

Abstract
Background
Placing a self-expandable metallic stent (SEMS) is safe and effective for the palliative treatment of malignant gastroduodenal (GD) strictures. SEMS abutment in the duodenal wall is associated with increased food impaction, resulting in higher stent malfunction and shorter stent patency. The desire to evaluate the mechanism and significance of stent abutment led us to design an in vitro experiment using a flexible anthropomorphic three-dimensional (3D)-printed GD phantom model.
Results
A GD phantom was fabricated using 3D printer data after performing computed tomography gastrography. A partially covered (PC) or fully covered (FC) stent was placed so that its distal end abutted onto the duodenal wall in groups PC-1 and FC-1 or its distal end was sufficiently directed caudally in groups PC-2 and FC-2. The elapsed times of the inflowing of three diets (liquid, soft, and solid) were measured in the GD phantom under fluoroscopic guidance. There was no significant difference in the mean elapsed times for the liquid diet among the four groups. For the soft diet, the mean elapsed times in groups PC-1 and FC-1 were longer than those in groups PC-2 and FC-2 (P = 0.018 and P < 0.001, respectively). For the solid diet, the mean elapsed time in group PC-1 was longer than that in group PC-2 (P < 0.001). The solid diet could not pass in group FC-1 due to food impaction. The mean elapsed times were significantly longer in groups FC-1 and FC-2 than in groups PC-1 and PC-2 for soft and solid diets (all P < 0.001).
Conclusions
This flexible anthropomorphic 3D–printed GD phantom study revealed that stent abutment can cause prolonged passage of soft and solid diets through the stent as well as impaction of solid diets into the stent.
Keywords: 3D Printing, Self-expandable metallic stent, Stent abutment, Gastroduodenal phantom
Background
The placement of a partially covered (PC) or fully covered (FC) self-expandable metallic stent (SEMS) is safe, easy, and effective for the palliative treatment of malignant gastroduodenal (GD) strictures [1–7]. Their overall technical and clinical success rates have been reported to be 94 to 100% and 94 to 94.8%, respectively, in studies that have included >74 but <213 patients [3–7]. Recently, our experience with the placement of a SEMS bridging the gastric pylorus for gastric outlet obstruction (GOO) caused by inoperable gastric cancer showed that the distal end of the stent abutted onto the duodenal wall in 107 (33.6%) of 318 patients. Further, stent abutment was associated with increased food impaction, resulting in higher stent malfunction and shorter stent patency [8].
However, the study was a retrospective analysis and was not sufficient to reveal the mechanism of food impaction related with stent abutment. Moreover, only a PC stent was used. The desire to evaluate the mechanism and significance of stent abutment in the duodenal wall led us to design an in vitro experiment using a flexible anthropomorphic three-dimensional (3D)-printed GD phantom model. Recently, 3D printing (3DP) has been commonly used in various fields of medicine, including for personalized treatment, medical research, and premedical education, for soft and hard tissues [9–12]. Therefore, the purpose of this study was to investigate the significance of stent abutment in food passage in comparison with non-stent abutment using an anthropomorphic 3D–printed GD phantom model.
Methods
Design of the 3D–printed GD phantom model
Computed tomography gastrography (CTG) findings of a patient (62-year-old man with advanced gastric cancer involving the gastric pyloric antrum) were retrospectively used to construct an anthropomorphic 3D–printed GD phantom model. The patient had fasted for at least 8 h prior to undergoing CTG. In total, 10 mg of butylscopolamine (Buscopan, Boehringer Ingelheim, Seoul, Korea) was intravenously injected to decrease bowel peristalsis. The patient received 6 g of effervescent granules (Taejeon Pharmaceuticals, Kyungki-Do, Korea) with 10 ml of water to achieve gastric distension prior to CT. Triphasic CT scans (Somatom Sensation 16, Siemens, Erlangen, Germany) were performed during the arterial phase (start of delay, 30 s) with the patient in the left posterior oblique (LPO) position, during the portal phase (72 s) with the patient in the supine position, and during the delayed phase (150 s) with the patient in the prone position after the injection of 120 ml of a nonionic contrast material (Ultravist, Schering, Berlin, Germany) at 4 ml/s via the antecubital vein using an 18-gauge needle and an automatic injector. The LPO position was maintained by placing a pillow below the patient’s back [13].
