

Abstract
Background:
Numerous empirical evidences have shown that social and environmental circumstances and social relations have an important impact on pregnancy outcomes, women's ability to cope with stressful situations, and childbirth pain management. The present study was conducted to determine the relationship between perceived social support and fear of childbirth.
Materials and Methods:
The present descriptive correlational study was conducted on 270 nulliparous pregnant women who referred for pregnancy care in 2016. The subjects were selected through convenience sampling method. The data collection tools were a demographic characteristics form, the Multidimensional Scale of Perceived Social Support (MSPSS), and the Wijma Delivery Expectancy/Experience Questionnaire (W-DEQ). The collected data were analyzed using descriptive and inferential statistics tests.
Results:
The mean perceived social support score of the participants was 77.90 and a significant correlation was observed between the perceived social support score and fear of childbirth score (β = −0.18, p = 0.004). The participants' mean score of fear of childbirth was 36.8. The results of study after the evaluation of the effect of predictive variables on the fear of childbirth are as follows: pregnancy preparation classes: (β = 3.50, p = 0.220); observation of natural childbirth videos: (β = 5.26, p = 0.040); and use of educational software: (β =5.82, p = 0.080).
Conclusions:
In order to reduce the fear of childbirth, women's social support structure during pregnancy should be assessed. Moreover, demographic characteristics form the structure and determine the extent of individuals' social network and, through the evaluation of these characteristics during pregnancy, the rate of effective support can be predicted in individuals.
Keywords: Childbirth, fear, Iran, pregnancy, social support
Introduction
Childbirth is a social occurrence all around the world and can be considered as the happiest occurrence in any parent's life. Becoming a parent is accompanied by obtaining a high social status, and the majority of parents describe it as a positive experience. However, pregnancy in itself is a traumatic occurrence and the mother who encounters can potentially be stressful.[1] The birth of the first child, in particular, is categorized as an extremely stressful event in psychosocial stress tables.[2] Concern about the adverse physical–psychological effects of pregnancy and fear of childbirth can be noted as two of the stressors of this period. It has been estimated that 1 out of 5 pregnant women have fear of childbirth. Moreover, approximately 6–13% of pregnant women experience severe and debilitating fear, which, in addition to physical outcomes, can result in psychological complications such as depression and anxiety, negative mood after childbirth, eating disorders,[3] and even uninformed selection of delivery method. It has been proven that fear of childbirth has an important role in the selection of cesarean section by Iranian women.[4] Based on the statistics reported by the World Health Organization (WHO), the prevalence of cesarean section was 46% in Iran in 2014; however, the recommendation of the WHO for an acceptable prevalence of cesarean section by 2014 was a maximum of 5–15%.[5]
Fear of childbirth is an important issue during pregnancy and during and after childbirth, and psychological and social factors have an effective role in its creation.[6] The results of the study by Fisher et al.[7] illustrated that fear of childbirth has two dimensions: individual and social dimension. The social dimension has received less attention in most studies,[6] although it has been found that the social dimension not only affects women's identity but also their perception of childbirth as an abstract event. Social relations, the unofficial support networks of pregnant women, and strong support by midwives can strengthen women's perception of childbirth as a physiological and controllable process.[7] On the contrary, researches have shown that Iranian women's perception of childbirth is derived from their culture and values and is rooted in the environment in which they live.[8] It must be noted that social support has two main dimensions: received and perceived social support. Received social support is the rate of support received by the individual. Perceived social support is the individual's evaluation of the availability of support when necessary and required and is a qualitative-mental and measurable concept.[9] It is affected by culture, evolution, personality, and support systems.[7] Theoreticians believe relationships are not a source of social support unless the individual perceives them as a suitable and available source for fulfilling their needs.[10]
