

Abstract
Low back pain (LBP) is encountered frequently in clinical practice. The superior and the middle cluneal nerves (SCN and MCN) are cutaneous nerves that are purely sensory. They dominate sensation in the lumbar area and the buttocks, and their entrapment around the iliac crest can elicit LBP. The reported incidence of SCN entrapment (SCN-E) in patients with LBP is 1.6%–14%. SCN-E and MCN entrapment (MCN-E) produce leg symptoms in 47%–84% and 82% of LBP patients, respectively. In such patients, pain is exacerbated by lumbar movements, and the symptoms mimic radiculopathy due to lumbar disorder. As patients with failed back surgery or Parkinson disease also report LBP, the differential diagnosis must include those possibilities. The identification of the trigger point at the entrapment site and the disappearance of symptoms after nerve block are diagnostically important. LBP due to SCN-E or MCN-E can be treated less invasively by nerve block and neurolysis. Spinal surgeons treating patients with LBP should consider SCN-E or MCN-E.
Keywords: Superior cluneal nerve, Middle cluneal nerve, Entrapment, Low back pain, Neurolysis, Clinical review
INTRODUCTION
The etiology of low back pain (LBP), a common complaint, is nonspecific in 85% of sufferers [1]. When LBP is due to superior or middle cluneal nerve entrapment (SCN-E or MCN-E), it may be alleviated by nerve block and neurolysis. If SCN-E or MCN-E are not considered in patients scheduled for surgery, the outcome can be failed back surgery syndrome (FBSS).
In 1957, Strong and Davila [2] reported that the SCN and MCN can be entrapped around the iliac crest (Fig. 1). Their success rate was 80% in 30 patients (36 sides) who underwent surgical decompression at the site where the nerves penetrate the thoraco-lumbar fascia. They also reported that SCN-E elicited groin pain and/or leg symptoms in 57% of their patients and that SCN-E is not a simple causative factor in patients with LBP.
Fig. 1.
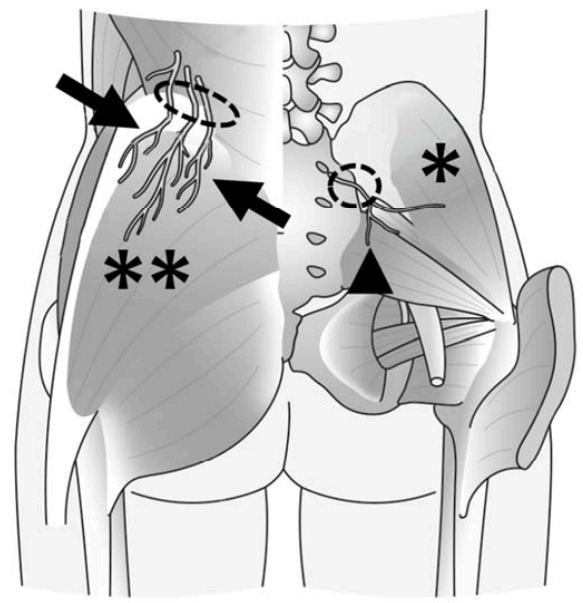
Superior cluneal nerve (SCN) (arrows) and middle cluneal nerve (MCN) (arrowhead). Dotted circles indicate the nerve blockage sites. Adapted from Kim and Isu. Curr Pract Neurosurg In press 2018.36 *Gluteus medius muscle. **Gluteus maximus muscle.
In a series of Japanese LBP patients reported by Takayama and Utsumi in 1961,3 LBP was thought to be attributable to SCN-E. They found that in some of their patients with intractable LBP due to several factors, manual compression at the site where the SCN penetrated the thoraco-lumbar elicited pain around the iliac crest. They addressed LBP due to several lumbar disorders by SCN blockage. Patients who experienced only transient pain relief subsequently underwent neurectomy and in 87% the treatment outcome was good.
As spinal surgeons are not sufficiently aware of the role SCN-E and MCN-E in LBP, we present a review of the literature and review the diagnosis and treatment of this common clinical entity (Tables 1, 2).
Table 1.