CT image data were imported to the in-house advanced software (AVIEW, Asan Medical Center, Seoul, Korea) to obtain a 3D visualization model of the entire stomach and duodenum, which was saved in the Stereolithography (STL) file format. Based on the 3D reconstructed models, the length (40 mm) and diameter (18 mm) of the gastric outlet were modified according to stent size using two open source programs (MeshLab and MeshMixer) because the 3D printable material was not flexible enough to stretch from in vivo dimensions. Degree of thickness of the model wall was generated by 2 mm. The modified 3D visualization model was saved in the G-code format and exported to a 3D printer (Objet500 Connex3, Stratasys Corporation, Rehovot, Israel). The 3D–printed GD phantom was made of 100% rubber-like material (Tango™ Family) (Fig. 1).
Fig. 1.
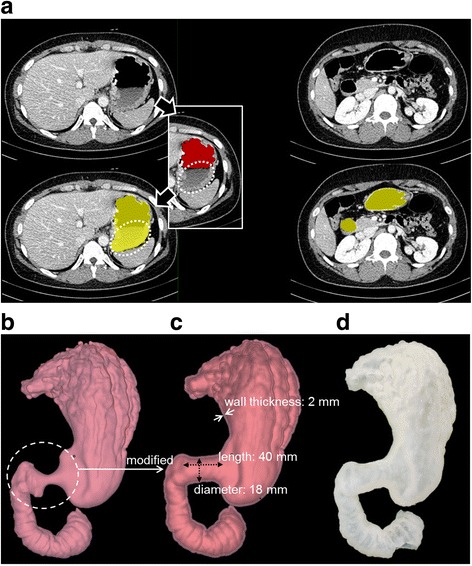
Process for preparing the 3D–printed GD phantom from CTG data. a CT images with segmentation masks. A red mask was made using a simple thresholding setting. Yellow masks were the final segmentation result after multi-step imaging. b Initial 3D GD digital model. c Modified 3D GD digital model for stent placement. d Anthropomorphic 3D–printed GD phantom model
Stents and placement
Two types of SEMS were used: a PC stent (S&G Biotech, Seongnam, Korea) and a FC stent (Taewoong Medical, Gimpo, Korea) (Fig. 2). The PC stent consisted of two stents: an outer, partially covered stent and an inner, bare nitinol stent. The inner and outer stents were 18 mm in diameter, with their ends flared up to 28 mm. Both ends of the FC stent were 24 mm in diameter and 20 mm in length when fully expanded, and its body was 18 mm in diameter. A detailed description of the stent and delivery systems with their placement techniques has been previously reported [3, 4].
Fig. 2.
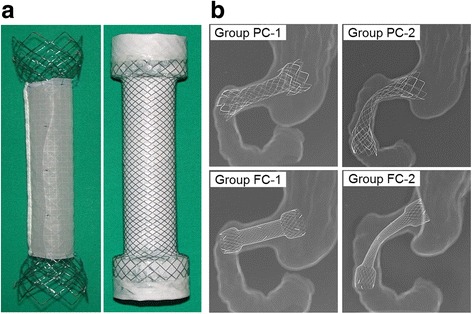
Two types of SEMSs. a PC stent (left) and FC stent (right). b Radiographs of the four groups. Groups PC-1 and Group FC-1 indicate the PC and FC stents with abutment in the duodenal wall, respectively. Groups PC-2 and Group FC-2 indicate the PC and FC stents without abutment, respectively
The stents were divided into four groups according to the types of stents and the location of their distal ends. PC and FC stents were placed so that their distal ends abutted the duodenal wall: groups PC-1 and FC-1, respectively. Conversely, PC and FC stents were placed so that their distal ends were sufficiently directed caudally to prevent stent abutment: groups PC-2 and FC-2, respectively.
