

Abstract
Objectives
This analysis examines the etiology of caries development in adolescents by using structural equation modeling to identify behavioral mediators of the relationship between socioeconomic status (SES) and caries incidence, and to investigate the role of sex on caries preventive behavior and caries.
Methods
This analysis was based on data from the Iowa Fluoride Study, a longitudinal study of a birth cohort. We hypothesized that socioeconomic status earlier in life has a direct effect on caries development and an indirect effect from improved behavioral variables – dental visit attendance, tooth brushing frequency, and percentage of beverage intake consisting of sugar-sweetened beverages – and that sex also plays a role in behavioral variables, as well as caries. A structural equation model was developed based on these hypotheses and direct and indirect standardized path coefficients were calculated, as well as their standard errors.
Results
Based on our proposed model, SES at birth significantly influences SES during adolescence, but not adolescent behaviors. The effect of SES during adolescence on caries in the permanent dentition is mediated by adolescent behaviors. Female participants have worse caries than male participants, despite lower self-reported percentages of sugar-sweetened beverage intake and more frequent brushing and dental attendance.
Conclusions
This analysis models the relationships among known causal factors for caries and suggests that the role of SES in caries may not be as important as previously thought and different behaviors that affect oral health between males and females as well as differences in caries between the sexes could begin during adolescence. These findings could help improve caries prevention programs for adolescents.
Keywords: Caries, Diet, Oral Hygiene, Pediatric Dentistry, Prevention
Introduction
Dental caries is the most prevalent chronic disease in American children and adolescents1. Although many factors associated with caries incidence such as tooth brushing, sugar intake, and socioeconomic status (SES) are well established2,3,4,5, quantification of the relationships between adolescents’ caries and cariogenic factors - especially dietary factors - is needed to enhance interventions to prevent caries. In particular, it is important to understand how behavioral and/or dietary habits during adolescence mediate the impact of SES on caries. Studies of caries in late childhood and adolescence are relatively uncommon, despite the fact that many changes in behavioral and dietary patterns occur as children become more independent6,7.
Many studies that aim to determine factors associated with caries development use regression models consisting of an outcome variable measuring extent of caries and a list of predictors. These models do not describe relationships among predictor variables inherent in the mechanism of caries development, limiting their practical value. Some studies have examined the relationships among cariogenic predictor variables in adolescents using structural equation modeling with similar hypotheses, but did not consider dietary variables or sex8,9. We hypothesize that behavioral factors such as tooth brushing frequency, dental visit attendance, and sugar-sweetened beverage intake are mediators of the effects of SES on caries in adolescence, and sex could play a role in caries preventive behavior or caries development.
The Iowa Fluoride Study (IFS) has followed a birth cohort through adolescence, regularly collecting demographic, behavioral, and dietary information, as well as conducting caries examinations. The objective of this study is to utilize the structural equation modeling framework to assess the strength of hypothesized relationships among a number of caries predictor variables using data from the IFS.
Methods
Iowa Fluoride Study
After receiving University of Iowa institutional review board approval, the IFS recruited mothers and newborns from maternity wards in eight Iowa hospitals between 1992 and 1995. Additional written consent and assent was obtained at each clinical examination. The study methods of the IFS are described briefly here, but more detailed descriptions can be found in earlier publications10,11,12,13. Overall, semi-annual questionnaires were collected to monitor participant diet and oral health habits such as brushing frequency and dental visit attendance. Caries in the permanent dentition, as well as demographic and behavioral variables, were assessed at clinical examinations at ages 9, 13, and 17.
Risk Factor Variables
The questionnaires, sent to the participants’ parents at 6-month intervals during the study period, asked about participant beverage intakes and oral health habits over the previous week, as well as whether the participant had seen a dentist in the previous 6 months. These questionnaires were internally validated12. For this analysis, the percentage of daily beverage intake consisting of sugar-sweetened beverages (%SSB) was calculated using questionnaire responses. For each participant, %SSB and daily tooth brushing frequency were averaged over two groups of questionnaires – the first for ages 13, 13.5, 14.0, 14.5, and 15 years, and the second for ages 15.5, 16, 16.5, and 17 years. A composite measure of dental visit attendance consisted of the proportion of questionnaires returned between ages 13 and 17 where the participant visited their dentist within the six months before completing the questionnaire. SES information was collected at recruitment and in a separate mailing in 2007. SES at recruitment was categorized into low (household income <$30,000 and participant mother not having a 4-year college degree), middle (household income $30,000 - $49,999 and participant mother without a graduate/professional degree or household income <$30,000 and participant mother with at least a 4-year college degree), and high (household income ≥$50,000 regardless of educational level or household income ≥$30,000 and participant mother with a graduate/professional degree). Household income level in 2007 was measured in $20,000 increments. At the time of clinical examinations, parents/participants were asked additional questions about participant behaviors and dietary habits, including how many meals and snacks the participant typically consumed per day. This was used to assess the number of eating events per day for each participant.