Summary of reports on the features and treatment of superior cluneal nerve entrapment
| Study | Study summary |
|---|---|
| Strong and Davila (1952) [2] | The success rate was 80% in 39 operated patients with superior- or middle cluneal nerve entrapment (SCN-E, MCN-E); 57% of patients with SCN-E reported groin pain and/or leg symptoms. |
| Takayama and Utsumi (1961) [3] | Intractable low back pain (LBP) was attributable to SCN-E in 200 Japanese patients. The surgical outcomes were rated ‘good’ in 87% of operated patients. |
| Kuniya et al. (2013) [4] | An anatomical study of the SCN in 109 usable specimens revealed several anatomical variations in the run patterns of SCN branches. |
| Lu et al. (1998) [5] | A study was performed on the relationship between the SCN and the posterior iliac crest and thoracolumbar fascia in 15 cadavers. The osteofibrous tunnel was cited. |
| Maigne and Doursounian (1997) [6] | Among 1,800 patients with LBP, 29 (1.6%) presented with SCN-E. SCN block only was effective in 10 of these patients, the other 19 underwent surgery. After 3.2 years, the surgical treatment outcome was rated as excellent in 13- and as unsatisfactory in 6 patients. |
| Maigne et al. (1989) [7] | An anatomical study of 37 dissected SCNs. The osteofibrous tunnel was cited. |
| Konno et al. (2017) [8] | In 16 cadavers, the SCN originated at the T12 to L5 nerve root. These anatomical findings may explain why patients with SCN-E often suffer leg pain or tingling that mimics sciatica. |
| Tubbs et al. (2010) [9] | The relationship between the SCN and the MCN and the posterior superior iliac spine on 20 cadaveric sides was discussed. |
| Maigne and Maigne (1991) [10] | This anatomical study of 37 dissected SCNs examined the relationship between the SCN and clinical symptoms around the iliac crest. |
| Kuniya et al. (2014) [11] | A prospective study of 834 patients, 113 of whom (13.5%) suffered LBP due to SCN-E; 54 of these (49%) also manifested leg symptoms. SCN block therapy was often useful; 19 patients underwent SCN neurolysis. Complete or almost complete relief of leg symptoms was obtained in 5 of the operated patients. |
| Morimoto et al. (2013) [17] | A detailed description of a successful, less invasive surgical procedure to treat 55 sides with SCN-E by neurolysis under local anesthesia. |
| Ermis et al. (2011) [18] | The quality of life in individuals with LBP was examined. The study included 25 patients with SCN-E, 25 patients with lumbar disc herniation, and 25 healthy subjects. SCN-E was successfully treated by only SCN blocks. Patients with SCN-E scored lower on the mental health section of SF-36 than individuals with lumbar disc herniation. The physical health score and LBP indices were not significantly different. |
| Aly et al. (2001) [19] | Two female teenagers whose condition was diagnosed late. Both had engaged in vigorous sports activities; SCN block was effective in the abatement of their LBP. |
| Speed et al. (2011) [20] | A young professional cricketer with severe LBP due to SCN-E who responded to SCN neurolysis. |
| Berthelot et al. (1996) [21] | LBP due to SCN-E was successfully treated by SCN neurolysis in a 48-year-old woman with LBP. |
| Akbas et al. (2005) [22] | A 62-year-old male with SCN-E diagnosed 8 years after decubitus surgery. His LBP improved by only SCN block. |
| Talu et al. (2000) [23] | Successful treatment of a 55-year-old patient with acute unilateral intractable LBP by only SCN block. |
| Iwamoto et al. (2016) [24] | Severe LBP was alleviated in 8 Parkinson patients by SCN entrapment treatment; 4 patients each underwent SCN block only or SCN neurolysis. The Hoehn-Yahr classification improved in 7 of the 8 patients. |
| Morimoto et al. (2017) [25] | A study of the long-term surgical outcomes (41.3 months) in 79 sides with SCN-E. LBP associated with leg symptoms was reported by 60% of the patients. While all patients experienced symptom improvement, LBP due to SCN-E recurred on 10 sides (13%) and required additional treatment for SCN-E. At the last follow- up visit all patients reported significant improvement. |
| Trescot (2003) [26] | A review of the effectiveness of cryoanalgesia for interventional pain management. SCN-E was reported to mimic radiculopathy due to lumbar disorder. |
| Kim et al. (2017) [27] | LBP and leg pain in patients with paralumbar spine diseases including SCN-E entrapment, can be misdiagnosed as lumbar disc herniation. As treatment based on a misdiagnosis may result in failed back-surgery syndrome, SCN-E must be differentiated from lumbar disc herniation. |
| Chiba et al. (2015) [28] | In 5 patients with intermittent LBP due to SCN-E, SCN neurolysis was successful. SCN-E should not be over-looked as a causal factor in patients in whom walking elicits LBP. |
