

Abstract
Regular alcohol consumption in unfamiliar social settings has been linked to problematic drinking. A large body of indirect evidence has accumulated to suggest that alcohol’s rewarding emotional effects—both negative-mood relieving and positive-mood enhancing—will be magnified when alcohol is consumed within unfamiliar vs. familiar social contexts. But empirical research has never directly examined links between contextual familiarity and alcohol reward. In the current study, we mobilized novel ambulatory technology to examine the effect of social familiarity on alcohol reward in everyday drinking contexts while also examining how alcohol reward observed in these field contexts corresponds to reward observed in the laboratory. Heavy social drinking participants (N=48, 50% male) engaged in an intensive week of ambulatory assessment. Participants wore transdermal alcohol sensors while they reported on their mood and took photographs of their social contexts in response to random prompts. Participants also attended two laboratory beverage-administration sessions, during which their emotional responses were assessed and transdermal sensors were calibrated to estimate BrAC (eBrAC). Results indicated a significant interaction between social familiarity and alcohol episode in everyday drinking settings, with alcohol enhancing mood to a greater extent in relatively unfamiliar vs. familiar social contexts. Findings also indicated that drinking in relatively unfamiliar social settings was associated with higher eBrAC’s. Finally, results indicated a correspondence between some mood effects of alcohol experienced inside and outside the laboratory. This study presents a novel methodology for examining alcohol reward, and indicates social familiarity as a promising direction for research seeking to explain problematic drinking.
Keywords: Alcohol, emotion, social context, ambulatory methodology, familiarity
Researchers have long held that an understanding of alcohol’s emotional rewards is integral to an understanding of alcohol use disorder (AUD) (Blane & Leonard, 1999; Koob & Le Moal, 1997). Emotions are critical determinants of action—people are motivated to behave in ways that increase pleasure and decrease pain (Keltner & Gross, 1999). Drinkers report that alcohol consumption carries powerful emotional rewards, and that a primary factor motivating their drinking is alcohol’s ability to enhance positive mood and to relieve distress (Cooper, Frone, Russell, & Mudar, 1995; Jones, Corbin, & Fromme, 2002). Importantly, the intensity of emotional reward from alcohol longitudinally predicts drinking outcomes, with greater mood enhancement from alcohol predicting more severe drinking trajectories over time (King, de Wit, McNamara, & Cao, 2011; King, McNamara, Hasin, & Cao, 2014).
Scores of studies, conducted over the course of decades, have examined variation in emotional responses to drinking (Levenson, Sher, Grossman, Newman, & Newlin, 1980; Wilson & Abrams, 1977). Of note, a central focus of this line of research has been characteristics of the individual drinker. Researchers have examined a host of individual difference criteria as moderators of alcohol response, including genetic profile (Creswell et al., 2012), personality (Hefner & Curtin, 2012), cognitive capabilities (Sher, Bartholow, Peuser, Erickson, & Wood, 2007), gender (Fairbairn, Sayette, Aalen, & Frigessi, 2015), family history (Finn & Pihl, 1987), and alcohol expectancies (Sher, 1985). Conspicuously absent from this exploration has been a consideration of drinking context. In other words, in seeking to understand differences in alcohol emotional reward and thus elucidate mechanisms of risk for AUD, researchers have focused overwhelmingly on the “who” of the drinker rather than the “where” of the drinking setting (Corbin, Scott, Boyd, Menary, & Enders, 2015; Fromme & Dunn, 1992). Of note, an exclusive focus on the individual is largely incapable of accounting for the substantial variation in rates of AUD that are observed at the level of geographic region and cultural group membership (Heath, 1995; World Health Organization, 2014), and further seems perplexing in light of the premise, put forward in some of the most prominent theories of alcohol’s effects, that it is context that serves as the primary moderator of alcohol’s emotional rewards (e.g., Steele & Josephs, 1990). The current study employs multiple methods to address this research gap, examining contextual moderators of alcohol’s mood enhancing effects in order to elucidate pathways of AUD risk.
Social Context and Social Familiarity
The contexts in which people typically consume alcohol are highly variable. Individuals may drink alcohol at home in their living room, in a crowded club, at a formal cocktail party, or outside on a clear day (Heath, 2000; Single & Wortley, 1993). One factor that varies across contexts, and is known to influence peoples’ emotions, are the social characteristics and nature of the relationships among individuals present (Fairbairn & Sayette, 2014). Humans are fundamentally social beings (Baumeister & Leary, 1995; Bowlby, 1969). The need to belong, to form social connections with other individuals, has been identified as a core human motive (Baumeister & Leary, 1995) and, importantly, alcohol is believed to interact with social factors in a variety of ways thought relevant for the understanding of AUD and AUD risk (Fairbairn & Sayette, 2014). For example, research indicates that, among both problem and non-problem drinkers, the majority of alcohol consumption takes place in social contexts (Bourgault & Demers, 1997; Single & Wortley, 1993), that alcohol’s emotional rewards are significantly more pronounced when alcohol is consumed in the presence of other individuals vs. when it is consumed alone (Armeli et al., 2003; Doty & de Wit, 1995; Kirkpatrick & de Wit, 2013; Pliner & Cappell, 1974), and the expectation that alcohol will enhance social interactions is among the more robust predictors of AUD (Fairbairn & Sayette, 2014; Jones et al., 2002).
One factor that varies considerably across drinking contexts is the drinker’s level of social familiarity with individuals present. Importantly, evidence has accumulated to indicate a link between drinking in the company of unfamiliar individuals and risk for AUD (Fairbairn & Sayette, 2014). Regular drinking among strangers and/or within contexts that facilitate stranger interaction (e.g., public drinking establishments, large parties, social groups including unfamiliar individuals) is a robust predictor of heavy drinking (e.g., S. A. Brown, 1985; Casswell & Zhang, 1997; Scribner et al., 2008; Senchak, Leonard, & Greene, 1998). In contrast, drinking mainly among familiar individuals (e.g., within families, couples, and close friend groups) has been indicated as a potential protective factor against problem drinking (e.g., Ahlström-Laakso, 1976; Reboussin, Song, & Wolfson, 2012; Roberts & Leonard, 1998; Room & Makela, 2000). Further, and importantly, key factors determining the likelihood that an individual will encounter unfamiliar social settings also represent what are among the most robust risk factors for AUD (e.g., metropolitan dwelling, young age, male gender). Although alternative mechanisms have been proposed to partially explain the relationship between some of these factors and AUD, their sheer number and diversity—spanning realms from developmental to geographical—indicates that social familiarity is overdue for systematic investigation as a framework for understanding mechanisms of AUD risk (Fairbairn, 2017; Fairbairn & Bresin, 2017; Fairbairn & Sayette, 2014).
One possible explanation for links between unfamiliar drinking contexts and problematic consumption is that individuals experience heightened emotional reinforcement from alcohol when drinking in unfamiliar contexts (Fairbairn & Sayette, 2014). Importantly, alcohol’s ability to boost mood in the face of stress is pronounced under specific conditions including when outcomes are perceived as uncertain or unpredictable (Hefner & Curtin, 2012; Moberg & Curtin, 2009), when the stressor induces a negative consciousness of self (Hull, 1981, 1987) and/or when stressors evoke a mixture of negative and also positive emotions (Curtin, Lang, Patrick, & Stritzke, 1998; Steele & Josephs, 1990; Stritzke, Lang, & Patrick, 1996). Unfamiliar social contexts possess all three of these characteristics, reliably evoking negative emotions connected with feelings of both uncertainty (Berger & Calabrese, 2006) and self-consciousness (Leary & Kowalski, 1995), while at the same time offering the promise of particularly potent positive feelings associated with the acquisition of a new social relationship (Baumeister & Leary, 1995). Within our social-attributional model of alcohol’s mood enhancing effects, we predicted that alcohol reward will be most pronounced when consumed in the presence of unfamiliar vs. familiar individuals (Fairbairn & Sayette, 2014), a premise for which we subsequently produced some support using meta-analytic methods (Fairbairn, 2017) as well as within a questionnaire-based alcohol expectancy study (Fairbairn & Bresin, 2017). But empirical research has yet to directly test this premise.1 The present study looks to real-life drinking settings to fill this gap, employing novel ambulatory technology to better understand the effects of alcohol and familiarity in the real-life contexts in which alcohol is actually consumed.
Measuring Alcohol’s Effects in Everyday Drinking Contexts
Ambulatory methods have enormous potential for capturing alcohol response across a range of real-life drinking contexts (Trull & Ebner-Priemer, 2013). Until recently, however, the range of measures available for assessing experience in everyday life was limited, and so researchers were forced to rely overwhelmingly on self-reports to assess alcohol use and elements of the ambulatory environment (Shiffman, Stone, & Hufford, 2008). It has been argued that self-reports can often represent the most appropriate choice for assessing particular aspects of experience, such as internal subjective responses and mood states (Fairbairn & Sayette, 2013; Robinson & Clore, 2002). However, researchers have raised a number of concerns with self-report measures of alcohol use, noting that drinkers may not always be aware of the alcohol content of the beverages they consume and, further, that alcohol’s effects on cognition may impair memory abilities required for self-report, particularly at very high levels of consumption (Shiffman, 2009). Researchers have also sometimes noted the limits of in-vivo self-reports for assessing context, since some environmental elements (e.g., precise level of acquaintance with all individuals present) may be burdensome and complex to assess in the moment and might also potentially lead to measurement reactivity (Barta, Tennen, & Litt, 2012). These issues emerge as particularly concerning within the context of an examination of social drinking behaviors, since research suggest that alcohol depletes cognitive resources and impairs memory to an even greater extent when drinking is combined with other cognitively taxing activities such as social interaction (Josephs & Steele, 1990; Steele & Josephs, 1990).
Perhaps partially due to the challenges surrounding the assessment of alcohol’s effects in everyday contexts, researchers have often chosen to examine the acute effects of alcohol on emotion in laboratory settings (Sayette, 1993; Sher, Wood, Richardson, & Jackson, 2005). Often focusing on negative mood outcomes and on contextual manipulations intended to be aversive (Sayette, 1993), laboratory-based alcohol-administration studies allow researchers to precisely measure and manipulate alcohol intoxication and context of consumption (Fairbairn & Sayette, 2014). While alcohol-administration procedures offer key advantages when causal inference is the point of central interest, laboratory paradigms are unlikely to capture the variety of social relationships and the range of emotional experiences that manifest outside the lab (Wilhelm & Grossman, 2010). It is also worth noting that the correspondence between alcohol response inside and outside the laboratory has not been explicitly tested. Thus, while it might be assumed that emotional response to alcohol is similar inside and outside the laboratory, and some evidence suggests that this may be the case (Sher & Wood, 2005; Sher et al., 2005), the extent to which laboratory contexts capture alcohol emotional reinforcement as it is typically experienced outside the lab is as yet unknown.