Outcome Variables
Caries examinations were carried out at ages 9, 13, and 17 by trained and calibrated dental examiners using a portable dental chair, mouth mirror, and examination light, where each tooth surface was examined for fillings and cavitated caries. The number of decayed and filled surfaces on the permanent incisors and first molars was determined from the age 9 examination. Adjusted DFS Increments (or Adjusted Caries Increments, ADJCI) were calculated according to Beck et al.14 for ages 9-13 and 13-17.
Statistical Analyses
For a structural equation model (SEM), proposing variables and associations and subsequently estimating coefficients and assessing model fit is a multi-step process. First, the pertinent latent variables and the causal relationships between them are hypothesized, and estimation of the parameters in the proposed model is conducted. Typically, re-formulation of the SEM is necessary. Goodness-of-fit measures are used to ensure that the model is not poorly specified. In this manuscript, “relationship” is used to refer to hypothesized causal associations. Due to the observational nature of our study, these hypothesized causal associations should be interpreted cautiously.
Initially, a simple model was proposed including three broadly defined latent variables - SES, ADJCI, and modifiable behaviors. This model examined the direct relationship between SES and ADJCI as mediated by modifiable behaviors. The original hypothesized model, based solely on an understanding of the available data from previous analyses and substantive reasoning, suffered from improper solutions and inadequate fit, in part due to poorly-defined latent variables. Therefore, careful re-formulation was conducted, with heavy emphasis on hypothesizing clinically-meaningful relationships between variables. The proposed model is the result of this re-formulation process.
In SEM, latent variables allow for the representation of unobservable constructs and the dimension reduction of longitudinal data. In this analysis, the means and variances of the latent variables were fixed to zero and one, respectively, to ensure model identifiability.
In SEMs, path coefficients quantify the relationship between two variables. Unstandardized path coefficient estimates and their standard errors were calculated using the sem function in Version 0.5-20 of the lavaan package15 in R16. Unstandardized path coefficient estimates were obtained using robust diagonally weighted least squares as derived by Muthén17,18 and implemented in lavaan. This estimation method is recommended for non-normal and categorical variables19. Unstandardized path coefficients depend on the units of measured variables, while standardized path coefficients do not. Since the model contains variables with different units, standardized path coefficient estimates were also calculated using the lavaan package.
Ordinal, count, and continuous variables were used in this analysis. Based on simulation studies, non-continuous variables with less than 5 categories are considered categorical and the use of polychoric or polyserial correlations is recommended20. In this analysis, SES level at participant birth (3 categories), household income category in 2007 (4 categories), and participant sex (2 categories) were considered categorical, while all other variables were deemed quantitative.
In this analysis, multiple imputation was used to complete cases for participants with all three caries examinations, but missing information for one or more of the other variables used in the proposed model. Multiple imputation was conducted using the mice21 and semTools22 packages in R, versions 2.22 and 0.4-13, respectively. Predictive mean matching was used to impute missing values and 5 imputations were used. The point estimates are averages of the estimates from each imputation, while the standard errors account for within- and between-imputation variation in the point estimates. Two models were compared during the multiple imputation process: a model based on only complete cases (n= 344) who had information for all measured variables and a model based on multiply imputed data derived using all participants with caries examinations conducted at ages 9, 13, and 17 (n=413).
Finally, model fit was assessed using the chi-square goodness of fit test and the root mean square error of approximation (RMSEA). Detailed discussion of these fit indices is in the references19. The chi-square test statistic and the RMSEA are goodness-of fit criteria with smaller values corresponding to better overall fit. The RMSEA is a more refined version of the chi-square test statistic, which is frequently reported but has limitations - primarily that the probability of rejecting the test statistic is strongly related to the sample size19.
Results
There were 413 participants with caries examinations at ages 9, 13, and 17. There were 69 participants with missing data for at least one of the other measured variables in the model. Summary statistics for the measured variables included in this analysis are presented in Table 1. Most participants’ families had middle or high SES (77.2%) at participant birth and 48.1% of households had incomes ≥$80,000 in 2007. The sample was 53% female. Daily brushing frequency and %SSB remained relatively consistent between ages 13 and 17. However, ADJCI was highest from age 13 to 17. Weighted kappas were used to assess inter-examiner reliability for classification of sound, non-cavitated caries, and cavitated/filled caries at the surface level. For all teeth examined at approximate ages 9, 13, and 17, these kappa statistics are 0.82, 0.62, and 0.62, respectively.