| Kim et al. (2013) [29] | Indocyanine green (ICG) video angiography was reported to be useful for SCN neurolysis. As the peripheral nerve is supplied from epineurial vessels around the nerve, ICG video angiography facilitated inspection of peripheral nerves such as the SCN, helped to identify the SCN, and could be used to confirm sufficient SCN-E decompression intraoperatively. |
| Kokubo et al. (2017) [30] | Seventeen consecutive elders with LBP and leg pain improved by SCN entrapment and gluteus medius muscle pain treatments. Even very old patients with symptoms due to SCN entrapment can be treated successfully by less-invasive surgery and local block. |
| Kim et al. (2015) [31] | Of 27 patients with LBP due to SCN-E elicited by vertebral compression fractures, 17 responded to SCN block only. The other 10 reported pain alleviation after SCN neurolysis. |
| Matsumoto et al. Forthcoming [32] | Residual symptoms were reported by 27% of patients who had undergone lumbar decompression surgery. They required additional treatments for para-lumbar- and peripheral nerve diseases including SCN-E. |
| Iwamoto et al. (2017) [33] | After lumbar fusion surgery, 8 patients reported LBP. SCN-E was treated by SCN neurolysis and their LBP improved significantly. |
| Yamauchi et al. Forthcoming [34] | Persistent or recurrent LBP and/or leg pain after lumbar discectomy were significantly improved in 13 patients by treating peripheral neuropathy including SCN-E. |
| Kim et al. Forthcoming [35] | SCN neurectomy was performed to treat 7 nerves in patients with intractable LBP. Their symptoms improved after surgery. A review of the pathologic features and the effectiveness of SCN neurectomy suggest that SCN neuropathy elicited LBP via nerve compression. |
Table 2.
Summary of reports on the features and treatment of middle cluneal nerve entrapment
| Study | Study summary |
|---|---|
| Strong and Davila (1957) [2] | The success rate was 80% in 39 operated patients with superior- or middle cluneal nerve entrapment (SCN-E, MCN-E); 57% of patients with SCN-E reported groin pain and/or leg symptoms. |
| Tubbs et al. (2010) [9] | A study of 20 cadaveric sides pointed to a relationship between entrapment syndromes and the SCN, the MCN, and the posterior superior iliac spine. |
| Konno et al. (2017) [12] | A detailed anatomical study of MCN-E in 30 hemipelves. The MCN originated at S1–S4. |
| McGrath et al. (2005) [13] | Anatomical study of 25 sides from cadaveric pelvises examining the relationship between the long posterior sacroiliac ligament (LPSL) and the lateral branches of the dorsal sacral nerve plexus. |
| Aota (2016) [14] | Report on a patient with severe low back pain (LBP) due to MCN-E who underwent neurolysis of the MCN passing under the LPSL. |
| Kim et al. Forthcoming [15] | A Parkinson patient with severe LBP due to MCN-E under the LPSL who was treated by neurolysis under a microscope using local anesthesia. |
| Matsumoto et al. Forthcoming [16] | A report of 11 patients with MCN-E who underwent treatment under a microscope using local anesthesia. Their symptoms improved postoperatively. |
ANATOMY
The SCN and MCN, cutaneous, pure sensory nerves comprised of 4–6 branches that may be connected, dominate in the sensory perception in the lumbar area and buttocks. The SCN originates at the lower thoracic and lumbar posterior nerve root. Its course is superior-medial- to inferior-lateral (Fig. 1). At the iliac crest, it penetrates the thoraco-lumbar fascia 3–4 cm (medial branch) and 7–8 cm (middle branch) from the midline [4-9]. A portion of the SCN passes through the osteofibrous tunnel formed by the thoraco-lumbar fascia and the iliac crest [10]. According to Kuniya et al. [4], on 56% of the 109 sides, at least one SCN passed through the osteofibrous tunnel; the medial-, middle-, and lateral portion of the branch was involved in 39%, 28%, and 13% of cases, respectively. In anatomical studies, SCN-E was detected in 1.8%–13.0% of sampled cases [4,5,7]; in patients subjected to surgery, the incidence of SCN-E at the osteofibrous tunnel was relatively low [11]. Entrapment at that site results in LBP.
The MCN originates at S1–S4 (Fig. 1) [12]. It passes below and sandwiches the long posterior sacroiliac ligament (LPSL) between the posterior superior iliac spine (PSIS) and the posterior inferior iliac spine (PIIS) and courses over the iliac crest to the buttocks [9,12,13]. Although Tubbs et al. [9] claimed that the MCN cannot be entrapped because it runs superficial to the LPSL, others considered MCN-E possible because the lateral branches of the dorsal sacral rami penetrate the LPSL [12,13]. In patients with LBP the putative cause was MCN-E [14-16].