Another option for understanding emotional response to alcohol has emerged with recent technological advances for ambulatory assessment. Within the past several decades, transdermal measures of alcohol consumption have emerged, providing capabilities for the measurement of alcohol use through the analysis of fluids excreted through the skin (Swift & Swette, 1992). Blood alcohol content (BAC) cannot be estimated from transdermal data alone, since individual-level parameters, such as the thickness of the skin, can lead to differing transdermal readings and differing latency to peak across individuals at the same alcohol dose (Luczak & Rosen, 2014). But procedures have recently been developed that use breathalyzer readings (BrAC) derived from an alcohol-administration “calibration” session, thus enabling researchers to translate transdermal readings into BAC or BrAC estimates (eBAC/eBrAC) for each individual and device (Dumett et al., 2008; Luczak & Rosen, 2014; Rosen, Luczak, & Weiss, 2014). Recent decades have also seen significant progress in methods for digital capture and storage of photographic images, presenting new possibilities for the examination of environments and environmental cues (Mehl & Conner, 2013). These image-capture methods have been used to assess a range of environmental factors, including substance use and cues to substance use (Conklin, 2006; Luczak, Rosen, & Wall, 2015), and have been combined with cued self-report procedures completed retrospectively to gather more information on contextual factors (N. A. Brown, Blake, & Sherman, in press).
The Present Study
The current study mobilizes novel ambulatory technology combined with laboratory alcohol-administration procedures to explore the effects of contextual factors on alcohol’s emotional rewards. Ambulatory procedures involve continuous, transdermal assessment of alcohol consumption together with real-time photographic image-capture measures of context to examine alcohol’s emotional rewards in real-life drinking environments. We pair these novel ambulatory methods with experimental beverage administration procedures during which alcohol’s emotional effects are assessed in a laboratory (unfamiliar) social drinking environment2 and, importantly, transdermal sensors are calibrated for each individual in the study.
The study includes an intensive, 1-week period of ambulatory assessment and examines alcohol use among a sample of relatively heavy drinkers—individuals who typically engage in multiple drinking episodes within a 7-day span. Heavy drinkers are not only of clinical interest because of their enhanced risk for developing AUD later on, but, in addition, their current heavy drinking behavior (i.e., frequent binge drinking) represents a significant problem that has been associated with major economic and interpersonal costs (Bouchery, Harwood, Sacks, Simon, & Brewer, 2011; Hingson, Zha, & White, 2017; Sacks, Gonzales, Bouchery, Tomedi, & Brewer, 2015; Wechsler, Lee, Kuo, & Lee, 2000).
Our primary aim in the current study is to examine the hypothesis that alcohol-related positive mood enhancement and negative mood reduction are more pronounced in relatively unfamiliar vs. familiar everyday drinking settings. A secondary aim of the study is to examine the impact of laboratory vs. real-world drinking settings on alcohol-related mood enhancement, examining the extent to which alcohol-reward experienced inside the laboratory corresponds to alcohol-reward in everyday drinking contexts.
Methods
Participants
Participants consisted of 48 heavy social drinkers, recruited via internet advertisements and posted notices in the local community, and via friend referrals from other participants. Exclusion criteria included medical conditions that contraindicated alcohol consumption, a diagnosis of Alcohol Use Disorder as indexed by the Diagnostic and Statistical Manual of Mental Disorders (5th ed.), pregnancy in women and being uncomfortable with study drinking requirements. Potential participants with a body mass index (BMI) less than 19 or greater than 27 were excluded, due to alcohol dosing requirements. Of participants, 56% were European American, 13% were African American, 6% were Hispanic, and 17% were Asian. Half the participants were men and half women, with an average age of 22.6 (range 21-28 years old). At baseline, participants reported drinking an average of two to three times per week and consuming 3.8 (SD = 1.7) drinks/occasion. Participants reported binge drinking on an average of 3.8 days in the past month, and 40% of participants (N=19) reported at least one episode of extreme binge drinking (>=8 standard drinks in a sitting for women and >=10 standard drinks in a sitting for men) in the past month (Hingson et al., 2017). All participants in our study met the National Institute on Alcohol Abuse and Alcoholism’s criteria for heavy or “at risk” drinking (NIAAA, 2017). The 48 individuals enrolled in the current study represent those participants who were assigned to the ambulatory procedures described below—the larger laboratory study involved a total of 60 individuals.3
Procedures
Study Initiation and Ambulatory Orientation
Participants who met eligibility criteria were invited to a study initiation visit, where they were oriented to ambulatory assessment procedures and fitted with the transdermal sensor. Participants were instructed not to drink alcohol for at least 12 hours prior to all laboratory visits and were breathalyzed (Intoximeters Alco Sensor IV) upon arrival at the laboratory to ensure 0.00 BrAC. Consistent with our prior work, participants attended all laboratory visits in groups of 3 individuals, a measure taken to increase the ecological validity of our laboratory drinking context (Sayette et al., 2012). Participants attended all 3 visits with the same group of individuals to ensure that, as much as possible, all conditions were held constant across the experimental beverage-administrations sessions aside from beverage content. Measures were taken to ensure that members of these laboratory drinking groups were not previously acquainted prior to study participation (see Sayette et al., 2012; see also footnote 2).
During this study initiation visit, participants were fitted with transdermal sensors (see measures below) and were oriented to the ambulatory assessment procedures in separate rooms. Participants were informed that, for the next 7-days, in addition to wearing the transdermal sensor, they would be completing surveys in response to random prompts. They were informed that they would receive 6 prompts a day and that, within 15 minutes of the prompts sounding, they would need to report on their mood and provide a photograph of their surroundings. Participants were instructed to respond to prompts using the Metricwire survey app (Trafford, 2016) directly on their smartphones or, for those who did not own smartphones, on one of the laboratory’s iPod touch devices. After responding to mood items (see below), participants were instructed to take a photograph of “your environment right now. Take a picture of what you see” (see Figure 1 for example photos taken by participants). Participants were instructed to capture as much as possible of their current setting (e.g., to zoom out and/or take a step back to get the entire scene). After taking photographs, participants also supplied brief captions describing the scene depicted—i.e., what they are currently doing. Participants also supplied daily self-reports regarding their alcohol consumption (see below).
Figure 1.

Participants in the current study took photographs of their environments in response to random prompts, and then indicated their precise relationship with individuals featured in photographs through our photo-cued task. Above are a selection of photographs taken by participants displaying social drinking contexts. All participants whose photographs are displayed above consented for the dissemination of their photos in scientific publications. For the sake of publication, we mask the faces of the individuals displayed in photographs (photographs displayed to participants in the photo-cued task were, of course, unmasked).
Beverage Administration Sessions
Following the study initiation visit, each participant attended 2 beverage administration sessions, both held at approximately 3pm. The first of these sessions was held 4 days after the study initiation visit, and the second visit occurred 7 days after the study initiation visit (see Figure 2 for timeline). The first of these visits overlapped with the period of intensive ambulatory assessment, and thus functioned as a combined experimental visit and ambulatory compliance check-in, encouraging compliance with procedures. Participants did not respond to ambulatory assessment prompts during experimental laboratory procedures. During one of these experimental sessions, groups were administered an alcoholic beverage and, during the other session, they were administered a control beverage, with the order of sessions being counterbalanced across groups.
Figure 2.
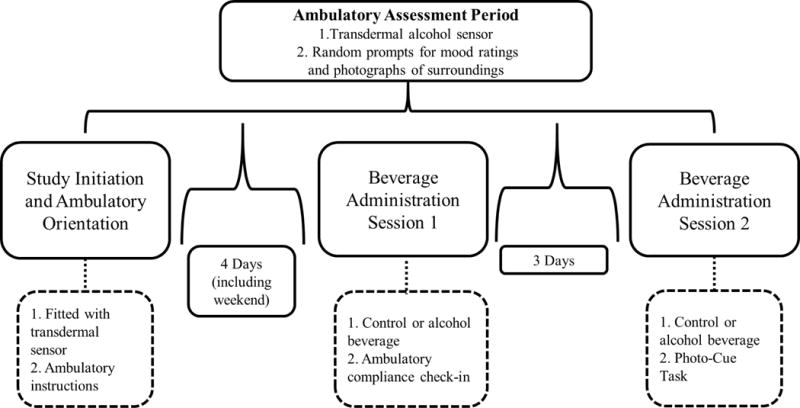
A timeline of experimental and ambulatory procedures. In the current study, one experimental laboratory visit (Beverage Administration Session 1) overlapped with the period of ambulatory assessment. The issue of reactivity to experimental procedures is addressed in the results section.
During both beverage administration sessions, the three participants were seated together around a round table for drink administration (Sayette et al., 2012). During the alcohol session, participants consumed an alcoholic beverage consisting of 1 part 100-proof vodka and 3.5 parts cranberry juice. To adjust for gender effects, men in the alcohol condition were administered a 0.82 g/kg dose of alcohol, and women were administered a 0.74 g/kg dose (Sayette, Martin, Perrott, Wertz, & Hufford, 2001). On the control session, participants consumed an isovolumic amount of cranberry juice, and were not deceived about the content of their beverages. Our choice to omit the placebo condition was driven by a variety of considerations, including research suggesting that placebo manipulations can lead to unanticipated compensatory effects (Fairbairn, Sayette, Amole, et al., 2015; Testa et al., 2006). Participants remained seated for a total of 36 min while beverages were administered in three equal parts at 0 min, 12 min, and 24 min.
Immediately after drinking, we recorded participants’ BrACs, and they were brought into separate rooms to complete measures of mood (see below). They then performed some additional cognitive tasks unrelated to the current research questions. On their final experimental session, before leaving the laboratory, participants engaged in our photo-cued self-report task (see measures below). When the final session coincided with an alcohol-administration session, participants only completed the photo-cued self-report task after their BrAC’s dropped below .04%. In addition, all participants except the first 5 groups enrolled in the study reported on the extent to which ambulatory procedures impacted the amount they drank, their mood, and the contexts in which they drank alcohol. During the alcohol session, participants were required to remain in the laboratory until their BrAC dropped below .03% and/or transdermal alcohol readings had reached a peak and begun to descend. Upon completion of the final experimental session, participants were paid $160 for attending all laboratory sessions and for wearing the transdermal sensor, and a bonus of $40 for responding to at least 70% of the ambulatory assessment prompts.
