

Abstract
Aim and Objective:
This study aims to evaluate the knowledge and attitude of practicing dental health professionals (DHPs) (dentist and dental auxiliaries) toward Middle East Respiratory Syndrome coronavirus (MERS-CoV) in Saudi Arabia.
Materials and Methods:
A cross-sectional descriptive study was undertaken among practicing DHPs in Saudi Arabia. A total of 202 DHPs participated in this study. Knowledge and attitude were assessed using self-administered and pretested questionnaire. The questionnaire was administered online through Survey Monkey® program by sending link to the registered E-mail. Descriptive statistics were performed on demographic data. Mean knowledge and mean attitude scores of DHPs were calculated. Mann–Whitney U-test and Kruskal–Wallis tests were used to disclose the differences between study variables. Chi-square tests and Spearman's correlation tests were applied to find the associations between the variables.
Results:
The study participants showed mean knowledge score of 12.26 ± 2.27 (based on 17 knowledge questions) and attitude score of 8.63 ± 1.68 (based on 10 attitude questions). The spearman's test showed the positive correlation between knowledge and attitude of DHPs about MERS (r = 0.093, P = 0.188). Knowledge gaps were reflected in questions related to the duration of infectivity (47.5%), treatment of MERS (39.6%), reservoir of MERS-CoV (38.1%), availability of vaccination against MERS-CoV (25.2%), the likelihood of infection (24.3%), and the type of MERS-CoV (23.3%). DHPs showed a positive attitude toward adherence to universal precautions given by CDC and WHO (0.94 ± 0.25), active participation infection control program (0.94 ± 0.24), and use of gowns, gloves, mask, and goggles while dealing with MERS-CoV patients (0.97 ± 0.17). Male DHPs showed significantly higher knowledge and positive attitude toward MERS-CoV infection compared to females.
Conclusion:
DHPs participated in this study showed good knowledge and positive attitude toward MERS. However, still few lacunae in the knowledge and attitudes toward MERS-CoV were found requiring extensive educational programs.
Keywords: Attitude, coronavirus, dental professionals, knowledge, middle east respiratory syndrome
INTRODUCTION
Middle East respiratory syndrome (MERS) was first identified from the Kingdom of Saudi Arabia (KSA) in September 2012. It is caused by the novel ß coronavirus MERS-(CoV).[1] Since its first appearance more than 1400 cases reported with mortality of these cases nearly 40% were identified in Saudi Arabia. MERS-CoV transmission within the community is mostly associated with close households and crowded living areas.[2,3] Dromedary camels were recognized as reservoirs of MERS-CoV and close contact with them denotes risk for MERS.[4] Within the health-care setups, disease was observed in outbreak clusters. Persons with middle and old ages with comorbidities found to be at high risk of MERS-CoV infections with higher mortality rate. MERS patients from KSA have shown 4.1 times higher 14-day mortality risk compared to patients from other countries.[5]
The clinical presentation of MERS-CoV infection ranges from asymptomatic or mild respiratory symptoms to severe acute respiratory disease and death. Clinically, MERS-CoV disease manifestations include fever, cough, and shortness of breath. Pneumonia is a common finding, not always present. Gastrointestinal symptoms, including diarrhea, have also been reported.[6]
The existence of asymptomatic and subclinical MERS-CoV infection within the community or in health-care facilities can pose colossal danger to the public health. Due to this, health-care worker's risk of getting infected with MERS-CoV can increase with further possibilities of infection transmission to the patients and other health-care staff. Hence, there is a pressing need to formulate and disseminate comprehensive MERS-CoV awareness program among health-care workers.[7] Ministry of health, Saudi Arabia reacted quickly to counteract this serious MERS-CoV outbreak by developing educational guidelines to health-care workers based on WHO recommendations. These guidelines mainly focused on standard precautions while dealing with patients.
Dental professionals are very frequently exposed to the bioaerosols generated during certain dental treatments. These bioaerosols composed of relatively small particle size that can lead to increased risk of infection among dental professionals.[8] In addition, masks worn by the dental professionals provide limited protection against small particles.[9] Hence, these factors can also be an important part in the transmission of viral infection among dental health professionals (DHPs).
