

Abstract
Objective
The aim of this in vitro study was to evaluate marginal adaptation and fracture strength of inlays produced by CEREC Omnicam using different types of blocs and heat-pressed technique. Methods: Seventy-five extracted human mandibular molars were divided randomly into 5 groups (n=15). 60 molars in four groups received MOD inlay preparations. Experimental groups were CO: Intact teeth, EC: IPS e.max CAD and CEREC, LU: Lava Ultimate and CEREC, EL: IPS Empress CAD and CEREC, EP: IPS Empress Esthetic ingots and heat-pressed technique. Marginal gap measurements were taken with a stereomicroscope. Restorations were cemented with Variolink N and stored in distilled water at 37°C for 24 hours. All samples were subjected to thermocycling. The fracture strength of specimens was determined at a 0.5 mm/min crosshead speed until fracture. Fracture modes were determined. Statistical analyses were performed using one-way analysis of variance for fracture strength data and Kruskal–Wallis for marginal gap data (p=0.05).
Results
The mean marginal gap size of EC, LU, EL, and EP were 33.54 µm, 33.77 µm, 34.23 µm, and 85.34 µm, respectively. EP had statistically higher values than other groups. The fracture strength values were significantly higher in the intact teeth group (3959,00 ± 1279,79 N) than those of restored groups EC (2408,00 ± 607,97 N), LU (2206,73 ± 675,16), EL (2573.27 ± 644,73) ve EP (2879,53 ± 897,30).
Conclusion
Inlays fabricated using CEREC Omnicam demonstrated better marginal adaptation than inlays produced with heat-pressed technique, whereas fracture strength values of inlays fabricated with different type of blocks using CEREC Omnicam exhibited similarity to those fabricated with heat-pressed technique.
1. Introduction
Multiple parameters influence the longevity of dental restorations such as material properties, patient's health status, dentist's experience, and fabrication methods [1]. Restorations generated with indirect methods have desirable mechanical properties, and they are produced under slightly ideal in vitro conditions [2]. Additionally, patients' increasing demand for tooth-colored posterior restorations has stimulated the improvement of indirect methods and materials for posterior esthetic restorations [1]. Heat-pressed technique is one of the frequently used methods for making ceramic restorations. Leucite-reinforced glass ceramic IPS Empress System was manufactured with heat-pressed technique for the intention of restoring single units, including esthetic inlays [3]. Industrially fabricated machinable ceramics are produced for technician use in laboratory and clinician use for chair-side applications. Digital systems such as computer aided design and computer aided manufacturing (CAD/CAM) have evolved as an alternative for high-temperature injection molding using the lost-wax technique [4]. Moreover, with advancements in material sciences, ceramic restorations have shown better results to fulfil mechanical and esthetic necessities for patients [5]. Restorations fabricated using industrially made CAD/CAM ceramic blocks have remarkably improved mechanical properties such as reduction in cracks and voids in comparison with restorations produced in laboratory [6]. A wide collection of ceramic materials has been available for both CAD/CAM technology and heat-pressed technique, ranging from relatively weak leucite glass ceramic to high-strength lithium disilicate glass ceramic [7]. Different ceramic blocs are used for CAD/CAM technology such as IPS e.max CAD (Ivoclar Vivadent AG, Liechtenstein), a lithium disilicate improved glass-ceramic material with a relatively high fracture strength [8] and Lava Ultimate (3M-ESPE, St Paul, USA), a resin nanoceramic with an elastic modulus value similar to dentin [9]. Material properties can be an important factor for fracture strength [10]. Furthermore, the fracture strength of ceramic restorations is also influenced by elastic modulus [11].
Marginal adaptation is also crucial for ceramic inlay restorations to avoid resin cement wear and plaque accumulation. Marginal gap formations at restorations exposes resin cement to the oral environment leading to resin cement wear. Marginal discrepancies cause debris and food to act as potential irritants which might induce secondary caries and devitalization of the pulp [12]. Moreover, an unsuitable fit of the restoration cannot be well supported by the remaining tooth substance and influences the longevity of the restoration [13]. One of the most significant advances in dentistry has been the introduction of CAD/CAM systems. Popularity of these systems has increased significantly in the last decade due to the simplicity of their application [14]. Some studies which examined the marginal adaptation of different ceramic inlay systems have shown acceptable results [15, 16].
In the dental field, to improve impression techniques, lately a powder-free 3D oral scanning camera (CEREC Omnicam) was introduced to produce more precise teeth scans. However, the marginal adaptation of ceramic mesio-occlusal-distal (MOD) inlays produced by the heat-pressed technique has not been compared to those produced by the CEREC Omnicam CAD/CAM systems. Therefore, the aim of this study was to evaluate and compare the marginal adaptation and the fracture strength of MOD ceramic inlay restorations fabricated by CEREC Omnicam CAD/CAM system and heat-pressed technique. Also different types of ceramic blocs were compared in the means of fracture strength for ceramic inlays fabricated by CEREC Omnicam system.
2. Materials and Methods
In this in vitro study, 75 extracted, caries-free human mandibular third molars with similar buccolingual and mesiodistal dimensions were selected. Ethics Committee approval (GO 14/138-16) was obtained for the extracted human teeth. An electronic digital caliper (Absolute Digimatic Mitutoyo, Tokyo, Japan) were used for measurement. Teeth were stored in distilled water after calculus and soft-tissues were removed with a hand scaler and cleaned using a rubber cup. Teeth were examined under magnifying glasses (Hires 2.5, Orascoptic, CA, USA) to detect any preexisting defects. Only intact, noncarious, unrestored teeth were included in the study. These teeth were randomly divided into four groups (n=15). The root of each tooth was embedded in an autopolymerizing acrylic resin (Meliodent, Heraeus Kulzer GmbH, Hanau, Germany) up to 2 mm below the cementoenamel junction. Experimental groups were as follows:
CO: intact teeth, no treatment (control group)
EC: teeth restored with lithium disilicate glass-ceramic (IPS e.max CAD, Ivoclar Vivadent AG) using CEREC Omnicam
LU: teeth restored with resin nanoceramic (Lava Ultimate, (3M ESPE, Seefeld, Germany) using CEREC Omnicam
EL: teeth restored with leucite-reinforced glass ceramic (IPS Empress CAD, Ivoclar Vivadent AG) using CEREC Omnicam
EP: teeth restored with leucite-reinforced glass ceramic (IPS Empress Esthetic, Ivoclar Vivadent AG) and hot pressed technique
Teeth in EC, LU, EL, and EP groups first received a standardized mesio-occlusal-distal preparation with the geometry of an inlay cavity using a straight fissure flat-ended diamond bur (Diatech Dental, Coltene-Whaledent, Altstatten, Switzerland) on a high-speed handpiece with water spray cooling. Diamond burs were used for five preparations, and a new bur was used after 5 specimen. Mesial and distal finishing lines of the proximal boxes were 1 mm above the cementoenamel junction and the proximal boxes had 2 mm width mesiodistally. Pulpal floors were prepared flat, and angles were rounded. The width of the occlusal cavity was designed to prepare 1/3 of that of the tooth, and the occlusal depth was prepared to 3 mm from the occlusal margin. The occlusogingival dimension of the proximal box was approximately 4.0 to 4.5 mm, depending on the length of the crown. A 6° divergence of the walls of the occlusal and proximal boxes was prepared using a tapered diamond with a convergence angle of 6°.
