. Retail clinics, primary care physicians, and emergency depart- ments: a comparison of patients’ visits. Health Aff (Millwood) 2008;27:1272–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Whittaker W, Anselmi L, Kristensen SR, et al. Associations between extending access to primary care and emergency department visits: a difference-in-differences analysis. PLoS Med 2016;13:e1002113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Martsolf G, Fingar KR, Coffey R, et al. Association between the opening of retail clinics and low-acuity emergency department visits. Ann Emerg Med 2017;69:397.e5–403.e5. [DOI] [PubMed] [Google Scholar]
- [20].Ashwood JS, Gaynor M, Setodji CM, et al. Retail clinic visits for low-acuity conditions increase utilization and spending. Health Aff (Millwood) 2016;35:449–55. [DOI] [PubMed] [Google Scholar]
- [21].Smits M, Rutten M, Keizer E, et al. The development and performance of after-hours primary care in the Netherlands: a narrative review [published online Apr 18, 2017]. Ann Intern Med 2017;166:737–42. [DOI] [PubMed] [Google Scholar]
- [22].Science. Rise of the urban planet. Available at: http://www.sciencemag.org/news/2016/05/use-our-infographics-explore-rise-urban-planet?utm_source=print_feature_drupal&utm_medium=magazine&utm_campaign=campaign-4278. Accessed April 17, 2017. [Google Scholar]
- [23].The Voice of Vietnam Online. Japan company helps Hanoi operate urban railway system. Available at: http://english.vov.vn/economy/japan-company-helps-hanoi-operate-urban-railway-system-347271.vov. Accessed April 17, 2017. [Google Scholar]
- [24].Updating Filipinos Online. Japan to start constructing railway in PH this year. Available at: http://www.update.ph/2017/01/japan-to-start-constructing-railway-in-ph-this-year/13100. Accessed April 17, 2017. [Google Scholar]