Studies from Saudi Arabia have reported good knowledge and positive attitude of MERS-CoV among health-care workers.[7] Dental students of higher levels have also shown good knowledge of MERS-CoV.[10] Survey of droplet and airborne isolation precautions during MERS outbreak showed that the DHPs had good knowledge and attitude of adhered infection control.[11]
Distinctive work setting makes DHPs to come in close contact with the patients and aerosols during certain dental procedures leading to the heightened risk of MERS-CoV transmission from infected patients.[12] To formulate and implement effective prevention and control strategies of MERS-CoV within the dental field, comprehensive knowledge of the MERS-CoV dynamics is needed. Previous studies that assessed the knowledge and attitude of DHPs were in limited to the dental students, interns, and other staff without much emphasis on registered dental practitioners. Hence, the main aim of this study was to evaluate the knowledge and attitude of practicing DHPs (Dentist and Dental auxiliaries) toward MERS-CoV in Saudi Arabia.
MATERIALS AND METHODS
ETHICAL APPROVAL
The study approved by the Research Center of Riyadh Elm University, Riyadh. The institutional review board approval number is RC/IRB/2016/622.
STUDY DESIGN AND TARGET POPULATION
A cross-sectional descriptive study was undertaken for 2 months (June–July 2017) among DHPs in Saudi Arabia. Study participants were active practicing members registered with Saudi Dental Society in Riyadh, Saudi Arabia. The DHPs including practicing dentist and dental auxiliaries were considered in the study. Through the Saudi dental society office, E-mail addresses of registered dental professionals were retrieved, and all the dental professionals were informed by E-mail that included a link to the survey on Survey Monkey®.
SAMPLE SIZE CALCULATION
Sample size calculation was made using Raosoft online sample size calculator assuming 3000 active SDS members, a response distribution of 50%, while margin of error and confidence intervals of 5% and 95%, respectively. Thus, a required sample of 341 DHPs was arrived.
DATA COLLECTION TOOL
Questionnaire developed by Khan et al.,[7] to assess the knowledge and attitude of healthcare professionals in Saudi Arabia was modified and used in the present study. Four new questions of “bats can serve as reservoir of MERS-CoV, camel to human transmission of MERS-CoV comes from study in KSA, dental patients suffering with MERS-CoV can spread infection in dental clinics, the duration of infectivity for MERS-CoV infection is clearly known” were added to the existing questionnaire making it a total of 17 questions. After modification questionnaire was pilot tested by giving it to 10 DHPs and their opinions regarding the questions were evaluated and amendments were made accordingly while making sure the consistency with reported literature. Questionnaire reliability coefficient obtained by calculating Cronbach's Alfa was found to be adequate (0.72).
QUESTIONNAIRE CONTENT
The questionnaire was divided into four main parts. The first included personal information (age, gender, nationality, category of DHP, qualification, and main work area) of the study participants. The second part explored the sources (Radio, TV, internet, newspaper, pamphlets, etc.), MERS-CoV information. The third part elicited knowledge of DHP toward MERS-CoV by giving correct or incorrect options for every question. The fourth part assessed the DHPs attitude toward MERS-CoV infection through five-point (strongly agree, agree, neutral, disagree, and strongly disagree) Likert scale of agreement.
Knowledge domain evaluated the DHPs regarding reservoir, causes, source of transmission, symptoms, risk group, prevention, and treatment options of MERS-CoV. Knowledge scores ranged from 0 to 17 and cutoff level of <13 were set for poor knowledge and ≥13 for good knowledge.
Attitude evaluation was performed through 10 questions in which responses were recorded on five-point Likert scales. A score of 1 was assigned to strongly agree and agree responses, whereas neutral, strongly disagree, and disagree responses were scored zero for all the items except for item number 10, in which strongly disagree and disagree responses were given a score of 1, and all other responses were scored 0. Hence, an attitude scale ranged from 0 to 10. A mean score of ≥7 was considered as positive attitude while score of lower than 7 was considered for negative attitude.