Measures
Ambulatory Alcohol Consumption
The Secure Remote Alcohol Monitoring System (SCRAM©; Alcohol Monitoring Systems, Inc., Littleton, CO) bracelet—a device that fits around participants’ ankles—was used to measure transdermal alcohol concentration (TAC). SCRAM was chosen as the device that is currently the most reliable and valid transdermal alcohol-sensor (Leffingwell et al., 2013). Readings derived from transdermal sensors were translated into eBrAC estimates of BrAC using the BrAC Estimator software, a Matlab code based on a first principles forward model for the transport of alcohol from the blood through the skin and measurement by a transdermal sensor (Dumett et al., 2008; Luczak & Rosen, 2014; Luczak, Rosen, & Weiss, 2013; Rosen, Luczak, Hu, & Hankin, 2013; Rosen et al., 2014). The parameters in the model are estimated or tuned to the particular device and participant using BrAC and TAC data collected at the laboratory-calibration session attended by all study participants, during which simultaneous breathalyzer and transdermal readings were taken (see Figure S1).
For the purposes of examining mood effects, our continuous eBrAC output was then converted into a binary variable distinguishing alcohol vs. no-alcohol episodes (Barnett, Meade, & Glynn, 2014; Barnett, Tidey, Murphy, Swift, & Colby, 2011). In these analyses, we did not examine eBrAC as a continuous predictor of mood for several reasons including: 1) Our laboratory examination of alcohol mood effects was necessarily binary, as only one dose of alcohol was administered in the lab, and so an examination of a binary alcohol variable in the field facilitated the comparison of laboratory to ambulatory alcohol effects (our secondary study aim); and 2) Our sample engaged in heavier drinking practices, and at higher doses, the relationship between BAC and subjective reinforcement becomes non-linear (Pohorecky, 1977). A cutoff of .01% eBrAC was chosen as a threshold for determining an alcohol episode—participants whose eBrAC>=.01% at the time of a mood/context (ambulatory survey) assessment were classified as engaging in an alcohol episode. The .01% eBrAC cutoff was selected as the threshold at which the average of all ambulatory eBrAC estimates for alcohol episodes was equivalent to the .08% alcohol dose administered in the laboratory, and so this threshold was selected to facilitate comparison across laboratory and ambulatory alcohol effects. While our mood models focused mainly on binary alcohol effects (although see supplementary models), continuous eBrAC scores, as well as peak eBrAC values reached within a given drinking episode, were examined in our analysis of drinking outcomes.
In addition to our primary transdermal measure of alcohol consumption, we assessed participants’ drinking via two secondary measures, used as internal validation checks of transdermal alcohol data: 1) Participants provided daily self-reports of their alcohol consumption via ambulatory survey prompts, indicating the precise number of standard drinks they had consumed on the previous day; 2) The photographs taken by participants together with their accompanying captions were coded for evidence of drinking (e.g., people drinking and/or drinking paraphernalia displayed in photographs and/or text indicative of alcohol consumption in captions). One research assistant coded all photographs, and a second coded a random sub-sample for reliability (average agreement across coders was 95%).
Mood
Laboratory positive and negative mood was assessed using an 8-item mood scale. This measure was chosen as one that had proven sensitive to alcohol’s effects in a laboratory context within our prior research (Fairbairn, Sayette, Wright, et al., 2015; Fairbairn & Sayette, 2013). The eight-item mood measure indexes four negative mood states (annoyed, sad, irritated, bored) and four positive mood states (cheerful, upbeat, happy, content), selected to represent all quadrants of the affective circumplex (Russell, 2003). Participants responded on a 6-point Likert scale from 0 (not at all) to 5 (extremely). The negative and positive items were averaged to create separate subscales (α = .64 for negative scale4, α = .89 for positive scale).
In constructing the ambulatory mood measure, we chose the six mood items—3 positive and 3 negative—from the laboratory 8-item mood measure indicated by our prior research as being most sensitive to alcohol’s effects. With a view to avoiding anchoring effects and eliciting variation in response, we referenced research on emotion and also ambulatory alcohol response (Armeli et al., 2003; Yik, Russell, & Steiger, 2011) and also consulted a team of 13 lab assistants, to select 4 additional mood items. This process produced a ten-item ambulatory mood measure including five negative mood states (nervous, sad, irritated, lonely, bored; α = .62) and five positive mood states (upbeat, content, happy, euphoric, energized; α = .90).
Social Context and Social Familiarity
Contextual familiarity in everyday settings was assessed via a photo-cued self-report task (N. A. Brown et al., in press)—the last task completed by all participants on their final day in the study. Within this task, participants self-reported on their level of acquaintance with all individuals featured in the photographs they took during the ambulatory assessment period. We chose to assess social familiarity using this photo-cued self-report paradigm, rather than simply asking participants to report on familiarity within the ambulatory surveys themselves, for the following reasons: 1) As participants might often find themselves in relatively large social groups, we were concerned that the length of surveys required to assess individual relationships in such groups would lead to haphazard responding (Shiffman et al., 2008); 2) As noted earlier, level of familiarity in social settings is closely related to mood. Given this relationship, we thought it not implausible that, by making familiarity salient to participants through repeated questioning, in-vivo mood might be impacted, thus confounding our independent and dependent variables. Note that the oldest picture participants reviewed in this task was seven days old, and so we viewed recall bias as a relatively minor concern (N. A. Brown et al., in press).
A software program—custom-designed for the purposes of this experiment—displayed each photograph that featured other individuals to participants together with questions concerning individuals in the photographs. Within the program, each screen identified a specific individual (e.g., 2nd person from the left) together with accompanying questions about that individual. We assessed participants’ social familiarity using 3 items: 1) Participants indicated their relationship with the individual pictured, using the following categories—romantic partner, family member, close friend, friend, acquaintance, coworker, stranger, or other. In choosing the stranger category, participants were instructed to consider their relationship with that individual at the time the photo was taken (rather than at the time of review); 2) Participants indicated the number of years they had known the individual (Years Known); 3) In order to assess not only the time of initial contact, but also the amount of time spent together over the course of the relationship (Starzyk, Holden, Fabrigar, & MacDonald, 2006), participants estimated the total number of hours they had spent in the individual’s company at the time the photograph was taken (Time Spent). Participants were given benchmarks for translating the frequency of their interaction and total time of acquaintance into total number of hours. Familiarity in ambulatory settings was estimated at the level of the context—by summing the total number of individuals in the case of the Number of Strangers variable, or averaging across ratings of each individual in the case of the Time Spent and Years Known variables.
Physical Location
A research assistant categorized all photographs according to the physical context depicted—1-Outdoors; 2-Private Home/Residence; 3-Bar/Club/Restaurant; 4-Work/school; 5-Other. A 2nd research assistant then coded a random sub-sample of 40 photographs for reliability (100% interrater agreement).
Data Analysis Plan
We used multilevel modeling to examine alcohol’s effects on mood within both laboratory and ambulatory data (Raudenbush & Bryk, 2002). Ambulatory models incorporated 2 levels of analysis—within person and between person. Laboratory models incorporated 3 levels of analysis—within person (2 experimental sessions), within groups (3-person drinking groups), and between groups.
In ambulatory models we incorporated several covariates, since conditions were not randomly assigned, including adjustments for time of day and day of the week at level-1, and basic demographic variables (gender, age, and typical drinking patterns) at level 2 (Miranda et al., 2014; Piasecki, Wood, Shiffman, Sher, & Heath, 2012). In examining the main effect of alcohol in ambulatory settings, we parsed between- from within-subject effects by centering alcohol episode for each individual at level-1, and then entering individual-level averages at level-2 (Raudenbush & Bryk, 2002).
Level of social familiarity was examined primarily within observations featuring social contexts (i.e., where photographs featured at least one other individual aside from the participant)—social context itself (i.e., others featured vs. no others featured) was examined as a moderator of alcohol’s effects in separate analyses. Familiarity was entered into models as a continuous variable and, where analyses indicated a significant moderation effect, we examined simple contrasts by centering familiarity at one standard deviation above and below the mean. To examine correlations between ambulatory and laboratory effects, an effect was estimated for each individual and then the relationship between these individual-level variables was examined within regression models.
Results
Overall Attrition and Compliance
Rates of compliance were high. No participants dropped out of the study and no participants who attended the study initiation visit missed either of the laboratory beverage-administration visits. Participants responded to an average of 93.1% of prompts (SD=10.6).
Laboratory Manipulation Check
On alcohol-administration laboratory sessions, participants were on the ascending limb of the BrAC curve immediately following the interaction period (M=0.064%; SD=.01), ultimately rising to a peak BrAC of .074% (SD=.01) about 60 minutes post-interaction.
Ambulatory Alcohol Consumption
All but 3 participants (94%) engaged in at least one drinking episode outside the laboratory over the 7-day ambulatory assessment period. On average, participants drank on 3.3 days (SD=1.56), not counting drinks consumed during the laboratory visit, with an average eBrAC of .081% (SD=.11) on drinking episodes.
eBrAC corresponded closely with both daily self-reports of drinking and also with momentary drinking data. The correlation between daily self-reports of the number of drinks and the daily average eBrAC was large in magnitude, β=.73, t=5.66, p<.0001. With respect to the momentary drinking data, when photographs and/or their accompanying captions indicated a drinking setting, 82% of the time the eBrAC also was positive for that same time point.
Ambulatory Mood and Context—Descriptive Statistics
Overall, 31% of photographs taken by participants depicted social contexts (i.e., other people). On average, participants took 10.21 (SD=6.03) photographs depicting social contexts, showing an average of 4.29 (SD=7.03) people per photograph. Of these photographs, 33% contained at least one individual identified by participants as a “stranger” at the time the photo was taken, 39% contained a “close friend,” 26% a “friend,” 5% a family member, 14% a romantic partner, 9% a coworker, and 9% an “acquaintance.” Reports of positive mood were higher, b= 0.37, SE=.049, t=7.58, p<.0001, and reports of negative mood were lower, b=-0.14, SE=.025, t=-5.78, p< .0001 when photos depicted others present (i.e., social contexts) vs. when photographs depicted no other individuals present. Within social contexts, negative mood increased with the number of strangers present, b=.01, SE=.004, t=3.36, p=.0008, and decreased with the average amount of time participants reported previously spending in these individuals’ company, b=-.01, SE=.006, t=-2.37, p=.02.5 Participants in our study did revisit the same physical spaces during ambulatory assessment—photos displayed an average of 18.29 (SD=5.53) unique contexts per participant. Repeated photographs of the same contexts were more common when participants were alone vs. when they were in social settings, such that only 26% of photographs taken in social settings, and even fewer (13%) photographs taken in unfamiliar social settings, represented repetitions of previous contexts.
Measurement Effects and Reactivity
Most participants did not report substantial reactivity to the transdermal sensor and/or the photo/survey procedures. One participant indicated that s/he drank more than usual because of the ambulatory procedures, 6 participants indicated that they were sometimes made uncomfortable or irritated by the ambulatory procedures, and one participant indicated that the ambulatory procedures impacted the settings in which s/he drank alcohol (noting that s/he avoided bars a bit more than usual).
