

Abstract
Purpose
We evaluated the effect on long-term survival of adding rituximab (R) to BEAM (carmustine, etoposide, cytarabine, and melphalan) conditioning with or without yttrium-90 ibritumomab tiuxetan (90YIT) in patients with relapsed diffuse large B-cell lymphoma (DLBCL) undergoing autologous stem cell transplant (ASCT).
Experimental design
Patients were enrolled on three consecutive phase 2 clinical trials. Patients received two doses of rituximab (375 mg/m2 and 1000 mg/m2) during mobilization of stem cells, followed by 1000 mg/m2 on days +1 and +8 after ASCT with R-BEAM or 90YIT-R-BEAM (90YIT dose of 0.4 mCi/kg) conditioning.
Results
One hundred thirteen patients were enrolled, with 73 receiving R-BEAM and 40 receiving 90YIT-R-BEAM. All patients had a prior exposure to rituximab. The median follow-up intervals for survivors were 11.8, 8.1, and 4.2 years in the three trials, respectively. The 5-year disease-free survival (DFS) rates were 62% for R-BEAM and 65% for 90YIT-R-BEAM (P =0.82). The 5-year overall survival rates were 73%, and 77%, respectively (P = 0.65). In patients with de novo DLBCL, survival outcomes of the germinal center/activated b-cell histologic subtypes were similar with 5-year OS rates (P = 0.52) and DFS rates (P = 0.64), irrespective of their time of relapse (< vs. > 1 year) after initial induction chemotherapy (P = 0.97).
Conclusions
Administering ASCT with rituximab during stem cell collection and immediately after transplantation induces long-term disease remission and abolishes the negative prognostic impact of cell-of-origin in patients with relapsed DLBCL. The addition of 90YIT does not confer a further survival benefit.
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common type of B-cell non-Hodgkin lymphoma, constituting up to 35% of all cases worldwide (1). Currently, a 5-year disease-free survival of 70% is achievable for patients with favorable prognostic factors at diagnosis (2). Unfortunately, about one-third of patients will eventually experience relapse. For these patients, the Parma trial established the use of high-dose chemotherapy with autologous stem cell transplant (ASCT) as the standard of care (3). The combination of carmustine, etoposide, cytarabine, and melphalan (BEAM) is commonly used as a conditioning regimen for these patients (4). However, in more than 50% of patients undergoing ASCT, disease relapse remains the cause of treatment failure (3–5). None of the different tested chemotherapy-based conditioning regimens have proven superior to any other.
DLBCL is a heterogeneous disease that includes at least three major subtypes: germinal center B-cell–like (GCB), activated B-cell–like, and primary mediastinal large B-cell lymphoma; and these subtypes differ in their activation of signaling pathways, and clinical outcomes (6,7). In recent years, studies have suggested that patients who were previously exposed to rituximab, or had experienced a relapse within one year of induction chemotherapy, or had de novo DLBCL of non-GCB histologic subtype, have been associated with poor outcomes after ASCT with BEAM alone, without rituximab (8).
A major concern in the use of ASCT is the potential presence of occult tumor cells in the harvested stem cells that may contribute to disease relapse (9, 10). Studies have shown that in vivo therapy with rituximab is highly effective in purging B-cells from clonal cancer cells (11, 12) We have previously reported that concurrent administration of rituximab with stem cell collection and immediately after ASCT results in significantly improved overall survival (OS) (80% vs 53%, P = 0·002) and disease-free survival (DFS) (67% vs 43%, P = 0.004) (13). Furthermore, radiolabeled anti-CD20 monoclonal antibodies, such as yttrium-90 ibritumomab tiuxetan (90YIT), have been added to the conditioning regimen with the premise of enhancing the antitumor effects for DLBCL. While several prospective phase 1 and 2 reports showed promising safety profiles and responses (14–17), multi-center randomized trials failed to show improved survival compared with standard BEAM (18, 19). However, none of these studies incorporated rituximab for in vivo purging and none have addressed whether the addition of rituximab with or without radio-immunotherapy could overcome the negative prognostic factors described that include non-GCB histologic subtype, especially in patients who were previously exposed to rituximab or experienced a relapse within one year of induction chemotherapy. Herein, we report long-term survival outcomes of the use of rituximab from two prospective phase 2 trials and one randomized phase 2 investigator-initiated trial, with or without the addition of 90YIT to the conditioning regimen.
