

Abstract
Background
Many U.S. health departments have implemented Data to Care interventions, which use HIV surveillance data to identify persons who are inadequately engaged in HIV medical care and assist them with care re-engagment, but the effectiveness of this strategy is uncertain.
Methods
We conducted a stepped wedge cluster randomized evaluation of a Data to Care intervention in King County, Washington 2011–2014. Persons diagnosed with HIV for ≥6 months were eligible based on one of two criteria: 1) VL >500 copies/mL and CD4 <350 cells/μL at last report in the past 12 months or 2) no CD4 or viral load (VL) reported to the health department for ≥12 months. The intervention included medical provider contact, patient contact, and a structured individual interview. Health deparment staff assisted patients with reengagement using health systems navigation, brief counseling, and referral to support services. We clustered all eligible cases in the county by the last known medical provider and randomized the order of clusters for intervention, creating contemporaneous intervention and control periods (cases in later clusters contributed person-time to the control period at the same time that cases in earlier clusters contributed person-time to the intervention period). We compared the time to viral suppression (VL<200 copies/mL) for individuals during intervention vs. control periods using a Cox Proportional Hazards model.
Results
We identified 997 persons [intention to treat (ITT)], 18% of whom had moved or died. Of the remaining 822 (modified ITT), 161 (20%) had an undetectable VL reported before contact and 164 (20%) completed the individual interview. The hazard ratio (HR) for time to viral suppression did not differ between the intervention and control periods in ITT [HR 1.21 (95% CI: 0.85–1.71)] or modified ITT [HR 1.18 (95% CI: 0.83–1.68)] analysis.
Conclusion
The Data to Care intervention did not impact time to viral suppression.
Keywords: HIV Care Continuum, Retention in Care, Data to Care, HIV Surveillance, Cluster Randomized Trial
INTRODUCTION
Antiretroviral therapy decreases HIV transmission and improves the health of persons living with HIV (PLWH).1,2 Increasing the percentage of PLWH who are engaged in medical care and virally suppressed are centerpieces of the U.S. National HIV/AIDS Strategy.3 In most states in the U.S., laboratories report the results of CD4 count and HIV RNA [viral load (VL)] tests to health departments.4 The Centers for Disease Control and Prevention (CDC) encourage health departments to use HIV surveillance data to identify PLWH who have had gaps in care or are not virally suppressed and work to engage these individuals in HIV care and treatment. 5,6 However, the effectiveness of this strategy, called “Data to Care,” is unknown. The rationale for it is strong, but at least three factors could blunt the impact of this approach. First, inaccurate surveillance data could limit health department’s ability to identify out-of-care persons. A lack of laboratory reports often indicates that an individual has moved out of the surveillance jurisdiction rather than disengaged from care.7 Second, many PLWH have periods of care disengagement interspersed with periods of engagement and reengage in care without intervention. Third, little evidence is available to guide the process of reengaging a person who has disengaged from HIV care.8 Most health departments use an approach that blends traditional public health case investigation with brief counseling, patient navigation, or case management.9–17 Although some jusridictions have reported outcomes from their Data to Care programs,10,12–15,17 no controlled study has been published.
We implemented a Data to Care intervention in Seattle-King County, WA in 2011.6,18,19 In the Care and Antiretroviral Promotion Program (CAPP), health department disease intervention specialists (DIS) use surveillance data to identify persons who appear to be poorly engaged in HIV care, contact the last known medical provider for each case, contact patients, and attempt to reengage persons in care using structured brief counseling, health systems navigation, and referral to support services. DIS are front-line public health workers who typically work with persons who are infected with or have been exposed to HIV or other sexually transmitted infections to ensure access to treatment.
The objective of this program evaluation was to determine the effectiveness of the Data to Care strategy in Seattle & King County. To do this, we instituted and evaluated CAPP using a stepped wedge cluster design. In stepped wedge cluster randomized trials investigators randomly assign the order in which groups of persons (“clusters”) receive an intervention.20,21 The stepped wedge approach creates contemporaneous intervention and control periods: clusters initiated later contribute person-time to the control period at the same time that clusters initiated earlier contribute person-time to the intervention period. This method facilitates more rigorous evaluation than comparison of post-intervention outcomes to pre-intervention outcomes because it controls for secular trends. It is well-suited to evaluation of public health interventions because it does not require withholding the intervention from any group. In situations where it is not possible to deploy the intervention to all eligible persons simultaneously, such as our countywide Data to Care intervention, randomizing the order of intervention initiation is a pragmatic way to facilitate evaluation. The cluster approach provides a means to decrease “contamination” between intervention and control arms that could occur if individuals, rather than clusters, were randomized. Medical provider communication was a key element of our Data to Care approach. If medical providers attempted to re-engage their patients who were poorly engaged in care, the intervention effect could be obscured with individual patient randomization. Thus, we grouped cases into clusters defined by their last known medical provider to minimize contamination between intervention and control periods. The primary outcome of our analysis, time to viral suppression, pertained to individual PLWH.