The period for ambulatory assessment overlapped with the first experimental visit (see Figure 2), but we did not observe substantial reactivity to laboratory procedures. Specifically, there was no significant difference in either positive mood, p=.40, or negative mood, p=.49, between subjects who had been assigned to receive alcohol first vs. control beverage first on the day following this experimental session. Participants who had been assigned to consume alcohol appeared to drink slightly less alcohol on the day following this session, than those who had been assigned to consume control beverage but the difference in average eBrAC was not large (.012%, p=.03).
Main Effects of Alcohol
Next, we examined the effects of alcohol on mood in both laboratory (alcohol session vs. control session) and ambulatory (alcohol episode vs. no-alcohol episode) arms of the study. In the laboratory arm of the study, positive mood was higher, β=.36, t=3.81, p=.0003, and negative mood lower, β=-.30, t=-3.46, p=.0009, following beverage administration on alcohol sessions (Positive Mood: M= 4.61, SE=0.18; Negative mood: M=1.18, SE=0.07) vs. control sessions (Positive Mood: M= 3.84, SE=0.20; Negative mood: M=1.53, SE=0.09). In the ambulatory arm of the study, positive mood was higher, β=.13, t=4.73, p<.001, and negative mood lower, β=-.07, t=-2.62, p=.009, during alcohol episodes (Positive Mood: M=3.89, SE=1.03; Negative mood: M=1.27, SE=0.46) vs. no-alcohol episodes (Positive Mood: M=3.56, SE=1.02; Negative mood: M=1.36, SE=0.47), although effect sizes were smaller than in the laboratory arm of the study. Of note, when we decomposed effects of alcohol observed in the ambulatory arm of the study into between- and within- subject components (see data analysis plan), results indicated that the effect of alcohol on positive mood and negative mood were explained entirely by variability within-subjects (Positive Mood: b=0.33, SE=.069, t=4.82, p<.0001; Negative Mood: b=-0.08, SE=.033, t=-2.57, p=0.01), and not by variability between subjects, p’s>.41.
In terms of the correspondence between laboratory and ambulatory effects, across both measures of positive mood, β=.58, t=4.81, p<.0001, and measures of negative mood, β=.57, t=4.68, p<.0001, an individual’s average mood score measured inside the laboratory was related to that individual’s average mood measured outside the laboratory. In terms of concordance in the effects of alcohol, the effect of alcohol on an individual’s negative mood in a laboratory setting was related to the effect of alcohol on that individual’s negative mood outside the laboratory, β=.31, t=2.18, p=.035. The relationship between ambulatory and laboratory measures of alcohol’s effects on positive mood did not reach significance, β=-.15, t=-1.01, p=.32. These effects remained unchanged when only the 6 mood items that overlapped across ambulatory and laboratory mood assessments (see methods) were examined (Negative mood: β=.36, t=2.59, p=.013; Positive mood: β=-.05, t=-.34, p=.74).6
Moderating Effects of Social Context
Findings indicated an interaction between alcohol episode and social context in predicting both positive mood, b= 0.27, SE=.124, t=2.18, p=.03, and negative mood, b= −0.18, SE=.055, t=-3.35, p=.0008. In social contexts (i.e., when photographs displayed other individuals present) there was a significant main effect of alcohol on mood, with positive mood being higher, b=0.43, SE=.091, t=4.73, p<.0001, and negative mood being lower, b= −0.17, SE=.043, t=-3.95, p<.0001, during alcohol episodes vs. no-alcohol episodes. In contrast, when participants were alone, the main effects of alcohol on mood did not reach significance (Positive Mood: b= 0.16, SE=.087, t=1.84, p=.07; Negative Mood: b= 0.01, SE=.038, t=.37, p=.71). See below for further exploration of these effects.
Moderating Effects of Social Familiarity
Next, we looked within social drinking contexts themselves to address our aim of examining the extent to which social familiarity interacts with alcohol in predicting mood. Here, consistent with our hypotheses, results revealed an interaction between Number of Strangers and alcohol episode in predicting negative mood, b= −0.02, SE=.004, t=-4.59, p<.0001. Irrespective of the number of strangers present, negative mood was lower during alcohol episodes compared with no-alcohol episodes, but this alcohol effect was significantly larger in the presence of strangers, b= −0.27, SE=.040, t=-6.73, p<.0001, vs. when no strangers were present, b= −0.11, SE=.041, t=-2.75, p=.006. The interaction between Number of Strangers and alcohol episode in predicting positive mood did not reach significance, b= 0.01, SE=.011, t=1.26, p=.210.7
We next introduced a greater level of specificity into our examination of familiarity and, rather than simply examining categories of individuals, instead examined Time Spent with other individuals in drinking context as a continuous moderator of alcohol’s effects. Again, consistent with hypotheses, results revealed an interaction between Time Spent and alcohol episode in predicting both positive mood, b= −0.07, SE=.024, t=-3.06, p=.002, and negative mood, b= 0.03, SE=.012, t=2.43, p=.02. When participants indicated they had previously spent little time in the company of others present, there was a significant effect of alcohol on mood, with positive mood being higher, b=0.67, SE=.18, t=3.74, p=.0002, and negative mood being lower, b= −0.28, SE=.062, t=-4.52, p<.0001, during alcohol episodes vs. no-alcohol episodes. In contrast, when participants indicated they had previously spent a great deal of time in the company of others present, the main effects of alcohol on mood did not reach significance, p’s>.09 (Figure 3). Importantly, these results remained significant even after controlling for the physical context of drinking (see Table 1 for full results of models controlling for physical drinking context).
Figure 3.
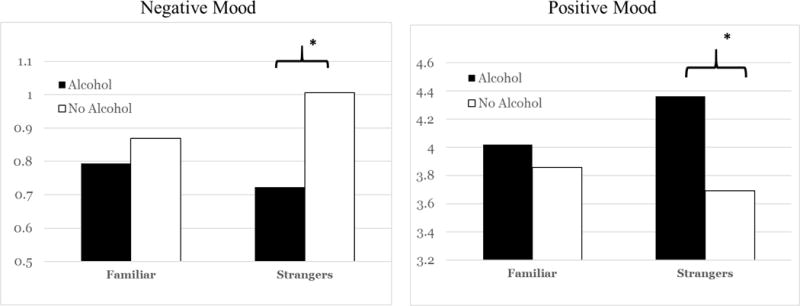
Results revealed a significant interaction between social familiarity and alcohol consumption in predicting positive mood and negative mood in everyday drinking settings. The above graphs reflect the interaction between alcohol and the familiarity variable Average Time Spent, centered at 1SD above and below the mean (-SD was equivalent to “0 hours,” labeled above as ―strangers‖).
Table 1.
The effect of social familiarity and alcohol consumption on positive and negative mood, controlling for time of day, day of the week, gender, age, typical drinking patterns, and physical location
| Number of Strangers | ||||||
|---|---|---|---|---|---|---|
|
| ||||||
| Negative Mood | Positive Mood | |||||
|
|
||||||
| b | SE | p value | b | SE | p value | |
| Strangers | 0.017 | 0.003 | <.001 | −0.009 | 0.005 | 0.049 |
| AlcoholEpsde | −0.070 | 0.037 | 0.058 | 0.191 | 0.087 | 0.029 |
| Strangers*AlcoholEpsde | −0.016 | 0.004 | <.001 | 0.008 | 0.010 | 0.431 |
| Evening | 0.019 | 0.035 | 0.581 | 0.166 | 0.084 | 0.049 |
| Weekend | −0.044 | 0.032 | 0.166 | 0.201 | 0.101 | 0.047 |
| Age | 0.003 | 0.015 | 0.859 | −0.037 | 0.042 | 0.383 |
| Drinking patterns | 0.003 | 0.005 | 0.602 | 0.014 | 0.018 | 0.434 |
| Gender | 0.115 | 0.064 | 0.079 | −0.188 | 0.198 | 0.347 |
| Location (Priv Home Ref) | ||||||
| Outdoors | 0.005 | 0.049 | 0.921 | 0.160 | 0.160 | 0.320 |
| Bar/Club/Restaurant | −0.055 | 0.033 | 0.102 | 0.230 | 0.106 | 0.032 |
| Work/School | 0.214 | 0.070 | 0.003 | −0.538 | 0.128 | <.001 |
| Other | −0.007 | 0.060 | 0.903 | 0.113 | 0.126 | 0.375 |
| Time Spent | ||||||
|---|---|---|---|---|---|---|
|
| ||||||
| Negative Mood | Positive Mood | |||||
|
|
||||||
| b | SE | p value | b | SE | p value | |
| HoursSpent | −0.017 | 0.006 | 0.008 | 0.025 | 0.019 | 0.183 |
| AlcoholEpsde | −0.230 | 0.056 | <.001 | 0.505 | 0.165 | 0.002 |
| HoursSpent* AlcoholEpsde | 0.026 | 0.012 | 0.023 | −0.063 | 0.024 | 0.008 |
| Evening | 0.017 | 0.041 | 0.679 | 0.160 | 0.086 | 0.064 |
| Weekend | −0.033 | 0.032 | 0.306 | 0.184 | 0.096 | 0.056 |
| Age | 0.006 | 0.017 | 0.737 | −0.040 | 0.040 | 0.320 |
| Drinking patterns | 0.004 | 0.005 | 0.495 | 0.013 | 0.018 | 0.464 |
| Gender | 0.126 | 0.067 | 0.065 | −0.203 | 0.196 | 0.306 |
| Location (Priv Home Ref) | ||||||
| Outdoors | 0.025 | 0.057 | 0.656 | 0.167 | 0.128 | 0.195 |
| Bar/Club/Restaurant | −0.038 | 0.035 | 0.285 | 0.215 | 0.106 | 0.045 |
| Work/School | 0.192 | 0.075 | 0.012 | −0.497 | 0.130 | <0.001 |
| Other | −0.033 | 0.064 | 0.610 | 0.162 | 0.135 | 0.232 |
Strangers=Number of strangers present in social context; HoursSpent=Average number of hours spent with individuals in social context; AlcoholEpsde=Coded 1 if eBrAC is greater than or equal to .01% and 0 if eBrAC is less than .01%; Evening=Coded 1 if 5pm-midnight and 0 if midday to 5pm; Weekend=Coded 1 if Friday-Sunday and 0 if Monday-Thursday; Drinking Patterns=The number of days/30 the participant reported drinking at baseline; Location was coded such that the reference group was house/private residence.
Next, we re-ran our primary models exploring the Alcohol X Familiarity interaction while subjecting our alcohol variable to a range of permutations, including models that examined the binary alcohol episode variable according to different thresholds (.02% and .04%) as well as models representing eBrAC in various continuous forms intended to mirror conceptual understandings of the relationship between BAC and mood, accounting for diminishing increments in reinforcement at higher doses (Pohorecky, 1977; see also Figure S2 for graphs of the relationship between eBrAC and mood in our data). These new models produced similar results to those reported above, although the Hours Spent X Alcohol interaction in predicting negative mood became a trend in most models (see Table S1).