Food materials
Three different kinds of radiopaque food materials that varied in their degree of thickness were prepared. Telebrix (30 meglumine, 300 mg/ml; Guerbet, Gorinchem, the Netherlands) was used as the liquid diet. A mixture of yogurt and barium sulfate (98% w/w; E-Z-HD; E-Z-EM Canada Inc., NJ, Canada) in a 3:1 ratio and a mixture of congee and barium sulfate in a 3:1 ratio were used as the soft and solid diets, respectively.
Experiments
Figure 3 shows the experimental setup in the GD phantom. The prepared GD phantom was fixed in an expanded polystyrene foam box, and a silicone tube was connected to the inlet of the GD phantom for inflowing of food materials under fluoroscopic guidance. Inflowing of food materials was controlled by two-piece ball valves to control the flow rate and a general valve for inflowing on/off. Inflowing in the liquid diet was carefully controlled by the ball valve to mimic the situation of drinking water for approximately 4 s (300 ml). To quantitatively evaluate food inflowing differences, elapsed times were measured from when the food material (300 ml in volume) started into the inlet to when the food material (200 ml in volume) passed through the outlet of the GD phantom and was filled in an exit beaker. Twelve elapsed times were acquired with respect to the two conditions of stent placement, two kinds of stents, and three food materials. Each elapsed time was repeated 10 times.
Fig. 3.
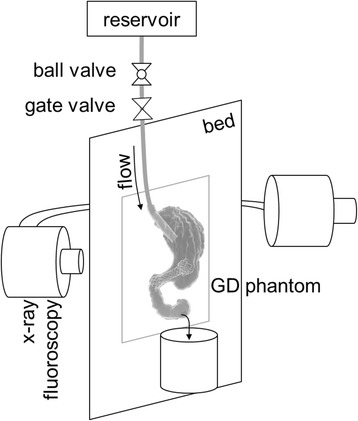
Schematic image of the experimental setup under fluoroscopic guidance: reservoir, two valves, the GD phantom fixed in a foamed polystyrene box, and an exit beaker
Statistical analysis
Variables were compared using Student’s unpaired t test. A two-sided P-value of <0.05 was considered to indicate statistical significance. All statistical analyses were performed using SPSS (version 21, SPSS).
Results
The mean elapsed times for the liquid diet were not significantly different among the four groups (4.21 ± 0.04 s in group PC-1, 4.22 ± 0.04 s in group FC-1, 4.22 ± 0.05 s in group PC-2, and 4.23 ± 0.04 s in group FC-2). For the soft diet, the mean elapsed times were longer in groups PC-1 (7.00 ± 0.09 s) and FC-1 (9.06 ± 0.25 s) than in groups PC-2 (6.88 ± 0.10 s) and FC-2 (8.32 ± 0.10 s), with a statistically significant difference between the stent types (P = 0.018 and P < 0.001, respectively). For the solid diet, the mean elapsed times were longer in group PC-1 (32.35 ± 1.10 s) than in group PC-2 (24.53 ± 0.37 s) (P < 0.001). The mean elapsed time was 42.78 ± 1.33 s in group FC-2; conversely, in group FC-1, the solid diet could not pass through the FC stent because food impaction occurred immediately (Fig. 4).
Fig. 4.