STATISTICAL ANALYSIS
Normality distribution of the data was checked using Shapiro–Wilk and Kolmogorov–Smirnov tests and data were found to be not normally distributed (P < 0.05).
Descriptive statistics of frequency distribution and percentage was reported. Chi-square test was applied to know the association between study variables and attitude questions. Nonparametric tests of Mann–Whitney U-test and Kruskal–Wallis tests were used to evaluate the significance among the study variables. Further, Spearman's rank correlation coefficient test was applied to evaluate the correlation between knowledge and attitude. P < 0.05 was considered statistically significant for all statistical purposes. All the statistical analysis was performed using IBM-SPSS Version 21 software, Armonk: NY, USA.
RESULTS
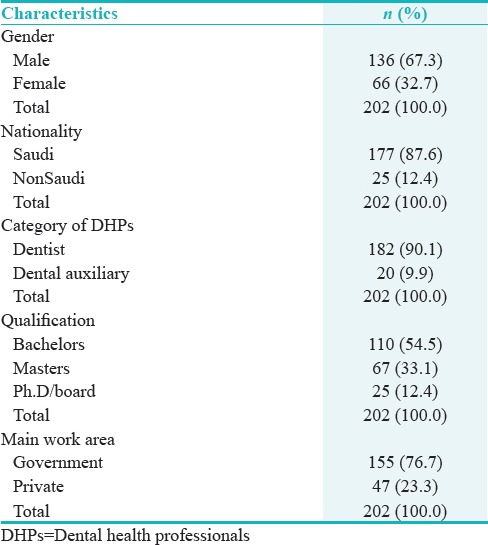
A total of 202 DHPs answered the questionnaire providing the response rate of 59.23%. Most of them were male (67.3%) and belonged DHP with dentist most in number (90.1%). Majority of them were having (54.5%) bachelor's degree in dental profession and (76.7%) working in government institutions. The characteristics of the study participants are shown in Table 1.
Table 1.
Characteristics of the study participants
Television (26.8%) followed by Radio (17.4%), Internet (13%), pamphlets (11.1%), posters (8.9%), Newspapers (7%), continuing education programs (6%), peers (6%), and articles (3.9%) were found to be the sources of information of MERS-CoV among the study participants as depicted in Figure 1.
Figure 1.
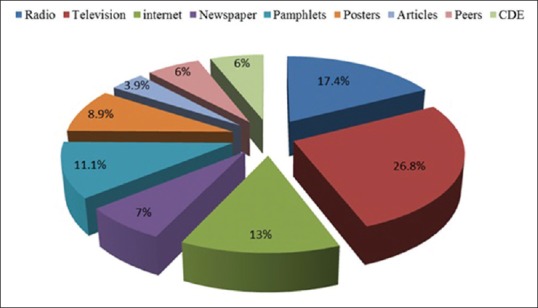
Source of Middle East respiratory syndrome-coronavirus information
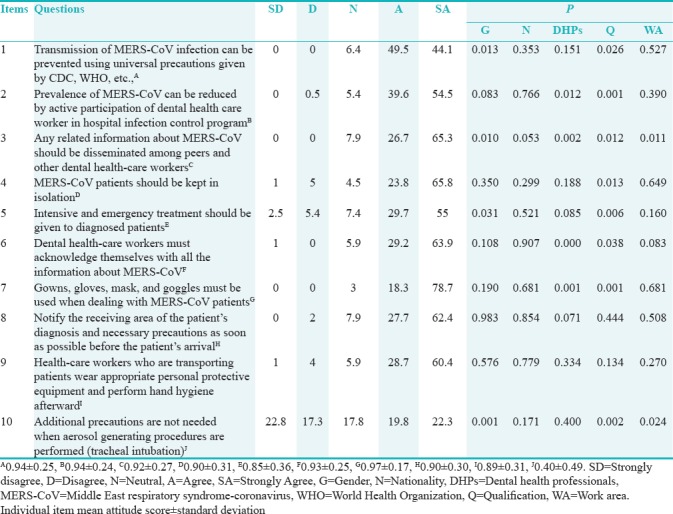