Finally, we replicated analyses above in which we examined the overall moderating effect of social contexts (i.e., with others vs. alone), but this time we examined the extent to which social context continued to moderate alcohol’s mood enhancing effects when only familiar social contexts, and not social contexts including strangers, were considered. Of note, when we re-ran these models examining only the 67% of contexts that featured familiar individuals (see descriptive statistics above), social context no longer significantly moderated alcohol’s effects on positive mood, b=.20, SE=.124, t=1.59, p=.11, and the effect for negative mood was somewhat diminished in magnitude, b=-.15, SE=.054, t=-2.72, p=.007. In contrast, when these analyses were re-run considering only social contexts involving strangers, social context interacted with alcohol episode in predicting both positive mood, b=.42, SE=.174, t=2.43, p=.02, and negative mood, b=-.27, SE=.093, t=-2.95, p=.003.
Drinking Outcomes
In a final analysis, we examined whether drinking alcohol among strangers was associated with increased levels of consumption compared with drinking alcohol among familiar individuals, an analysis for which we had no a-priori predictions. Since many settings do not readily allow for the option of drinking alcohol, here we limited our analyses to alcohol episodes (see above). In these analyses, we examined continuous eBrAC at the time of the mood/photo prompt as a continuous outcome. The number of strangers present in social contexts predicted participants’ eBrAC during alcohol episodes, with eBrAC increasing by approximately .01% with the introduction of each stranger into the drinking context, b=0.01, SE=.003, t=3.25, p=.002.8 Similarly, the average number of hours spent with those in social drinking contexts also predicted eBrAC, b=-0.04, SE=.016, t=-2.60, p=.01, with eBrAC decreasing by approximately .04% with each standard deviation increase in average amount of time spent with those in the social context. These relationships remained significant even after controlling for a range of contextual and individual-difference factors, including the physical context of drinking and typical patterns of consumption. The total number of individuals present in social context—minus the total number of strangers—did not significantly predict eBrAC during drinking episodes, p=.47.
Finally, we examined whether indexes of familiarity predicted the peak eBrAC reached during a given drinking episode. Since participants often visited multiple contexts over the course of a single drinking episode, we examined aggregate indexes of familiarity within these episodes. Overall average levels of familiarity across contexts within a drinking episode only marginally predicted peak eBrAC for that drinking episode, p’s>.064. In contrast, peak eBrAC was significantly predicted by levels of familiarity present within the most unfamiliar context participants had visited over the course of a drinking episode (Number of Strangers: b= .007, SE=.002, t=2.88, p=.006; Time Spent: b= −0.015, SE=.005, t=-3.24, p=.002).
Discussion
So am now cut to one wine glass with the evening meal. Must cut it out entirely it seems but they do not want to treat the nervous system too violently…Anyway, let’s not talk about it. Makes you plenty nervous and very difficult to be with people you don’t know. (Hemingway, 1981)
When writer Ernest Hemingway is required by his doctors to reduce his alcohol consumption at the age of 57, a major concern he notes in facing his future life of sobriety is that of interacting with unfamiliar people. Although authors and casual observers have not infrequently commented on alcohol’s powers to relieve negative emotions in unfamiliar social contexts, scientists have heretofore been silent on this point. In the current study, we conducted the first empirical examination of social familiarity as a moderator of alcohol reward in real-world drinking contexts. Employing novel ambulatory procedures, we examined whether emotional rewards from alcohol are enhanced when alcohol is consumed in relatively unfamiliar vs. familiar social contexts in a sample of heavy social drinkers at risk for AUD.
Results indicated that alcohol consumption was associated with significantly greater negative mood reduction and, in some cases, greater positive mood enhancement in relatively unfamiliar social settings vs. familiar settings. In other words, alcohol appeared to confer more emotional rewards when consumed in the presence of individuals with whom participants were less well acquainted. Analyses also indicated that drinking in relatively unfamiliar (vs. familiar) social contexts was associated with higher levels of consumption within a given drinking episode (see further discussion of this point below). In terms of the implications of this work for understanding AUD, research employing longitudinal designs and clinical samples would be required to support conclusions. Nonetheless, when considered together with prior research pointing to links between alcohol’s socially enhancing effects and the subsequent development of problematic drinking (see Fairbairn et al., in press; Fairbairn & Sayette, 2014), these findings indicate that social familiarity may be a factor in AUD etiology and further offer a new framework for the identification of those vulnerable to developing AUD. The results of this study might also ultimately have implications for those who have already developed AUD, potentially helping refine the understanding of “high risk” settings for relapse (Marlatt, 1996), and further, by identifying specific affective functions of alcohol in these high-risk contexts, helping inform appropriate alternative coping measures.
In addition to its conceptual contributions, the current research may also have methodological implications for the study of alcohol use in everyday life. Transdermal sensors provide novel capabilities for continuous measurement of TAC, but since individual-level variables such as the thickness of the skin can affect TAC, quantitative levels of BAC/BrAC cannot be determined directly from these sensors (Leffingwell et al., 2013; Luczak & Rosen, 2014; Swift & Sweete, 1992). In the current study, we used algorithms that integrate TAC and BrAC data from the laboratory session for the conversion of TAC to eBrAC in the ambulatory assessment phase (Luczak & Rosen, 2014; Luczak et al., 2015). We further combine this eBrAC with image-capture methods for examining contextual elements, using random sampling methods to obtain rich photographic representations of drinking setting (N. A. Brown et al., in press). These methods offer alternatives to self-reports, which rely on cognitive and memory capabilities depleted by alcohol, and provide promising methods to those seeking to understand patterns of alcohol consumption in everyday settings.
One intriguing finding emerging from this study pertains to the relation between the presence of others (i.e., social context), social familiarity, and alcohol reward. As noted previously, prior research has consistently suggested that alcohol’s mood-enhancing effects are significantly larger when alcohol is consumed in the company of others vs. alone. In the present study, we replicated the interaction between social context and alcohol observed in these prior studies, but found that the effects of social context were mainly driven by unfamiliar contexts (contexts involving strangers). These findings indicate the importance of social familiarity in examinations of social influences on alcohol reward. Such analyses seem particularly relevant given that prior laboratory studies examining the effect of social context on alcohol response have only examined social contexts in which the majority of study participants would necessarily have been strangers (del Porto & Masur, 1984; Doty & de Wit, 1995; Kirkpatrick & de Wit, 2013; Pliner & Cappell, 1974).
Another finding of the current study is the association between unfamiliar drinking contexts and increased levels of alcohol consumption. Our analyses suggested that unfamiliar drinking contexts were associated with higher levels of alcohol consumption, with the introduction of each stranger into the drinking context being associated with increases in estimated BAC. This finding is intriguing, and, if replicated, might suggest that social familiarity could have relevance for understanding context-specific patterns of heavy alcohol use. Importantly, however, while increased alcohol consumption may take place within some unfamiliar drinking settings, it is unclear whether such immediate associations will consistently emerge (see Fairbairn, 2017). Unfamiliar settings can increase vigilance and self-presentational concerns, and therefore it’s feasible that, despite increased mood-enhancement from alcohol in such settings, the presence of strangers may sometimes suppress heavier drinking within a given drinking episode. Importantly, we propose social familiarity as a broader, learning-based framework for understanding expectancies for alcohol reward and risk for AUD. We therefore don’t necessarily predict that people will consistently drink alcohol in greater quantities in unfamiliar social contexts. Instead we predict that individuals who repeatedly drink in unfamiliar vs. familiar drinking contexts will, over time, develop more positive conceptualizations surrounding alcohol’s effects, and will be more likely to drink heavily (Fairbairn, 2017). Research assessing context-specific alcohol effects and also employing prospective study designs would be required to establish a role for acute alcohol reward in explaining links between habitual drinking in unfamiliar contexts and risk for AUD.
The current study is also the first to examine alcohol-related mood enhancement both inside and outside the laboratory. Each participant in the current study not only engaged in intensive ambulatory assessment, but also attended both alcohol and no-alcohol sessions in the laboratory. The effect of alcohol on an individual’s negative mood assessed inside the laboratory was significantly related to the effect of alcohol on that individual’s negative mood assessed outside the laboratory, whereas the relationship between laboratory and ambulatory measures of alcohol’s effects did not reach significance for positive mood. Of note, the effect of alcohol in enhancing positive mood and decreasing negative mood emerged as substantially magnified (nearly 3 times larger) within controlled laboratory procedures vs. using ambulatory procedures. These disparities might be attributed to a wide range of factors that differed across ambulatory and laboratory arms of the study. A small sample of these factors include: 1) Participants drank only with unfamiliar individuals in the laboratory, whereas they drank both with familiar and unfamiliar individuals outside the laboratory; 2) Participants’ precise position on the BAC curve could not be held constant across laboratory and ambulatory arms of the study (although see footnote 7), and so differences could be partially attributable to limb effects. Relatedly, the variability in alcohol dose was much larger outside the laboratory; 3) Participants chose when to self-administer alcohol in everyday contexts; and 4) The current study featured a relatively small sample size and a brief period of ambulatory assessment, and future studies would do well to examine the correspondence between laboratory and ambulatory positive and negative mood among larger numbers of individuals and over longer periods of time.
Limitations and Future Directions
As noted previously, we instructed participants to capture as much as possible of their current context in the photographs. It’s worth noting, however, that there were likely times when other individuals were present but were not captured in photographs. Second, consistent with sample sizes employed in studies that have used similarly intensive methods (Fairbairn & Cranford, 2016; Mehl & Conner, 2013), the present study involved a relatively small sample of participants. The time period for ambulatory assessment was also relatively short, although it was sufficiently long to capture multiple drinking episodes for most of our heavy drinking participants. Replication of effects in a larger sample of participants and over longer time periods would be an important next step. Third, methods for estimating BrAC from transdermal devices are still in a relatively early stage of development, and situation-level factors (e.g., physical activity, ambient temperature) may influence TAC above and beyond individual and device level parameters. Further research is needed to better understand the relationship between transdermal data and BAC. Fourth, the items used to assess positive mood in the current study largely represented high-arousal positive mood, and so, to the extent to which low arousal positive mood items capture relief of negative affect, analyses may have been less informative regarding potential negative reinforcement from alcohol in unfamiliar social contexts. Finally, in this first empirical study of the effect of familiarity on alcohol response, we opted to focus on natural drinking behaviors and everyday drinking contexts. Thus, this study is unable to speak to whether effects are causal or correlational in nature. Future research employing randomized designs would be required to inform causal inferences. Such research might further consider employing a placebo manipulation in the laboratory, since the current study leaves unanswered the question of whether effects are driven by pharmacology or expectancy. Such an examination might have clinical implications, since prevention/intervention implications might be different for expectancy (e.g., expectancy challenge) vs. pharmacology (e.g., naltrexone) mechanisms.