Social support is an interpersonal relationship which provides individuals with psychological help when required. Those who provide this help include family members, neighbors, colleagues, relatives, and the treatment team, who provide mothers with psychological support and information.[1] Relatives, especially the spouse, illustrate their high regard for the pregnant woman through their support for her and this gives her hope. Previous studies have shown that social support has a significant relationship with reduction of stress during pregnancy,[11] and the lack of support has a relationship with unwillingness to breastfeed,[12] low IQ in infants,[13] postpartum depression (PPD),[14] depression during pregnancy,[15] and cleft palate incidence.[16] Some researchers have reported contradictory results regarding this issue. Some studies have shown that sometimes the support provided is inappropriate, untimely, and contrary to the mother's wishes.[17] Other studies have illustrated that this support was ineffective. Jirka et al. found no difference in the rate of social support of pregnant and nonpregnant couples; they received the same rate of support.[18]
Due to the importance of the role of perceived social support in individuals' psychological wellbeing, the contradictory results of previous studies, the role of cultural difference in social support patterns,[19] and the important role of fear of childbirth in the selection of cesarean section by Iranian women,[4] the present study was undertaken. The present study was conducted to determine the possible challenges regarding mothers' social support and the role of predictive variables on fear of childbirth. It is hoped that with the presentation of the results to prenatal caregivers plans can be made for the improvement of mothers' social support, and thus, a small step can be taken toward the improvement of mothers' health and their empowerment.
Materials and Methods
The present descriptive correlational study was conducted on 270 nulliparous pregnant women who referred to health and treatment centers in Isfahan, Iran, for pregnancy care in 2016. The division of perceived social support in the population into two groups of adequate social support and lack of adequate social support required at least 135 subjects from each population and a total of 270 individuals to observe, with a 90% probability, a significant difference of 0.4 in mean score of fear of childbirth between the two populations at 5% significance level. The study environment consisted of the health and treatment centers of Isfahan. The centers were selected through cluster-nonrandom and quota sampling methods after obtaining the approval of the Ethics Committee of Isfahan University of Medical Sciences, Isfahan. These centers were selected due to the possibility of easy access to study subjects. The inclusion criteria consisted of nulliparous pregnancy, Persian nationality, gestational age of 35 weeks and higher, lack of recognized psychological disorders, such as depression and mood disorder (these data were retrieved from the mothers' pregnancy care file), and low-risk pregnancy such as lack of chronic diseases like heart disease, hypertension, and diabetes. In addition, the subjects were questioned regarding participation in childbirth preparation classes, use of computer training programs, and observation of natural childbirth videos; these variables are effective on the mean score of fear of childbirth and their impact was studied in regression analysis.
Data were collected through self-report method and if necessary through interviews using three questionnaires. The data collection tools were a demographic characteristics form, the Multidimensional Scale of Perceived Social Support (MSPSS),[20] and the Wijma Delivery Expectancy/Experience Questionnaire (W-DEQ).[21] The demographic characteristics form assessed the age and occupation of the mother and her spouse, education level, and economic status. The MSPSS is a 12-item tool that evaluates perceived social support in the three dimensions of family (questions 3, 4, 8, 11), friends (questions 6, 7, 9, 12), and specific individual (questions 1, 2, 5, 10). This tool is scored based on seven-point Likert scale (completely agree = 7; agree = 6; somewhat agree = 5; I have no opinion = 4; somewhat disagree = 3; disagree = 2; completely disagree = 1). The minimum and maximum obtained scores of the MSPSS are, respectively, 12 and 84, and higher scores represent higher social support.[20] The W-DEQ consists of 16 items scored based on a four-point Likert scale (lack of fear = 1; low = 2; average = 3; high = 4). Its total score ranges from 16 to 64 and higher scores represent greater fear.[21]