METHODS
Prior to implementing the CAPP intervention, we conducted formative work to obtain feedback on and adapt the intervention. This included in-depth qualitative interviews with PLWH and HIV medical providers,19 and presentations to provider and community groups. The program was implemented and evaluated for a public health purpose and was not human subjects research requiring IRB oversight.
Participants and Clusters
We identified eligible cases from the King County enhanced HIV/AIDS Registry System (eHARS) in Washington State, regardless of the jurisdiction of diagnosis, who had been diagnosed with HIV for ≥6 months. Persons found to have died or moved out of county through routine surveillance procedures or a prior project that investigated cases missing recent laboratory reports7 were excluded. In 2013, CD4 reporting was 95% complete and VL reporting was 97% complete in King County.22 We used two criteria to identify cases of PLWH who were out of or poorly engaged in HIV care: 1) VL>500 and CD4<350 cells/mm3 at the time of last report in the prior year (“recent unsuppressed VL”) or 2) no CD4 or VL in the past year (“12 month gap in laboratory reports”) or 2. Our decision to restrict the recent unsuppressed VL group to persons with CD4<350 cells/mm3 reflected the community standard and U.S. treatment guidelines in place when we designed the intervention.23 By July 2012, when we added the criterion of no CD4 or VL in the past year, the community standard had evolved to treat patients regardless of CD4 count24 and guidelines recommended initiation of ART for all HIV-infected individuals.25
We grouped participants based on their last known medical provider to form the clusters for randomization by identifying providers associated with the most recently reported laboratory result. The definition of the provider cluster depended on the characteristics of the care facility associated with the most recently reported CD4/VL. PLWH who received care in clinics with ≤2 providers or <10 total HIV-infected patients were grouped at the clinic level; otherwise cases were grouped by provider. We exempted cases with no CD4/VL (i.e. never linked to care) from randomization in order to prioritize them for immediate partner services intervention. The rationale for this was that CAPP was a novel intervention designed to re-engage PLWH who were poorly engaged in care or who had fallen out of care after linkage to initial care. It did not replace the standard-of-care HIV partner services procedures for linkage to initial care in King County, an approach which results in >95% of cases being successfully linked.22 For cases missing provider data, we attempted to determine the provider through a search of records available to the surveillance team prior to randomization. If this failed, we grouped the case with the first provider cluster from the reporting facility.
Intervention
The CAPP intervention included medical provider contact, patient contact, and structured individual counseling. Thus, it pertained to both the cluster level and the individual participant level. Two DIS investigated cases according to a standardized protocol described in detail elsewhere.26 DIS searched all available HIV/STD public health databases, electronic health records, death records, and a Lexis Nexis® database. If this did not yield a disposition, DIS contacted the medical provider. Providers received one list of their eligible patients and had the opportunity to opt-out of contact for patients on a case-by-case basis.
After notifying providers, the DIS contacted eligible individuals by phone and offered a face-to-face meeting, which took approximately 45 minutes for which the participant was compensated $50. The meeting included a structured interview to identify barriers to care and treatment and development of a plan to address identified barriers. The structured interview methods are described in detail elsewhere.18 DIS assisted patients with HIV care re-engagement according to a protocol. Most counseling sessions were conducted at the PHSKC STD Clinic, but when this was not feasible, the DIS met with patients in the field or by phone. If the participant consented, the DIS sent letters summarizing the encounter to the participant’s medical provider and case manager. DIS routinely attempted to contact all participants one month after the baseline appointment to assess whether they had seen their medical provider and offer additional assistance, but could also follow-up with patients sooner if indicated.