EPIDEMIOLOGY
According to Kuniya et al. [11], the incidence of SCN-E in patients with LBP was unexpectedly high (14%); in 1.6% of LBP patients without sciatic pain SCN-E was involved [6]. The incidence of bilateral SCN-E was 20% and 33% in Japanese studies [3,17]. Females comprised 55%–63% of all patients with SCN-E, however, the role of the habitus, of the spine alignment, and of childbirth in females has not been reported. Although the average age at onset ranged from 55–68 years [6,11,17], young individuals, i.e., soldiers and athletes, with SCN-E have been reported [18-20].
The true incidence of MCN-E is still unknown. Only one comprehensive study has been reported [16]. It involved 11 patients ranging in age from 52–86 years, 8 patients were female and 2 patients presented with bilateral MCN-E. Although the study population was small, its findings suggest similarities between SCN-E and MCN-E.
SYMPTOMS
LBP due to SCN-E is exacerbated by lumbar movement such as extension, bending, rotating, prolonged standing, sitting, walking, and rolling [11,19,21-24]. It produces leg symptoms in 47%–84% of patients2,6,11,25 and mimics radiculopathy due to lumbar disorder [2,3,11,26,27]. SCN-E also elicits intermittent claudication due to worsening LBP during walking [28]. As these symptoms are similar to those of lumbar disease, a differential diagnosis is necessary.
In patients with SCN-E, a Tinel-like sign is detected at the site of nerve penetration i.e. 3–4 cm (medial branch) and 7–8 cm (middle branch) from the midline. Patients experience numbness and radiating pain in the MCN area upon trigger-point compression, a symptom of diagnostic importance. Ermis et al. [18] reported that patients with SCN-E had a lower score on the mental health short form (SF-36) than individuals with lumbar disc herniation although their physical health score and Oswestry disability indices are not significantly different. SCN-E may go undiagnosed for a long time in patients with LBP.
LBP due to MCN-E is also affected by lumbar movement; in 82% of patients it elicited leg symptoms [14-16] and was aggravated by short- and long periods of standing, lumbar flexion, rolling, prolonged sitting, and especially by walking [2,14-16]. As these symptoms are also similar to those of patients with lumbar disease, a differential diagnosis must be made. In the presence of MCN-E, a Tinel-like sign is found 35 mm caudal to the PSIS at a slightly lateral point at the edge of the iliac crest, an area that corresponds with the nerve compression zone [15,16]. Afflicted patients report numbness and radiating pain in the MCN area upon trigger-point compression, a highly important diagnostic finding.
DIAGNOSIS
The correct identification of symptoms is mandatory for the diagnosis of SCN-E and MCN-E (Tables 3, 4). Because the SCN an MCN are very thin (diameter, 1–3 mm), computed tomography (CT)- and magnetic resonance imaging studies are not diagnostically informative. High-resolution CT may help to detect the bony groove at the osteofibrous tunnel [4].
Table 3.
Diagnostic criteria for superior cluneal nerve (SCN) entrapment
| 1 | Low back pain involving the iliac crest and buttocks |
| 2 | Symptoms aggravated by lumbar movement or posture |
| 3 | Trigger point over the posterior iliac crest corresponding to the nerve compression zone |
| 4 | Patients report numbness and radiating pain in the SCN area (Tinel sign) when the trigger point is compressed. |
| 5 | Symptom relief by SCN block at the trigger point |
Table 4.
Diagnostic criteria for middle cluneal nerve (MCN) entrapment
| 1 | Low back pain involving the buttocks |
| 2 | Symptoms exacerbated by lumbar movement or posture |
| 3 | Trigger point 35 mm caudal to the posterior superior iliac spine at a slightly lateral point at the edge of the iliac crest (corresponding to the nerve compression zone) |
| 4 | Patients report numbness and radiating pain in the MCN area (Tinel sign) when the trigger point is compressed |
| 5 | Symptom relief by MCN block at the trigger point |
When SCN-E or MCN-E is suspected in patients with LBP, the detection of a Tinel-like sign at the point of penetration of the thoraco-lumbar fascia and pain disappearance upon nerve blockage are of diagnostic relevance (Fig. 1) [6,14-17].
In the presence of SCN-E, the trigger point is the site where the SCN passes and courses over the iliac crest through the thoraco-lumbar fascia,4-7,17 3–4 cm (medial branch) and 7–8 cm (middle branch) from the midline on the iliac crest. In patients with MCN-E, the trigger point is where the MCN passes and runs over the LPSL between the PSIS and the PIIS on the edge of the iliac crest and it coincides with the entrapment site located 35 mm caudal to the PSIS or slightly more lateral [14-16].