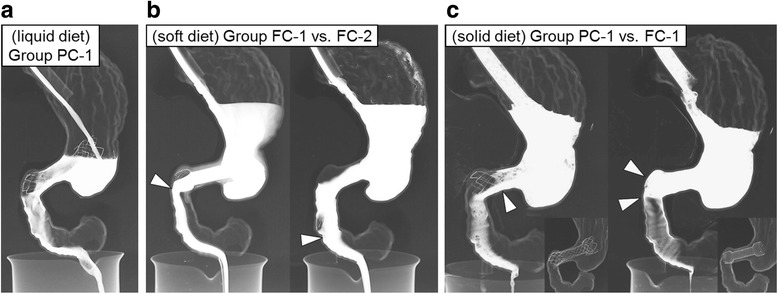
Representative radiographs of food inflowing in the GD phantom. a Radiograph obtained 20 s after inflowing in group PC-1 using the liquid diet shows the disturbance-free passage of radiopaque liquid diet. b Radiographs obtained 20 s after inflowing in groups FC-1 and FC-2 using the soft diet show the narrowing passage of the diet (arrowhead) though the distal end of the stent in group FC-1 and relatively better passage of the diet (arrowhead) though the distal end of the stent in group FC-2. c Radiographs obtained 20 s after inflowing in groups PC-1 and FC-1 using the solid diet show poor passage of the diet through the wire mesh of the stent (arrowhead) in group PC-1 and food impaction (arrowheads) in group FC-1
The mean elapsed times in groups FC-1 and FC-2 was significantly longer than in groups PC-1 and PC-2 for the soft and solid diets (all P < 0.001). The mean elapsed times are summarized in Tables 1 and 2.
Table 1.
Mean elapsed times between the stent abutment and non-stent abutment groups
| Diet type | Partially Covered Stent | Fully Covered Stent | ||||
|---|---|---|---|---|---|---|
| PC-1 | PC-2 | P-value | FC-1 | FC-2 | P-value | |
| Liquid | 4.21 ± 0.04 | 4.22 ± 0.05 | 0.625 | 4.22 ± 0.04 | 4.23 ± 0.03 | 0.609 |
| Soft | 7.00 ± 0.09 | 6.88 ± 0.10 | 0.018 | 9.06 ± 0.25 | 8.32 ± 0.07 | <0.001 |
| Solid | 32.35 ± 1.10 | 24.53 ± 0.38 | <0.001 | FI | 42.78 ± 1.33 | NA |
Note. Unit of data is seconds; FI Food impactiong, NA not applicable
Table 2.
Mean elapsed times between the partially and fully covered stent groups
| Diet type | Stent abutment condition | Non-stent abutment condition | ||||
|---|---|---|---|---|---|---|
| PC-1 | FC-1 | P-value | PC-2 | FC-2 | P-value | |
| Liquid | 4.21 ± 0.04 | 4.22 ± 0.04 | 0.630 | 4.22 ± 0.05 | 4.23 ± 0.03 | 0.714 |
| Soft | 7.00 ± 0.09 | 9.06 ± 0.25 | <0.001 | 6.88 ± 0.10 | 8.32 ± 0.07 | <0.001 |
| Solid | 32.35 ± 1.10 | FI | NA | 24.53 ± 0.38 | 42.78 ± 1.33 | <0.001 |
Note. Unit of data is seconds; FI Food impactiong, NA not applicable
Discussion
It is still not known how food materials move down the GD pathway according to SEMS locations and stent types (PC or FC). Park et al. recently reported that patients with stent abutment were more likely to have food impaction than those without stent abutment, resulting in higher rates of stent malfunction and shorter stent patency durations [8]. They indicated that the distal landing zone of the stent should be located in the second portion of the duodenum to prevent stent abutment. The concept of stent abutment may be useful for avoiding stent malfunction, particularly from food impaction. An experimental study that quantitatively explains food inflowing differences according to stent abutment, even using an artificial GD phantom model, is required.
The results of the present study demonstrated that the mean elapsed times in the passage of a soft and solid diet were significantly longer in the stent abutment groups (PC-1 and FC-1) than in the non-stent abutment groups (PC-2 and FC-2) and that the mean elapsed times were statistically longer with FC stents than with PC stents. Mention The results of our experimental study correlated with clinically significant findings of stent abutment in patients with GOO [8].