Sample Size and Randomization
The sample size for this program evaluation was defined by the number of eligible cases in King County; the intervention list was a complete enumeration of eligible cases. The sample size included all eligible persons in the county because we conceptualized the intervention from a public health perspective. In other words, we did not restrict our analysis or sample size to the subset of persons who successfully completed a structured interview. Assuming initiation of the intervention with 196 providers, a mean of 1.75 participants per provider, 35% viral suppression in the control period and a coefficient of variation of 0.4, we estimated 90% power to detect an increase in viral suppression to 47.5%.20 This estimate was informed by analysis of surveillance data in the year prior to the intervention and our assessment of what would constitute a meaningful level of intervention effect. We used a simple randomization scheme to order the clusters using computer-generated random numbers. The surveillance epidemiologist generated the case list, the lead investigator designated the cluster groupings, the epidemiologist performed the randomization, and the lead investigator assigned the list to DIS for intervention. This allocation was not blinded since it was not feasible to do so.
Outcomes and Statistical Methods
We identified the eligible cases in two groups at separate times. Group 1, identified in May 2011, included only cases with a recent unsuppressed VL and CD4 count <350 cells/μL. Group 2, identified in July 2012, included cases with a recent unsupressed VL and CD4 count <350 cells/μL as well as cases with a 12 month gap in laboratory reports. We did not include cases with a 12 month gap in laboratory reports in Group 1 because our surveillance team had not yet finished the investigation of cases with a 12 month gap in laboratory reports from 2006–2010.7 As demonstrated in Figure 1, all cases had an analysis period of 420 days. The start date of the analysis period was the day we drew the list of eligible cases from surveillance. We defined the end date of the analysis period a priori as 6 months after the day we initiated the last group of eligible persons in Group 2 and applied an equal observation time to Group 1. Our rationale for this was that 6 months following the initiation of the last group would provide sufficient time to detect an effect of the intervention in the contemporary ART era and the context of the King County HIV medical care resources. Cases were identified as eligible, clustered by provider, and clusters were randomized for Group 1, then separately and later, eligible cases were identified, clustered by provider, and clusters randomized for Group 2. The analysis period for Group 1 was May 1, 2011 to June 24, 2012, and the analysis period for Group 2 was July 25, 2012 to September 18, 2013. The control periods were the times between the start of the analysis period and the start of the intervention for each provider cluster, which we defined as the date that the DIS faxed the list of eligible patients to the provider.
Figure 1.
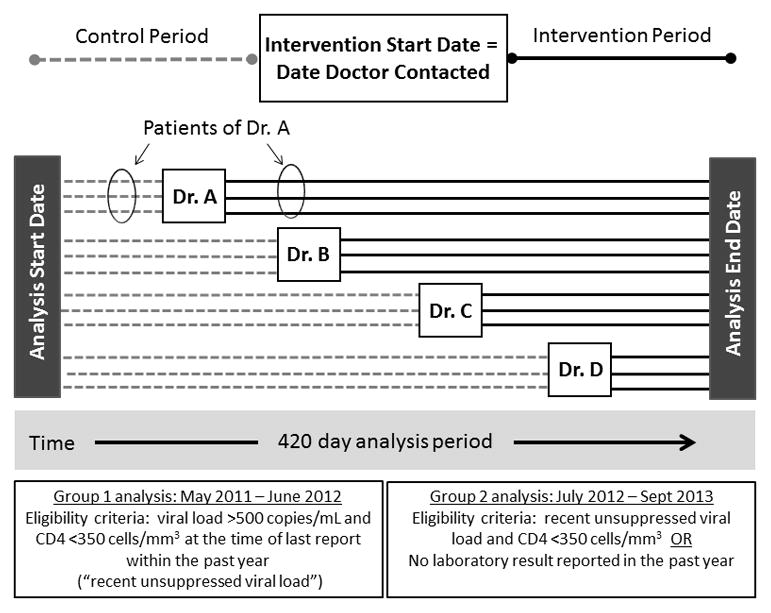
Schema of the Stepped Wedge Cluster Randomization
All outcomes pertained to the individual participant level. To assess the outcome measures, we used routinely reported HIV surveillance data. We defined the primary analysis outcome, time to viral suppresion, as the time between the analysis start date and the date of the first VL< 200 copies/mL. We defined the secondary outcome, relinkage to care among cases identified on the basis of having a 12 month gap in laboratory reports, as the date of the first VL or CD4 reported. Our rationale for selecting viral suppression as the primary outcome for both eligibility categories was that this was goal of the intervention for participants in both eligibility categories. We reasoned that a public health intervention which impacted relinkage to care without a subsequent difference in viral suppression would not constitute a potent public health intervention. Our rationale for excluding the cases with a recently reported unsuppressed VL from the secondary outcome was that they were already “linked to care” by surveillance criteria with ≥1 laboratory report in the past year.