The present situation of MERS knowledge among DHPs is displayed in Table 2. A total of 85 (42.1%) participants exhibited good knowledge while 117 (57.9%) demonstrated poor knowledge of MERs. Poor knowledge was more obvious in questions related to duration of infectivity, treatment, reservoir, vaccination, people more likely to get infected, and the type of virus causing MERS-CoV infection in which the wrong responses rate were 47.5%, 39.6%, 38.1%, 25.2%, 24.3%, and 23.3%, respectively as shown in Table 2. Mean knowledge score of 12.26 ± 2.27, minimum and maximum scores were 5 and 17 respectively were observed among the DHPs as shown in [Figure 2]. Out of 202 respondents, 187 (92.6%) showed a positive attitude toward MERS whereas 15 (7.4%) DHPs showed a negative attitude toward MERS. Mean attitude score of 8.63 ± 1.68, minimum and maximum scores were 0 and 10 respectively were observed among the DHPs Figure 2. Mean attitude of DHPs was found to be lower when enquired about additional precautions are not needed when aerosol-generating procedures are performed (0.40 ± 0.49). On contrary, most of the participants showed high attitude scores toward prevention of MERS-CoV by adhering to universal precautions given by CDC, WHO (0.94 ± 0.25), reduction in prevalence by active participation of dental health-care worker in hospital infection control program (0.94 ± 0.24), dissemination of MERS-CoV information among other DHPs (0.92 ± 0.27), dental health-care workers must acknowledge themselves with all the information about MERS-CoV (0.93 ± 0.25), Gowns, gloves, mask, and goggles must be used when dealing with MERS-CoV patients (0.97 ± 0.17). The results are summarized in Table 3.
Table 2.
Knowledge of Middle East respiratory syndrome among dental health professionals
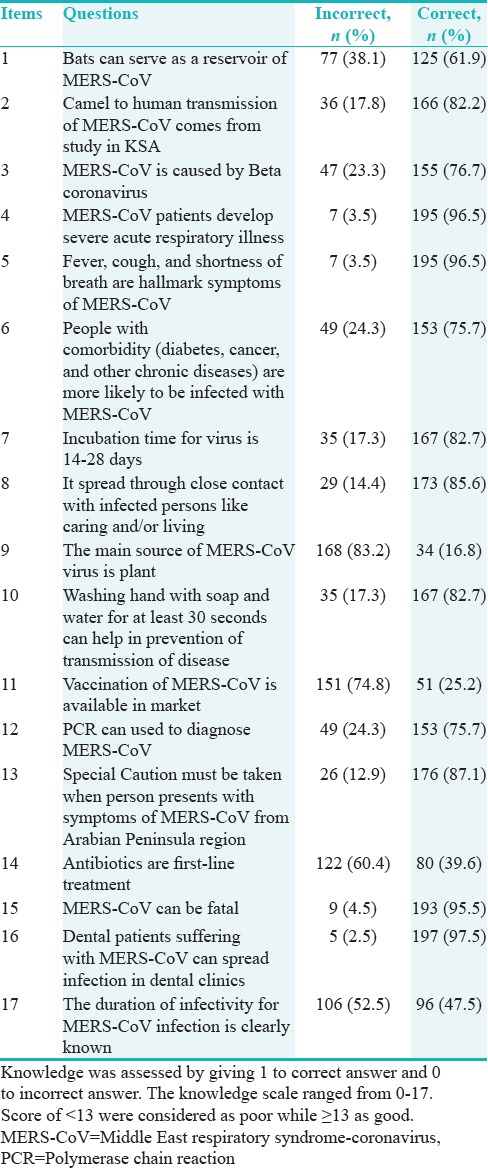
Figure 2.
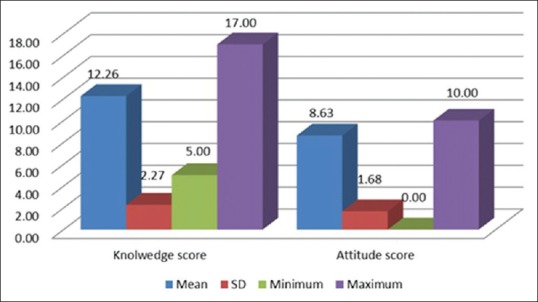
Mean knowledge and attitude scores
Table 3.