The GOO scoring system [14] the Song dysphagia classification [3] was routinely used to evaluate the severity of dysphagia before and after stent placement. The scores were based on the ability to swallow liquid, soft, and solid diets [3, 14]. To establish radiopaque liquid, soft, and solid diets, a water-soluble contrast medium and barium sulfate with a mixture of yogurt and congee were used in the present study. The elapsed times using these diets were investigated according to the stent abutment with two different types of SEMS. The results of our experimental study under fluoroscope guidance showed different elapsed times according to the food materials.
In the representative radiographs (Fig. 4), a typical liquid diet showed inflowing without any disturbance in the experimental setup. For soft diets with the FC stent, the non-stent abutment group showed better inflowing performance at the end of the stent than the stent abutment group (white arrow heads in Fig. 4b). Figure 4c shows food impaction found in the FC stent group under stent abutment for the solid diet (white arrow heads on the right). Conversely, in the PC stent group, diet inflowing in the GD phantom was very narrow but food impaction did not occur under the same stent abutment conditions (white arrow head on the left). We believe that the position of the distal ends of the stent is very important during stent placement in patients with GOO.
3D reconstructed images are not only pivotal in making a diagnosis but also essential in the advent of 3DP in the medical field using a tangibly fabricated 3D model [15, 16]. With the recent medical trend toward “personalized” or “patient-specific” treatment, 3DP has well-suited characteristics in the field of medicine [16]. It can perform one-stop manufacturing from radiological images to patient-specific phantoms, simulators, surgical guides, or implantable devices [17–21]. The recently commercialized 3D printable multi-materials with transparent, full-colored, and flexible properties accelerate its applications to more extensive medical fields [16, 22–24]. In the present study, a patient-specific and anthropomorphic GD phantom was fabricated using 3DP based on CTG images. However, the GOO region of the initial GD STL model was modified to fit the stent size.
We attempted to mimic GD food inflowing with the maximum amount of effort in the present phantom study, but it is still far from reality. Firstly, the 3D printable material used is flexible but not enough to mimic real GD properties due to their technical limitations. One could also utilize a 3D printing-based molding method using silicone materials whose mechanical properties are more controllable. The mechanical properties of GD tissue, such as shore hardness and elongation, also need to be determined. Secondly, we need to materialize gastric peristalsis with a motorized system for obtaining more realistic digesting situations. With these methodological advances, it is expected that more realistic GD situations can be mimicked in future experimental phantom studies.
Conclusions
The findings of the present study revealed that stent abutment can cause prolonged passage of soft and solid diets through the stent and can also cause impaction of the solid diet into the stent. Therefore, we believe that when a stent is placed in the gastric outlet bridging the gastric pylorus, the distal end of the stent should be directed caudally to prevent stent abutment.
Acknowledgments
This research was supported by a grant (2015-672 and 2016-681) from the Asan Institute for Life Sciences, Asan Medical Center, Seoul, Korea.
Funding
This study was supported by grants (2015–672 and 2016–681) from the Asan Institute for Life Sciences, Asan Medical Center, Seoul, South Korea.
Availability of data and materials
Readers interested in the data should contact the authors.
Abbreviations
- 3D
Three-dimensional
- 3DP
3D printing
- CTG
Computed tomography gastrography
- FC
Fully covered
- GD
Gastroduodenal
- GOO
Gastric outlet obstruction
- LPO
Left posterior oblique
- PC
Partially covered
- SEMS
Self-expandable metallic stent
- STL
Stereolithography
Authors’ contributions
GK designed of the study and drafted the manuscript. JP also designed the study and performed the in vitro experiments. GK and JP contributed equally to this work and share first authorship. HS supervised the preparation of the manuscript as a corresponding author. NK supervised the designing of the study as a corresponding author. HS and NK contributed equally to this work as corresponding authors. KK performed the in vitro experiments. JT and EJ designed the study and drafted the manuscript. DK analyzed the study parameters from the clinical point of view. GL analyzed the study parameters and prepared the 3D printing phantom. All authors read and approved the final manuscript.
Ethics approval and consent to participate
This manuscript contains a retrospective CTG data of human. (IRB may be not required.)