TREATMENT
1. Block Therapy
A specific treatment for SCN-E and MCN-E is nerve blockage above the trigger point. Ermis et al. [18] successfully treated SCN-E in 25-year-old individuals by nerve block alone. They delivered one block in 20-, 2 blocks in 3-, and 3 blocks in 2 instances. Kuniya et al. [11] reported that 68% of their patients experienced LBP relief by more than 50% after 1–3 SCN blocks. On the other hand, according to Maigne and Doursounian [6], only 8 of their 29 patients benefited from 1–3 SCN blocks. These findings suggest that SCN blockage may be sufficient in some patients whose backgrounds are favorable. As others also found that intractable LBP was dramatically improved by only SCN blockage [19,22,23], this treatment method should be considered in patients with intractable LBP due to SCN-E.
While MCN-E can also be addressed by MCN blockage [14-16], information on its success rate is limited.
2. Surgical Treatment
In patients with SCN-E or and MCN-E whose pain is not relieved by conservative treatment with drugs or nerve blockage, surgical release of the entrapment may be effective.
In 1997, Maigne and Doursounian [6] reported the surgical decompression of 2–3 SCNs measuring 1–2 mm in width. They placed a 6-cm skin incision in 19 patients under general anesthesia. In all cases, the SCN-E site coincided with the trigger point. They observed ring-like compression in 15 of their patients, in 7 they noted severe compression. In 2011, Speed et al. [20] documented good surgical outcomes after of SCN decompression at the osteofibrous tunnel. Their patients also underwent the procedure under general anesthesia.
Subsequently, successful, less invasive surgery was performed by Morimoto et al. [17] They treated 34 patients (55 sides) with SCN-E by decompressing the nerve at the penetration site at the thoraco-lumbar fascia under a surgical microscope. The skin incision measured 5 cm and their patients were under local anesthesia. They reported that local anesthesia contributed to identifying the SCN by applying intraoperative nerve stimulation and that successful completion of the procedure was confirmed by intraoperative symptom abatement. Kim et al. [29] who used intraoperative ICG-video angiography during SCN surgery, focused on flow improvement in peripheral blood vessels to ascertain sufficient nerve decompression. Their observations indicate that the blood flow can be monitored under a special microscope after the intravenous injection of ICG.
MCN-E has also been treated by neurolysis under a microscope using local- or general anesthesia [2,14-16]. With the patient in the prone position, a linear skin incision was placed across the trigger point from the PSIS to the caudal side. After splitting the gluteus maximus muscle and opening the fascia, the distal portion of the MCN was explored. As the MCN penetrates the LPSL between the PSIS and the PIIS, it is decompressed by LPSL cutting, resulting in a release of the MCNs to its distal portion.
Because these surgical procedures are less invasive and can be performed under local anesthesia, they can be used even in very old patients with LBP [30]. Postoperatively, patients may be able to walk freely without restrictions or external fixation and may be able to resume their activities of daily living on the next day [15-17,25].
3. Surgical Results
Maigne and Doursounian [6] obtained good surgical outcomes in 13 of 19 patients with SCN-E; their follow-up lasted 3.2 years. Morimoto et al. [17] also reported LBP abatement in 34 operated patients with SCN-E (55 sides); their Roland-Morris Disability Questionnaire (RDQ) and Japanese Orthopedic Association (JOA) scores improved from 14.1 to 7.3 and from 13.9 to 21.1, respectively. In a prospective study of Kuniya et al. [11] operated 19 of 113 patients (17%) with LBP and leg symptoms. Their visual analogue scale fell from74 to 35 and their RDQ score from 15.0 to 7.4. Factors predictive of a good treatment outcome were a symptom duration not exceeding 3 years and the SCN block effectiveness lasting more than 3 days. While these are relatively short-term findings, positive long-term results are expected.
Our group [25] reported the 41.3-month follow-up results of SCN neurolysis (mean, 1.4 branches; range, 1–4 branches). While the symptoms improved in all patients, 13% suffered pain recurrence and underwent repeat surgery. In the second operation, 2.0 additional SCN branches were addressed (range, 1–4). In 20% of these patients, a formerly decompressed SCN was reentrapped; in the others, pain recurrence was attributable to nerves that had not been decompressed during the first procedure. This experience led us to suggest that as many SCN branches as possible should be decompressed in a single procedure to avoid symptom recurrence.
