

Abstract
Objectives
Recent evidence suggests a role of androgen receptor expression as a prognostic and therapeutic biomarker in endometrial carcinoma, therefore in the present study we aimed to evaluate the frequency of androgen expression in different subtypes of endometrial carcinoma and its association with clinic-pathologic features.
Results
18/89 (20.2%) cases of endometrial carcinoma showed positive androgen receptor expression. On the other hand, low, moderate and high androgen receptor expression was noted in 7/89 (7.9%), 10/89 (11.2%) and 1/89 (1.1%) cases respectively. 15/77 (19.48%) of endometrioid cancers and 3/7 (42.28%) cases of serous carcinoma showed androgen receptor expression; while none of the cases of clear cell or carcinosarcoma revealed androgen receptor expression. No significant association of androgen receptor expression with various clinicopathologic features of endometrial carcinoma was noted. We found that a significant subset of endometrial cancers express androgen receptor especially a serous cancers; therefore we suggest that androgen receptor expression testing should be done in endometrial carcinoma.
Keywords: Androgen receptor, Endometrial cancer, Endometrioid carcinoma, Serous carcinoma, Carcinosarcoma
Introduction
Endometrial carcinoma (EC) is one of the most common gynecological malignancies [1]. There are various histologic subtypes of EC including endometrioid, serous, clear cell, mucinous carcinoma and carcinosarcoma. These have been historically categorized into two major groups (type I and type II cancers) [2]. Endometrioid cancers are typically hormone (estrogen) driven and they are strongly linked to estrogen exposure [3]. On the other hand, recent evidence suggest that serous cancers may also be associated with hormone exposure [4, 5]. Progesterone and related compounds halts estrogen driven proliferation and they can be used in the therapy for low grade endometrioid cancers [6]. Androgens also display anti-proliferative effect in normal endometrium and therefore can theoretically play a role similar to progestins [7]. Recent studies revealed that loss of androgen receptor (AR) expression was found to be with poor survival in EC [8]. On the other hand, AR expression may serve as a potential therapeutic target in EC. Therefore, in the present study we aimed to evaluate the expression of AR in EC in our population and its association with various clinic-pathologic parameters.
Main text
Case selection
Total 103 cases of endometrial carcinoma were selected from records of pathology department archives. All patients underwent surgeries at Liaquat National hospital, Karachi from January 2012 till December 2017 over a period of 6 years. The study was approved by research and ethical review committee of Liaquat National Hospital and informed written consent was taken from all patients at the time of surgery. Hematoxylin and eosin stained slides and paraffin blocks were retrieved and new sections were cut where necessary. Slides of all cases were reviewed by two senior histopathologists and pathologic characteristics like histologic type, tumor grade, T-stage, lymphovascular invasion were evaluated. Moreover, representative tissue blocks of 89 cases were available for AR immunohistochemistry.
Immunohistochemistry
Androgen receptor IHC was performed using DAKO EnVision method using monoclonal mouse anti-human androgen receptor; clone AR441 according to manufacturer’s protocol (dilution of 1:50). Nuclear staining for AR was both quantitatively and qualitatively evaluated. Hormone receptor IHC scoring was based on the Liverpool endometrial steroid quick score with a final score out of 12 calculated by multiplying the proportion of positive tumor nuclei (1–10% = 1, 11–20% = 2, 21–40% = 3, > 40% = 4) by the staining intensity (0 = no staining, 1 = weak, 2 = moderate, 3 = strong). Scores of 1–4 were characterized as low, scores of 5–8 were considered moderate, and scores of 9–12 were classified as high (Fig. 1).
Fig. 1.