Attitude of dental health professionals toward Middle East respiratory syndrome
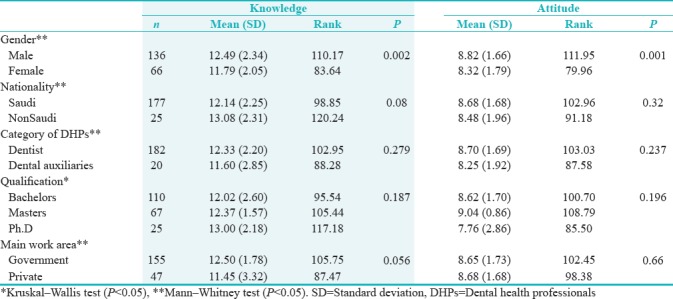
The relationship of demographic characteristics and overall mean knowledge and attitude questions is shown in Table 4. Among the demographic factors considered in the present study gender was the only factor that was significantly associated with mean knowledge and attitude scores. Male DHPs exhibited more knowledge (12.49 ± 2.34 vs. 11.79 ± 2.05, P = 0.002) and positive attitude (8.82 ± 1.66 vs. 8.32 ± 1.79, P = 0.001) toward MERS when compared to the female DHPs. On contrary, nationality, category of DHPs, qualification, and main work area of the DHPs did not show any significant differences in knowledge and attitude toward MERS [Table 4]. The spearman's test showed weak positive correlation between knowledge and attitude of DHPs about MERS (r = 0.093, P = 0.188).
Table 4.
Mean knowledge and attitude scores
DISCUSSION
To the best of our understanding, there are no cases of MERS among dentist is being reported until now. On contrary, there are several reports that have disclosed mortality and morbidity among hospital health-care workers being infected with MERS. In general, health-care workers including DHPs are at increased risk of MERS-CoV infection. Hence, the present study explored the knowledge and attitude of DHPs toward MERS-CoV in Saudi Arabia. The present study findings are compared with physicians and health-care workers due to the limited number publications on DHPs.
The findings of this study displayed good knowledge and positive attitude of DHPs toward MERS-CoV. In the present study, most of the DHPs had received knowledge of MERS from Television. This result is supported by previous studies in which media (TV) was the main source of information about MERS among dental students.[13] On contrary, health-care workers from Al-Qassim mentioned that the source of MERS–CoV information was internet.[7] Radio was the second and internet was the third-most common source for obtaining information about MERS-CoV among DHPs. It is advisable for the DHPs to access the ministry of health website to gain updated knowledge and educational content on MERS-CoV. In addition, published research articles and continuing dental educational programs were the less utilized sources of MERS information among DHPs.
In addition, the majority of the respondents correctly answered to the questions about the possibility of transfer of MERS-CoV infection in dental clinics, followed by symptoms and fatality of MERS-CoV infection, and importance of hand hygiene in the prevention of disease transmission. This discrepancy could be due to the fact that various health educational authorities in Saudi Arabia have focused more on signs and symptoms of MERS-CoV that enhanced the knowledge of health-care workers including DHPs in this area.[14] These findings are similar to that reported in previous studies carried out among dental students[10,13] and hospital health-care workers. It can be assumed that the outbreak of MERS in Saudi Arabia is very recent there is more discussion about it among the health-care workers and society. Scant epidemiologic knowledge in public domain has led to the dependence mostly on the clinical indicators to diagnose MERS-CoV.[15] Hence, the concentration is more toward symptoms and prevention that may have increased the knowledge of MERS among DHPs.[7]
On the other hand, DHPs were less knowledgeable about the duration of the infectivity MERS-CoV as nearly half of the respondents gave false responses. Similarly, DHPs showed lower knowledge toward treatment of MERS-CoV as 39.6% of the DHPs said antibiotics are first-line treatment and one-fourth of the participants said that vaccination of MERS-CoV is available in the market for prevention of MERS-CoV infection. This response is lower than reported among health-care workers from Al-Qassim region.[7] These finding speculative of lacunae in the educational programs that did not clearly informed about the management of MERS-CoV patients.