MCN neurolysis is also effective in patients with MCN-E [14-16]. Matsumoto et al. [16] treated 11 patients, encountered no surgical complications, and their symptoms improved postoperatively. Their pain numeric rating scale fell from 7.0 to 1.4, their RDQ from 10.8 to 1.4, and their JOA score rose from 13.7 to 23.6. In that series, we decompressed one MCN branch in 9 patients, 2 branches in 1 patient, and 3 branches in 1 patient. A single patient required reoperation because we failed to explore other MCNs during the first procedure. Based on those findings we suggest that besides the decompressed MCN, surgeons must be on the look-out for other MCNs because 11%–18% of these nerves feature 2 or more branches [12,16]. It is of interest that among the patients who underwent surgery for MCN-E, 3 required additional procedures to treat SCN-E, suggesting that in some patients, both MCN-E and SCN-E may be present simultaneously.
SCN-E/MCN-E AND OTHER LUMBAR DISEASES
1. Lumbar Disease
SCN-E and MCN-E have been diagnosed in the presence of other lumbar diseases such as lumbar spinal canal stenosis, lumbar disc herniation, scoliosis, and vertebral fractures [15-17,25,28,31].
In a series reported by Kuniya et al. [11], SCN-E produced LBP in 27% of patients with a history of vertebral fractures and in 12% of those without a history of vertebral fractures. Kim et al. [31] also treated 27 patients with vertebral fractures and LBP due to SCN-E successfully; 17 responded to only SCN block and the other 10 to SCN neurolysis.
In such cases, LBP may be controlled by less invasive SCN-E treatment without treating the radiological abnormalities.
2. FBSS
SCN-E and MCN-E may result in FBSS. According to Matsumoto et al. [32], 27% of their patients who underwent lumbar decompression surgery reported some residual symptoms that were controlled by additional treatments for para-lumbar- and peripheral nerve diseases. SCN-E had the greatest effect on their symptoms and SCN-E treatment alleviated residual symptoms after lumbar surgery. SCN-E also plays a role in the symptoms experienced after lumbar fusion- and lumbar disc herniation surgery [33,34]. Therefore, SCN-E treatment appears to be a viable option to address LBP and leg symptoms in patients with FBSS.
3. Parkinson Disease
Many patients with Parkinson disease (PD) suffer LBP whose treatment can be difficult. Iwamoto et al. [24] reported 8 patients with PD and SCN-E who suffered severe LBP that was alleviated by SCN-E treatment; 4 each were treated by SCN block only or SCN neurolysis. The Hoehn-Yahr classification improved in 7 of their 8 patients. Moreover, in a PD patient with severe LBP, Kim et al. [15] identified MCN-E. We think that SCN-E and MCN-E may be present in PD patients with LBP because their muscle tonus is increased and overloading of the paravertebral and buttock muscles elicits an abnormal posture.
4. Etiology
The etiology of SCN-E and MCN-E remains to be fully elucidated. The SCN can be entrapped not only in the osteofibrous tunnel in the iliac crest but also at the site where it penetrates the thoraco-lumbar fascia [2,6,11,17,28,35]. SCN entrapment neuropathy has been reported35 and LBP due to SCN-E can be elicited by different lumbar postures and dynamic motions [11,19,21-24]. SCN-E has been found in the presence of diseases that are prone to increase the paravertebral muscle tonus, e.g. PD [24], and in young athletes and soldiers [18-20]. Consequently, SCN-E may be associated with SCN stretching due to lumbar movement and the body posture due to an increase in the paravertebral muscle tonus [2,25].
With respect to the etiology of MCN-E, the MCN may be compressed at the narrow space between the iliac bone and the LPSL, an area around the sacro-iliac joint whose movement, loading, and minor subluxation may result in MCN-E [15,16]. The MCN passes the gluteus maximus muscle and an increase in its tonus may result in MCN stretching during body posture- and motion changes [15,16]. Therefore, there is a relationship between LBP due to MCN-E and various lumbar postures.
CONCLUSION
The incidence of LBP due to SCN-E and MCN-E is unexpectedly high and despite severe symptoms, their diagnosis can be difficult. In some patients, refractory LBP can be addressed by nerve blockage only. Spinal surgeons must rule out SCN-E and MCN-E in patients with LBP.
Footnotes
The authors have nothing to disclose.