We used chi-square tests to compare the characteristics of the identified cases with those of the overall population of HIV-diagnosed persons in King County at the end of 2012.27 We used Cox Proportional Hazards, with the analysis start date as time 0 and accounting for case clustering by provider,28 to compare outcomes during intervention periods versus control periods, censoring cases at the end of the observation period or on the date of death or the date that DIS ascertained relocation. The intention to treat (ITT) analysis included all randomized cases. Because it was not feasible in most cases for the DIS to determine the exact date a person who had relocated had moved away, the date of censoring for relocated cases was later than the actual relocation date. Thus, the modified ITT (mITT) population excluded all cases found to have relocated or died. In all analyses, we included the case group as a covariate. We conducted sensitivity analyses to determine whether the effect of the intervention varied by patient subgroups defined a priori: eligibility criterion, sex at birth, HIV risk factor, and CD4 count at baseline and to evaluate the impact of censoring deaths.
RESULTS
Analysis Population
We identified 997 cases that met CAPP criteria: 381 (38%) with a 12 month gap in laboratory reports and and 616 (62%) with a recent unsuppressed VL. These represented 14% of the estimated 7104 HIV-diagnosed person living in King County at the end of 2012.27 The cases were clustered in 281 provider groups with a median of 2 cases [interquarterile range (IQR: 1–5)] per cluster. The analysis population was younger (32% vs 24% under age 40; p<0.001) and had more advanced immunosuppression (25% vs. 8% had CD4 counts <200 at last report; p<0.001) than the general population of HIV-diagnosed persons in King County (Table 1).
Table 1.
Demographic characteristics of HIV-diagnosed persons in King County at the end of 2012 (N=7104) and the study population (N=997)
| HIV-Diagnosed Persons living in King County (N=7104) | Study Population (N=997) | Study Population vs. County Population | |||
|---|---|---|---|---|---|
| N | % | N | % | P-value | |
| Sex at Birth | 0.02 | ||||
| Male | 6353 | 89 | 865 | 87 | |
| Female | 751 | 11 | 131 | 13 | |
| Race/Ethnicity | <0.001 | ||||
| White, Non-Hispanic | 4709 | 66 | 424 | 43 | |
| Black, Non-Hispanic | 1201 | 17 | 161 | 16 | |
| Hispanic | 758 | 11 | 87 | 9 | |
| Asian or Pacific Islander | 248 | 3 | 30 | 3 | |
| American Indian | 68 | 1 | 5 | <1 | |
| Multiple & Missing | 120 | 2 | 290 | 29 | |
| HIV transmission risk factor† * | 0.01 | ||||
| MSM | 4904 | 69 | 645 | 65 | |
| MSM-IDU | 612 | 9 | 97 | 10 | |
| IDU | 326 | 5 | 49 | 5 | |
| Heterosexual | 694 | 10 | 97 | 10 | |
| Other/Missing | 568 | 8 | 109 | 11 | |
| Age, years† | <0.001 | ||||
| <30 | 462 | 7 | 83 | 8 | |
| 30–39 | 1206 | 17 | 240 | 24 | |
| 40–49 | 2530 | 36 | 381 | 38 | |
| ≥50 | 2906 | 41 | 289 | 29 | |
| Missing | 0 | 0 | 4 | <1 | |
| CD4 count at the time of last report (cells/mm3) | <0.001 | ||||
| <200 | 583 | 8 | 249 | 25 | |
| 200–500 | 2268 | 32 | 491 | 49 | |
| >500 | 3629 | 51 | 211 | 21 | |
| Missing | 624 | 9 | 46 | 5 | |
| Eligibility criterion for CAPP | NA | ||||
| CD4<500 & VL>500 | NA | NA | 616 | 62 | |
| No labs 12 months | NA | NA | 381 | 38 | |
NA, not applicable
Intervention Completion
DIS determined that 145 (15%) of the eligible persons had moved out of the area and 30 (3%) died (Figure 2). Of the 822 cases presumed to reside in the area (the mITT population), 20% (N= 161) had an undetectable VL reported to surveillance before DIS initiated contact attempts with the provider. DIS initiated CAPP procedures for the remaining 661 cases, 130 (20%) of which were closed when the medical provider asked the health department staff not to contact the patients. Most often this was because the provider had started the patient on ART in the interim since the patient was identified as eligible. DIS attempted to contact 531 persons and successfully contacted 243 (46%); 192 (79%) agreed to complete the CAPP interview, and 164 (85%) completed the structure interview (16% of the ITT and 19% of the mITT population).
Figure 2.