The validity and reliability of the MSPSS were reported for the first time by Zimet et al.[20] (Cronbach's alpha = 0.88). In the study by Gao [22] performed on 68 nulliparous pregnant women in China, the validity of the MSPSS was approved through content validity and its reliability was obtained through the calculation of Cronbach's alpha (α = 0.85). The validity and reliability of the MSPSS have also been approved in Iran.[8] The validity and reliability of the W-DEQ were obtained for the first time by Wijma et al.[21] (Cronbach's alpha = 0.89). In the study by Carlson on 406 nulliparous pregnant women in Sweden, the validity and reliability of the W-DEQ were calculated through content validity and Cronbach's alpha (α = 0.92), respectively.[23] The validity and reliability of this questionnaire have also been approved in Iran.[24]
After obtaining permission and an introduction letter, the researcher referred to the intended treatment centers, presented the introduction letter to the authorities of the centers, and explained the goals of the study to the personnel of the centers. The researcher referred to the health and treatment centers every day during working hours [8,9,10,11,12,13] and selected women who referred for regular pregnancy care and had the inclusion criteria through simple sampling method. The questionnaires were distributed among the subjects and their completion method was explained to them. Before the completion of the questionnaire, a suitable environment was prepared for the participants. The questionnaires were completed in one stage and through self-report method and, if necessary, through interviews. After collecting the completed questionnaires, the subjects were thanked and catered for. The collected data were analyzed using descriptive (mean, median, prevalence distribution, and percentage) and analytical statistics (Pearson coefficient, and regression) at 95% confidence interval in Statistical Package for the Social Sciences (SPSS) software (version 16, SPSS Inc., Chicago, IL, USA).
Ethical considerations
Ethical principles were respected in all stages of the study. The objectives of the study were fully explained to the participants. Mothers who were willing to participate in the study were entered into the study after obtaining informed written consents from them. The subjects were completely free to leave the study at any moment of its execution. Moreover, they were assured of the confidentiality of their information.
Results
In the present study, the mean age of the women was 26 years. The mean age of their spouses was 30 years. The education level of most of the participants was higher than diploma (41.30%) and university degree (41.35%). The majority of women were homemakers (85.92%) and most of their spouses were employed (87.71%). In addition, most of the subjects had an average economic status (93%). Their mean MSPSS score was 77.90%; the scores of support by family, friends, and spouse were 28.11, 22.42, and 27.73, respectively. The mean W-DEQ score of the subjects was 36.81%.
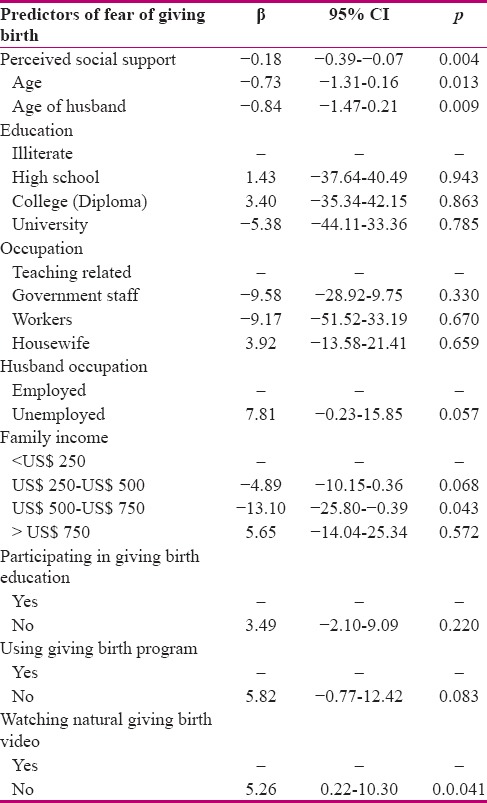
The results of single-variable linear regression analysis showed that perceived social support, age, and spouse's age were predictors of fear of childbirth; 1 point increase in the perceived social support score, 1 year increase in the mother's age, and 1 year increase in the spouse's age resulted in the significant reduction of the mean score of fear of childbirth by, respectively, 0.23, 0.73, and 0.84 points. Education, mother's occupation, spouse's employment, lack of participation in pregnancy preparation classes, and lack of use of pregnancy education software did not cause a significant difference in the fear of childbirth. Nevertheless, household income significantly reduced the fear of childbirth, but observation of natural childbirth videos significantly increased the fear of childbirth [Table 1].