REFERENCES
- 1.Deyo RA, Weinstein JN. Low back pain. N Engl J Med. 2001;344:363–70. doi: 10.1056/NEJM200102013440508. [DOI] [PubMed] [Google Scholar]
- 2.Strong EK, Davila JC. The cluneal nerve syndrome; a distinct type of low back pain. Ind Med Surg. 1957;26:417–29. [PubMed] [Google Scholar]
- 3.Takayama T, Utsumi T. Superior cluneal syndrome as a cause of low back pain. (in Japanese) Surgery. 1961;23:885–900. [Google Scholar]
- 4.Kuniya H, Aota Y, Saito T, et al. Anatomical study of superior cluneal nerve entrapment. J Neurosurg Spine. 2013;19:76–80. doi: 10.3171/2013.4.SPINE12683. [DOI] [PubMed] [Google Scholar]
- 5.Lu J, Ebraheim NA, Huntoon M, et al. Anatomic considerations of superior cluneal nerve at posterior iliac crest region. Clin Orthop Relat Res. 1998;347:224–8. [PubMed] [Google Scholar]
- 6.Maigne JY, Doursounian L. Entrapment neuropathy of the medial superior cluneal nerve. Nineteen cases surgically treated, with a minimum of 2 years' follow-up. Spine (Phila Pa 1976) 1997;22:1156–9. doi: 10.1097/00007632-199705150-00017. [DOI] [PubMed] [Google Scholar]
- 7.Maigne JY, Lazareth JP, Guérin Surville H, et al. The lateral cutaneous branches of the dorsal rami of the thoraco-lumbar junction. An anatomical study on 37 dissections. Surg Radiol Anat. 1989;11:289–93. doi: 10.1007/BF02098698. [DOI] [PubMed] [Google Scholar]
- 8.Konno T, Aota Y, Kuniya H, et al. Anatomical etiology of "pseudo-sciatica" from superior cluneal nerve entrapment: a laboratory investigation. J Pain Res. 2017;10:2539–45. doi: 10.2147/JPR.S142115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tubbs RS, Levin MR, Loukas M, et al. Anatomy and landmarks for the superior and middle cluneal nerves: application to posterior iliac crest harvest and entrapment syndromes. J Neurosurg Spine. 2010;13:356–9. doi: 10.3171/2010.3.SPINE09747. [DOI] [PubMed] [Google Scholar]
- 10.Maigne JY, Maigne R. Trigger point of the posterior iliac crest: painful iliolumbar ligament insertion or cutaneous dorsal ramus pain? An anatomic study. Arch Phys Med Rehabil. 1991;72:734–7. [PubMed] [Google Scholar]
- 11.Kuniya H, Aota Y, Kawai T, et al. Prospective study of superior cluneal nerve disorder as a potential cause of low back pain and leg symptoms. J Orthop Surg Res. 2014;9:139. doi: 10.1186/s13018-014-0139-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Konno T, Aota Y, Saito T, et al. Anatomical study of middle cluneal nerve entrapment. J Pain Res. 2017;10:1431–5. doi: 10.2147/JPR.S135382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.McGrath MC, Zhang M. Lateral branches of dorsal sacral nerve plexus and the long posterior sacroiliac ligament. Surg Radiol Anat. 2005;27:327–30. doi: 10.1007/s00276-005-0331-x. [DOI] [PubMed] [Google Scholar]
- 14.Aota Y. Entrapment of middle cluneal nerves as an unknown cause of low back pain. World J Orthop. 2016;7:167–70. doi: 10.5312/wjo.v7.i3.167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kim K, Isu T, Matsumoto J, et al. Low back pain due to middle cluneal nerve entrapment neuropathy. Eur Spine J. 2017 Jul 5; doi: 10.1007/s00586-017-5208-2. [Epub]. https://doi.org/10.1007/s00586-017-5208-2. [DOI] [PubMed] [Google Scholar]
- 16.Matsumoto J, Isu T, Kim K, et al. Surgical treatment of middle cluneal nerve entrapment neuropathy - technical note- J Neurosurg Spine. Forthcoming 2018 doi: 10.3171/2017.12.SPINE17991. [DOI] [PubMed] [Google Scholar]
- 17.Morimoto D, Isu T, Kim K, et al. Surgical treatment of superior cluneal nerve entrapment neuropathy. J Neurosurg Spine. 2013;19:71–5. doi: 10.3171/2013.3.SPINE12420. [DOI] [PubMed] [Google Scholar]
- 18.Ermis MN, Yildirim D, Durakbasa MO, et al. Medial superior cluneal nerve entrapment neuropathy in military personnel; diagnosis and etiologic factors. J Back Musculoskelet Rehabil. 2011;24:137–44. doi: 10.3233/BMR-2011-0287. [DOI] [PubMed] [Google Scholar]