2.1. Fabrication of Inlay Restorations with CEREC Omnicam CAD/CAM System
In the EC, LV, and EL groups, inlays were fabricated by CEREC Omnicam (Sirona Dental System, GmbH, Bensheim, Germany). Digital impressions were taken without powder application using CEREC SW 4.2.3 software. Following impressions and design (Figures 1(a) and 1(b)), occlusal thicknesses of restorations were checked using “cursor details” tools of the programme. It was ensured that all occlusal thicknesses were between 2.6 and 2.8 mm before milling procedure. Restorations from group EC were designed and milled with from presintered lithium disilicate glass-ceramic blocks (IPS e.max CAD, Ivoclar Vivadent, Schaan, Liechtenstein). Crystallization of IPS e.max CAD restorations was performed in Progmat P310 (Ivoclar Vivadent, Schaan, Liechtenstein) furnace after the milling procedure following the manufacturer's instruction. The temperature was 840°C, and the dwell time was 7 min. The restorations were then glazed with IPS e.max Ceram Glaze Liquid and Paste (Ivoclar Vivadent, Schaan, Liechtenstein). A single-glaze firing was performed in Progmat P310 (Ivoclar Vivadent, Schaan, Liechtenstein) furnace at 840°C with a dwell time of 3 min. Restorations from group EL were designed and fabricated from leucite-reinforced glass ceramic (IPS Empress CAD, Ivoclar Vivadent AG). The restorations were then glazed with IPS Empress CAD Universal Glaze Stain Liquid and Paste (Ivoclar Vivadent, Schaan, Liechtenstein). A single-glaze firing was performed in Progmat P310 (Ivoclar Vivadent, Schaan, Liechtenstein) furnace at 840°C with a dwell time of 3 min. On the other hand, LU restorations received a sandblasting treatment to the internal surfaces with 50 μm alumina particles at an air pressure of 30 PSI. Finishing and polishing procedure of LU group was conducted with Sof-Lex discs (3M ESPE, St. Paul, USA, Batch number 5082S).
Figure 1.

(a) Digital impression of a preparation in CEREC Omnicam. (b) Restoration design of Lava Ultimate restoration. (c) Lava Ultimate inlay restoration after cementation.
2.2. Fabrication of Inlay Restorations with Heat-Pressed Technique
A pressable leucite-reinforced glass-ceramic material was used in group EP (IPS Empress Esthetic, Ivoclar Vivadent AG). Impressions were taken using an elastometic material (Virtual Putty and Virtual Light Body, Ivoclar Vivadent, Schaan, Liechtenstein). After preparing stone dies, die spacer was applied, and wax models were fabricated according to appropriate anatomic functional form of each tooth. The wax models were invested in [SheraFina 2000] (SHERA Werkstoff-Technologie GmbH & Co., Lemförde, Germany, Batch number: 30894) investment material. The investment ring was heated at 1060°C for 60 min for the burn-out of the wax analog, and the ingots were pressed into the investment mold using a Programat EP 5000 (Ivoclar Vivadent, Schaan, Liechtenstein) furnace following the manufacturer's instructions. The press temperature was 1075°C, and the dwell time was 23 min. All restorations' occlusal thicknesses were checked using a digital caliper. If a restorations' thickness was not between 2.6 and 2.8, the procedure was repeated for standardization. Finally, a single-glaze firing was performed with Programat EP 5000 (Ivoclar Vivadent, Schaan, Liechtenstein) furnace using IPS Empress Universal Glaze and Stain Liquid and Paste (Ivoclar Vivadent, Schaan, Liechtenstein).
2.3. Marginal Gap Evaluation
For marginal gap measurements, inlays were placed, and to maintain the right position, a specially made clamp was applied. The marginal gaps were measured by one operator under a stereomicroscope (Leica MZ 16A, Leica Microsystems, Switzerland) using Leica Application Suite (Leica Microsystems, Switzerland) software, visually at 12 preselected locations, three on the mesial and 3 on the distal surfaces and 6 on the occlusal surface (3 occlusobuccal and 3 occlusolingual) of the MOD inlay (Figures 2 and 3).
Figure 2.
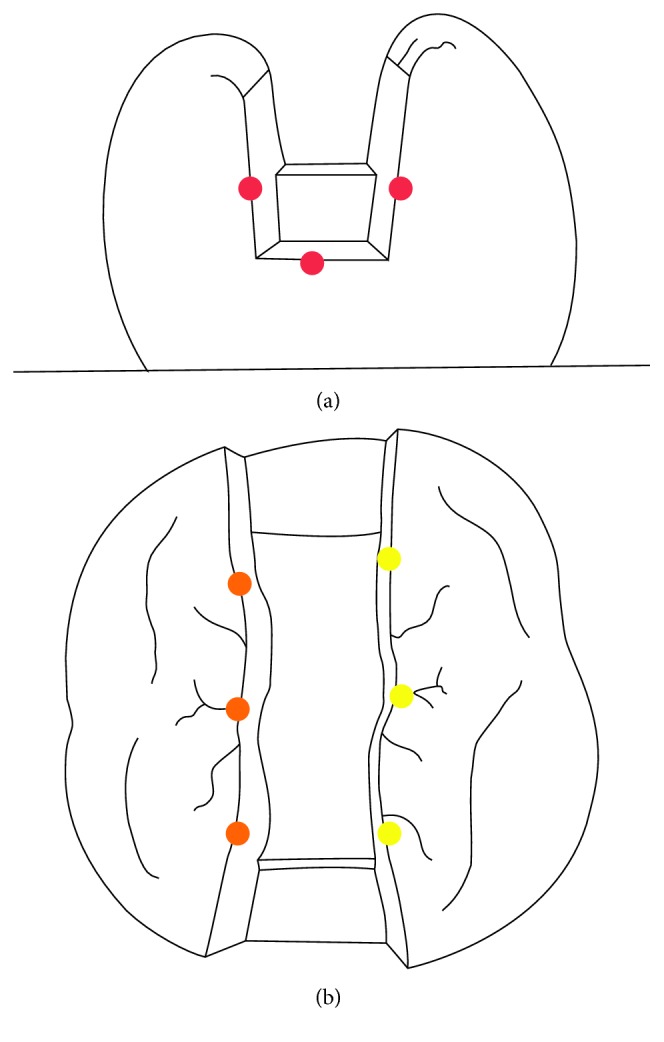
Marginal gap measurement points. (a) Location of measuring points mesially and distally. (b) Location of measuring points on the occlusal aspect.