Table 1.
Predictors of fear of giving birth: Results of univariate linear regression
Discussion
The rate of social support in the present study was 77.90%, which was in agreement with the results of the studies by Sadeghe,[8] Jamshidimanesh,[25] and Gao.[22] In the study by Sadeghe, the mean perceived social support score was 62.71 and the scores of support by family, friends, and spouse were 22.53, 16.56, and 23.61, respectively.[8] In the study by Gao,[22] the mean perceived social support score was 68%. The similarity of the findings in the study by Gao to the present study may be due to the fact that China is also an eastern country with a traditional culture in which the family is the main unit of society. In eastern societies, women have an important and high status in the family and the majority of families with different cultures and statuses provide pregnant women with suitable support. In the present study, family support was the most important source of social support and being in the family environment was an unconditional membership in a support group.[25] Moreover, the support of the spouse is an important source which creates a sense of respect, self-esteem, and safety during pregnancy.[8]
The mean score of fear of childbirth in the present study was 36.8%, which was in agreement with the results of the studies by Khorsande [3] and Nasiri.[26] In the study by Khorsande,[3] the mean score of fear of childbirth of nulliparous women was 26%. In the study by Nasiri,[26] the mean score of fear of childbirth was 33.45. From these results it can be inferred that the W-DEQ is a valid tool that is effective in determining women with fear of childbirth and planning to control their fear. If the pregnant mother imagines she cannot control the situation and believes herself to be unable to tolerate the pain, the resulting fear and anxiety will cause her to accept cesarean section without medical indication. In addition, she will not be immune to the negative effects of stress on health.
There was a negative significant relationship between the perceived social support score of and fear of childbirth. In this respect, the study by Fisher et al. showed that social relations, unofficial support networks of pregnant women, and the strong support by midwives can strengthen women's belief that childbirth is a physiological and controllable process, and thus, result in psychological wellbeing and reduced fear of childbirth.[7] Furthermore, Pasha and Faramarze reported that one-third of women experienced pregnancy as a stressful event and the most unpleasant experience of pregnancy was related to the third trimester. They also found that social support had a negative significant relationship with pregnancy stress; with increase in social support score, pregnancy stress decreased (p < 0.05).[11]
Najafe et al.[27] observed a negative significant relationship between pregnancy preparation classes and fear of childbirth (p < 0.001). However, this relationship was not significant in the present study. The difference between Najafi et al. study and the present study may be due to the fact that the study by Najafi et al. was an interventional study or due to the difference in the quality of pregnancy preparation classes. Today, one of the causes of the increase in the prevalence of cesarean section in the world is the fear of childbirth. Furthermore, the statistics of cesarean section in Iran are higher than global standards.[5] Thus, pregnancy preparation classes centered on pregnant women with fear of childbirth can be an effective measure in the reduction of fear of childbirth and the promotion of natural childbirth.
No similar study was found on the relationship between observation of natural childbirth videos and fear of childbirth. However, the results of the present study (conducted for the first time in Iran) can reinforce the belief that common natural childbirth videos have not been prepared with the aim of education and empowerment of women. It can also be stated that these videos can increase tension, and thus, inefficiency and fear. Through the conveyance of this important issue to pregnant mothers by health personnel and informing them, a small step can be taken toward decreasing the fear of childbirth. The results of the study by Hamzekhane [28] suggest that educational software can be more effective in increasing the awareness and knowledge of individuals compared to traditional education methods. Nevertheless, they did not decrease the fear of childbirth in the present study.
The findings of the present research were studied along with its limitations such as cultural factors, beliefs, and traditions which could impact the responses of the subjects and could not be controlled by the researcher.