Table 1.
Demographic and Behavioral Characteristics and Outcomes of Iowa Fluoride Study Participants (Number of participants with available data is provided for each variable)
| Demographic Variables | Count (%) |
|---|---|
| SES at Participant Birth (n=399) | |
| Low | 91 (22.8%) |
| Middle | 141 (35.3%) |
| High | 167 (41.9%) |
| Household Income in 2007 (n=395) | |
| < $40,000 | 57 (14.4%) |
| $40,000 – $59,999 | 67 (17.0%) |
| $60,000 – $79,999 | 81 (20.5%) |
| ≥ $80,000 | 190 (48.1%) |
| Sex (n=413) | |
| Male | 194 (47.0%) |
| Female | 219 (53.0%) |
| Behavioral Variables | Mean (SD) |
|
| |
| Proportion of Questionnaire Responses with Dental Attendance in the Previous 6 Months (n=411) | 0.8 (0.3) |
| Daily Brushing Frequency Averaged over 13- to 15-year-old Questionnaires (n=411) | 1.6 (0.5) |
| Daily Brushing Frequency Averaged over 15.5- to 17-year-old Questionnaires (n=384) | 1.7 (0.6) |
| Proportion Of Daily Beverage Intake Consisting of Sugar-Sweetened Beverages Averaged over 13- to 15-year-old Questionnaires (n=411) | 0.3 (0.2) |
| Proportion Of Daily Beverage Intake Consisting of Sugar-Sweetened Beverages Averaged over 15.5- to 17-year-old Questionnaires (n=384) | 0.3 (0.2) |
| Eating Events Per Day at Age 13 (n=406) | 4.9 (1.3) |
| Outcome Variables | Mean (SD) |
|
| |
| Permanent DFS Count Age 9 (n=413) | 0.5 (1.2) |
| Adjusted DFS Increment Ages 9 – 13 (n=413) | 0.7 (1.7) |
| Adjusted DFS Increment Ages 13 - 17 (n=413) | 2.1 (3.3) |
The proposed model presented in Figure 1 has three major components: SES variables, behavioral variables, and caries variables. Children from high SES backgrounds consistently have less caries4,5,8,9. Also, studies outside the U.S. which examine the effect of early life SES on adolescent caries have shown that higher SES early in life is associated with less caries or better oral health during adolescence23,24 Therefore, it was proposed that participants from high-SES households were likely to have less caries directly (due to factors not accounted for by the proposed model) and indirectly (through improved oral health habits and lower sugar-sweetened beverage intake). Also, SES at birth and during adolescence should play a role in caries and caries preventive behaviors. There is some evidence for higher SSB intakes and lower dental visit attendance among children with low SES backgrounds25,26. There has been some study of the association between SES and oral health habits such as tooth brushing for U.S. adolescents, which suggests that brushing is associated with SES27, but earlier results from the IFS have shown little association28. These proposed indirect relationships are also viable to consider because of the known associations of tooth brushing and SSB intake with caries2,3,8. This indirect relationship could also reflect the life course hypothesis that SES early in life influences oral health beliefs and behaviors later in life, as suggested by Broadbent et al.9. The direct relationship between eating events per day and caries also was modeled. Eating frequency has been associated with caries in young children29. Although there is not sufficient evidence for a consensus, some evidence of sex differences in caries incidence have been observed in the literature, with females having greater caries experience than their male counterparts30,31,32,33,34. Therefore, it was hypothesized that factors related to being female were associated with more caries, and a direct relationship between sex and ADJCI was considered. We also hypothesized behavioral differences between male and female participants by including a path from participant sex to each of the behavioral variables in the model (eating events per day, oral health habits, and %SSB) based on literature showing significant differences in sweetened soft drinks and breakfast eating frequency between sexes35.
Figure 1.