Figure 3.
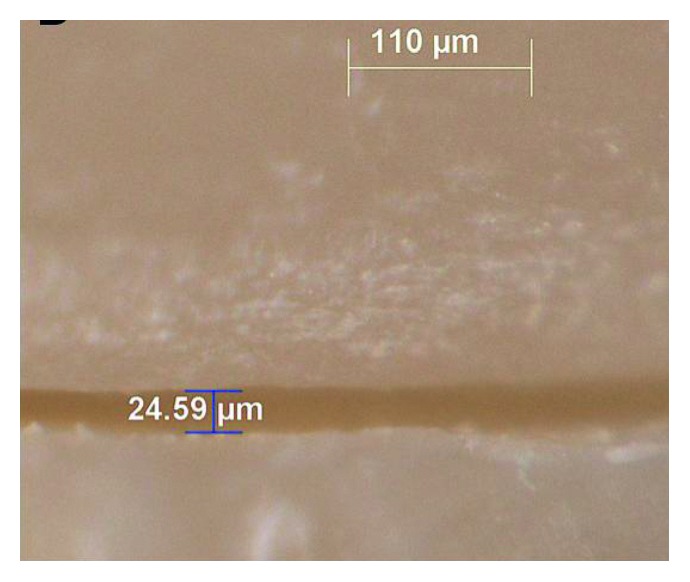
Measurement of marginal gap using a stereomicroscope (Leica MZ 16A, Leica Microsystems, Switzerland), Lava Ultimate inlay, distal.
2.4. Adhesive Placement of Restorations
All groups were cemented using Variolink N (Ivoclar Vivadent, Schaan, Liechtenstein). The inner surfaces of the restorations at EC, EL, and EP groups were etched with a 9.5% hydrofluoric acid gel (Bisco Porcelain Etchant, Bisco Inc., Illinois, USA) for 1 minute, rinsed with a water spray, and dried with oil-free air. According to the manufacturer's instructions, LU group was not etched. Then, a silane coupling agent (Monobond S, Ivoclar Vivadent, Schaan, Lichtenstein) followed by a light curing bonding agent (Heliobond, Ivoclar Vivadent, Schaan, Lichtenstein) was applied. Teeth were etched (30 s for enamel and 15 s for dentine) with 37% phosphoric acid. Tooth surfaces were conditioned with Syntac Primer, Adhesive, and Heliobond (Ivoclar Vivadent, Schaan, Lichtenstein). A dual-polymerising resin composite Variolink N (Ivoclar Vivadent, Schaan Lichtenstein) was placed on the inner surfaces of all restorations and cavity walls. Restorations were seated with finger pressure. Any excess cement was removed, and all surfaces of the restorations (occlusal, mesial, and distal) were then light-cured with a LED curing light wavelength of 470 nm and a power of 1200 mW/cm2 (Bluephase®, Ivoclar Vivadent, Schaan, Liechtenstein, 1200 mW/cm2) for 30 s. Excess cement was removed using polishing discs (Kerr OptiDisc, Bioggio, Switzerland) (Figure 1(c)).
All specimens were stored in distilled water at 37°C for 24 hours and then subjected to thermocycling at 5000 cycles in water baths between 5°C and 55°C. The dwell time at each temperature was 20 seconds, and the transfer time from one bath to the other was 5 seconds.
2.5. Fracture Strength Measurement
The teeth were subjected to axial compressive loading using a metal sphere of 5 mm diameter applied vertically and centered on the occlusal surface of the restoration at a crosshead speed of 0.5 mm/min in a universal testing machine (Lloyd Instruments LR 50K, AMETEK GmbH, Meerbusch, Germany). A thin plastic tape was placed on the surface of the ball to ensure a stable contact between the steel ball and tooth structure. The force (N) required to fracture the restoration was recorded for each specimen. The mode of fracture for each specimen was classified according to Burke [17] (Table 1).
Table 1.
Results of the mean marginal gap. Standard deviation (SD) of the impression methods evaluated at each surface and overall mean marginal gap and SD of each impression method
| Groups (n=15) | Inlay surface | Mean marginal gap (µm) | Standard deviation (SD) | Overall mean marginal gap | Standard deviation (SD) |
|---|---|---|---|---|---|
| EC | Mesial | 32.81 | 16.74 | 33.54a | 15.83 |
| IPS e.max CAD | Distal | 36.05 | 20.54 | ||
| CEREC Omnicam | Occlusobuccal | 32.69 | 12.69 | ||
| Occlusolingual | 32.60 | 12.15 | |||
|
| |||||
| LU | Mesial | 30.55 | 19.80 | 33.77a | 17.35 |
| Lava ultimate | Distal | 29.11 | 18.92 | ||
| CEREC Omnicam | Occlusobuccal | 38.48 | 15.97 | ||
| Occlusolingual | 36.93 | 12.44 | |||
|
| |||||
| EL | Mesial | 32.71 | 18.94 | 34.23a | 17.67 |
| IPS empress CAD | Distal | 31.94 | 18.51 | ||
| CEREC Omnicam | Occlusobuccal | 36.82 | 17.22 | ||
| Occlusolingual | 35.45 | 16.03 | |||
|
| |||||
| EP | Mesial | 88.64 | 37.51 | 85.34b | 38.19 |
| IPS empress esthetic | Distal | 86.80 | 44.29 | ||
| CEREC Omnicam | Occlusobuccal | 84.16 | 32.67 | ||
| Occlusolingual | 81.78 | 38.35 | |||
Values with the same superscript letter are not significantly different (p < 0.001). aSame superscript letters in same column indicates no significant difference (p > 0.05). bDifferent superscript letters in same column indicates significant difference (p < 0.001).