In sum, this research represents a step forward in both conceptual and methodological domains. We present a novel combined ambulatory-laboratory platform with potential implications for understanding AUD risk, mobilizing cutting-edge ambulatory technology that allows the researcher to bring some of the precision of the laboratory into the real world. The results of this study also emphasize the importance of context in determining alcohol response, indicating that, beyond the “who” of the drinker, the “where” of the drinking setting may have important implications for determining alcohol’s emotional rewards and thus for understanding problematic drinking. Finally, and importantly, the current study indicates the importance of familiarity as a promising framework for understanding heavy drinking and potentially AUD etiology.
Supplementary Material
General Scientific Summary.
Research has indicated a link between alcohol consumption in unfamiliar social settings and problematic patterns of drinking. This study provided a potential explanation for this link, indicating that people may get more out of drinking in unfamiliar social settings. More specifically, results suggested that alcohol was associated with greater mood enhancement when it was consumed in relatively unfamiliar (e.g., with strangers) vs. familiar (e.g., with close friends) drinking contexts.
Acknowledgments
This research was supported by National Institutes of Health Grant R01AA025969 to Catharine E. Fairbairn. Support for this research was also provided by NIH grant R21 AA17711 to Susan Luczak. Procedures were approved by the University of Illinois at Urbana-Champaign Institutional Review Board (IRB Protocol Number 16263). Thanks to Thomas Kwapil, R. Chris Fraley, John Dimoff, Howard Berenbaum, Steffen Reindl, Nikki Craycraft, Kaleigh Wilkins, and Michael Sayette for their assistance with the procedures used in this research. Thanks also to the many outstanding undergraduate students of the Alcohol Research Laboratory.
Footnotes
One investigation measured the effects of both alcohol and familiarity within a sample of 16 individuals using a between-subjects experimental design (Lindfors & Lindman, 1987). However, the researchers only report main effects of these two factors, and not their interaction.
Consistent with our prior work (Sayette et al., 2012), the laboratory portion of the study includes only groups of unfamiliar individuals, a configuration chosen to reflect a reasonably common, real-world drinking setting (Fairbairn & Sayette, 2014). The laboratory sessions were required for the calibration of transdermal sensors, and to provide data towards our secondary aim of examining the correspondence between alcohol reward experienced in laboratory vs. real-world drinking contexts. An examination of the effects of familiarity on alcohol reward inside the laboratory was beyond the scope of this work (see also discussion section).
The first 12 participants in the study wore the Electronically Activated Recorder (EAR). No ambulatory mood or contextual familiarity data was collected for these individuals.
We note that the alpha is low for both of our negative mood measures. As noted by Schmitt (1996), this should only influence the interpretation of nonsignificant results because lower alphas make it more difficult to detect significant effects (Schmitt, 1996). Thus, any significant effects should still be significant at higher reliabilities, whereas some nonsignificant results may be significant with more reliable scales.
The variable Years Known was not significantly related to either positive mood or negative mood, p’s>.14. Further, there was only a moderate association between Time Spent and Years Known—it appeared that, in some cases, individuals had been acquainted for some time, but spent little time in one-another’s company or, conversely, have only met several months previously, but been almost continuously together. We therefore focused on Time Spent and Number of Strangers, and not Years Known, as our primary measures of familiarity.
Given the fixed laboratory dose would have led to relatively low BAC variability inside vs. outside the laboratory, we re-ran our models restricting ambulatory observations to those between .04%-.12% eBrAC. Effects were largely similar to results in the non-restricted sample [Negative mood: β=.26, t=1.84, p=.072; Positive mood=NS]. Further, since laboratory BAC was estimated on the ascending limb of the BAC curve, we performed these comparisons limiting ambulatory data to only those observations taken while participants’ BAC’s were ascending, and these comparisons were again largely consistent with those above [Negative mood: β=.28, t=1.99, p=.052; Positive mood=NS].
We also examined the total number of each category of non-strangers—acquaintances, family members, romantic partners, coworkers, friends, and close friends—present in social context as a moderator of alcohol response. Results indicated that the two most prevalent of these categories—friends and close friends—each significantly interacted with alcohol episode. The number of friends interacted with alcohol in predicting negative mood, b=0.03, SE=.015, t=2.07, p=.04, and the number of close friends interacted with alcohol in predicting both positive mood, b=-0.24, SE=.083, t=-2.86, p=.004, and negative mood, b=0.09, SE=.035, t=2.67, p=.008. Importantly, these analyses indicated that alcohol’s tendency to enhance positive mood and relieve negative mood emerged as weaker in the presence of greater numbers of friends and close friends. No other relationship category of familiar individual significantly interacted with alcohol, p’s>.16, possibly because of the relative scarcity of such individuals in our data (see descriptive statistics above).
Importantly, note that interactions between familiarity and alcohol episode in predicting mood (primary finding described above) were not accounted for by higher eBrAC levels during alcohol episodes that took place within unfamiliar social settings. Within drinking episodes, the relationship between both positive and negative mood and social familiarity remained unchanged after the introduction of precise eBrAC level as a covariate.
Contributor Information
Catharine E. Fairbairn, University of Illinois at Urbana-Champaign
Konrad Bresin, University of Illinois at Urbana-Champaign.
Dahyeon Kang, University of Illinois at Urbana-Champaign.
I. Gary Rosen, University of Southern California.
Talia Ariss, University of Illinois at Urbana-Champaign.
Susan E. Luczak, University of Southern California
Nancy P. Barnett, University of Illinois at Urbana-Champaign
Brown University, University of Illinois at Urbana-Champaign.
Nathaniel S. Eckland, University of Illinois at Urbana-Champaign
Catharine E. Fairbairn, Department of Psychology, University of Illinois—Urbana-Champaign
Konrad Bresin, Department of Psychology, University of Illinois—Urbana-Champaign
Dahyeon Kang, Department of Psychology, University of Illinois—Urbana-Champaign.
Talia Ariss, Department of Psychology, University of Illinois—Urbana-Champaign
Nathaniel S. Eckland, Department of Psychology, University of Illinois—Urbana-Champaign
I. Gary Rosen, Department of Mathematics, University of Southern California
Nancy P. Barnett, Center for Alcohol and Addiction Studies and Department of Behavioral and Social Sciences, Brown University
Susan E. Luczak. Ph.D., Department of Psychology, University of Southern California
References
- Ahlström-Laakso S. European drinking habits: A review of research and some suggestions for conceptual integration of findings. In: Everett MW, Wadell JO, Heath DB, editors. Cross-cultural approaches to the study of alcohol An interdisciplinary perspective. The Hague/Paris: Mouton; 1976. pp. 119–132. [Google Scholar]
- Armeli S, Tennen H, Todd M, Carney MA, Mohr C, Affleck G, Hromi A. A daily process examination of the stress-response dampening effects of alcohol consumption. Psychology of Addictive Behaviors. 2003;17:266–276. doi: 10.1037/0893-164X.17.4.266. https://doi.org/10.1037/0893-164X.17.4.266. [DOI] [PubMed] [Google Scholar]
- Barnett NP, Meade EB, Glynn TR. Predictors of detection of alcohol use episodes using a transdermal alcohol sensor. Experimental and Clinical Psychopharmacology. 2014;22(1):86–96. doi: 10.1037/a0034821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barnett NP, Tidey J, Murphy JG, Swift R, Colby SM. Contingency management for alcohol use reduction: A pilot study using a transdermal alcohol sensor. Drug and Alcohol Dependence. 2011;118(2):391–399. doi: 10.1016/j.drugalcdep.2011.04.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barta WD, Tennen H, Litt MD. Measurement reactivity in diary research. In: Mehl MR, Conner TS, editors. Handbook of research methods for studying daily life. New York, NY: Guilford Press; 2012. pp. 108–123. [Google Scholar]
- Baumeister RF, Leary MR. The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychological Bulletin. 1995;117(3):497–529. https://doi.org/10.1037/0033-2909.117.3.497. [PubMed] [Google Scholar]
- Berger CR, Calabrese RJ. Some explorations in initial interaction and beyond: Toward a developmental theory of interpersonal communication. Human Communication Research. 2006;1(2):99–112. https://doi.org/10.1111/j.1468-2958.1975.tb00258.x. [Google Scholar]
- Blane HT, Leonard KE. Psychological Theories of Drinking and Alcoholism. Second. 2nd. New York: Guilford Press; 1999. [Google Scholar]
- Bouchery EE, Harwood HJ, Sacks JJ, Simon CJ, Brewer RD. Economic costs of excessive alcohol consumption in the US, 2006. American Journal of Preventive Medicine. 2011;41(5):516–524. doi: 10.1016/j.amepre.2011.06.045. [DOI] [PubMed] [Google Scholar]
- Bourgault C, Demers A. Solitary drinking: A risk factor for alcohol-related problems? Addiction. 1997;92(3):303–312. https://doi.org/10.1111/j.1360-0443.1997.tb03200.x. [PubMed] [Google Scholar]
- Bowlby J. Attachment and Loss: Attachment. New York, NY: Basic Books; 1969. [Google Scholar]
- Brown NA, Blake AB, Sherman RA. A snapshot of the life as lived: Wearable cameras in social and personality psychological science. Social Psychology and Personality Science (in press) [Google Scholar]
- Brown SA. Expectancies versus background in the prediction of college drinking patterns. Journal of Consulting and Clinical Psychology. 1985;53(1):123–130. doi: 10.1037//0022-006x.53.1.123. https://doi.org/10.1037/0022-006X.53.1.123. [DOI] [PubMed] [Google Scholar]
