

Summary
Burns are the most devastating form of trauma. They are among the most devastating injuries a child can sustain, and coupled with prolonged aggressive and non-aggressive medical and nursing therapies, can result in long-term physical and psychological concerns. Data were obtained from medical records of burned patients treated in our clinic from January 1, 2006 to December 31, 2015. Subsequent details are examined, such as age, gender, etiologic factor, surface of the affected area, depth of burn, localization of injury by region, season when they happened the most, methods of treatment and duration of hospitalization. A total of 1268 patients with burns were admitted to the Clinic of Plastic Surgery Kosovo for treatment between 1 January 2006 and 31 December 2015. During the period of our research, male patients were predominant, accounting for 835 cases (65.85%) of burns while 433 (34.14%) patients were female. The average age in this study was 23 years. Our findings, even with the caveats known to this study, suggest that there is still a high number of patients with burn injury requiring hospital admission.
Keywords: burns, injury, epidemiology, Kosovo
Abstract
Les brûlures sont la forme la plus dévastatrice des traumatismes, parmi les plus délabrantes chez l’enfant et, en raison aussi des la longueurs des soins nécessaires, peuvent être responsables de séquelles physiques et psychiques majeures. Les données ont été retrouvées dans les dossiers des 1 268 patients hospitalisés dans notre unité entre le 1er janvier 2006 et le 31 décembre 2015. L’âge, le sexe, l’agent causal, la surface, la profondeur, la localisation, la saisonnalité, le traitement et la durée d’hospitalisation ont été colligés. Les hommes (835) représentaient 68,85% des patients (433 - 34,14% de femmes). L’âge moyen était de 23 ans. Nos données, avec les limites de ce type d’étude, laissent à penser que le nombre de patients brûlés nécessitant une hospitalisation reste élevé.
Introduction
Burns are the most devastating form of trauma. They are among the most devastating injuries a child can sustain, and coupled with prolonged aggressive and non-aggressive medical and nursing therapies, can result in long-term physical and psychological concerns. Burn trauma is still a significant cause of morbidity and mortality in the world. Burn injury is a major component of unintentional injuries worldwide. It is the leading cause of death from injury in some countries. Burns represent an important health and economic problem in Kosovo and in underdeveloped and developed countries. A huge number of victims each year suffer irreplaceable physical, psychological, mental, economic and social consequences, and even death. Although mortality from burn injury worldwide has been on the decline, it is still a significant contributor to morbidity and mortality in Kosovo. Developments that have helped to reduce mortality in the advanced world include promulgation of prevention program advances in pre-hospital care and management in intensive care. In addition, the absence of adequate facilities and trained medical personnel for treatment and rehabilitation contributes to increasing morbidity and mortality. Burn devastates the individual as well as the community. The physical and psychological scars take a long time to recede. The primary objective of this study is to provide an epidemiological description of burns in Kosovo in the 10-year period from January 1, 2006 to December 31, 2015, the incidence and cause of burns, burn size in terms of percentage of total body surface area (TBSA), depth of injuries, methods of treatment, duration of hospitalization, location of burns by region, season, burns analysis by year from 2006 to 2015 and possible differences.
Materials and methods
Data were obtained from medical records of burn patients treated in our burn unit between January 1, 2006 and December 31, 2015. This is a retrospective study where subsequent details are examined, such as age, gender, etiologic factor, surface of the affected area, depth of burn, localization of the injury by region, season when they happened the most, methods of treatment and duration of hospitalization.
We have not included in this study severely injured patients with massive burns who were admitted to the ICU and referred abroad for treatment or those with fatal burns. Electrical and chemical burns, second degree burns with TBSA <15%, third and fourth degree burns with TBSA <3%, burns on neurogenic areas like the face, palms and soles, inguinal region, patients with critical illnesses and those over 60 years or under 2 years old were admitted and treated in our semi-intensive department, while all others who exceeded these criteria were admitted to the ICU.