Intervention Flow Chart
Outcomes
The pre-intervention and intervention periods had a median duration of 210 days, with interquartile ranges of 140–343 days and 77–280 days, respectively. Of the 30 deaths, 19 occurred during the control period, 6 in the intervention period, and the death date was unknown for 5.
By the end of the observation period, 301 persons had a suppressed VL, representing 30% of the ITT and 37% of the mITT population. The point estimate of the hazard ratio (HR) for viral suppression was in the direction of a positive effect (shorter time to viral suppression), but was not statistically significant in the ITT analysis [HR 1.21 (95% CI: 0.85–1.71)] or the mITT analysis [HR 1.18 (95% CI: 0.83–1.68)] (Figure 3). Among 276 persons in the mITT population eligible based on a 12 month gap in laboratory reports, 131 (47%) relinked to care by the end of the observation period, but the time to relinkage did not differ in the intervention versus control periods [(HR 0.99 (95% CI: 0.64 – 1.55)]. By the end of the observation period, 77 (28%) of these cases had achieved viral suppression, but the time to viral suppression was similar in the intervention and control periods [HR 0.79 (95% CI: 0.40 – 1.55)]. Among 546 persons in the mITT population eligible based on a recent unsuppressed VL, 224 (41%) achieved viral suppression by the end of the observation period, and there was a non-significant trend toward shorter time to viral suppression in the intervention period [HR 1.45 (95% CI: 0.96 – 2.19)]. The outcome did not differ significantly between patient subgroups, and sensitivity analyses varying the approach to censoring deaths did not change the results (data not shown). In lieu of an intracluster correlation, we report the variance of the (gamma distributed) shared fraility from a Cox model as 0.21.
Figure 3. Kaplan-Meier Curves for Time to Viral Suppression According to Intervention vs. Control Period.

All cases identified (intention-to-treat), N=997 participants in 281 clusters (A). Excluding deaths and relocations (modified intention-to-treat), N= 822 participants in 252 clusters (B).
Among persons who completed the structured interview, 49 (30%) relinked to care within 1 month, 78 (48%) relinked within 3 months and 56 (34%) achieved viral suppression within 6 months of the interview. However, as shown in Table 2, from the entire analysis population of 997 eligible persons, approximately half of all persons who achieved viral suppression during the analysis period did so before DIS attempted to contact them [161 of 301; (53%)].
Table 2.
Viral suppression prior to and during the analysis period in the study population, by eligibility criterion, and by case disposition
| Population | Total | Suppressed viral load (VL)1 at the time of most recent report prior to the observation period | Suppressed VL reported by the end of the observation period2 | ||
|---|---|---|---|---|---|
| N | N | % (row) | N | % (row) | |
| Eligibility criterion | |||||
| All cases identied (ITT population) | 997 | 214 | 21 | 301 | 30 |
| Excluding cases that moved or died (mITT population) | 822 | 141 | 17 | 301 | 37 |
| No CD4 or VL reported (in mITT population) | 276 | 141 | 51 | 77 | 28 |
| VL>500 and CD4<350 at last report (in mITT population) | 546 | 0 | 0 | 224 | 41 |
| Case disposition | |||||
| Undetectable VL before contact attempted | 161 | 46 | 29 | 161 | 100 |
| Provider declined | 130 | 16 | 12 | 45 | 35 |
| No response | 288 | 57 | 20 | 45 | 16 |
| Patient declined | 51 | 7 | 14 | 12 | 24 |
| Accepted but did not complete intervention | 28 | 1 | 4 | 7 | 25 |
| Completed intervention | 164 | 14 | 9 | 52 | 32 |
HIV RNA <200 copies/mL
Includes both control and intervention periods
ITT, intention to treat; mITT, modified intention to treat
DISCUSSION
In a pragmatic randomized controlled evaluation, we found no significant effect of a health department Data to Care intervention on viral suppression or relinkage to care. Only a minority of persons who appeared to be poorly engaged in care based on surveillance data were contactable, and about half of all persons who achieved viral suppression did so before DIS attempted to contact them. These results are somewhat at odds with reports which have suggested that this type of Data to Care effort can be effective.9,13–15,17 This may reflect the absence of a control group or period in prior studies. Many persons in our analysis achieved viral suppression in the absence of any intervention from the health department. This may have been influenced by interventions such as case management outreach and other evolving community outreach efforts. For this reason, a simple pre- vs. post-intervention analysis would not have allowed us to assess the independent effect of our intervention. Since more deaths occurred in the control period than the intervention period (19 vs. 6), it is possible that our intervention averted some deaths without impacting viral suppression or relinkage to care in the overall population.