The data obtained for the marginal gap were analyzed statistically using Kruskal–Wallis test and Mann–Whitney U test. Fracture resistance results were analyzed statistically by one-way ANOVA and Tukey HSD tests. The selected level of statistical significance was p < 0.05.
3. Results
The overall mean marginal gaps (μm) for the three groups were EC = 33.54 (±13.83); LU = 33.77 (±17.35); EL = 34.23 (±16.62), and EP = 85.34 (±38.19). EC and LU marginal gaps were similar, and both were significantly less than EP (Table 1).
Statistical differences of surfaces mean marginal gaps (μm) are shown at Table 2. Different surfaces' mean marginal gap values were not significantly different at EC and EP groups; however, at LU occlusobuccal and occlusolingual mean marginal gap calculations were significantly higher than mesial and distal surfaces values (p < 0.05) (Table 2).
Table 2.
Cross table and comparison of different surfaces marginal gap results.
| EC | LU | EL | EP | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IPS e.max CAD | Lava Ultimate | IPS Empress CAD | IPS Empress Esthetic | |||||||||||||
| CEREC Omnicam | CEREC Omnicam | CEREC Omnicam | CEREC Omnicam | |||||||||||||
| Mesial | Distal | Occlusobuccal | Occlusolingual | Mesial | Distal | Occlusobuccal | Occluso lingual | Mesial | Distal | Occlusobuccal | Occlusolingual | Mesial | Distal | Occlusobuccal | Occlusolingual | |
| Mesial | — | 0.696 | 0.608 | 0.589 | — | 0.439 | 0.008s | 0.001s | — | 0.537 | 0.438 | 0.379 | — | 0.526 | 0.564 | 0.260 |
| Distal | 0.696 | — | 0.907 | 0.910 | 0.439 | — | 0.004s | 0.001s | 0.669 | — | 0.715 | 0.744 | 0.526 | — | 0.875 | 0.597 |
| Occlusobuccal | 0.608 | 0.907 | — | 0.990 | 0.008s | 0.004s | — | 0.713 | 0.622 | 0.652 | — | 0.538 | 0.564 | 0.875 | — | 0.300 |
| Occlusolingual | 0.589 | 0.910 | 0.990 | — | 0.001s | 0.001s | 0.713 | — | 0.511 | 0.685 | 0.687 | — | 0.260 | 0.597 | 0.300 | — |
Values with the “s” letter are significantly different according to the Mann–Whitney U analysis. (p < 0.05).
The means and standard deviations for the fracture strength of the test groups are shown in Table 3. One-way ANOVA analysis showed that there were statistically significant differences among the groups. The Tukey HSD test revealed that the control group (CO = 3959.00 N) showed significantly higher fracture strength values than the other groups (p < 0.05). No significant differences were observed between the fracture strength values of the groups restored with inlays (EC: 2408.00 N, LU: 2206.73, EL: 2573.27, and EP: 2879.53 N). The mode of fracture for each group is shown in Table 4. Fracture classifications of specimens were decided under a stereomicroscope (Leica MZ 16A, Leica) with inspection of all sides. Samples of each mode are given in Figure 4.
Table 3.
Mean fracture resistance values, standard deviations, and statistical categories of all experimental groups (n=15).
| Groups | Material | Fracture strength mean values (N) | Standard deviation (SD) |
|---|---|---|---|
| CO | Control | 3959.00a | 1279.79 |
| EC | IPS e.max CAD | 2408.00b | 607.97 |
| LU | Lava Ultimate | 2206.73b | 675.16 |
| EL | IPS Empress CAD | 2573.27b | 644.73 |
| EP | IPS Empress Esthetic | 2879.53b | 897.30 |
Groups with different superscript letters are statistically significantly different according to the Tukey HSD test (p < 0.05). aDifferent superscript letters in same column indicates significant difference (p < 0.001). bSame superscript letters in same column indicates no significant difference (p > 0.05).
Table 4.
Fracture modes of restored specimens according to Burke [17].
| Mode of failure | EC | LU | EL | EP |
|---|---|---|---|---|
| IPS e.max CAD | Lava Ultimate | IPS Empress CAD | IPS Empress Esthetic | |
| CEREC Omnicam | CEREC Omnicam | CEREC Omnicam | CEREC Omnicam | |
| I | 6 (40.0%) | 2 (13.3%) | 5 (33.3%) | 5 (33.3%) |
| II | 4 (26.7%) | 6 (40.0%) | 5 (33.3%) | 5 (33.3%) |
| III | - (0%) | 3 (20%) | 2 (13.3%) | 1 (6.7%) |
| IV | 5 (33.3%) | 4 (26.7%) | 3 (20%) | 4 (26.7%) |
Mode I: isolated fracture of the restoration; mode II: restoration fracture involving a small tooth portion; mode III: fracture involving more than half of the tooth, without periodontal involvement; mode IV: fracture with periodontal involvement.
Figure 4.

Fracture modes. (a) Type 1. (b) Type II. (c) Type III. (d) Type IV.
4. Discussion
Ceramic inlays has many advantages, which include high esthetic values and less tooth reduction compared to crowns or onlays; hence, more preservation of healthy tooth structures. Furthermore, with the development of CAD/CAM systems, the clinical process of placing inlays has become more efficient and convenient, which greatly improves the quality of the restoration and decreases the patient's visit time [18].
CAD-CAM technology has been introduced in the dental field to improve conventional impression techniques and manufacturing phases. Some studies show a higher marginal accuracy of restorations derived from an intraoral scanner in comparison to conventional impressions [19, 20]. Moreover, in this way, the dentist is able to check the preparation and can view the preparation simultaneously and discuss possible problems. On the other hand, scanning with a powder-free 3D measuring unit produces good values that are reliable, in particular, for single-tooth scans [21]. Conversely, an in vitro study showed that using powder before digital impression making with CEREC Omnicam resulted in significantly smaller marginal gap formations in crowns [22].