The average time between injury and initial evaluation (hospitalization) was 2 ± 4,6h. Patients were resuscitated using Parkland formula for the initial dehydration period. Surgical treatment included bulectomy, escharotomy, fasciotomy for circumferential burns and those who developed compartment syndrome, debridement of devitalised tissues, tangential necrotomy and bandaging of the affected area
Results
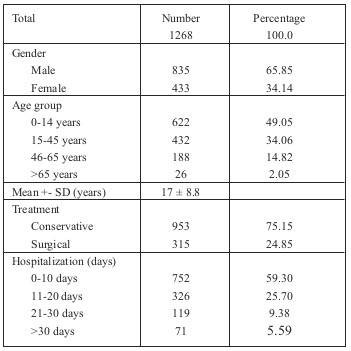
A total of 1268 patients with burns were admitted to the Clinic of Plastic Surgery Kosovo for treatment between January 1, 2006 and December 31, 2015.
From the data we collected during the period of study, the most affected gender was men with 835 cases (65.85%) compared to 433 (34.14%) women patients (Table I). Regarding age, the most affected age group with burn related injuries was the 0-14 group with 623 cases (49.13%) followed by the 14- 45 group with 431 cases (33.99%), the 46-65 group with 188 cases (14.82%) and the over 65-year-olds with 26 cases (2.05%). Average age was 23 ± 17.53 years.
Table I.
Median TBSA burned was determined based on medical records and found to be 18.8% with a range of 1-70%. As regards cause of the burn injury, we had 662 patients (52.20% cases) with thermal injuries, 367 cases (28.94%) with burns caused by flame, 211 cases (16.64%) with electrical burns and 28 cases (2.20%) with burns caused by chemical substances (Fig. 1).
Fig. 1.
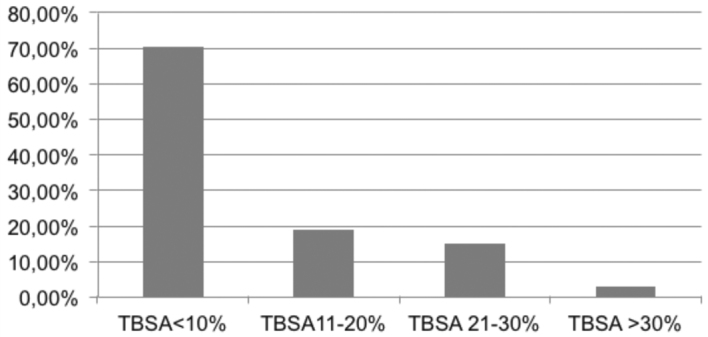
Out of 1268 cases, 939 (74.05%) had superficial and partial thickness burns, 224 patients (17.66%) had full thickness burns, and 105 (8.28%) patients had fourth degree burns involving the muscles and bones (Fig. 2). A total of 953 (75.15%) patients required conservative treatment only, 315 (24.85%) patients underwent surgical intervention for necrotomy and skin graft, and 43 patients with fourth degree burns involving the muscles and bones underwent amputations in different parts of both extremities. A small group of 14 patients (1.01%) refused surgical treatment. Regarding TBSA, we had 895 (70.58%) cases with burns up to 10% TBSA, 239 (18.84%) patients between 11-20%, 116 (14.9%) patients between 21-30% and 39 (3.07%) patients with TBSA over 30% who were initially treated in the ICU then transferred to our unit (Fig. 3). From the data we obtained, we found that there is no correlation between depth of burn and TBSA.
Fig. 2.
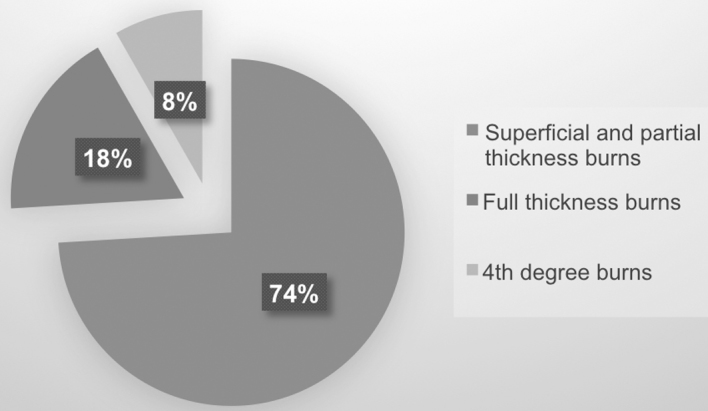
Fig. 3.