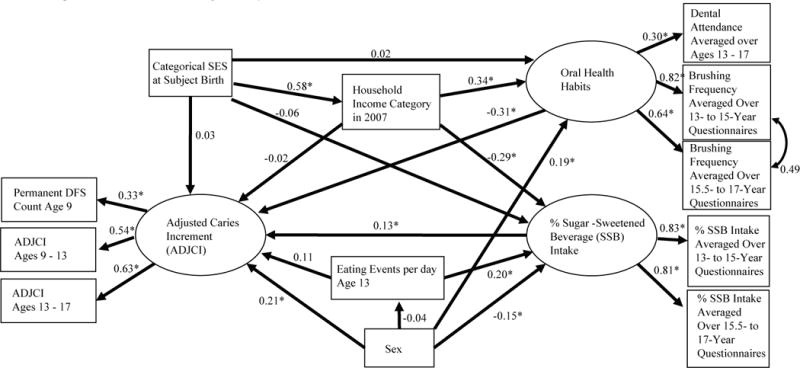
Path Diagram of Proposed Model for Mechanism of Caries Development among Iowa Fluoride Study Participants. Multiple imputation was used (n=413). Latent variables are represented by circular nodes, while measured (or observed) variables are represented by rectangular nodes. An asterisk (*) indicates path coefficients which are significantly different from zero at the 0.05 level. Note that males were coded as “0” and females were coded as “1”.
In the measurement model, the ADJCI latent variable was defined using baseline DFS count for permanent teeth at age 9 and two ADJCIs (9 to 13 and 13 to 17) for the permanent teeth only. The %SSB latent variable was defined using two measured variables which quantified %SSB intake during the two periods, and the oral health habits latent variable was defined using two measured variables which quantified daily brushing frequency over two periods, as well as dental attendance between ages 13 and 17. Note that the covariance between the error terms for the two daily brushing frequency variables was free to vary. Latent variables represent the variability common to a group of measured variables, and there was some variability shared by the two brushing frequency variables which was not shared with the dental visit attendance variable. The covariance term accounts for variability common to the two brushing frequency variables due to repeated measures, but not shared by the dental visit attendance variable.
Figure 1 provides standardized path coefficient estimates for the proposed model fit after employing multiple imputation. The standardized path coefficients in Figure 1 are generally between −1 and 1 and represent the magnitude and direction of the hypothesized causal relationships between pairs of variables. The corresponding unstandardized estimates, as well as their standard errors (which are used to calculate p-values), are given in Table 2.
Table 2.
Summary of Path Coefficients – Imputed Model for Etiology of Caries Development among Iowa Fluoride Study Participants. This table summarizes standardized and unstandardized path coefficient estimates, and their corresponding standard errors and p-values.
| Latent Variable Loadings | Standardized Estimate | Estimate (SE) | p-value |
|---|---|---|---|
| Oral Health Habits | |||
| Dental Visit Attendance | 0.299 | 0.076 (0.019) | <0.001 |
| Daily Brushing Frequency 13-15 | 0.821 | 0.393 (0.091) | <0.001 |
| Daily Brushing Frequency 15.5-17 | 0.641 | 0.328 (0.086) | <0.001 |
| % Sugar-Sweetened Beverage | |||
| % SSB Ages 13 – 15 | 0.828 | 0.125 (0.011) | <0.001 |
| % SSB Ages 15.5 – 17 | 0.805 | 0.138 (0.012) | <0.001 |
| Adjusted DFS Increment | |||
| Permanent DFS Count Age 9 | 0.328 | 0.347 (0.057) | <0.001 |
| Adjusted DFS Increment Age 9-13 | 0.541 | 0.820 (0.098) | <0.001 |
| Adjusted DFS Increment Ages 13-17 | 0.628 | 1.896 (0.217) | <0.001 |
|
| |||
| Direct Effects | Standardized Estimate | Estimate (SE) | p-value |
|
| |||
| Household Income in 2007 by | |||
| Categorical SES at Birth | 0.579 | 0.906 (0.080) | <0.001 |
| Oral Health Habits by | |||
| Household Income in 2007 | 0.341 | 0.303 (0.099) | 0.002 |
| Categorical SES at Birth | 0.020 | 0.028 (0.112) | 0.804 |
| Sex | 0.191 | 0.417 (0.154) | 0.007 |
| % Sugar Sweetened Beverage by | |||
| Categorical SES at Birth | −0.056 | −0.078 (0.101) | 0.438 |
| Household Income in 2007 | −0.292 | −0.262 (0.069) | <0.001 |
| Eating Events Per Day at Age 13 | 0.204 | 0.173 (0.044) | <0.001 |
| Sex | −0.154 | −0.339 (0.117) | 0.004 |
| Eating Events Per Day at Age 13 by | |||
| Sex | −0.040 | −0.105 (0.132) | 0.428 |
| Adjusted DFS Increment by | |||
| Sex | 0.208 | 0.451 (0.176) | 0.010 |
| Eating Events Per Day at Age 13 | 0.114 | 0.095 (0.056) | 0.091 |
| % Sugar Sweetened Beverage | 0.127 | 0.126 (0.058) | 0.030 |
| Oral Health Habits | −0.308 | −0.307 (0.126) | 0.015 |
| Household Income in 2007 | −0.015 | −0.013 (0.098) | 0.891 |
| Categorical SES at Birth | 0.034 | 0.047 (0.115) | 0.682 |
|
| |||
| Covariance Path | Standardized Estimate | Estimate (SE) | p-value |
|
| |||
| Between Daily Brushing Frequency for Ages 13–15 and Ages 15.5–17 | 0.487 | 0.062 (0.060) | 0.301 |
The results presented in Figure 1 generally reflect what was hypothesized, with the exception of the hypothesized relationships with SES at birth, the direct relationship between household income in 2007 and ADJCI, and the hypothesized relationships with eating events per day at age 13. The path coefficients representing the direct effects of household income in 2007 and SES at participant birth on ADJCI are small and not significant. While SES at participant birth strongly influenced 2007 household income, it had weak relationships with %SSB intake and oral health habits. Eating events per day did not have a significant relationship with ADJCI.