Our findings have implications for public health Data to Care programs and for how such programs are studied. First, Data to Care efforts that rely on surveillance data are relatively inefficient since many persons who appear to be out of care have actually moved away. Our data, as well as a number of prior reports, have all found that less than half of persons who appear to be out of care based on surveillance data are truly out of care.10,12,14–16 While the percentage of persons classified as out of care declines as surveillance data improves -- only 15% of apparently “out-of-care” cases in this analysis were defined as having relocated compared to 47% when our group began to investigate such cases in 2007 – it remains large, especially when persons whom staff could not reach, most of whom were almost certainly also out of the area, are grouped with persons confirmed to have relocated. From a public health programmatic perspective, this reality means surveillance-based Data to Care is inefficient. From a reseach perspective, when evaluating an intervention like ours, it diminishes the intervention’s effect size and and statistical power. It should be noted, this problem is not unique to surveillance-based interventions like the one we studied. HIV care relinkage interventions that use clinic data have also found that many persons who appear to be out of care have actually transferred care or moved away and that only about half or less of those remaining can be successfully re-engaged.29, 30
Second, relinkage-focused interventions appear to be relatively weak. Even among persons who completed our intervention, only about one-third achieved viral suppression within 6 months. This finding needs to be confirmed elsewhere before drawing generalizable conclusions, but our results suggest that relatively low-intensity interventions – at least in a place like Seattle, Washington – have relatively little impact. Attempting to relink PLWH to the same healthcare system that failed to engage them in the first place is not an effective strategy. Ideally, a comprehensive approach to improving retention in care should combine interventions of varying intensity matched to the needs of the out-of-care PLWH, which might need to include structural changes in the healthcare system To address the need for an alternative HIV medical care models for the hardest-to-reach PLWH, PHSKC and the Madison (HIV) Clinic in Seattle implemented a low-threshold incentivized care model with intensive outreach support (the MAX Clinic) in 2015.31
The primary strength of our analysis was the randomized, controlled evaluation design. Our analysis also had important limitations. It was conducted in a single jurisdiction, and its generalizability is uncertain. However, several other health departments in multiple regions of the country have now reported preliminary results demonstrating that only a minority of persons who appear to be out of care can be successfully engaged with existing Data to Care strategies.10,12,14–16 Despite extensive investigation, we were unable to determine the true status of many cases. Finally, we used surveillance data to ascertain outcomes, which may have underestimated the level of viral suppression achieved during the observation period, though laboratory reporting in King County is >90% complete.
In summary, we found in a randomized controlled analysis that a health department surveillance-based outreach strategy was ineffective. While additional studies in other locations are needed, our findings highlight the need to consider this type of Data to Care strategy as just one component of public health efforts to improve engagement in HIV care and treatment. Facility-based identification of out-of-care persons as they enter jails, emergency departments, and hospitals may be more effective than the outreach investigations we describe.32 To the extent that surveillance-based outreach is employed, prioritizing cases with recently reported high viral loads, rather than a gap in laboratory reports, may improve the impact of the strategy. Data sharing procedures between jurisdictions and between surveillance and healthcare entities could improve surveillance data. Finally, to successfully reach individuals who are not engaged in traditional HIV care and treatment, we may need higher intesity interventions with novel care delivery strategies.
Supplementary Material
1. CONSORT checklist for cluster randomized trials, completed for the current paper
SUMMARY.
A randomized controlled evaluation of a health department Data to Care intervention found that the strategy did not impact viral suppression or relinkage to care among persons with evidence of poor engagement in HIV care.
Acknowledgments
Sources of Funding: This work was supported by a grant to JCD from the National Institute of Mental Health (5K23MH090923); the University of Washington Center for AIDS Research (CFAR), an NIH funded program under award number P30AI027757 which is supported by the following NIH Institutes and Centers (NIAID, NCI, NIMH, NIDA, NICHD, NHLBI, NIA, NIGMS, NIDDK); programmatic funding from the Health Resources & Services Administration to Public Health – Seattle & King County and from the Centers for Disease Control and Prevention to the Washington State Department of Health.
JCD has conducted research unrelated to this work supported by grants to the UW from the following companies: Hologic, Genentech, Melinta Therapuetics, Curatek Pharmaceuticals, ELITech and the Quidel Corporation. MRG has conducted research unrelated to this work supported by grants to the UW from the following companies: Cempra pharmaceuticals and Melinta Therapeutics.