Materials and Methods
Study design and eligibility criteria
This study represents the combined analysis of 113 adult patients with persistent or relapsed DLBCL who received ASCT on two consecutive phase 2 trials and one randomized phase 2 investigator-initiated trial conducted at The University of Texas MD Anderson Cancer Center (Houston, TX, USA). The trials included one using rituximab with BEAM, or R-BEAM (1999-2003), and reported on 57 patients with relapsed DLBCL (group A); a second trial (NCT01538472; 2004-2006) of 90YIT with R-BEAM, or 90YIT-R-BEAM (26 patients) (group B); and a randomized phase 2 trial (NCT00591630; 2007-2010) comparing R-BEAM to 90YIT-R-BEAM (16 [group C] and 14 [group D] patients, respectively). The first trial has been published (13) and additional follow-up is provided here after excluding 10 patients who had follicular lymphoma in the original report. The phase 2 randomized clinical trial was monitored by the Data and Safety Monitoring Board at our institution and was closed early due to slow accrual. Patients were then grouped into those receiving the R-BEAM conditioning regimen (n = 73, groups A and C) and those receiving the 90YIT-R-BEAM conditioning regimen (n = 40, groups B and D).
The eligibility criteria were similar in all three trials. Patients with CD20-positive DLBCL with persistent or relapsed disease chemosensitive to salvage treatments were included. Other inclusion criteria were age 18-65 years (later changed to 70 years in groups C and D); less than 10% bone marrow involvement by lymphoma at the time of study entry as defined by bone marrow histologic examination; an Eastern Cooperative Oncology Group performance status score of 0-2; adequate liver function with serum bilirubin level of ≤1.5 mg/dL and liver enzyme concentrations no more than 2 times the upper limit of normal; adequate renal function with a serum creatinine level of <1.6 mg/dL; adequate cardiac function defined as an ejection fraction higher than 50%; and adequate pulmonary function defined as higher than 50% of predictive value. In addition, patients enrolled on 90YIT-containing trials were required to have a platelet count of ≥ 100 x109/L and an absolute neutrophil count of ≥ 1.5 x109/L.
The treatment trials and this study analysis were reviewed and approved by the Institutional Review Board. They were conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all patients.
Procedures
All patients received rituximab at a dose of 375 mg/m2 the day before chemo-mobilization (which consisted of ifosfamide [3.33 g/m2 daily for 3 days] and etoposide [150 mg/m2 twice per day, or bid, for 3 days] in most patients) and again at 1000 mg/m2 7 days later and on days +1 and +8 after transplant (13). The BEAM conditioning regimen before transplant was prescribed previously (13). In addition to this R-BEAM regimen, patients in groups B and D received 90YIT. On day −21 before ASCT, rituximab (250 mg/m2) was followed immediately by a dosage of the murine monoclonal anti-CD20 IT radioiodinated with 5 mCi indium-111 (111InIT) infused intravenously over 10 minutes, for radioimaging. Next, a 90YIT infusion at a therapeutic dosage (0.4 mCi/kg) was performed on day −14 before the transplant. The BEAM regimen was started on day −7. Stem cells were infused on day 0.
The histologic findings in all cases were reviewed by a hematopathologist for confirmation of the diagnosis. The cell-of-origin was mainly determined using the Hans immunohistochemical algorithms in coordination with Visco and/or Choi algorithms in 52 of 70 (74%) patients with de novo DLBCL and available biopsy specimens from lymph nodes (20–22). Disease stage was evaluated using Ann Arbor criteria, and each patient was assigned an International Prognostic Index (IPI) score (23) at the time of study entry. Patients enrolled in the randomized phase 2 trial underwent pre-transplant measurement of rituximab serum concentrations by an enzyme-linked immunosorbent assay. Whole body fluorine-18 fluorodeoxyglucose positron emission tomography (PET)-x-ray computed tomography (CT) scanning was routinely performed for all patients at our center starting in December, 2002. Patients were assessed by CT of the neck, chest, abdomen, and pelvis or whole body PET-CT imaging 1, 3, 6, and 12 months after the end of treatment, then every 6 months for 5 years, and then yearly afterwards using the criteria of Cheson et al (23, 24).