The indirect and total effects of certain variables of interest on ADJCI also were examined, and these results are presented in Table 3. The indirect relationship between two variables can be quantified by summing the product of the standardized path coefficients for each indirect path between two variables, and these can be conceptualized as mediating effects. The direct effect of SES at birth on ADJCI is not significant and in the opposite of the hypothesized direction, while the indirect effect (which is primarily through the strong relationship between SES at birth and household income in 2007) is marginally significant and in the hypothesized direction. This leads to a total effect of SES at birth which is in the hypothesized direction, although not statistically significant. The interpretation of direct and indirect effects for household income in 2007 is similar, indicating that higher SES leads to improved behavioral variables, which in turn may lead to lower ADJCI. Also, in this dataset, female participants tended to have worse caries, before and after accounting for the very small indirect effects of their lower %SSB intakes and better oral health habits.
Table 3.
Standardized Direct and Indirect Effects (p-value) of Variables of Interest on Adjusted DFS Increment for Models of Etiology of Caries Development among Iowa Fluoride Study Participants.
| Variable | Direct Effect | Indirect Effect | Total Effect |
|---|---|---|---|
| SES at Birth | 0.03 (0.682) | −0.11 (0.046) | −0.07 (0.321) |
| Household Income in 2007 | −0.02 (0.891) | −0.14 (0.037) | −0.16 (0.057) |
| Oral Health Habits | −0.31 (0.015) | – | −0.31 (0.015) |
| %SSB Intake | 0.13 (0.030) | – | 0.13 (0.030) |
| Sex | 0.21 (0.010) | −0.03 (0.049) | 0.18 (0.023) |
| Eating Events/Day | 0.11 (0.091) | 0.03 (0.051) | 0.14 (0.034) |
The results for the model that did not use multiple imputation were similar and therefore, were not shown. Of note, in the complete case model, the magnitude of the effects of oral health habits on ADJCI was smaller, while the magnitudes of the effects of %SSB and household income in 2007 on ADJCI were larger. However, the conclusions based on the p-values are the same in the complete case model.
The RMSEA for the imputed model was 0.049, with a 90% confidence interval of (0.033, 0.064), which is almost completely below a conventionally-used benchmark of 0.06. While the chi-square test for goodness of fit was statistically significant, the ratio of the chi-square test statistic and the degrees of freedom was 1.99, below the recommended threshold of 5, also indicating good model fit. The sensitivity of the chi-square test statistic increases with increasing sample size and the p-value for this test could, therefore, be an unnecessarily strict measure of model fit. Thus, the fit indices for the hypothesized model do not provide strong evidence of lack of fit.
Discussion
In this analysis, an SEM was used to examine the strength of relationships in a proposed causal model, allowing for examination of the relationships among variables which have been considered predictors in other modeling frameworks. Overall, better oral health habits and lower %SSB intake accounted for the effect of SES on the caries outcome (ADJCI). SES at birth was not directly related to %SSB intake or oral health habits in adolescence, but was indirectly related through household income in 2007 Also, eating events per day did not have a significant effect on ADJCI.
Female participants overall had more caries, despite having lower %SSB intakes and better oral health habits. Sex could be associated with caries incidence, as shown by some results in the literature, as well as previous IFS results during the adolescent period, however, there is not a consensus in the literature30,31,32. This possible difference could be due to earlier tooth eruption in females, differences in dental care utilization, hormonal changes during puberty, and genetic differences30,31,33,34.