- Casswell S, Zhang JF. Access to alcohol from licensed premises during adolescence: A longitudinal study. Addiction. 1997;92(6):737–745. https://doi.org/10.1111/j.1360-0443.1997.tb02940.x. [PubMed] [Google Scholar]
- Conklin CA. Environments as cues to smoke: Implications for human extinction-based research and treatment. Experimental and Clinical Psychopharmacology. 2006;14(1):12–19. doi: 10.1037/1064-1297.14.1.12. [DOI] [PubMed] [Google Scholar]
- Cooper ML, Frone MR, Russell M, Mudar P. Drinking to regulate positive and negative emotions: A motivational model of alcohol use. Journal of Personality and Social Psychology. 1995;69:990–1005. doi: 10.1037//0022-3514.69.5.990. https://doi.org/10.1037/0022-3514.69.5.990. [DOI] [PubMed] [Google Scholar]
- Corbin WR, Scott C, Boyd SJ, Menary KR, Enders CK. Contextual influences on subjective and behavioral responses to alcohol. Experimental and Clinical Psychopharmacology. 2015;23(1):59–70. doi: 10.1037/a0038760. https://doi.org/10.1037/a0038760. [DOI] [PubMed] [Google Scholar]
- Creswell KG, Sayette MA, Manuck SB, Ferrell RE, Hill SY, Dimoff JD. DRD4 polymorphism moderates the effect of alcohol consumption on social bonding. PloS One. 2012;7:e28914. doi: 10.1371/journal.pone.0028914. https://doi.org/10.1371/journal.pone.0028914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Curtin JJ, Lang AR, Patrick CJ, Stritzke WGK. Alcohol and fear-potentiated startle: The role of competing cognitive demands in the stress-reducing effects of intoxication. Journal of Abnormal Psychology. 1998;107(4):547–557. doi: 10.1037//0021-843x.107.4.547. https://doi.org/10.1037/0021-843X.107.4.547. [DOI] [PubMed] [Google Scholar]
- del Porto JA, Masur J. The effects of alcohol, THC and diazepam in two different social settings: A study with human volunteers. Research Communications in Psychology, Psychiatry & Behavior. 1984;9(2):201–212. [Google Scholar]
- Doty P, de Wit H. Effect of setting on the reinforcing and subjective effects of ethanol in social drinkers. Psychopharmacology. 1995;118(1):19–27. doi: 10.1007/BF02245245. https://doi.org/10.1007/BF02245245. [DOI] [PubMed] [Google Scholar]
- Dumett MA, Rosen IG, Sabat J, Shaman A, Tempelman L, Wang C, Swift RM. Deconvolving an estimate of breath measured blood alcohol concentration from biosensor collected transdermal ethanol data. Applied Mathematics and Computation. 2008;196(2):724–743. doi: 10.1016/j.amc.2007.07.026. https://doi.org/10.1016/j.amc.2007.07.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fairbairn CE. Drinking among strangers: A meta-analysis examining familiarity as a moderator of alcohol’s rewarding effects. Psychology of Addictive Behaviors. 2017;31(3):255–264. doi: 10.1037/adb0000264. https://doi.org/10.1037/adb0000264. [DOI] [PubMed] [Google Scholar]
- Fairbairn CE, Bresin KW. The effects of contextual familiarity on alcohol expectancies. Experimental and Clinical Psychopharmacology. 2017;25(1):13–23. doi: 10.1037/pha0000103. https://doi.org/10.1037/pha0000103. [DOI] [PubMed] [Google Scholar]
- Fairbairn CE, Briley DA, Kang D, Fraley RC, Hankin BL, Ariss T. A meta-analysis of attachment security and substance use. Psychological Bulletin. doi: 10.1037/bul0000141. (in press) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fairbairn CE, Cranford JA. A multimethod examination of negative behaviors during couples interactions and problem drinking trajectories. Journal of Abnormal Psychology. 2016;125(6):805–810. doi: 10.1037/abn0000186. https://doi.org/10.1037/abn0000186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fairbairn CE, Sayette MA. The effect of alcohol on emotional inertia: A test of alcohol myopia. Journal of Abnormal Psychology. 2013;122(3):770–781. doi: 10.1037/a0032980. https://doi.org/10.1037/a0032980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fairbairn CE, Sayette MA. A social-attributional analysis of alcohol response. Psychological Bulletin. 2014;140(5):1361–1382. doi: 10.1037/a0037563. https://doi.org/10.1037/a0037563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fairbairn CE, Sayette MA, Aalen OO, Frigessi A. Alcohol and emotional contagion: An examination of the spreading of smiles in male and female drinking groups. Clinical Psychological Science. 2015;3(5):686–701. doi: 10.1177/2167702614548892. https://doi.org/10.1177/2167702614548892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fairbairn CE, Sayette MA, Amole MC, Dimoff JD, Cohn JF, Girard JM. Speech volume indexes sex differences in the social-emotional effects of alcohol. Experimental and Clinical Psychopharmacology. 2015;23(4):255–264. doi: 10.1037/pha0000021. https://doi.org/10.1037/pha0000021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fairbairn CE, Sayette MA, Wright AGC, Levine JM, Cohn JF, Creswell KG. Extraversion and the rewarding effects of alcohol in a social context. Journal of Abnormal Psychology. 2015;124(3):660–673. doi: 10.1037/abn0000024. https://doi.org/10.1037/abn0000024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finn PR, Pihl RO. Men at high risk for alcoholism: The effect of alcohol on cardiovascular response to unavoidable shock. Journal of Abnormal Psychology. 1987;96:230–236. doi: 10.1037//0021-843x.96.3.230. https://doi.org/10.1037/0021-843X.96.3.230. [DOI] [PubMed] [Google Scholar]
- Fromme K, Dunn ME. Alcohol expectancies, social and environmental cues as determinants of drinking and perceived reinforcement. Addictive Behaviors. 1992;17:167–177. doi: 10.1016/0306-4603(92)90021-m. https://doi.org/10.1016/0306-4603(92)90021-M. [DOI] [PubMed] [Google Scholar]
- Heath DB. International handbook on alcohol and culture. Westford, CT: Greenwood; 1995. [Google Scholar]
- Heath DB. Drinking occasions: Comparative perspectives on alcohol & culture. Philadelphia: Routledge; 2000. [Google Scholar]
- Hefner KR, Curtin JJ. Alcohol stress response dampening: Selective reduction of anxiety in the face of uncertain threat. Journal of Psychopharmacology. 2012;26(2):232–244. doi: 10.1177/0269881111416691. https://doi.org/10.1177/0269881111416691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hemingway E. Ernest Hemingway Selected Letters 1917–1961. New York, NY: Scribner Classics; 1981. [Google Scholar]
- Hingson RW, Zha W, White AM. Drinking beyond the binge threshold: Predictors, consequences, and changes in the US. American Journal of Preventive Medicine. 2017;52(6):717–727. doi: 10.1016/j.amepre.2017.02.014. [DOI] [PubMed] [Google Scholar]
- Hull JG. A self-awareness model of the causes and effects of alcohol consumption. Journal of Abnormal Psychology. 1981;90(6):586–600. doi: 10.1037//0021-843x.90.6.586. https://doi.org/10.1037/0021-843X.90.6.586. [DOI] [PubMed] [Google Scholar]
- Hull JG. Self-awareness model. In: Blane HT, Leonard KE, editors. Psychological theories of drinking and alcoholism. New York, NY: Guilford Press; 1987. pp. 272–304. [Google Scholar]
- Jones BT, Corbin W, Fromme K. A review of expectancy theory and alcohol consumption. Addiction. 2002;96(1):57–72. doi: 10.1046/j.1360-0443.2001.961575.x. https://doi.org/10.1046/j.1360-0443.2001.961575.x. [DOI] [PubMed] [Google Scholar]
- Josephs RA, Steele CM. The two faces of alcohol myopia: Attentional mediation of psychological stress. Journal of Abnormal Psychology. 1990;99(2):115–126. doi: 10.1037//0021-843x.99.2.115. https://doi.org/10.1037/0021-843X.99.2.115. [DOI] [PubMed] [Google Scholar]
- Keltner D, Gross JJ. Functional accounts of emotions. Cognition & Emotion. 1999;13(5):467–480. [Google Scholar]
- King AC, de Wit H, McNamara PJ, Cao D. Rewarding, stimulant, and sedative alcohol responses and relationship to future binge drinking. Archives of General Psychiatry. 2011;68(4):389–399. doi: 10.1001/archgenpsychiatry.2011.26. https://doi.org/10.1001/archgenpsychiatry.2011.26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- King AC, McNamara PJ, Hasin DS, Cao D. Alcohol challenge responses predict future alcohol use disorder symptoms: A 6-year prospective study. Biological Psychiatry. 2014;75(10):798–806. doi: 10.1016/j.biopsych.2013.08.001. https://doi.org/10.1016/j.biopsych.2013.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirkpatrick MG, de Wit H. In the company of others: Social factors alter acute alcohol effects. Psychopharmacology. 2013;230(2):215–226. doi: 10.1007/s00213-013-3147-0. https://doi.org/10.1007/s00213-013-3147-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koob GF, Le Moal M. Drug abuse: Hedonic homeostatic dysregulation. Science. 1997;278(5335):52–58. doi: 10.1126/science.278.5335.52. [DOI] [PubMed] [Google Scholar]
- Leary MR, Kowalski RM. Social Anxiety. New York: Guilford Press; 1995. [Google Scholar]
- Leffingwell TR, Cooney NJ, Murphy JG, Luczak S, Rosen G, Dougherty DM, Barnett NP. Continuous objective monitoring of alcohol use: Twenty-first century measurement using transdermal sensors. Alcoholism: Clinical and Experimental Research. 2013;37(1):16–22. doi: 10.1111/j.1530-0277.2012.01869.x. https://doi.org/10.1111/j.1530-0277.2012.01869.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levenson RW, Sher KJ, Grossman LM, Newman J, Newlin DB. Alcohol and stress response dampening: Pharmacological effects, expectancy, and tension reduction. Journal of Abnormal Psychology. 1980;89(4):528–538. doi: 10.1037//0021-843x.89.4.528. https://doi.org/10.1037/0021-843X.89.4.528. [DOI] [PubMed] [Google Scholar]
- Lindfors B, Lindman R. Alcohol and previous acquaintance: Mood and social interactions in small groups. Scandinavian Journal of Psychology. 1987;28(3):211–219. doi: 10.1111/j.1467-9450.1987.tb00757.x. https://doi.org/10.1111/j.1467-9450.1987.tb00757.x. [DOI] [PubMed] [Google Scholar]
- Luczak SE, Rosen IG. Estimating BrAC from transdermal alcohol concentration data using the BrAC estimator software program. Alcoholism: Clinical and Experimental Research. 2014;38(8):2243–2252. doi: 10.1111/acer.12478. https://doi.org/10.1111/acer.12478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luczak SE, Rosen IG, Wall TL. Development of a real-time repeated-measures assessment protocol to capture change over the course of a drinking episode. Alcohol and Alcoholism. 2015;50(2):180–187. doi: 10.1093/alcalc/agu100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luczak SE, Rosen IG, Weiss J. American Control Conference (ACC), 2013. IEEE; 2013. Determining blood and/or breath alcohol concentration from transdermal alcohol data; pp. 473–478. [Google Scholar]