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Guk Bae Kim, Email: geud.kim@gmail.com.
Jung-Hoon Park, Email: jhparkz1125@gmail.com.
Ho-Young Song, Phone: 82-2-3010-4370, Email: hysong@amc.seoul.kr.
Namkug Kim, Phone: 82-2-3010-6573, Email: namkugkim@gmail.com.
Hyun Kyung Song, Email: songhk092@gmail.com.
Min Tae Kim, Email: soir09@naver.com.
Kun Yung Kim, Email: kky2kkw@gmail.com.
Jiaywei Tsauo, Email: 80732059@qq.com.
Eun Jung Jun, Email: ejjun@amc.seoul.kr.
Do Hoon Kim, Email: dohoon.md@gmail.com.
Gin Hyug Lee, Email: jhlee409@amc.seoul.kr.
References
- 1.Jung G-S, Song H-Y, Kang S-G, et al. Malignant gastroduodenal obstructions: treatment by means of a covered expandable metallic stent—initial experience 1. Radiology. 2000;216:758–763. doi: 10.1148/radiology.216.3.r00au05758. [DOI] [PubMed] [Google Scholar]
- 2.Park KB, Do YS, Kang WK, et al. Malignant obstruction of gastric outlet and duodenum: palliation with flexible covered metallic stents 1. Radiology. 2001;219:679–683. doi: 10.1148/radiology.219.3.r01jn21679. [DOI] [PubMed] [Google Scholar]
- 3.Song H-Y, Shin JH, Yoon CJ, et al. A dual expandable nitinol stent: experience in 102 patients with malignant gastroduodenal strictures. J Vasc Interv Radiol. 2004;15:1443–1449. doi: 10.1097/01.RVI.0000142594.31221.AF. [DOI] [PubMed] [Google Scholar]
- 4.Kim JH, Song H-Y, Shin JH, et al. Metallic stent placement in the palliative treatment of malignant gastroduodenal obstructions: prospective evaluation of results and factors influencing outcome in 213 patients. Gastrointest Endosc. 2007;66:256–264. doi: 10.1016/j.gie.2006.12.017. [DOI] [PubMed] [Google Scholar]
- 5.Tringali A, Didden P, Repici A, et al. Endoscopic treatment of malignant gastric and duodenal strictures: a prospective, multicenter study. Gastrointest Endosc. 2014;79:66–75. doi: 10.1016/j.gie.2013.06.032. [DOI] [PubMed] [Google Scholar]
- 6.Park J-H, Song H-Y, Yun S-C, et al. Gastroduodenal stent placement versus surgical gastrojejunostomy for the palliation of gastric outlet obstructions in patients with unresectable gastric cancer: a propensity score-matched analysis. Eur Radiol. 2016;26:2436–45. [DOI] [PubMed]
- 7.Park J-H, Lee JH, Song H-Y, et al. Over-the-wire versus through-the-scope stents for the palliation of malignant gastric outlet obstruction: a retrospective comparison study. Eur Radiol. 2016;26:4249–58. [DOI] [PubMed]
- 8.Park J-H, Kim GB, Song H-Y, et al. Significance of stent abutment in gastroduodenal stent placement for gastric outlet obstructions. J Vasc Interv Radiol. 2017;28(8):1147–1153. doi: 10.1016/j.jvir.2017.01.013. [DOI] [PubMed] [Google Scholar]
- 9.Zein NN, Hanouneh IA, Bishop PD, et al. Three-dimensional print of a liver for preoperative planning in living donor liver transplantation. Liver Transpl. 2013;19:1304–1310. doi: 10.1002/lt.23729. [DOI] [PubMed] [Google Scholar]
- 10.Akiba T, Inagaki T, Nakada T. Three-dimensional printing model of anomalous bronchi before surgery. Ann Thorac Cardiovasc Surg. 2014;20:659–662. doi: 10.5761/atcs.cr.13-00189. [DOI] [PubMed] [Google Scholar]
- 11.Bustamante S, Bose S, Bishop P, Klatte R, Norris F. Novel application of rapid prototyping for simulation of bronchoscopic anatomy. J Cardiothorac Vasc Anesth. 2014;28:1134–1137. doi: 10.1053/j.jvca.2013.08.015. [DOI] [PubMed] [Google Scholar]