In order to get a more complete picture of the causal pathway for caries incidence in adolescence, many variables are required, including SES, dietary, and behavioral information. The IFS has collected this information on a moderately-sized sample of participants with good retention. This analysis also benefits from the use of multiple imputation. The estimation methodology used in this analysis relies on asymptotic assumptions and, therefore, performs better with larger sample sizes. Also, excluding participants without complete cases can lead to a biased sample. Since it is reasonable to assume that the data in this analysis are missing at random (MAR), multiple imputation was used to reduce possible bias and to increase the size of the usable sample. The multiple imputation model results had similar path coefficient estimates compared to the estimates based on the complete-case sample.
However, there are some important limitations to this analysis. First, the IFS is limited to one geographical region (Iowa). Second, participants with lower SES were more likely to leave the study before late childhood and adolescence, and these participants were not included in the multiple imputation procedure, which could lead to bias. Third, other factors, such as fluoride exposures aside from dentifrice, the use of sealants and the presence of cariogenic bacteria, have been shown to play a role in the development of caries36,37, but were not included in this analysis. Fourth, robust diagonally-weighted least squares estimation assumes the existence of an underlying “latent” continuous variable that is manifest in each categorical variable, and that this continuous variable is approximately normally distributed. Our analysis included many participants with moderate to high SES and fewer participants with low SES, and this skewness could lead to bias in the estimated path coefficients. However, based on simulation studies, this estimation technique is robust to moderate skewness of the underlying continuous variable19. Finally, there is some controversy surrounding the use of SEMs with observational data which propose causal hypotheses19,20. The proposed model was hypothesized based on substantive knowledge, and causality cannot be established from this analysis, in part due to model re-formulation and the use of observational data. However, no single study can establish causality20. Instead, this study confirms results of previous studies and provides a better conceptualization of the relationships among variables which are simply classified as predictors in other modeling frameworks.
Few authors have used SEM to examine SES and behavioral factors associated with caries incidence. Polk et al.8 found that lower SES led to higher caries incidence in Pennsylvania high school students. They observed differences in brushing frequency, use of sealants, and frequency of dental attendance with changes in SES, but changes in these mediating factors were not associated with differences in caries prevalence. Broadbent et al.9 used SEM to investigate the hypotheses that SES during childhood (ages 3-15) influences SES during adolescence and adulthood (ages 15, 26, 32), as well as oral health attitudes and behaviors in adolescence and adulthood, and that these oral health attitudes and behaviors would then influence caries and oral health-related quality of life into adulthood. In their final model, they found that nearly all hypothesized paths were statistically significant. In our analysis, female participants had more caries despite better oral health behaviors, described by higher tooth brushing frequency and more frequent dental visit attendance. Examination of the direct relationship between childhood SES and caries later in life or differences between male and female participants by Polk et al.8 and Broadbent et al9. could have allowed for better comparison between these models and the current analysis.
Based on the relationships evident in this analysis, improved dietary and oral health habits could potentially lead to lower caries rates in late childhood and adolescence. After accounting for these behaviors, SES appears to play less of a role in caries development than previously thought. However, the effect of SES could be mediated by factors not considered in this model, such as overall diet quality and food availability38. In addition, preventive programs might need to account for differences in cariespreventive behaviors and caries between males and females, which could start in adolescence or even late childhood. Confirming the results of previous studies, children and adolescents from low-SES backgrounds should be the focus of caries-preventive programs.
Additional studies using SEM are needed to verify this study’s findings. Future studies with a less homogenous sample, especially in terms of SES, and models which include other risk factors, such as presence of cariogenic bacteria or more detailed information on behavioral factors such as the effectiveness of brushing, could address many limitations of our study, and lead to a stronger conclusion.
Acknowledgments
This study was supported by the National Institutes of Health grants R03-DE023784, R01-DE12101, R01-DE09551, UL1-RR024979, UL1-TR000442, UL1-TR001013, M01-RR00059, the Roy J. Carver Charitable Trust, and Delta Dental of Iowa Foundation.
Footnotes
MS ALEXANDRA M CURTIS (Orcid ID : 0000-0002-6742-062X)
DR JOHN WARREN (Orcid ID : 0000-0002-0090-9973)
The authors have no conflicts of interest to report.