- 19.Aly TA, Tanaka Y, Aizawa T, et al. Medial superior cluneal nerve entrapment neuropathy in teenagers: a report of two cases. Tohoku J Exp Med. 2002;197:229–31. doi: 10.1620/tjem.197.229. [DOI] [PubMed] [Google Scholar]
- 20.Speed S, Sims K, Weinrauch P. Entrapment of the medial branch of the superior cluneal nerve – a previously unrecognized cause of low back pain in cricket fast bowlers. J Med Cases. 2011;2:101–3. [Google Scholar]
- 21.Berthelot JM, Delecrin J, Maugars Y, et al. A potentially underrecognized and treatable cause of chronic back pain: entrapment neuropathy of the cluneal nerves. J Rheumatol. 1996;23:2179–81. [PubMed] [Google Scholar]
- 22.Akbas M, Yegin A, Karsli B. Superior cluneal nerve entrapment eight years after decubitus surgery. Pain Pract. 2005;5:364–6. doi: 10.1111/j.1533-2500.2005.00040.x. [DOI] [PubMed] [Google Scholar]
- 23.Talu GK, Ozyalçin S, Talu U. Superior cluneal nerve entrapment. Reg Anesth Pain Med. 2000;25:648–50. doi: 10.1053/rapm.2000.18189. [DOI] [PubMed] [Google Scholar]
- 24.Iwamoto N, Isu T, Kim K, et al. Low back pain caused by superior cluneal nerve entrapment neuropathy in patients with Parkinson disease. World Neurosurg. 2016;87:250–4. doi: 10.1016/j.wneu.2015.11.043. [DOI] [PubMed] [Google Scholar]
- 25.Morimoto D, Isu T, Kim K, et al. Long-term outcome of surgical treatment for superior cluneal nerve entrapment neuropathy. Spine (Phila Pa 1976) 2017;42:783–8. doi: 10.1097/BRS.0000000000001913. [DOI] [PubMed] [Google Scholar]
- 26.Trescot AM. Cryoanalgesia in interventional pain management. Pain Physician. 2003;6:345–60. [PubMed] [Google Scholar]
- 27.Kim K, Isu T, Morimoto D, et al. Common diseases mimicking lumbar disc herniation and their treatment. Mini-inv Surg. 2017;1:43–51. [Google Scholar]
- 28.Chiba Y, Isu T, Kim K, et al. Association between intermittent low-back pain and superior cluneal nerve entrapment neuropathy. J Neurosurg Spine. 2015:1–5. doi: 10.3171/2015.1.SPINE14173. [DOI] [PubMed] [Google Scholar]
- 29.Kim K, Isu T, Chiba Y, et al. The usefulness of ICG video angiography in the surgical treatment of superior cluneal nerve entrapment neuropathy: technical note. J Neurosurg Spine. 2013;19:624–8. doi: 10.3171/2013.7.SPINE1374. [DOI] [PubMed] [Google Scholar]
- 30.Kokubo R, Kim K, Isu T, et al. Superior cluneal nerve entrapment neuropathy and gluteus medius muscle pain: their effect on very old patients with low back pain. World Neurosurg. 2017;98:132–9. doi: 10.1016/j.wneu.2016.10.096. [DOI] [PubMed] [Google Scholar]
- 31.Kim K, Isu T, Chiba Y, et al. Treatment of low back pain in patients with vertebral compression fractures and superior cluneal nerve entrapment neuropathies. Surg Neurol Int. 2015;6(Suppl 24):S619–21. doi: 10.4103/2152-7806.170455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Matsumoto J, Isu T, Kim K, et al. Impact of additional treatment of paralumbar spine and peripheral nerve diseases after lumbar spine surgery. World Neurosurg. 2018 Feb 2; doi: 10.1016/j.wneu.2018.01.154. [Epub]. pii: S1878-8750(18)30197-9. https://doi.org/10.1016/j.wneu.2018.01.154. [DOI] [PubMed] [Google Scholar]
- 33.Iwamoto N, Isu T, Kim K, et al. Treatment of low back pain elicited by superior cluneal nerve entrapment neuropathy after lumbar fusion surgery. Spine Surg Relat Res. 2017;1:152–7. doi: 10.22603/ssrr.1.2016-0027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Yamauchi T, Kim K, Isu T, et al. Additional treatments on undiagnosed peripheral nerve diseases as a possible solution for failed lumbar disc surgery. Asian Spine J. Forthcoming 2018 doi: 10.31616/asj.2018.12.4.720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kim K, Shimizu J, Isu T, et al. Low back pain due to superior cluneal nerve entrapment - Clinicopathological study. Muscle Nerve. Forthcoming 2018 doi: 10.1002/mus.26007. [DOI] [PubMed] [Google Scholar]
- 36.Kim K, Isu T. Update of peripheral nerve disease treatment (in Japanese) Curr Pract Neurosurg. Forthcoming 2018 [Google Scholar]