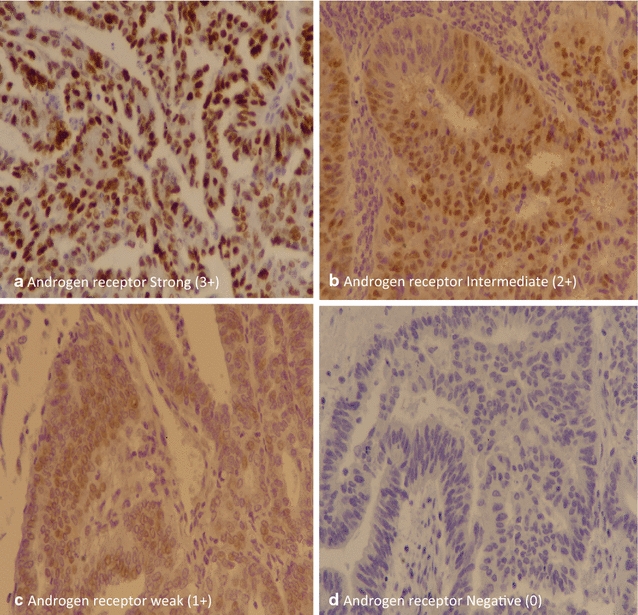
Androgen receptor expression in endometrial carcinoma
Statistical analysis
Statistical package for social sciences (SPSS 21) was used for data compilation and analysis. Mean and standard deviation were calculated for quantitative variables. Frequency and percentage were calculated for qualitative variables. Fisher exact test was applied to determine association. P value ≤ 0.05 was taken as significant.
Demographic patient’s profile
Table 1 shows demographic profile of patients. Mean age of the patients was 56.34 years (+ 9.79). 81.6% patients were post menopausal at the time of presentation. Most common histologic subtype of EC was endometrioid (87/103, 84.5%) followed by serous (9/103, 8.7%) and carcinosarcoma (6/103, 5.8%). Most patients had more than half of myometrial invasion (59/103, 57.3%), while cervical invasion, adnexal involvement and nodal metastasis was present in 26/103 (25.2%), 11/103 (10.7%) and 7/103 (6.8%) cases respectively. 89/103 (86.4%) cases were at stage T1/T2 while 71/103 (68.9%) were correspondingly at FIGO stage 1 (Table 1).
Table 1.
Demographic profile of patients involved in the study (n = 103)
| n (%) | |
|---|---|
| Age (years) | 56.34 ± 9.79 |
| Menopausal status | |
| Pre menopausal | 19 (18.4) |
| Post menopausal | 84 (81.6) |
| Histological type | |
| Endometrioid | 87 (84.5) |
| Serous | 9 (8.7) |
| Clear cell | 1 (1) |
| Carcinosarcoma | 6 (5.8) |
| Grade | |
| Grade I | 41 (39.8) |
| Grade II | 40 (38.8) |
| Grade III | 22 (21.4) |
| Myometrial invasion | |
| Limited to endometrium | 6 (5.8) |
| Less than half of myometrium | 38 (36.9) |
| More than half of myometrium | 59 (57.3) |
| Cervical invasion | |
| Present | 26 (25.2) |
| Absent | 77 (74.8) |
| Adnexal involvement | |
| Present | 11 (10.7) |
| Absent | 92 (89.3) |
| Nodal status | |
| N0 | 96 (93.2) |
| N1 | 6 (5.8) |
| N2 | 1 (1) |
| Lymphovascular invasion | |
| Present | 8 (7.8) |
| Absent | 95 (92.2) |
| T stage | |
| T1 | 72 (69.9) |
| T2 | 17 (16.5) |
| T3 | 10 (9.7) |
| T4 | 4 (3.9) |
| FIGO stage | |
| Stage IA | 40 (38.8) |
| Stage IB | 31 (30.1) |
| Stage II | 18 (17.5) |
| Stage IIIA | 8 (7.8) |
| Stage IIIB | 2 (1.9) |
| Stage IV | 4 (3.9) |
Androgen receptor expression in endometrial carcinoma
18/89 (20.2%) cases of EC showed positive AR expression. On the other hand, low, moderate and high AR expression was noted in 7/89 (7.9%), 10/89 (11.2%) and 1/89 (1.1%) cases respectively. 15/77 (19.48%) of endometrioid cancers and 3/7 (42.28%) cases of serous carcinoma showed AR expression; while none of the cases of clear cell or carcinosarcoma revealed AR expression. No significant association of AR expression with various clinicopathologic features of EC was noted (Table 2).