IPS Empress Esthetic restorations were fabricated using conventional two-step impression technique, whereas digital intraoral impressions were taken using CEREC Omnicam for IPS e.max CAD, Lava Ultimate, and IPS Empress CAD restorations.
Intact human teeth were used to evaluate and compare ceramic inlay restorations to obtain highly relevant clinical results. Also, adhesive cementation and bonding procedures were applied carefully to provide similar clinical outcomes [23]. The preparation was designed according to preparation guidelines for inlay restorations mentioned in the literature [19, 24]. Many variables in addition to ceramic type will influence the marginal gap value such as restoration fabrication method, location of the preparation, measuring techniques, number of measuring points, and tooth preparation design [25].
The direct measurement technique was used in the present study leaving the tooth intact and allowing for the reproducibility of measurements at different time intervals. This technique was used in several in vitro studies [26, 19, 27] and can therefore be considered as a well documented procedure. Direct measurement allows us to evaluate the marginal gaps from all angles and selected areas [26]. A large marginal discrepancy causes higher plaque index at restoration margins and periodontal problems. Thus, achieving a gap width below 100 μm is desirable for clinically acceptable restorations [28]. The mean marginal discrepancies of inlay restorations of the present study were 85.34 µm for IPS Empress Esthetic group, 33.54 µm for IPS e.max CAD group, 34.23 µm for IPS Empress CAD, and 33.77 µm for Lava Ultimate group. These values were all within the clinically acceptable range. Additionally, conventional impression technique revealed wider marginal gap formation compared to digital impression technique CEREC Omnicam. The difference was attributed to thermal shrinkage of wax pattern and contraction, and also the expansion of ceramic material might have caused wider marginal gap formation. Hahn et al. [29] evaluated the marginal gap of IPS Empress inlays fabricated with conventional technique before cementation, and the results were lower (47 µm) than the present study. However gap formations are both lower than clinically acceptable values. Guess et al. [30] reported 45 µm marginal gap with conventional technique and similar to the present study CAD/CAM restorations showed lower marginal gap values. CAD/CAM-manufactured restorations produced with previous CEREC systems exhibited significantly larger marginal gap values than acceptable range [31, 32]. Nevertheless, the mean marginal gap values of CAD/CAM-fabricated restorations seem to decrease significantly by developments in systems [33, 34]. Reich et al. [35] reported that hot-pressing technique showed better marginal adaptation compared to CEREC 3D fabricated restorations. On the contrary, Guess et al. [30] found no significant difference between the marginal gap formation of CEREC 3D and hot-pressing technique fabricated restorations. However, similarly to the present study, some authors demonstrated marginal gap values between 36 and 43 µm for CEREC 3 [19, 36, 37]. In the present study, it seems that the powder-free scans of teeth exhibited very low marginal gap values since the stereomicroscope measurements showed a high number of gap formations under 25 µm.
Mean marginal gap values of surfaces showed differences only in Lava Ultimate group, but all values were under 38.48 µm which is very lower than the clinically acceptable value.
In the literature, it is shown that the mean marginal gap values of heat-pressed and CAD/CAM-fabricated restorations increases significantly after cementation [30]. Beschnidt and Strub [38] reported that after cementation of ceramic restorations, marginal gap values increase 13-22 µm whereas Wolfart et al. [39] suggested the change range is between 20 and 40 µm. Therefore, the methodological differences for marginal adaptation measurements do not seem to affect clinically acceptable values in a drastic way.
In the present study, after adhesive cementation, thermal cycling was used to stimulate oral conditions. After simulated aging [30] of the inlay restorations, fracture strength test was applied using a metal sphere of 5 mm diameter to stimulate a molar cusp.
Teeth in posterior regions are subject to functional and parafunctional forces of varying magnitudes and directions [40]. Fractures in this region are a common problem which is affected by restoration type, fabrication methods, material structure, and finishing procedures [41–43].
The fracture strength was determined using a universal testing machine [24]. However, the universal testing machine did not reproduce oblique, torsional, and lateral shearing forces produced during chewing. During fracture strength tests, a single load increase was applied at a constant angle and the same area on the inlay received all forces. Nevertheless, masticatory forces are not constant but multidirectional and affect repeatedly larger surfaces [44]. The “vertical” or “compressive” nature of loading might be an oversimplification of the actual forces applied to the specimens.
The results of this study revealed that there were no significant differences between the fracture strength values of inlay groups; however, there were significant differences between inlay groups and control group. The unprepared molars achieved the highest mean fracture strength value of 3959.00 N. These results correlate with findings of other studies [24, 45]. Consistent with other studies, a large variability of fracture strength values was observed at fracture loading tests [46, 47]. Despite standard selection, storage, preparation of teeth, and milling the inlays in same conditions, it is impossible to control the distribution and length of internal cracks and flaws. IPS Empress glass ceramic has an increased dispersion of leucite caused by heat-pressing, and the high dispersion is expected to improve mechanical properties. Also, a more uniform dispersion of leucite may reduce the susceptibility of glass ceramics [48]. On the other hand, the milling process may cause a multitude of flaws which can act as potential cracking points. In contrast, a study reported a significantly higher fracture strength for CAD/CAM-produced leucite-reinforced glass ceramics than leucite-reinforced (IPS Empress) and lithium disilicate (IPS e.max Press) glass ceramics manufactured by the heat-pressed technique [49]. Similar to the present study, another investigation demonstrated no significant differences in fracture strength results of leucite-reinforced glass ceramics produced with CAD/CAM and heat-pressed technique [19]. Even though IPS e.max CAD has higher biaxial flexural strength values than Lava Ultimate [50], these results are not reflected in fracture strengths of restored teeth with MOD inlays.