References
- 1.U.S. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health; 2000. [Google Scholar]
- 2.Löe H. Oral hygiene in the prevention of caries and periodontal disease. Int Dent J. 2000;50:129–139. doi: 10.1111/j.1875-595x.2000.tb00553.x. [DOI] [PubMed] [Google Scholar]
- 3.Moynihan P, Petersen PE. Diet, nutrition and the prevention of dental diseases. Public Health Nutr. 2004;7:201–226. doi: 10.1079/phn2003589. [DOI] [PubMed] [Google Scholar]
- 4.Vargas CM, Crall JJ, Schneider DA. Sociodemographic distribution of pediatric dental caries: NHANES III, 1988-1994. J Am Dent Assoc. 1998;129:1229–1238. doi: 10.14219/jada.archive.1998.0420. [DOI] [PubMed] [Google Scholar]
- 5.Dye BA, Arevalo O, Vargas CM. Trends in paediatric dental caries by poverty status in the United States, 1988-1994 and 1999-2004. Int J Paediatr Dent. 2010;20:132–143. doi: 10.1111/j.1365-263X.2009.01029.x. [DOI] [PubMed] [Google Scholar]
- 6.Story M, Neumark-Sztainer D, French S. Individual and environmental influences on adolescent eating behaviors. J Am Diet Assoc. 2002;102:S40–S51. doi: 10.1016/s0002-8223(02)90421-9. [DOI] [PubMed] [Google Scholar]
- 7.Majewski R. Dental caries in adolescents associated with caffeinated carbonated beverages. Pediatr Dent. 2001;23:198–203. [PubMed] [Google Scholar]
- 8.Polk DE, Weyant RJ, Manz MC. Socioeconomic Factors in adolescents’ oral health: are they mediated by oral hygiene behaviors or preventive interventions? Community Dent Oral Epidemiol. 2010;38:1–9. doi: 10.1111/j.1600-0528.2009.00499.x. [DOI] [PubMed] [Google Scholar]
- 9.Broadbent JM, Zeng J, Foster Page LA, Baker SR, Ramrakha S, Thomson WM. Oral health-related beliefs, behaviors, and outcomes through the life course. J Dent Res. 2016;95:808–813. doi: 10.1177/0022034516634663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Warren JJ, Levy SA, Kanellis MJ. Dental caries in the primary dentition: Assessing prevalence of cavitated and noncavitated lesions. J Public Health Dent. 2002;62:109–114. doi: 10.1111/j.1752-7325.2002.tb03430.x. [DOI] [PubMed] [Google Scholar]
- 11.Warren JJ, Levy SM, Broffitt B, Kanellis MJ. Longitudinal study of non-cavitated carious lesion progression in the primary dentition. J Public Health Dent. 2006;66:83–87. doi: 10.1111/j.1752-7325.2006.tb02560.x. [DOI] [PubMed] [Google Scholar]
- 12.Marshall TA, Eichenberger Gilmore JM, Broffitt B, Stumbo PJ, Levy SM. Relative validity of the Iowa Fluoride Study targeted nutrient semi-quantitative questionnaire and the Block Kids’ Food Questionnaire for estimating beverage, calcium, and vitamin D intakes by children. J Am Diet Assoc. 2008;108:465–472. doi: 10.1016/j.jada.2007.12.002. [DOI] [PubMed] [Google Scholar]
- 13.Gilmore JME, Marshall TA, Levy SM, Stumbo PJ. Development of the Iowa bone nutrient food frequency questionnaire based on data from the US Department of Agriculture Continuing Survey of the Food Intake by Individuals. J Food Compost Anal. 2008;21:s60–s68. doi: 10.1016/j.jfca.2007.07.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Beck JD, Lawrence HP, Koch GG. A method for adjusting caries increments for reversals due to examiner misclassification. Community Dent Oral Epidemiol. 1995;23:321–330. doi: 10.1111/j.1600-0528.1995.tb00257.x. [DOI] [PubMed] [Google Scholar]
- 15.Yves R. lavaan: An R Package for Structural Equation Modeling. J Stat Softw. 2012;48:1–36. [Google Scholar]
- 16.R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing; Vienna, Austria: 2013. [Google Scholar]
- 17.Muthén BO. Goodness of fit with categorical and other non-normal variables. In: Bollen KA, Long JS, editors. Testing Structural Equation Models. Newbury Park, CA: Sage; 1993. [Google Scholar]
- 18.Muthén BO, du Toit SHC, Spisic D. Robust inference using weighted least squares and quadratic estimating equations in latent variable modeling with categorical and continuous outcomes. Unpublished technical report. 1997 Available from: http://gseis.ucla.edu/faculty/muthen/articles/Article_075.pdf.
- 19.Hoyle RH, editor. Handbook of Structural Equation Modeling. New York: Guilford; 2012. [Google Scholar]
- 20.Bollen KA. Structural Equations with Latent Variables. Wiley; 1989. (Wiley Series in Probability and Mathematical Statistics). [Google Scholar]
- 21.van Buuren S, Groothuis-Oudshoorn K. mice: Multivariate Imputation by Chained Equations in R. J Stat Softw. 2011;45:1–67. [Google Scholar]
- 22.semTools Contributors. semTools: Useful tools for structural equation modeling. 2016 Retrieved from https://CRAN.R-project.org/package=semTools.