It is also important to mention the lack of DHPs knowledge about the reservoir of MERS-CoV. About 38.1% of the DHPs answered it wrongly. Although research has revealed that bats could be the potential reservoir of MERS, and only camels may be the main source that spill over the human infection.[16] Hence, there is a need to improve knowledge in this area. In addition, human beings themselves could play a role in the transmission of this disease.[17] Therefore, nearly 97.5% of respondents mentioned that there is a possibility of spread of MERS-CoV infection within the dental operatory by infected patients.
In the present study, mean attitude score was observed within the positive range. Most positive attitude DHPs was toward the use of protective barrier techniques (gloves, Gowns, gloves, mask, and goggles) when dealing with MERS-CoV patients. This response was significantly associated with the category and qualification of DHPs. Dentists having master qualifications showed relatively higher positive attitude to this question compared dental auxiliaries. On contrary, reports have also suggested that the health-care worker's knowledge of newer infectious diseases was poor especially in use of personal protective measures, isolation, and infection control practices. They also found that the health-care worker's self-reported infection control practices were deficient and exaggerated.[18]
This finding is similar to the other reported studies in which DHPs showed a positive attitude toward the use of barrier precautions while dealing with health-care infections.[7] This response was significantly associated with category of DHPs and qualification of DHPs.
On the contrary, DHPs replied poorly when enquired about the need for additional precautions while aerosol-generating procedures were performed. Gender, qualification, and work area of the DHPs were significantly associated with this item. Females, Ph.D degree holders and those DHPs working in private sectors showed relatively more positive attitude in reply to this question. This finding is in contrast with other study conducted among DHPs during outbreak of MERS-CoV.[11]
DHPs responded positively to the question about their active participation in infection control program can reduce the prevalence of MERS-CoV. Category and qualifications of the DHPs were found to be significant association with this item. Dentists having masters or bachelors qualification showed relatively more positive attitude toward this item. This finding is contrary to the attitudes reported among health-care workers from Al-Qassim hospitals.[7]
Male DHPs showed significantly higher mean knowledge and attitude scores as compared to the female counterparts. The relationship between gender of DHPs and attitude could be clarified on the basis that the traditional norms and customary practices of Saudi Arabia allow males to have more interaction and socialization than females. As a result, males have more opportunities to meet with their fellow DHPs having higher qualification and specialization than females. This could have influenced knowledge and attitude toward infection control practices toward MERS.
Dentists, Saudi nationals, those having master qualification and working in private sectors showed more positive attitude toward MERS than their counterparts. Dentists showed more positive attitude toward MERS as compared to dental auxiliaries. This could be due to the fact that the dentist with master's qualification receives profound infection control training, and more chances for professional development when compared to the dental auxiliaries. This result is in agreement with the other reported studies in which physicians showed more positive attitude among other health-care professionals.[19]
In general, gender was the only demographic factor significantly associated with mean knowledge and attitude scores. Other study does not support this association of gender with knowledge and attitude of health professionals.[20] This could be due to traditional and cultural factors of Saudi Arabia, in which males have more exposure to dental health-care sector compared to females. Moreover, the established and lawful framework has endorsed more superiority to male regarding communication with other professionals. It allowed male to travel around the world for symposiums, conferences, and any other health-related activities. All these factors could have influenced the knowledge and attitude of DHPs.[21]
In the present study, positive correlation between knowledge and attitude of DHPs toward MERS confirms the association between knowledge and attitude toward MERS. From this correlation, it can be derived that DHPs with more positive attitude toward MERS are interested to receive more information and increase knowledge of MERS. This can be explained on the basis of theory of Reasoned Action.[22,23]
After careful review of existing literature Al-Tawfiq et al., pointed out toward the understanding of resolve the issues related to the particular host and the particular transmission mode, and identifying the factors that intensify transmission within health-care environments are essential. Movement of MERS-CoV in various body parts requires further investigation. Optimal treatment and predictive analyses are needed to identify occurrence and severity of MERS-CoV.[24] Moreover, institutional preparedness of future prevention of MERS should focus on high alert system to identify source and patients at earliest, build adequate number of airborne isolation chambers, proper training of donning and doffing of health-care workers, adequate number of well-trained health-care workers to care for the patients infected with MERS-CoV and small hospital rooms should be transformed into visitor controlled large rooms.[25]
The main strength of this study is that it reports important health issue that could threaten DHPs in Saudi Arabia, specifically during the times of outbreak of MERS. This study has featured an area where little information is available with regards to dental profession. Findings of the study are helpful in designing effective MERS prevention and control strategies among DHPs. However, some of the limitations of the study include; low response rate from DHPs, sample clustering, cross-sectional nature of the study and possible errors in statistical analysis may prevent generalizability of the results.