Resin restorations are more fracture resistant than ceramics, especially in relatively thinner reconstruction [51]. Although the color stainability is a problem for resin nanoceramic restorations [52], the mechanical properties such as fracture strength, compressive strength, and enamel antagonist wear characteristics have some advantages over glass ceramics [9]. The resin nanoceramic Lava Ultimate elastic modulus [9] is very similar to natural human dentin's elastic modulus [53] values whereas IPS e.max CAD has higher structural behaviors [9]. In the present study, even though materials had different physical properties, inlay groups had similar fracture strength values. Distinctively, Bakeman et al. [54] reported that using a lithium disilicate glass ceramic for restorations significantly improved fracture strength compared to using a leucite-reinforced glass ceramic and ceramic thickness or ceramic materials that had no influence on fracture strength of posterior ceramic restorations. In contrast to our study, Yildiz et al. [55] reported that the fracture strength of heat-pressed ceramics was significantly higher than that of CAD/CAM onlays. The voids and cracks in the restorations produced by heat-pressed technique might have acted as cushioning effect and resulted as higher fracture strength values. In the present study, all restored groups exhibited similar fracture strength, attributed to the dimensions of the inlays produced. Since the occlusal thickness of MOD inlays produced were not larger than 2.8 mm, materials with different physical properties and fabrication methods may have demonstrated similar results.
Harada et al. [56] demonstrated that computer-milled composite and resin nanoceramic restorations showed adequate function for lost tooth structure. Besides, resin nanoceramic blocs showed superior fracture strength compared to composite blocs. They were able to be easily fabricated at a reduced cost and perhaps applied without the need for additional tooth reduction.
The fracture patterns of restored teeth were very consistent in this study. EC, EL, and EP groups showed mostly isolated fractures of the restorations; however, the LU group revealed restoration fractures involving a small tooth portion. All groups demonstrated similar percentages of unrepairable fractures with periodontal involvement.
Recently, CAD/CAM restorations' high success rate, color stability, minimal wear values, and acceptable marginal adaptation [9, 30, 52] allowed them to become a better alternative for direct restorations. Additionally, compared to indirect restorations, they avoid the costs of dental technicians and impression materials [57] and give the opportunity to finish in single appointment. CEREC Omnicam system with a practical use without powder application allows the dentists to apply chair-side ceramic restorations using optical impression of the tooth preparation. Furthermore, digital imaging provides archives for dentists while treating with highly sophisticated dental equipments.
5. Conclusions
Within the limitations of this study, CEREC Omnicam-fabricated inlays showed better marginal adaptation than inlays produced with heat-pressed technique. There was no statistical difference between fracture strength results of inlays fabricated with different materials and methods. Fracture patterns of materials used in this study mostly did not show severe fractures.
Disclosure
The earlier version of the present study was presented as a poster at the 95th General Session and Exhibition of the IADR.
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
- 1.Manhart J., Chen H., Hamm G., Hickel R. Buonocore memorial lecture. Review of the clinical survival of direct and indirect restorations in posterior teeth of the permanent dentition. Operative Dentistry. 2004;29:481–508. [PubMed] [Google Scholar]
- 2.Ausiello P., Ciaramella S., Fabianelli A., et al. Mechanical behavior of bulk direct composite versus block composite and lithium disilicate indirect Class II restorations by CAD-FEM modeling. Dental Materials. 2017;33(6):690–701. doi: 10.1016/j.dental.2017.03.014. [DOI] [PubMed] [Google Scholar]
- 3.Conrad H. J., Seong W. J., Pesun I. J. Current ceramic materials and systems with clinical recommendations: a systematic review. Journal of Prosthetic Dentistry. 2007;98(5):389–404. doi: 10.1016/s0022-3913(07)60124-3. [DOI] [PubMed] [Google Scholar]
- 4.Kelly J. R., Benetti P. Ceramic materials in dentistry: historical evolution and current practice. Australian Dental Journal. 2011;56:84–96. doi: 10.1111/j.1834-7819.2010.01299.x. [DOI] [PubMed] [Google Scholar]
- 5.Rekow E. D., Silva N. R., Coelho P. G., Zhang Y., Guess P., Thompson V. P. Performance of dental ceramics: challenges for improvements. Journal of Dental Research. 2011;90(8):937–952. doi: 10.1177/0022034510391795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Beuer F., Schweiger J., Edelhoff D. Digital dentistry: an overview of recent developments for CAD/CAM generated restorations. British Dental Journal. 2008;204(9):505–511. doi: 10.1038/sj.bdj.2008.350. [DOI] [PubMed] [Google Scholar]
- 7.Bindl A., Luthy H., Mormann W. H. Strength and fracture pattern of monolithic CAD/CAM-generated posterior crowns. Dental Materials. 2006;22(1):29–36. doi: 10.1016/j.dental.2005.02.007. [DOI] [PubMed] [Google Scholar]
- 8.Asai T., Kazama R., Fukushima M., Okiji T. Effect of overglazed and polished surface finishes on the compressive fracture strength of machinable ceramic materials. Dental Materials Journal. 2010;29(6):661–667. doi: 10.4012/dmj.2010-029. [DOI] [PubMed] [Google Scholar]
- 9.Lawson N. C., Bansal R., Burgess J. O. Wear, strength, modulus and hardness of CAD/CAM restorative materials. Dental Materials. 2016;32(11):275–283. doi: 10.1016/j.dental.2016.08.222. [DOI] [PubMed] [Google Scholar]