- 12.Nakada T, Akiba T, Inagaki T, Morikawa T. Thoracoscopic anatomical subsegmentectomy of the right S2b+ S3 using a 3D printing model with rapid prototyping. Interact Cardiovasc Thorac Surg. 2014;19:696–698. doi: 10.1093/icvts/ivu174. [DOI] [PubMed] [Google Scholar]
- 13.Kim HJ, Kim AY, Lee JH, Yook JH, Yu ES, Ha HK. Positioning during CT gastrography in patients with gastric cancer: the effect on gastric distension and lesion conspicuity. Korean J Radiol. 2009;10:252–259. doi: 10.3348/kjr.2009.10.3.252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Adler DG, Baron TH. Endoscopic palliation of malignant gastric outlet obstruction using self-expanding metal stents: experience in 36 patients. Am J Gastroenterol. 2002;97:72–78. doi: 10.1111/j.1572-0241.2002.05423.x. [DOI] [PubMed] [Google Scholar]
- 15.Doi K. Diagnostic imaging over the last 50 years: research and development in medical imaging science and technology. Phys Med Biol. 2006;51:R5. doi: 10.1088/0031-9155/51/13/R02. [DOI] [PubMed] [Google Scholar]
- 16.Kim GB, Lee S, Kim H, et al. Three-dimensional printing: basic principles and applications in medicine and radiology. Korean J Radiol. 2016;17:182–197. doi: 10.3348/kjr.2016.17.2.182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rengier F, Mehndiratta A, von Tengg-Kobligk H, et al. 3D printing based on imaging data: review of medical applications. Int J Comput Assist Radiol Surg. 2010;5:335–341. doi: 10.1007/s11548-010-0476-x. [DOI] [PubMed] [Google Scholar]
- 18.Ventola CL. Medical applications for 3D printing: current and projected uses. Pharm Ther. 2014;39:704. [PMC free article] [PubMed] [Google Scholar]
- 19.Liew Y, Beveridge E, Demetriades AK, Hughes MA. 3D printing of patient-specific anatomy: a tool to improve patient consent and enhance imaging interpretation by trainees. Br J Neurosurg. 2015;29(5):712–4. [DOI] [PubMed]
- 20.Mitsouras D, Liacouras P, Imanzadeh A, et al. Medical 3D printing for the radiologist. Radiographics. 2015;35:1965–1988. doi: 10.1148/rg.2015140320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Valverde I, Gomez G, Coserria JF, et al. 3D printed models for planning endovascular stenting in transverse aortic arch hypoplasia. Catheter Cardiovasc Interv. 2015;85:1006–1012. doi: 10.1002/ccd.25810. [DOI] [PubMed] [Google Scholar]
- 22.Zopf DA, Hollister SJ, Nelson ME, Ohye RG, Green GE. Bioresorbable airway splint created with a three-dimensional printer. N Engl J Med. 2013;368:2043–2045. doi: 10.1056/NEJMc1206319. [DOI] [PubMed] [Google Scholar]
- 23.Ionita CN, Mokin M, Varble N, et al. Challenges and limitations of patient-specific vascular phantom fabrication using 3D Polyjet printing. In: SPIE Medical Imaging. International Society for Optics and Photonics, pp 90380M-90380M-90312; 2014. [DOI] [PMC free article] [PubMed]
- 24.Waran V, Narayanan V, Karuppiah R, Owen SL, Aziz T. Utility of multimaterial 3D printers in creating models with pathological entities to enhance the training experience of neurosurgeons: technical note. J Neurosurg. 2014;120:489–492. doi: 10.3171/2013.11.JNS131066. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Readers interested in the data should contact the authors.