Conclusion
The results of the present study showed that demographic factors determine the receiving of social support, because these factors form the structure and determine the extent of individuals' social network. It has been proven that lower income, education, economic status, and occupational position are accompanied by a smaller and less diverse social network. Thus, the rate of effective support in pregnant mothers can be predicted through the evaluation of the demographic factors of the support process from the beginning of pregnancy until after childbirth. Furthermore, through informing the treatment team of these results they can be asked to assess clients with characteristics such as low age of mother and spouse, low education, and low income in terms of perceived social support dimensions throughout their pregnancy. The continuous assessment of this support trend from the beginning of pregnancy until after childbirth by the treatment team resulted in the empowerment of women and reduced fear of childbirth which will, in turn, result in increased psychological wellbeing among mothers and reduced prevalence of cesarean section.
Financial support and sponsorship
Isfahan University of Medical Sciences.
Conflicts of interest
Nothing to declare.
Acknowledgement
The article was derived from the Master's thesis with project number 395096, Isfahan University of Medical Sciences, Isfahan, Iran.
References
- 1.Nazare S, Salare P, Mazlom R, Mehram F. The comparative study of social support postpartum mothers multiparity in the first and second month after delivery. Public Health Research Khorasa. 2014;8:1–9. [Google Scholar]
- 2.Pournamdarian S, Birashk B, Asgharnejad Farid A. The clarification of contribution of meta-cognitive beliefs in explaining the symptoms of depression, anxiety and stress in nurses. Knowledge & Research in Applied Psychology. 2012;13:86–94. [Google Scholar]
- 3.Khorsande M, Vakilian K, Masole M. The reasons natural childbirth. J Fasa Univ of Medi Sci. 2014;4:161–6. [Google Scholar]
- 4.Zahede M, Asemane O, Mahmodyan H. Given the role of medical in assistants in reducing caesarean sections; designed and evaluated the psychometric questionnaire to measure attitudes of residents towards elective caesarean sections and vaginal births. Iranian Journal of Medical Ethics and History. 2015;8:59–71. [Google Scholar]
- 5.Word Report on Knowledge for Better Health, Strengthening Health Systems, World Health Organization 2004. [Last accessed on 2009 Aug 29]. Available from: URL: www.who.int/rpc/meeting/publ/en/.
- 6.Taheri Z, Khorsande M, Amire M, Hasanzade A. Investigate the causes of childbirth in pregnant woman in Shahrekord. Univ of Medi Scirafsanjan. 2015;14:345–50. [Google Scholar]
- 7.Fisher C, Hauckb Y, Fenwickb J. How social context impacts on women's fears of childbirth. Soc Sci Med. 2006;63:64–75. doi: 10.1016/j.socscimed.2005.11.065. [DOI] [PubMed] [Google Scholar]
- 8.Sadeghe H, Mosave S, Jahde F, et al. The relationship between perceived social support with the consent of the pregnant women referred to health center martyr Akbarabadi Tehran. Journal of Preventive Care in Nursing and Midwifery. 2013;4:54–64. [Google Scholar]
- 9.Gulacti F. The effect of perceived social support on subjective well-being. Procedia-Social and Behavioral Sciences. 2010;2:3844–9. [Google Scholar]
- 10.Chadwick KA, Collins PA. Examining the relationship between social support availability urban center size, and self-perceived mental health of recent immigrants to Canada: A mixed-methods analysis. Soc Sci Med. 2015;128:220–30. doi: 10.1016/j.socscimed.2015.01.036. [DOI] [PubMed] [Google Scholar]
- 11.Pasha H, Faramarze M. The role of social support in predication of stress in pregnancy. Journal Babol Univ of Medi Sci. 2015;17:52–60. [Google Scholar]