- 10.Bindl A., Luthy H., Mormann W. H. Fracture load of CAD/CAM-generated slot-inlay FPDs. International Journal of Prosthodontics. 2003;16:653–660. [PubMed] [Google Scholar]
- 11.Costa A., Xavier T., Noritomi P., Saavedra G., Borges A. The influence of elastic modulus of inlay materials on stress distribution and fracture of premolars. Operative Dentistry. 2014;39(4):160–170. doi: 10.2341/13-092-l. [DOI] [PubMed] [Google Scholar]
- 12.Jokstad A. Secondary caries and microleakage. Dental Materials. 2016;32(1):11–25. doi: 10.1016/j.dental.2015.09.006. [DOI] [PubMed] [Google Scholar]
- 13.Larson T. D. The clinical significance of marginal fit. Northwest Dentistry. 2012;91:22–29. [PubMed] [Google Scholar]
- 14.Alghazzawi T. F. Advancements in CAD/CAM technology: options for practical implementation. Journal of Prosthodontic Research. 2016;60(2):72–84. doi: 10.1016/j.jpor.2016.01.003. [DOI] [PubMed] [Google Scholar]
- 15.Lange R. T., Pfeiffer P. Clinical evaluation of ceramic inlays compared to composite restorations. Operative Dentistry. 2009;34(3):263–272. doi: 10.2341/08-95. [DOI] [PubMed] [Google Scholar]
- 16.Morimoto S., Rebello de Sampaio F. B., Braga M. M., Sesma N., Ozcan M. Survival rate of resin and ceramic inlays, onlays, and overlays: a systematic review and meta-analysis. Journal of Dental Research. 2016;95(9):985–994. doi: 10.1177/0022034516652848. [DOI] [PubMed] [Google Scholar]
- 17.Burke F. J. The effect of variations in bonding procedure on fracture resistance of dentin-bonded all-ceramic crowns. Quintessence International. 1995;26:293–300. [PubMed] [Google Scholar]
- 18.Liu X., Fok A., Li H. Influence of restorative material and proximal cavity design on the fracture resistance of MOD inlay restoration. Dental Materials. 2014;30(3):327–333. doi: 10.1016/j.dental.2013.12.006. [DOI] [PubMed] [Google Scholar]
- 19.Keshvad A., Hooshmand T., Asefzadeh F., Khalilinejad F., Alihemmati M., Van Noort R. Marginal gap, internal fit, and fracture load of leucite-reinforced ceramic inlays fabricated by CEREC inLab and hot-pressed techniques. Journal of Prosthodontics. 2011;20(7):535–540. doi: 10.1111/j.1532-849x.2011.00745.x. [DOI] [PubMed] [Google Scholar]
- 20.Ng J., Ruse D., Wyatt C. A comparison of the marginal fit of crowns fabricated with digital and conventional methods. Journal of Prosthetic Dentistry. 2014;112(3):555–560. doi: 10.1016/j.prosdent.2013.12.002. [DOI] [PubMed] [Google Scholar]
- 21.Kurz M., Attin T., Mehl A. Influence of material surface on the scanning error of a powder-free 3D measuring system. Clinical Oral Investigations. 2015;19(8):2035–2043. doi: 10.1007/s00784-015-1440-5. [DOI] [PubMed] [Google Scholar]
- 22.Prudente M. S., Davi L. R., Nabbout K. O., et al. Influence of scanner, powder application, and adjustments on CAD-CAM crown misfit. Journal of Prosthetic Dentistry. 2017;119(3):277–383. doi: 10.1016/j.prosdent.2017.03.024. [DOI] [PubMed] [Google Scholar]
- 23.Ates S. M., Yesil Duymus Z. Influence of tooth preparation design on fitting accuracy of CAD-CAM based restorations. Journal of Esthetic and Restorative Dentistry. 2016;28(4):238–246. doi: 10.1111/jerd.12208. [DOI] [PubMed] [Google Scholar]
- 24.Soares C. J., Martins L. R., Fonseca R. B., Correr-Sobrinho L., Fernandes Neto A. J. Influence of cavity preparation design on fracture resistance of posterior Leucite-reinforced ceramic restorations. Journal of Prosthetic Dentistry. 2006;95:421–429. doi: 10.1016/j.prosdent.2006.03.022. [DOI] [PubMed] [Google Scholar]
- 25.Nawafleh N. A., Mack F., Evans J., Mackay J., Hatamleh M. M. Accuracy and reliability of methods to measure marginal adaptation of crowns and FDPs: a literature review. Journal of Prosthodontics. 2013;22(5):419–428. doi: 10.1111/jopr.12006. [DOI] [PubMed] [Google Scholar]
- 26.da Costa J. B., Pelogia F., Hagedorn B., Ferracane J. L. Evaluation of different methods of optical impression making on the marginal gap of onlays created with CEREC 3D. Operative Dentistry. 2010;35(3):324–329. doi: 10.2341/09-178-l. [DOI] [PubMed] [Google Scholar]
- 27.Weaver J. D., Johnson G. H., Bales D. J. Marginal adaptation of castable ceramic crowns. Journal of Prosthetic Dentistry. 1991;66(6):747–753. doi: 10.1016/0022-3913(91)90408-o. [DOI] [PubMed] [Google Scholar]
- 28.Kramer N., Lohbauer U., Frankenberger R. Adhesive luting of indirect restorations. American Journal of Dentistry. 2000;13:60–76. [PubMed] [Google Scholar]
- 29.Hahn P., Attin T., Grofke M., Hellwig E. Influence of resin cement viscosity on microleakage of ceramic inlays. Dental Materials. 2001;17(3):191–196. doi: 10.1016/s0109-5641(00)00067-1. [DOI] [PubMed] [Google Scholar]
- 30.Guess P. C., Vagkopoulou T., Zhang Y., Wolkewitz M., Strub J. R. Marginal and internal fit of heat pressed versus CAD/CAM fabricated all-ceramic onlays after exposure to thermo-mechanical fatigue. Journal of Dentistry. 2014;42(2):199–209. doi: 10.1016/j.jdent.2013.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.O’Neal S. J., Miracle R. L., Leinfelder K. F. Evaluating interfacial gaps for esthetic inlays. Journal of the American Dental Association. 1993;124(12):48–54. doi: 10.14219/jada.archive.1993.0253. [DOI] [PubMed] [Google Scholar]
- 32.Sjogren G. Marginal and internal fit of four different types of ceramic inlays after luting. An in vitro study. Acta Odontologica Scandinavica. 1995;53(1):242–248. doi: 10.3109/00016359509005940. [DOI] [PubMed] [Google Scholar]
- 33.Romao W., Jr., Miranda W. G., Jr., Cesar P. F., Braga R. R. Correlation between microleakage and cement thickness in three Class II inlay ceramic systems. Operative Dentistry. 2004;29:212–218. [PubMed] [Google Scholar]
- 34.Tsitrou E. A., Northeast S. E., van Noort R. Evaluation of the marginal fit of three margin designs of resin composite crowns using CAD/CAM. Journal of Dentistry. 2007;35(1):68–73. doi: 10.1016/j.jdent.2006.04.008. [DOI] [PubMed] [Google Scholar]