The authors would like to acknowledge James B. Kent for assistance with the surveillance aspects of this project ; Becca Hutcheson and Jeff Natter for contributions to the conception and implementation of the CAPP intervention ; the UW CFAR Community Action Board ; the Part A HIV Planning Council in Seattle & King County ; the HIV medical and social services providers in King County who contributed to the CAPP program ; and the PLWH who participated in CAPP.
Footnotes
Conflicts of Interest: All other authors report no conflicts of interest.
References
- 1.INSIGHT START Study Group. Lundgren JD, Babiker AG, et al. Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection. New Engl J Med. 2015;373:795–807. doi: 10.1056/NEJMoa1506816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cohen MS, Chen YQ, McCauley M, et al. Prevention of HIV-1 infection with early antiretroviral therapy. New Engl J Med. 2011;365:493–505. doi: 10.1056/NEJMoa1105243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Office of National AIDS Policy WHDPC. [Accessed August 17, 2015];The National HIV/AIDS Strategy: Updated to 2020. 2015 https://www.aids.gov/federal-resources/national-hiv-aids-strategy/nhas-update.pdf.
- 4.Lesko CR, Sampson LA, Miller WC, Clymore J, Leone PA, Swygard H, et al. Measuring the HIV Care Continuum Using Public Health Surveillance Data in the United States. J Acquir Immune Defic Syndr. 2015;70:489–94. doi: 10.1097/QAI.0000000000000788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Centers for Disease Control and Prevention. [Accessed December 9, 2016];Data to Care: Improving Health and Prevention. 2015 [updated June 12, 2015; cited 2016 Aug 17]. Available from: https://effectiveinterventions.cdc.gov/en/HighImpactPrevention/PublicHealthStrategies/DatatoCare.aspx.
- 6.Sweeny PA, Gardner LI, Buchacz K, Garland PM, Mugavero MJ, Bosshart JT, et al. Shifting the paradigm: public health surveillance programs and HIV care providers collaborating to improve HIV care and prevent HIV infection. Milbank Quarterly. 2013;91:558–603. doi: 10.1111/milq.12018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Buskin SE, Kent JB, Dombrowski JC, Golden MR. Migration distorts surveillance estimates of engagement in care: results of public health investigations of persons who appear to be out of HIV care. Sex Transm Dis. 2014;41:35–40. doi: 10.1097/OLQ.0000000000000072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.International Advisory Panel on HIVCCO. IAPAC Guidelines for optimizing the HIV care continuum for adults and adolescents. J Int Assoc Provid AIDS Care. 2015;14(Suppl 1):S3–4. doi: 10.1177/2325957415613442. [DOI] [PubMed] [Google Scholar]
- 9.Udeagu CC, Webster TR, Bocour A, Michel P, Shepard CW. Lost or just not following up: public health effort to re-engage HIV-infected persons lost to follow-up into HIV medical care. AIDS. 2013;27:2271–9. doi: 10.1097/QAD.0b013e328362fdde. [DOI] [PubMed] [Google Scholar]
- 10.Brantly A. Expanding the use of surveillance data to improve HIV medical care engagement and viral suppression. Presented at: 2015 National HIV Prevention Conference; December 6–9, 2015; Atlanta, Georgia. [Google Scholar]
- 11.Kulkarni S. Improvements in retention in care and viral suppression: results from the first year of the medical care coordination program in Los Angeles County. Presented at: 2015 National HIV Prevention Conference; December 6–9, 2015; Atlanta, Georgia. [Google Scholar]
- 12.Cassidy-Stewart H. Maryland’s PS12-1201 demonstration project: improving the health of Marylanders living with HIV through enhanced linkage-to-care systems and activities. Presented at: 2015 National HIV Prevention Conference; December 6–9, 2015; Atlanta, Georgia. [Google Scholar]
- 13.Buchacz K, Chen MJ, Parisi MK, et al. Using HIV surveillance registry data to re-link persons to care: the RSVP Project in San Francisco. PLoS One. 2015;10(3):e0118923. doi: 10.1371/journal.pone.0118923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nagavedu K, Hawrusik R, Hague J, et al. Using HIV laboratory surveillance data to identify out-of-care patients. Presented at: 2015 National HIV Prevention Conference; December 6–9, 2015; Atlanta, Georgia. [Google Scholar]