- 12.Hildingsson I, Tingvall M, Rubertsson C. Partner support in the childbearing period — A follow up study. Women Birth. 2008;21:141–8. doi: 10.1016/j.wombi.2008.07.003. [DOI] [PubMed] [Google Scholar]
- 13.Theodore RF, Thompson JM, Waldie KE, Bercroft DM, Robinson E, Wild CJ, et al. Determinants of cognitive ability at 7 years: A longitudinal case control study of children born small-for-gestational age at term. Eur J Pediatr. 2009;168:1217–24. doi: 10.1007/s00431-008-0913-9. [DOI] [PubMed] [Google Scholar]
- 14.Spoozak L, Gotman N, Smith MV, Belanger K, Yonkers KA. Evaluation of a social support measure that may indicate risk of depression during pregnancy. J Affect Disord. 2009;114:216–23. doi: 10.1016/j.jad.2008.07.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nore R, Kareme N, Mohamade M. The relationship Between Prenatal depression with Social Support and satisfaction. Journal Univ Tehran Iran. 2013;1:10–15. [Google Scholar]
- 16.Ma J, Huang YQ, Yao C, Ma SQ, Meng T, Ma M, et al. Parental Health and Social Support in the First Trimester of Pregnancy and the Risk of oral Cleft. Plast Reconstr Surg. 2015;135:212–8. doi: 10.1097/PRS.0000000000000778. [DOI] [PubMed] [Google Scholar]
- 17.Garcia MF, Ramirez M, Jariego MI. Social support and locus of control as predictors of psychological well-being in Moroccan and Peruvian immigrant women in Spain. International Journal of Intercultural Relations. 2002;26:287–310. [Google Scholar]
- 18.Jirka J, Schuett SH, Foxall MJ. Loneliness and Social Support in infertile couples. J Obstet Gynecol Neonatal Nurs. 1996;25:55–60. doi: 10.1111/j.1552-6909.1996.tb02513.x. [DOI] [PubMed] [Google Scholar]
- 19.Logsdon M. Social and professional support for pregnancy and parenting women. MCN Am J Matern Child Nurs. 2003;28:371–6. doi: 10.1097/00005721-200311000-00008. [DOI] [PubMed] [Google Scholar]
- 20.Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. Journal of Personality Assessment. 1998;52:30–41. doi: 10.1080/00223891.1990.9674095. [DOI] [PubMed] [Google Scholar]
- 21.Wijma K, Wijma B, Zar M. A new questionnaire for the measurement of fear of childbirth (Psychometric aspects of the W-DEQ) J Psychosom Obstet Gynecol. 1998;19:84–97. doi: 10.3109/01674829809048501. [DOI] [PubMed] [Google Scholar]
- 22.Gao L, Sun K, Chan SW. Social support and parenting self-efficacy among Chinese women in the perinatal period. Midwifery. 2014;30:532–8. doi: 10.1016/j.midw.2013.06.007. [DOI] [PubMed] [Google Scholar]
- 23.Carlsson M, Ziegert K, Nissen E. The relationship between childbirth self-efficacy and aspects of well-being, birth interventions and birth outcomes. Midwifery. 2015;31:1000–7. doi: 10.1016/j.midw.2015.05.005. [DOI] [PubMed] [Google Scholar]
- 24.Khorsandi M, Ghofranipour F, Heydarnia A, Faghih Zadeh S, Vafaei M, Rousta F, et al. The effect of childbirth preparation classes on childbirth fear and normal delivery among primiparous women. Arak Medical University Journal. 2008;11:9. [Google Scholar]
- 25.Jamshidimanesh M, Astaraki L, Moghadam ZM, Taghizade Z, Haghane H. Maternal-fetal attachment and its associated factor. Hayat. 2012;18:33–45. [Google Scholar]
- 26.Nasiri F, Sharifi SH. The relationship between personality type and childbirth in pregnant women. IJOGI. 2013;16:18–25. [Google Scholar]
- 27.Najafe F, Abozar K, Jafarzade F, Rahnama P, Gholame B. Corporate communications at antenatal classes with fear and type of delivery. Tehran Nursing and Midwifery School (Hayat) 2015;21:30–40. [Google Scholar]
- 28.Hamzekhane M, Hamidzade A, Vasegh F. The effect of computerized educational program on self-efficacy of pregnant women with postpartum adjustment. Journal of Knowledge and Health. 2013;9:13–20. [Google Scholar]