If we compare the monthly incidence of burn-related injuries, there is a higher incidence during the late spring and summer, June with 131 cases (10.31%), and a lower incidence in November with 84 cases (6.62%)
Distribution of burns by localization shows that the head (the face) and upper extremities were the most affected parts with 349 (27.52%) cases, and the least affected area was the body with 13 (1.02%) cases.
Type of injury was in many cases related to profession. Most thermal injuries occurred at home for 782 (61.67%) patients, where the causative agent was hot liquid, whereas 474 (37.38%) cases were injured in the workplace where the causative agent was flame and electrical power. Duration of treatment ranged from 1-68 days. Mean duration of hospitalization was 11.3 days.
Discussion
Burn injury is an important cause of hospital admission. Age and sex are important epidemiological determinants for injuries, and our study identifies young age and male gender as being at greater risk. These results correlate with studies conducted in Israel and Turkey.1 Home is the primary venue for burns and hot water is the main cause. The majority of burns are small (<10% of TBSA). Males accounted for 829 cases (65.37%) while 427 (33.67%) patients were females. This data correlates with most reported studies.1,2,3,4,5,6,7
A total of 622 (49.05%) patients with burns were 0-14 years old. Young people under twenty was the next age group most commonly involved. Lack of parental supervision and awareness of surroundings have been identified as reasons for the high incidence of burns in children.8 These findings were similar to those reported in Turkey and Israel, but different to other reports in China, India and African countries.9,10 The average age in this study was 23 years.
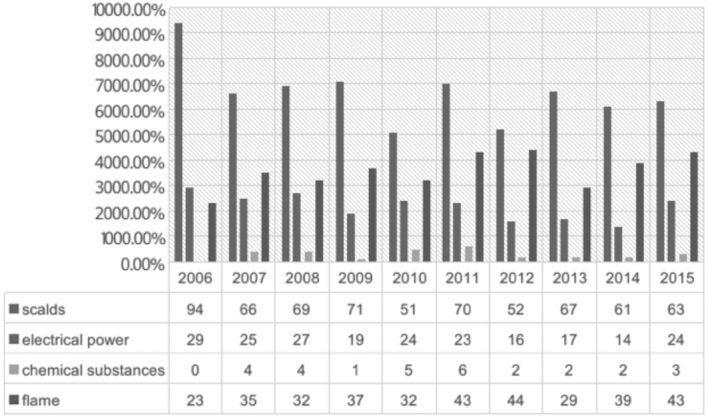
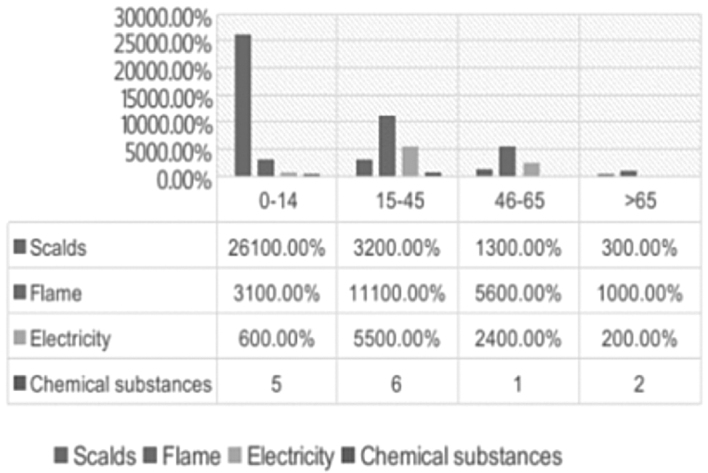
Regarding etiology, scalding was the most common type of burn with 662 cases (52.20%). Scald injuries were more frequent in children under 3 years old, and were caused by hot tea, hot coffee, soup or hot water 11,12,13,14,15 (Fig.4).