Further studies with larger sample size with many categories of DHPs would be needed to identify knowledge and attitudes of DHPs toward MERS. SDS should keep informing updating the MERS-CoV infection control and prevention measures to all its members.
CONCLUSION
Within the limitations of the study, it can be concluded that DHPs participated in the study showed good knowledge and positive attitude toward MERS. Still, there are few lacunae in the knowledge and attitudes requiring improvement. Large-scale health educational programs of MERS should be initiated from professional bodies to fill these lacunae and reinforce the knowledge to influence their behavior positively.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
There are no conflicts of interest.
ACKNOWLEDGMENTS
We would like to thank all the Dental professionals who have participated in this study.
REFERENCES
- 1.Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012;367:1814–20. doi: 10.1056/NEJMoa1211721. [DOI] [PubMed] [Google Scholar]
- 2.CDC. Interim Laboratory Biosafety Guidelines for Handling and Processing Specimens Associated with Middle East Respiratory Syndrome Coronavirus (MERS-CoV) 2015. [Last accessed on 2017 Nov 13]. Available from: http://www.cdc.gov/coronavirus/mers/guidelines-lab-biosafety.html .
- 3.WHO. Laboratory Testing for Novel Coronavirus: Interim Recommendations. 2012. [Last accessed on 2017 Nov 13]. Available from: http://www.who.int/csr/disease/coronavirus_infections/LaboratoryTestingNovelCoronavirus_21Dec12.pdf .
- 4.Dudas G, Carvalho LM, Rambaut A, Bedford T. MERS-coV spillover at the camel-human interface. Elife. 2018;7 doi: 10.7554/eLife.31257. pii: e31257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ahmed A. Estimating survival rates in MERS-CoV patients 14 and 45 days after experiencing symptoms and determining the differences in survival rates by demographic data, disease characteristics and regions: A worldwide study. Epidemiology and Infection. 2017:1–7. doi: 10.1017/S095026881700293X. doi:101017/S095026881700293X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.WHO. Middle East respiratory syndrome coronavirus (MERS-CoV) Summary of Current Situation. WHO. 2017 [Google Scholar]
- 7.Khan MU, Shah S, Ahmad A, Fatokun O. Knowledge and attitude of healthcare workers about middle east respiratory syndrome in multispecialty hospitals of Qassim, Saudi Arabia. BMC Public Health. 2014;14:1281. doi: 10.1186/1471-2458-14-1281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dutil S, Meriaux A, de Latremoille MC, Lazure L, Barbeau J, Duchaine C, et al. Measurement of airborne bacteria and endotoxin generated during dental cleaning. J Occup Environ Hyg. 2009;6:121–30. doi: 10.1080/15459620802633957. [DOI] [PubMed] [Google Scholar]
- 9.Checchi L, Montevecchi M, Moreschi A, Graziosi F, Taddei P, Violante FS, et al. Efficacy of three face masks in preventing inhalation of airborne contaminants in dental practice. J Am Dent Assoc. 