- 35.Reich S., Gozdowski S., Trentzsch L., Frankenberger R., Lohbauer U. Marginal fit of heat-pressed vs. CAD/CAM processed all-ceramic onlays using a milling unit prototype. Operative Dentistry. 2008;33(6):644–650. doi: 10.2341/07-162. [DOI] [PubMed] [Google Scholar]
- 36.Bindl A., Mormann W. H. Marginal and internal fit of all-ceramic CAD/CAM crown-copings on chamfer preparations. Journal of Oral Rehabilitation. 2005;32(6):441–447. doi: 10.1111/j.1365-2842.2005.01446.x. [DOI] [PubMed] [Google Scholar]
- 37.Neves F. D., Prado C. J., Prudente M. S., et al. Micro-computed tomography evaluation of marginal fit of lithium disilicate crowns fabricated by using chairside CAD/CAM systems or the heat-pressing technique. Journal of Prosthetic Dentistry. 2014;112(5):1134–1140. doi: 10.1016/j.prosdent.2014.04.028. [DOI] [PubMed] [Google Scholar]
- 38.Beschnidt S. M., Strub J. R. Evaluation of the marginal accuracy of different all-ceramic crown systems after simulation in the artificial mouth. Journal of Oral Rehabilitation. 1999;26(7):582–593. doi: 10.1046/j.1365-2842.1999.00449.x. [DOI] [PubMed] [Google Scholar]
- 39.Wolfart S., Wegner S. M., Al-Halabi A., Kern M. Clinical evaluation of marginal fit of a new experimental all-ceramic system before and after cementation. International Journal of Periodontics. 2003;16:587–592. [PubMed] [Google Scholar]
- 40.Ausiello P., Rengo S., Davidson C. L., Watts D. C. Stress distributions in adhesively cemented ceramic and resin-composite Class II inlay restorations: a 3D-FEA study. Dental Materials. 2004;20(9):862–872. doi: 10.1016/j.dental.2004.05.001. [DOI] [PubMed] [Google Scholar]
- 41.Attia A., Kern M. Influence of cyclic loading and luting agents on the fracture load of two all-ceramic crown systems. Journal of Prosthetic Dentistry. 2004;92(6):551–556. doi: 10.1016/j.prosdent.2004.09.002. [DOI] [PubMed] [Google Scholar]
- 42.Oh S. C., Dong J. K., Luthy H., Scharer P. Strength and microstructure of IPS Empress 2 glass-ceramic after different treatments. International Journal of Prosthodontics. 2000;13:468–472. [PubMed] [Google Scholar]
- 43.Pallis K., Griggs J. A., Woody R. D., Guillen G. E., Miller A. W. Fracture resistance of three all-ceramic restorative systems for posterior applications. Journal of Prosthetic Dentistry. 2004;91(6):561–569. doi: 10.1016/j.prosdent.2004.03.001. [DOI] [PubMed] [Google Scholar]
- 44.Tasaka A., Kikuchi M., Nakanishi K., Ueda T., Yamashita S., Sakurai K. Psychological stress-relieving effects of chewing–Relationship between masticatory function-related factors and stress-relieving effects. Journal of Prosthodontic Research. 2017;62(1):50–55. doi: 10.1016/j.jpor.2017.05.003. [DOI] [PubMed] [Google Scholar]
- 45.Saridag S., Sevimay M., Pekkan G. Fracture resistance of teeth restored with all-ceramic inlays and onlays: an in vitro study. Operative Dentistry. 2013;38(6):626–634. doi: 10.2341/12-211-l. [DOI] [PubMed] [Google Scholar]
- 46.Attia A., Kern M. Fracture strength of all-ceramic crowns luted using two bonding methods. Journal of Prosthetic Dentistry. 2004;91(3):247–252. doi: 10.1016/j.prosdent.2003.12.005. [DOI] [PubMed] [Google Scholar]
- 47.Yoshinari M., Derand T. Fracture strength of all-ceramic crowns. International Journal of Periodontics. 1994;7:329–338. [PubMed] [Google Scholar]
- 48.Tsitrou E. A., Helvatjoglu-Antoniades M., van Noort R. A preliminary evaluation of the structural integrity and fracture mode of minimally prepared resin bonded CAD/CAM crowns. Journal of Dentistry. 2010;38(1):16–22. doi: 10.1016/j.jdent.2009.07.003. [DOI] [PubMed] [Google Scholar]
- 49.Stappert C. F., Guess P. C., Chitmongkolsuk S., Gerds T., Strub J. R. All-ceramic partial coverage restorations on natural molars. Masticatory fatigue loading and fracture resistance. American Journal of Dentistry. 2007;20:21–26. [PubMed] [Google Scholar]
- 50.Sen N., Us Y. O. Mechanical and optical properties of monolithic CAD-CAM restorative materials. Journal of Prosthetic Dentistry. 2017;119(4):593–599. doi: 10.1016/j.prosdent.2017.06.012. [DOI] [PubMed] [Google Scholar]
- 51.Stawarczyk B., Ender A., Trottmann A., Ozcan M., Fischer J., Hammerle C. H. Load-bearing capacity of CAD/CAM milled polymeric three-unit fixed dental prostheses: effect of aging regimens. Clinical Oral Investigations. 2012;16(6):1669–1677. doi: 10.1007/s00784-011-0670-4. [DOI] [PubMed] [Google Scholar]
- 52.Acar O., Yilmaz B., Altintas S. H., Chandrasekaran I., Johnston W. M. Color stainability of CAD/CAM and nanocomposite resin materials. Journal of Prosthetic Dentistry. 2016;115(1):71–75. doi: 10.1016/j.prosdent.2015.06.014. [DOI] [PubMed] [Google Scholar]
- 53.Chun K., Choi H., Lee J. Comparison of mechanical property and role between enamel and dentin in the human teeth. Journal of Dental Biomechanics. 2014;5:117–121. doi: 10.1177/1758736014520809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Bakeman E. M., Rego N., Chaiyabutr Y., Kois J. C. Influence of ceramic thickness and ceramic materials on fracture resistance of posterior partial coverage restorations. Operative Dentistry. 2015;40(2):211–217. doi: 10.2341/12-459-l. [DOI] [PubMed] [Google Scholar]
- 55.Yildiz C., Vanlioglu B. A., Evren B., Uludamar A., Kulak-Ozkan Y. Fracture resistance of manually and CAD/CAM manufactured ceramic onlays. Journal of Prosthodontics. 2013;22(7):537–542. doi: 10.1111/jopr.12037. [DOI] [PubMed] [Google Scholar]
- 56.Harada A., Nakamura K., Kanno T., et al. Fracture resistance of computer-aided design/computer-aided manufacturing-generated composite resin-based molar crowns. European Journal of Oral Sciences. 2015;123:122–129. doi: 10.1111/eos.12173. [DOI] [PubMed] [Google Scholar]
- 57.Mehl A., Hickel R. Current state of development and perspectives of machine-based production methods for dental restorations. International Journal of Computerized Dentistry. 1999;2:9–35. [PubMed] [Google Scholar]