Table 2.
Association of androgen receptor expression with clinicopathologic features of endometrial carcinoma
| n (%) | P value | |||||
|---|---|---|---|---|---|---|
| Negative (n = 71) | Low (n = 7) | Moderate (n = 10) | High (n = 1) | Total (n = 89) | ||
| Menopausal status | ||||||
| Pre menopausal | 14 (19.7) | 2 (28.6) | 1 (10) | 0 (0) | 17 (19.1) | 0.743 |
| Post menopausal | 57 (80.3) | 5 (71.4) | 9 (90) | 1 (100) | 72 (80.9) | |
| Histological type | ||||||
| Endometrioid | 62 (87.3) | 5 (71.4) | 10 (100) | 0 (0) | 77 (86.5) | 0.117 |
| Serous | 4 (5.6) | 2 (28.6) | 0 (0) | 1 (100) | 7 (7.9) | |
| Clear cell | 1 (1.4) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | |
| Carcinosarcoma | 4 (5.6) | 0 (0) | 0 (0) | 0 (0) | 4 (4.5) | |
| Grade | ||||||
| Grade I | 28 (39.4) | 3 (42.9) | 4 (40) | 0 (0) | 35 (39.3) | 0.293 |
| Grade II | 30 (42.3) | 2 (28.6) | 6 (60) | 0 (0) | 38 (42.7) | |
| Grade III | 13 (18.3) | 2 (28.6) | 0 (0) | 1 (100) | 16 (18) | |
| Myometrial invasion | ||||||
| Limited to endometrium | 4 (5.6) | 0 (0) | 2 (20) | 0 (0) | 6 (6.7) | 0.518 |
| < 1/2 of myometrium | 26 (36.6) | 3 (42.9) | 2 (20) | 0 (0) | 31 (34.8) | |
| > 1/2 of myometrium | 41 (57.7) | 4 (57.1) | 6 (60) | 1 (100) | 52 (58.4) | |
| Cervical invasion | ||||||
| Present | 17 (23.9) | 3 (42.9) | 3 (30) | 0 (0) | 23 (25.8) | 0.581 |
| Absent | 54 (76.1) | 4 (57.1) | 7 (70) | 1 (100) | 66 (74.2) | |
| Nodal status | ||||||
| N0 | 67 (94.4) | 6 (85.7) | 10 (100) | 1 (100) | 84 (94.4) | 0.499 |
| N1 | 3 (4.2) | 1 (14.3) | 0 (0) | 0 (0) | 4 (4.5) | |
| N2 | 1 (1.4) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | |
| Lymphovascular invasion | ||||||
| Present | 5 (7) | 1 (14.3) | 0 (0) | 0 (0) | 6 (6.7) | 0.529 |
| Absent | 66 (93) | 6 (85.7) | 10 (100) | 1 (100) | 83 (93.3) | |
| T stage | ||||||
| T1 | 51 (71.8) | 4 (57.1) | 6 (60) | 1 (100) | 62 (69.7) | 0.607 |
| T2 | 10 (14.1) | 3 (42.9) | 3 (30) | 0 (0) | 16 (18) | |
| T3 | 7 (9.9) | 0 (0) | 1 (10) | 0 (0) | 8 (9) | |
| T4 | 3 (4.2) | 0 (0) | 0 (0) | 0 (0) | 3 (3.4) | |
| FIGO stage | ||||||
| Stage IA | 28 (39.4) | 2 (28.6) | 4 (40) | 0 (0) | 34 (38.2) | 0.853 |
| Stage IB | 22 (31) | 2 (28.6) | 2 (20) | 1 (100) | 27 (30.2) | |
| Stage II | 11 (15.5) | 3 (42.9) | 3 (30) | 0 (0) | 17 (19.1) | |
| Stage IIIA | 6 (8.5) | 0 (0) | 1 (10) | 0 (0) | 7 (7.9) | |
| Stage IIIB | 1 (1.4) | 0 (0) | 0 (0) | 0 (0) | 1 (1.1) | |
| Stage IV | 3 (4.2) | 0 (0) | 0 (0) | 0 (0) | 3 (3.4) | |
Fisher exact test applied
P value ≤ 0.05, considered as significant
In the present study, we aimed to evaluate the AR expression in endometrial cancers and found that a significant proportion of endometrial cancers especially serous cancers exhibit AR expression, that may have clinical and therapeutic significance.