Fig. 4.
Results of this research identify the direction that future prevention programs should take: specifically, educating the masses to pay more attention when caring for toddlers and young children. This is a problem not only in under-developed countries. We see this kind of injury in advanced societies too. Data show that in these countries the dominant cause of thermal injuries is hot liquid like tea, coffee, milk or soup.
In adults, the most common etiological factors of burns are flame-fire, electricity and chemical substances.16,17,18 We had 367 (28.94%) cases where the causative agent was flame-fire, most commonly gas flame which is often used for cooking and as a heating agent in Kosovo.19,20,21,22
Over ten years, we had 211 (16.64%) patients with electrical burns. Most of them were electrical engineers who had suffered injuries in the workplace, injuries caused by errors in electrical circuits etc.
Electrical burns that occurred in the workplace or at home were more often in vanished buildings or in houses near high voltage lines. It is not necessary to have direct contact with the line to cause combustion. Problems like these should be solved by the local authorities that license the new settlements, taking into account their location, which must be at a sufficient distance to prevent possible injury.
The management of burns is both capital- and labour-intensive. Poverty therefore continues to be a major impediment to caring for burn patients. The absence of a broad-based health insurance scheme means that burn victims have to pay for services out of their own pocket, and inability to pay has been associated with a worse outcome.
This research shows that there is no significant difference with other research conducted previously in Kosovo. The most affected age group in our country is children under 15 years old.
Conclusion
for inpatient care of just over 10,000 pediatric burn injured patients during the period 1994 to 2003. Our findings, even with the caveats known to this study, suggest that there has been a clear reduction in the number of patients with burn injury requiring hospital admission. We believe that this is due to safety initiatives to prevent burn injuries, as well as to improvements in the treatment of burns and hospital admission procedures. Therefore, educational efforts for prevention should be the keystone to minimizing the incidence of childhood burn injuries.
In summary, this report describes the epidemiological situation for inpatient care of 1268 burn injured patients during the period 2006-2016. Our findings, even with the caveats known to this study, suggest that there is still a high number of patients with burn injury requiring hospital admission. We believe that this is due to a lack of public health campaigns to educate the masses. Therefore, educational programs in schools, nurseries, community clinics and day care centres to promote prevention should be the keystone to minimizing the incidence of childhood and adult burn injuries.
We believe that updated burn data conveying a realistic picture and objective analysis of burn injuries in Kosovo should be published every year. This kind of database can provide the authorities with an up-to-date status of burns, and could be the basis for future prevention programs.
References
- 1.World Health Organization. Geneva: 2008. [Accessed on April 02, 2010]. World Health Organization: The Global Burden of Disease: 2004 Update.www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf [Google Scholar]
- 2.Hamayun M.HZ, Khan D, Khalid Aziz A. Epidemiology of burn injuries: mortality and morbidity in Hazara, 2013. http://www.pjmhsonline.com/epidemiology_of _burn_ injuries.htm [Google Scholar]
- 3.American Burn Association: Fact Sheet. Burn Incidence and Treatment in the United States. 2016 [Google Scholar]