- 15.Tesoriero J, Johnson BA, Cukrovany J, et al. Improving retention in HIV care through New York’s expanded partner services Data-to-Care pilot. J Public Health Manag Pract. 2017;23:255–63. doi: 10.1097/PHH.0000000000000483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Morrison M. Partnering HIV surveillance and prevention to identify and provide linkage to care for out of care diagnosed positive individuals. Presented at: 2015 National HIV Prevention Conference; 2015; Atlanta, Georgia. [Google Scholar]
- 17.Sachdev D, Pipkin S, Scheer S, Cohen SM, Antunez E. Short-term navigations successful at re-engaging patients in care. Presented at: Adherence 2015; June 28–30, 2015; Miami, FL. [Google Scholar]
- 18.Dombrowski JC, Simoni JM, Katz DA, Golden MR. Barriers to HIV Care and Treatment Among Participants in a Public Health HIV Care Relinkage Program. AIDS Patient Care STD. 2015;29:279–87. doi: 10.1089/apc.2014.0346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dombrowski JC, Carey JW, Craw JA, et al. Patient and provider perspectives on the development of a health department “Data to Care” program: a qualitative study. BMC Public Health. 2016;16:491. doi: 10.1186/s12889-016-3152-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hussey MA, Hughes JP. Design and analysis of stepped wedge cluster randomized trials. Contemp Clin Trials. 2007;28:182–91. doi: 10.1016/j.cct.2006.05.007. [DOI] [PubMed] [Google Scholar]
- 21.Hughes JP, Granston TS, Heagerty PJ. Current issues in the design and analysis of stepped wedge trials. Contemp Clinl Trials. 2015;45(Pt A):55–60. doi: 10.1016/j.cct.2015.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.HIV/AIDS Epidemiology Unit, Public Health - Seattle & King County and the Infectious Disease Assessment Unit, Washington State Department of Health. HIV/AIDS Epidemiology Report 2015. 84 [Google Scholar]
- 23.Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services; Washington, DC: Dec 1, 2009. [Accessed Sept 12, 2017]. Available at: https://aidsinfo.nih.gov/contentfiles/adultandadolescentgl001561.pdf. [Google Scholar]
- 24.Toren KG, Buskin SE, Dombrowski JC, Cassels SL, Golden MR. Time from HIV diagnosis to viral suppression: 2007–2013. Sex Transm Dis. 2016;43:34–40. doi: 10.1097/OLQ.0000000000000376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services; Washington, DC: Mar 27, 2012. [Accessed September 9, 2017]. Available at: https://aidsinfo.nih.gov/contentfiles/adultandadolescentgl003093.pdf. [Google Scholar]
- 26.Dombrowski JC, Bove J, Roscoe JC, et al. “Out of care” HIV case investigations: a collaborative analysis across six states in the Northwest US. J Acquir Immune Defic Syndr. 2017;74(Suppl 2):S81–87. doi: 10.1097/QAI.0000000000001237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.HIV/AIDS Epidemiology Unit, Public Health - Seattle & King County and the Infectious Disease Assessment Unit, Washington State Department of Health. HIV/AIDS Epidemiology Report, Second Half 2012. 81 [Google Scholar]
- 28.Lin DY, Wei LJ. The robust inference fo the Cox Proportional Hazards Model. J Am Stat Assoc. 1989;84:1074–8. [Google Scholar]
- 29.Bove J, Golden MR, Dhanireddy S, Harrington RD, Dombrowski JC. Outcomes of a Clinic-Based, Surveillance-Informed Intervention to Relink Patients to HIV Care. J Acquir Immune Defic Syndr. 2015;70:262–8. doi: 10.1097/QAI.0000000000000707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sitapati AM, Limneos J, Bonet-Vazquez M, Mar-Tang M, Qin H, Mathews WC. Retention: building a patient-centered medical home in HIV primary care through PUFF (Patients Unable to Follow-up Found) J Healthcare Poor Underserved. 2012;23(3 Suppl):81–95. doi: 10.1353/hpu.2012.0139. [DOI] [PubMed] [Google Scholar]
- 31.Dombrowski JC, Ramchandani M, Moore A, et al. The MAX Clinic: a structural healthcare systes intervention designed to engage the hardest-to-reach persons living with HIV/AIDS. Presented at: Adherence 2016; May 9–11, 2016; Fort Lauderdale, FL. [Google Scholar]
- 32.Magnus M, Herwehe J, Gruber D, et al. Improved HIV-related outcomes associated with implementation of a novel public health information exchange. Int J Med Inform. 2012;81:e30–38. doi: 10.1016/j.ijmedinf.2012.06.005. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
1. CONSORT checklist for cluster randomized trials, completed for the current paper