Variable expression of AR was seen in previous studies. Sasaki et al. reported 21% expression of AR [9]; on the other hand, as high as 89% AR expression was detected in another study [10]. Some studies reported degree of differentiation/grade of EC to be inversely associated with AR expression [11]; however, no such association was noted in our study. In the prior studies most of the work focused on endometrioid EC, as it seems to arise as a result of hormonal drive. In a recent study, it was noted that 70% of serous cancers and 50% of carcinosarcoma also show AR expression and high levels of AR expression was noted in half of serous carcinoma [12]. These findings correlate with results of our study as we found 42.8% serous cancers to express AR, while high AR expression was also noted in serous carcinoma. Some studies also revealed association of AR expression with good prognostic features and better disease free survival [13]; however, we didn’t found any significant association of AR expression with various pathologic parameters like tumor stage and nodal metastasis.
From a clinical standpoint, it is important to know if AR IHC expression can identify a subset of EC that can benefit from anti-androgen therapy. Recent evidence supports this speculation that androgen receptor antagonism can be a therapeutic option in EC [14, 15]. This becomes especially important in high grade endometrioid and serous cancers in which endocrine (ER/PR) therapeutic option is not available. In our study we found a high frequency of serous cancers to express AR.
Limitations
One of the major limitations of our study was lack of clinical follow up to elucidate AR expression with disease free survival and low number of cases of non-endometrioid cancer. Therefore, we suggest more large scale studies with clinical follow up to identify role of AR expression as prognostic marker in EC.
Authors’ contributions
AAH and ZFH: main author of manuscript, have made substantial contributions to conception and design of study. AQ, MI and SR: have been involved in requisition of data. NF, AK and MME have been involved in analysis of the data and revision of the manuscript. All authors revise the manuscript. All authors read and approved the final manuscript.
Acknowledgements
We gratefully acknowledge all staff members of Pathology, Liaquat National Hospital, Karachi, Pakistan for their help and cooperation.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
Please contact author, Atif Ali Hashmi (doc_atif2005@yahoo.com) for data requests.
Consent to publish
Not applicable.
Ethical approval and consent to participate
Ethics committee of Liaquat National Hospital, Karachi, Pakistan approved the study. Written informed consent was obtained from the patients for the participation.
Funding
There was no funding available for this manuscript.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- EC
endometrial carcinoma
- AR
androgen receptor
Contributor Information
Atif Ali Hashmi, Email: doc_atif2005@yahoo.com.
Zubaida Fida Hussain, Email: zaib2009@yahoo.com.
Amna Qadri, Email: lilac_docamna@yahoo.com.
Muhammad Irfan, Email: Irfan.zaffar@lnh.edu.pk.
Sahar Ramzan, Email: sahar.ramzan24@hotmail.com.
Naveen Faridi, Email: Naveen.faridi@lnh.edu.pk.
Amir Khan, Email: dramirkhan04@gmail.com.
Muhammad Muzzammil Edhi, Email: Muhammad_edhi@brown.edu.