- 4.Olaitan PB. Burns and scalds - epidemiology and prevention in a developing country. NJM. 2005;14(1):9–16. doi: 10.4314/njm.v14i1.37128. [DOI] [PubMed] [Google Scholar]
- 5.Forjuoh SN. Burns in low- and middle-income countries: a review of available literature on descriptive epidemiology, risk factors, treatment, and prevention. Burns. 2006;32:529. doi: 10.1016/j.burns.2006.04.002. [DOI] [PubMed] [Google Scholar]
- 6.Peck MD, Kruger GE, van der Merwe AE. Burns and fires from non-electric domestic appliances in low and middle-income countries Part I. The scope of the problem. Burns. 2008;34:303. doi: 10.1016/j.burns.2007.08.014. [DOI] [PubMed] [Google Scholar]
- 7.About Burns. How to prevent burn injuries. [Accessed on June 9, 2010];UC San Diego Health System Specialties & Programs. health.ucsd.edu/specialties/burn/about.htm [Google Scholar]
- 8.Haik J, Liran A, Tessone A, Givon A. Israeli Trauma Group: Burns in Israel: demographic, etiologic and clinical trends, 1997-2003. [PubMed] [Google Scholar]
- 9.Van der Merwe AE, Steenkamp WC. Prevention of burns in developing countries. Ann Burns and Fire Disasters. 2012;25(4):188–191. [PMC free article] [PubMed] [Google Scholar]
- 10.Ringo Y, Chilonga K. Burns at KCMC: Epidemiology, presentation, management and treatment outcome. Burns. 2014;40(5):1024–1029. doi: 10.1016/j.burns.2013.10.019. [DOI] [PubMed] [Google Scholar]
- 11.Ahuja RB, Bhattacharya S. Burns in the developing world and burn disasters. BMJ. 2004;329:447. doi: 10.1136/bmj.329.7463.447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Anlatici R, Ozerdem OR, Dalay C, Kesiktaş E. A retrospective analysis of 1083 Turkish patients with serious burns. Burns. 2002;28:231–237. doi: 10.1016/s0305-4179(01)00095-x. [DOI] [PubMed] [Google Scholar]
- 13.Burns in Sweden: an analysis of 24,538 cases during the period 1987-2004. Burns. 2007;33(1):31–36. doi: 10.1016/j.burns.2006.10.002. [DOI] [PubMed] [Google Scholar]
- 14.Peck M, Molnar J, Swart D. global plan for burn prevention and care. Bull World Health Organ. 2009;87:802–803. doi: 10.2471/BLT.08.059733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Golshan A, Patel C, Hyder AA. A systematic review of the epidemiology of unintentional burn injuries in South Asia. J Public Health (Oxf) 2013;35:384–396. doi: 10.1093/pubmed/fds102. [DOI] [PubMed] [Google Scholar]
- 16.Koushyar H, Amouzgar M, Shakeri M. The epidemiology of burns in Mashhad Imam Reza Burn Center (MIRBC). Horizon Med Sci. 2004;10:43–50. [Google Scholar]
- 17.Wasiak J, Spinks A, Ashby K, Clapperton A. The epidemiology of burn injuries in an Australian setting, 2000-2006. Burns. 2009;35(8):1124–1132. doi: 10.1016/j.burns.2009.04.016. [DOI] [PubMed] [Google Scholar]
- 18.Spinks A, Wasiak J, Cleland H, Beben N, Macpherson AK. Ten-Year epidemiological study of pediatric burns in Canada. J Burn Care Res. 2008;29(3):482–488. doi: 10.1097/BCR.0b013e3181776ed9. [DOI] [PubMed] [Google Scholar]
- 19.Duci SB, Arifi HM, Selmani ME, Gashi S. Pediatric burns in University Clinical Center of Kosovo from 2005 to 2010. Burns. 2014;14:125–129. doi: 10.1016/j.burns.2014.04.002. [DOI] [PubMed] [Google Scholar]
- 20.Arifi HM, Duci SB, Zatriqi VK, Ahmeti HR. retrospective study of 572 patients with hand burns treated at the Department of Plastic Surgery Kosovo during the period 2000-2010. Int J Burns Trauma. 2014;4(1):7–13. [PMC free article] [PubMed] [Google Scholar]
- 21.Duci SB, Arifi HM, Selmani ME, Mekaj AY. retrospective study of 69 patients admitted at the intensive care unit university Clinical Center of Kosovo during the period 2008-2012. Indian J Burns. 2014;22:88–92. [Google Scholar]
- 22.Arifi H, Zatriqi KV, Zatriqi S, Ahmeti H, Muqa S. Epidemiological and therapeutic aspects of burns in children in the territory of Kosovo. Ann Burns Fire Disasters. 2004;17(4):181–184. [Google Scholar]