2005;136:877–82. doi: 10.14219/jada.archive.2005.0288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kharma MY, Alalwani MS, Amer MF, Tarakji B, Aws G. Assessment of the awareness level of dental students toward middle east respiratory syndrome-coronavirus. J Int Soc Prev Community Dent. 2015;5:163–9. doi: 10.4103/2231-0762.159951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Baseer MA, Ansari SH, AlShamrani SS, Alakras AR, Mahrous R, Alenazi AM, et al. Awareness of droplet and airborne isolation precautions among dental health professionals during the outbreak of corona virus infection in Riyadh city, Saudi Arabia. J Clin Exp Dent. 2016;8:e379–87. doi: 10.4317/jced.52811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Al-Sehaibany FS. Middle east respiratory syndrome in children. Dental considerations. Saudi Med J. 2017;38:339–43. doi: 10.15537/smj.2017.4.15777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Almutairi MA. Awareness about Middle East Respiratory syndrome-corona virus (MERS-CoV) among dental students in Riyadh, Saudi Arabia. Pak Oral Dent J. 2016;36:426–9. [Google Scholar]
- 14.Command and Control Centre, Ministry of Health, Saudi Arabia. Coronavirus Website – Ministry of Health. [Last accessed on 2017 Dec 02]. Available from: http://www.moh.gov.sa/en/CCC/
- 15.Bawazir A, Al-Mazroo E, Jradi H, Ahmed A, Badri M. MERS-CoV infection: Mind the public knowledge gap. J Infect Public Health. 2018;11:89–93. doi: 10.1016/j.jiph.2017.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mohd HA, Al-Tawfiq JA, Memish ZA. Middle East Respiratory syndrome coronavirus (MERS-coV) origin and animal reservoir. Virol J. 2016;13:87. doi: 10.1186/s12985-016-0544-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hawkes N. Camels could be the source of MERS coronavirus, research finds. BMJ. 2013;347:f5052. doi: 10.1136/bmj.f5052. [DOI] [PubMed] [Google Scholar]
- 18.Alsahafi AJ, Cheng AC. Knowledge, attitudes and behaviours of healthcare workers in the Kingdom of Saudi Arabia to MERS coronavirus and other emerging infectious diseases. Int J Environ Res Public Health. 2016;13 doi: 10.3390/ijerph13121214. pii: E1214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Joukar F, Mansour-Ghanaei F, Soati F, Meskinkhoda P. Knowledge levels and attitudes of health care professionals toward patients with hepatitis C infection. World J Gastroenterol. 2012;18:2238–44. doi: 10.3748/wjg.v18.i18.2238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Isara AR, Akpodiete A. Concerns about the knowledge and attitude of multidrug-resistant tuberculosis among health care workers and patients in delta state, Nigeria. Niger J Clin Pract. 2015;18:664–9. doi: 10.4103/1119-3077.154212. [DOI] [PubMed] [Google Scholar]
- 21.Vidyasagar G, Rea DM. Saudi women doctors: Gender and careers within Wahhabic Islam and a “westernised” work culture. Womens Stud Int Forum. 2004;27:261–80. [Google Scholar]
- 22.Fisher WA, Fisher JD, Rye BJ. Understanding and promoting AIDS-preventive behavior: Insights from the theory of reasoned action. Health Psychol. 1995;14:255–64. doi: 10.1037//0278-6133.14.3.255. [DOI] [PubMed] [Google Scholar]
- 23.McEachan R, Taylor N, Harrison R, Lawton R, Gardner P, Conner M, et al. Meta-analysis of the reasoned action approach (RAA) to understanding health behaviors. Ann Behav Med. 2016;50:592–612. doi: 10.1007/s12160-016-9798-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Al-Tawfiq JA, Omrani AS, Memish ZA. Middle East Respiratory syndrome coronavirus: Current situation and travel-associated concerns. Front Med. 2016;10:111–9. doi: 10.1007/s11684-016-0446-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Jeon MH, Kim TH. Institutional preparedness to prevent future Middle East Respiratory syndrome coronavirus-like outbreaks in republic of Korea. Infect Chemother. 2016;48:75–80. doi: 10.3947/ic.2016.48.2.75. [DOI] [PMC free article] [PubMed] [Google Scholar]