References
- 1.Miller KD, Siegel RL, Lin CC, et al. Cancer treatment and survivorship statistics, 2016. CA Cancer J Clin. 2016;66:271–289. doi: 10.3322/caac.21349. [DOI] [PubMed] [Google Scholar]
- 2.Suarez AA, Felix AS, Cohn DE. Bokhman redux: endometrial cancer ‘‘types’’ in the 21st century. Gynecol Oncol. 2016;144:243–249. doi: 10.1016/j.ygyno.2016.12.010. [DOI] [PubMed] [Google Scholar]
- 3.Purdie DM, Green AC. Epidemiology of endometrial cancer. Best Pract Res Clin Obstet Gynaecol. 2001;15:341–354. doi: 10.1053/beog.2000.0180. [DOI] [PubMed] [Google Scholar]
- 4.Setiawan VW, Yang HP, Pike MC, et al. Type I and II endometrial cancers: have they different risk factors? J Clin Oncol. 2013;31:2607–2618. doi: 10.1200/JCO.2012.48.2596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Brinton LA, Trabert B, Anderson GL, et al. Serum estrogens and estrogen metabolites and endometrial cancer risk among postmenopausal women. Cancer Epidemiol Biomarkers Prev. 2016;25:1081–1089. doi: 10.1158/1055-9965.EPI-16-0225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Markman M. Hormonal therapy of endometrial cancer. Eur J Cancer. 2005;41:673–675. doi: 10.1016/j.ejca.2004.12.008. [DOI] [PubMed] [Google Scholar]
- 7.Gibson DA, Simitsidellis I, Collins F, et al. Evidence of androgen action in endometrial and ovarian cancers. Endocr Relat Cancer. 2014;21:T203–T218. doi: 10.1530/ERC-13-0551. [DOI] [PubMed] [Google Scholar]
- 8.Kamal AM, Bulmer JN, DeCruze SB, et al. Androgen receptors are acquired by healthy postmenopausal endometrial epithelium and their subsequent loss in endometrial cancer is associated with poor survival. Br J Cancer. 2016;114:688–696. doi: 10.1038/bjc.2016.16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sasaki M, Oh BR, Dharia A, et al. Inactivation of the human androgen receptor gene is associated with CpG hypermethylation in uterine endometrial cancer. Mol Carcinog. 2000;29:59–66. doi: 10.1002/1098-2744(200010)29:2<59::AID-MC2>3.0.CO;2-6. [DOI] [PubMed] [Google Scholar]
- 10.Ito K, Suzuki T, Akahira J, et al. Expression of androgen receptor and 5alpha-reductases in the human normal endometrium and its disorders. Int J Cancer. 2002;99:652–657. doi: 10.1002/ijc.10394. [DOI] [PubMed] [Google Scholar]
- 11.Kato J, Seto T. Correlation of androgen receptors with histological differentiation in human endometrial carcinomas. Acta Obstet Gynecol Scand. 1985;64:209–212. doi: 10.3109/00016348509155114. [DOI] [PubMed] [Google Scholar]
- 12.Zadeh SL, Duska LR, Mills AM. Androgen receptor expression in endometrial carcinoma. Int J Gynecol Pathol. 2018;37(2):167–173. doi: 10.1097/PGP.0000000000000401. [DOI] [PubMed] [Google Scholar]
- 13.Mahdi Z, Abdulfatah E, Pardeshi V, Hassan O, Schultz D, Morris R, Cote ML, Elshaikh MA, Bandyopadhyay S, Ali-Fehmi R. The impact of androgen receptor expression on endometrial carcinoma recurrence and survival. Int J Gynecol Pathol. 2017;36(5):405–411. doi: 10.1097/PGP.0000000000000355. [DOI] [PubMed] [Google Scholar]
- 14.Munoz J, Wheler JJ, Kurzrock R. Androgen receptors beyond prostate cancer: an old marker as a new target. Oncotarget. 2015;6:592–603. doi: 10.18632/oncotarget.2831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tangen IL, Onyango TB, Kopperud R, et al. Androgen receptor as potential therapeutic target in metastatic endometrial cancer. Oncotarget. 2016;7:49289–49298. doi: 10.18632/oncotarget.10334. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Please contact author, Atif Ali Hashmi (doc_atif2005@yahoo.com) for data requests.