- 23.Poulton R, Caspi A, Milne BJ, Thomson WM, Taylor A, Sears MR, Moffitt TE. Association between children’s experience of socioeconomic disadvantage and adult health: a life-course study. Lancet. 2002;360:1640–1645. doi: 10.1016/S0140-6736(02)11602-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Thomson WM, Poulton R, Milne BJ, Caspi A, Broughton JR, Ayers KM. Socioeconomic inequalities in oral health in childhood and adulthood in a birth cohort. Community Dent Oral Epidemiol. 2004;32:345–353. doi: 10.1111/j.1600-0528.2004.00173.x. [DOI] [PubMed] [Google Scholar]
- 25.Newacheck PW, Hung YY, Park MJ, Brindis CD, Irwin CE. Disparities in Adolescent Health and Health Care: Does socioeconomic status matter? Health Serv Res. 2003;38:1235–1252. doi: 10.1111/1475-6773.00174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Han E, Powell LM. Consumption Patterns of Sugar Sweetened Beverages in the United States. J Acad Nutr Diet. 2013;113:43–53. doi: 10.1016/j.jand.2012.09.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Maes L, Vereecken C, Vanobbergen J, Honkala S. Tooth brushing and social characteristics of families in 32 countries. Int Dent J. 2006;56:159–167. doi: 10.1111/j.1875-595x.2006.tb00089.x. [DOI] [PubMed] [Google Scholar]
- 28.Hamasha AA, Warren JJ, Levy SM, Broffitt B, Kanellis MJ. Oral health behaviors of children in low and high socioeconomic status families. Pediatr Dent. 2006;28:310–315. [PubMed] [Google Scholar]
- 29.Palmer CA, Kent R, Loo CY, Hughes CV, Stutius E, Pradhan N, Dahlan M, Kanasi E, Arevalo Vasquez SS, Tanner AC. Diet and caries-associated bacteria in severe early childhood caries. J Dent Res. 2010;89:1224–1129. doi: 10.1177/0022034510376543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Lukacs JR, Largaespada LL. Explaining sex differences in dental caries prevalence: Saliva, Hormones, and “Life-History” Etiologies. Am J Hum Biol. 2006;18:540–555. doi: 10.1002/ajhb.20530. [DOI] [PubMed] [Google Scholar]
- 31.Martinez-Mier EA, Zandona AF. The impact of gender on caries prevalence and risk assessment. Dent Clin N Am. 2013;57:301–315. doi: 10.1016/j.cden.2013.01.001. [DOI] [PubMed] [Google Scholar]
- 32.Warren JJ, VanBuren J, Levy SM, Marshall TA, Cavanaugh JE, Curtis AM, Justine K, Weber-Gasparoni K. Dental Caries Clusters Among Adolescents. Community Dent Oral Epidemiol. doi: 10.1111/cdoe.12317. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Almonaitiene R, Balciumiene I, Tutkuviene J. Factors influencing permanent teeth eruption. Baltic Dent Maxillofac J. 2010;12:67–72. [PubMed] [Google Scholar]
- 34.Shaffer JR, Wang X, McNeil DW, Weyant RJ, Crout R, Marazita ML. Genetic susceptibility to dental caries differs between the sexes: A family-based study. Caries Res. 2015;49:133–140. doi: 10.1159/000369103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Iannotti RJ, Wang J. Trends in physical activity, sedentary behavior, diet and BMI among US adolescents, 2001-2009. Pediatr. 2013;132:606–614. doi: 10.1542/peds.2013-1488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Azarpazhooh A, Main PA. Pit and fissure sealants in the prevention of dental caries in children and adolescents: A systematic review. J Can Dent Assoc. 2008;74:171–177. [PubMed] [Google Scholar]
- 37.Relvas M, Coelho C, Velazco Henriques C, Ramos E. Cariogenic bacteria and dental health status in adolescents: the role of oral health behaviors. Eur J Paediatr Dent. 2014;15:281–287. [PubMed] [Google Scholar]
- 38.Kell KP, Judd SE, Pearson KE, Shikany JM, Fernandez JR. Associations between socio-economic status and dietary patterns in US black and white adults. Br J Nutr. 2015;113:1792–1799. doi: 10.1017/S0007114515000938. [DOI] [PMC free article] [PubMed] [Google Scholar]