- Marlatt GA. Taxonomy of high-risk situations for alcohol relapse: Evolution and development of a cognitive-behavioral model. Addiction. 1996;91(12s1):37–50. https://doi.org/10.1046/j.1360-0443.91.12s1.15.x. [PubMed] [Google Scholar]
- Mehl MR, Conner TS, editors. Handbook of Research Methods for Studying Daily Life. New York: The Guilford Press; 2013. [Google Scholar]
- Miranda R, Monti PM, Ray L, Treloar HR, Reynolds EK, Ramirez J, et al. Characterizing subjective responses to alcohol among adolescent problem drinkers. Journal of Abnormal Psychology. 2014;123(1):117–129. doi: 10.1037/a0035328. https://doi.org/10.1037/a0035328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moberg CA, Curtin JJ. Alcohol selectively reduces anxiety but not fear: Startle response during unpredictable versus predictable threat. Journal of Abnormal Psychology. 2009;118(2):335–347. doi: 10.1037/a0015636. https://doi.org/10.1037/a0015636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NIAAA. National Institute on Alcohol Abuse and Alcoholism Webpage. 2017 Oct 15; Retrieved October 15, 2017, from https://www.niaaa.nih.gov/
- Organization WH. Global status report on alcohol and health 2014. Geneva, Switzerland: World Health Organization; 2014. [Google Scholar]
- Piasecki TM, Wood PK, Shiffman S, Sher KJ, Heath AC. Responses to alcohol and cigarette use during ecologically assessed drinking episodes. Psychopharmacology. 2012;223(3):331–344. doi: 10.1007/s00213-012-2721-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pliner P, Cappell H. Modification of affective consequences of alcohol: A comparison of social and solitary drinking. Journal of Abnormal Psychology. 1974;83(4):418–425. doi: 10.1037/h0036884. https://doi.org/10.1037/h0036884. [DOI] [PubMed] [Google Scholar]
- Pohorecky LA. Biphasic action of ethanol. Biobehavioral Reviews. 1977;1(4):231–240. [Google Scholar]
- Raudenbush SW, Bryk AS. Hierarchical linear models: Applications and data analysis methods. Vol. 2. Thousand Oaks, CA: Sage Publications; 2002. [Google Scholar]
- Reboussin BA, Song E, Wolfson M. Social influences on the clustering of underage risky drinking and its consequences in communities. Journal of Studies on Alcohol and Drugs. 2012;73(6):890–898. doi: 10.15288/jsad.2012.73.890. https://doi.org/10.15288/jsad.2012.73.890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roberts LJ, Leonard KE. An empirical typology of drinking partnerships and their relationship to marital functioning and drinking consequences. Journal of Marriage and the Family. 1998;60(2):515–526. https://doi.org/10.2307/353866. [Google Scholar]
- Robinson MD, Clore GL. Belief and feeling: evidence for an accessibility model of emotional self-report. Psychological Bulletin. 2002;128(6):934–960. doi: 10.1037/0033-2909.128.6.934. [DOI] [PubMed] [Google Scholar]
- Room R, Makela K. Typologies of the cultural position of drinking. Journal of Studies on Alcohol. 2000;61(3):475–475. doi: 10.15288/jsa.2000.61.475. https://doi.org/10.15288/jsa.2000.61.475. [DOI] [PubMed] [Google Scholar]
- Rosen IG, Luczak SE, Hu WW, Hankin M. 2013 Proceedings of the Conference on Control and its Applications. SIAM; 2013. Discrete-time blind deconvolution for distributed parameter systems with dirichlet boundary input and unbounded output with application to a transdermal alcohol biosensor; pp. 160–167. [Google Scholar]
- Rosen IG, Luczak SE, Weiss J. Blind deconvolution for distributed parameter systems with unbounded input and output and determining blood alcohol concentration from transdermal biosensor data. Applied Mathematics and Computation. 2014;231:357–376. doi: 10.1016/j.amc.2013.12.099. https://doi.org/10.1016/j.amc.2013.12.099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Russell JA. Core affect and the psychological construction of emotion. Psychological Review. 2003;110(1):145–172. doi: 10.1037/0033-295x.110.1.145. https://doi.org/10.1037/0033-295X.110.1.145. [DOI] [PubMed] [Google Scholar]
- Sacks JJ, Gonzales KR, Bouchery EE, Tomedi LE, Brewer RD. 2010 national and state costs of excessive alcohol consumption. American Journal of Preventive Medicine. 2015;49(5):e73–e79. doi: 10.1016/j.amepre.2015.05.031. [DOI] [PubMed] [Google Scholar]
- Sayette MA. An appraisal-disruption model of alcohol’s effects on stress responses in social drinkers. Psychological Bulletin. 1993;114(3):459–476. doi: 10.1037/0033-2909.114.3.459. https://doi.org/10.1037/0033-2909.114.3.459. [DOI] [PubMed] [Google Scholar]
- Sayette MA, Creswell KG, Dimoff JD, Fairbairn CE, Cohn JF, Heckman BW, Moreland RL. Alcohol and group formation: A multimodal investigation of the effects of alcohol on emotion and social bonding. Psychological Science. 2012;23(8):869–878. doi: 10.1177/0956797611435134. https://doi.org/10.1177/0956797611435134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sayette MA, Martin CS, Perrott MA, Wertz JM, Hufford MR. A test of the appraisal-disruption model of alcohol and stress. Journal of Studies on Alcohol. 2001;62(2):247–256. doi: 10.15288/jsa.2001.62.247. https://doi.org/10.15288/jsa.2001.62.247. [DOI] [PubMed] [Google Scholar]
- Schmitt N. Uses and abuses of coefficient alpha. Psychological Assessment. 1996;8(4):350–353. [Google Scholar]
- Scribner R, Mason K, Theall K, Simonsen N, Schneider SK, Towvim LG, DeJong W. The contextual role of alcohol outlet density in college drinking. Journal of Studies on Alcohol and Drugs. 2008;69(1):112–120. doi: 10.15288/jsad.2008.69.112. [DOI] [PubMed] [Google Scholar]
- Senchak M, Leonard KE, Greene BW. Alcohol use among college students as a function of their typical social drinking context. Psychology of Addictive Behaviors. 1998;12(1):62–70. https://doi.org/10.1037/0893-164X.12.1.62. [Google Scholar]
- Sher KJ. Subjective effects of alcohol: The influence of setting and individual differences in alcohol expectancies. Journal of Studies on Alcohol. 1985;46(2):137–146. doi: 10.15288/jsa.1985.46.137. https://doi.org/10.15288/jsa.1985.46.137. [DOI] [PubMed] [Google Scholar]
- Sher KJ, Bartholow BD, Peuser K, Erickson DJ, Wood MD. Stress-response-dampening effects of alcohol: Attention as a mediator and moderator. Journal of Abnormal Psychology. 2007;116(2):362–377. doi: 10.1037/0021-843X.116.2.362. https://doi.org/10.1037/0021-843X.116.2.362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sher KJ, Wood MD. Subjective effects of alcohol II: Individual differences. In: Earleywine M, editor. Mind Altering Drugs: Scientific Evidence for Subjective Experience. New York: Oxford; 2005. pp. 86–134. [Google Scholar]
- Sher KJ, Wood MD, Richardson AE, Jackson KM. Subjective effects of alcohol: Effects of the drink and drinking context. In: Earleywine M, editor. Mind Altering Drugs: The Science of Subjective Experience. New York: Oxford University Press; 2005. pp. 86–134. [Google Scholar]
- Shiffman S. Ecological momentary assessment (EMA) in studies of substance use. Psychological Assessment. 2009;21(4):486–497. doi: 10.1037/a0017074. https://doi.org/10.1037/a0017074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S, Stone AA, Hufford MR. Ecological momentary assessment. Annual Review of Clinical Psychology. 2008;4:1–32. doi: 10.1146/annurev.clinpsy.3.022806.091415. https://doi.org/10.1146/annurev.clinpsy.3.022806.091415. [DOI] [PubMed] [Google Scholar]
- Single E, Wortley S. Drinking in various settings as it relates to demographic variables and level of consumption: Findings from a national survey in Canada. Journal of Studies on Alcohol and Drugs. 1993;54(5):590–599. doi: 10.15288/jsa.1993.54.590. https://doi.org/10.15288/jsa.1993.54.590. [DOI] [PubMed] [Google Scholar]
- Starzyk KB, Holden RR, Fabrigar LR, MacDonald TK. The personal acquaintance measure: A tool for appraising one’s acquaintance with any person. Journal of Personality and Social Psychology. 2006;90(5):833–847. doi: 10.1037/0022-3514.90.5.833. https://doi.org/10.1037/0022-3514.90.5.833. [DOI] [PubMed] [Google Scholar]
- Steele CM, Josephs RA. Alcohol myopia: Its prized and dangerous effects. American Psychologist. 1990;45(8):921–933. doi: 10.1037//0003-066x.45.8.921. https://doi.org/10.1037/0003-066X.45.8.921. [DOI] [PubMed] [Google Scholar]
- Stritzke WG, Lang AR, Patrick CJ. Beyond stress and arousal: A reconceptualization of alcohol–emotion relations with reference to psychophysiological methods. Psychological Bulletin. 1996;120(3):376–395. doi: 10.1037/0033-2909.120.3.376. https://doi.org/10.1037/0033-2909.120.3.376. [DOI] [PubMed] [Google Scholar]
- Swift RM, Swette L. Assessment of ethanol consumption with a wearable, electronic ethanol sensor/recorder. In: Litten RZ, Allen JP, editors. Measuring alcohol consumption: Psychosocial and biochemical methods. Totowa, NJ: Humana Press; 1992. pp. 189–202. Retrieved from http://link.springer.com/chapter/10.1007/978-1-4612-0357-5_10. [Google Scholar]
- Testa M, Fillmore MT, Norris J, Abbey A, Curtin JJ, Leonard KE, George WH. Understanding alcohol expectancy effects: Revisiting the placebo condition. Alcoholism: Clinical and Experimental Research. 2006;30(2):339–348. doi: 10.1111/j.1530-0277.2006.00039.x. https://doi.org/10.1111/j.1530-0277.2006.00039.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trafford E. MetricWire (Version 2.2.10)[Mobile application software] 2016 [Google Scholar]
- Trull TJ, Ebner-Priemer U. Ambulatory assessment. Annual Review of Clinical Psychology. 2013;9:151. doi: 10.1146/annurev-clinpsy-050212-185510. https://doi.org/10.1146/annurev-clinpsy-050212-185510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wechsler H, Lee JE, Kuo M, Lee H. College binge drinking in the 1990s: A continuing problem results of the Harvard School of Public Health 1999 College Alcohol Study. Journal of American College Health. 2000;48(5):199–210. doi: 10.1080/07448480009599305. [DOI] [PubMed] [Google Scholar]
- Wilhelm FH, Grossman P. Emotions beyond the laboratory: Theoretical fundaments, study design, and analytic strategies for advanced ambulatory assessment. Biological Psychology. 2010;84(3):552–569. doi: 10.1016/j.biopsycho.2010.01.017. https://doi.org/10.1016/j.biopsycho.2010.01.017. [DOI] [PubMed] [Google Scholar]
- Wilson GT, Abrams D. Effects of alcohol on social anxiety and physiological arousal: Cognitive versus pharmacological processes. Cognitive Therapy and Research. 1977;1(3):195–210. https://doi.org/10.1007/BF01186793. [Google Scholar]
- Yik M, Russell JA, Steiger JH. A 12-point circumplex structure of core affect. Emotion. 2011;11(4):705–731. doi: 10.1037/a0023980. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.