Statistical analysis
The primary objective of this study was to compare the conditioning regimens R-BEAM and 90YIT-R-BEAM across three consecutive protocols at MD Anderson with regard to 5-year overall survival (OS) and disease-free survival (DFS) rates for ASCT in patients with relapsed DLBCL. The secondary objectives were determining predictors of OS and DFS, including histologic subtypes of DLBCL, time of relapse from initial induction chemotherapy, types of salvage therapy received, and evaluating treatment-related mortality.
The covariates of patient and disease characteristics were compared using the Wilcoxon rank-sum test, chi-square test, or Fisher exact test, as appropriate. OS was defined as the time from transplant to death from any cause. DFS was defined as the time to disease relapse or progression, or death, measured from the time of transplant, with patients censored at time of last contact.
The survival times (OS and DFS) were calculated in years from the date of transplant. Survival times were compared at 5 years after transplant to ensure the longest comparable follow-up intervals from the three trials.
A univariate analysis was conducted for each covariate of interest. Multivariate survival analysis was then conducted using backward elimination on the basis of the likelihood ratio test and including the conditioning regimens and all the factors with P < 0.1 in the univariate analyses. Kaplan-Meier survival analysis was used to calculate the median survival time estimations. Relapse mortality was assessed in a competing risk framework. All statistical analyses were conducted with SAS 9.4 (SAS Institute, Cary, NC) and R software. The statistical tests were two-sided, and P < 0·05 was considered statistically significant.
Results
Patient selection
Between June, 2000 through May, 2010, 113 patients with persistent or relapsed DLBCL at MD Anderson were enrolled on two phase 2 trials (one for R-BEAM [group A] and one for 90YIT-R-BEAM [group B]) and one randomized trial comparing these two conditioning regimens - R-BEAM and 90YIT-R-BEAM (groups C and D). Patient demographic characteristics and baseline disease characteristics of the four groups are listed in Appendix Table A1. The median number of prior lines of chemotherapy at study entry was the only covariate that differed significantly between the four groups, with the R-BEAM arms being more heavily pre-treated (Supplementary Table A1). Patients were grouped into those receiving the R-BEAM conditioning regimen (n = 73, groups A and C) and those receiving the 90YIT-R-BEAM conditioning regimen (n = 40, groups B and D). There were no significant differences in demographic or disease characteristics between the groups with and without 90YIT (Table 1).
Table 1.
Demographic characteristics and baseline disease characteristics
| Characteristic | Conditioning regimen
|
P | |
|---|---|---|---|
| R-BEAM (N = 73) | 90YIT-R-BEAM (N = 40) | ||
| Age | |||
| Median | 52.4 years | 52.4 years | 0.66a |
| Range | 19.6-69.7 years | 30.9-69.4 years | |
| Sex, no. (%) | |||
| Male | 41(56.2) | 25(62.5) | 0.51b |
| Female | 32(43.8) | 15(37.5) | |
| Disease status at transplant, no. (%) | |||
| PR | 35(47.9) | 20(50.0) | 0.95c |
| CR | 35(47.9) | 18(45.0) | |
| SD | 3(4.1) | 2(5.0) | |
| No. of prior chemotherapies | |||
| No., median | 73, 2.0 | 40, 2.0 | 0.08a |
| Range | 1.0-5.0 | 1.0-4.0 | |
| ≤2, no. (%) | 44(60.3) | 30(75.0) | 0.12b |
| >2, no. (%) | 29(39.7) | 10(25.0) | |
| ≤3, no. (%) | 66(90.4) | 39(97.5) | 0.26c |
| >3, no. (%) | 7(9.6) | 1(2.5) | |
| Salvage therapy pre-transplant, no. (%) | |||
| AP | 21(28.8) | 12(30.0) | 0.55b |
| ICE/IE | 37(50.7) | 23(57.5) | |
| Other | 15(20.6) | 5(12.5) | |
| LDH level at transplant | |||
| Normal, no. (%) | 61(83.6) | 32(80.0) | 0.64b |
| Elevated, no. (%) | 12(16.4) | 8(20.0) | |
| Beta2-microglobulin level, mg/L | |||
| No., median | 2.2 | 2.0 | 0.08a |
| Range | 1.3-8.0 | 1.2-6.5 | |
| Histologic subtype, no. (%) | |||
| De novo | 45(61.7) | 25(62.5) | 0.38b |
| -GCB | −11(15.1) | −10(25.0) | |
| -Non-GCB | −23(31.5) | −8(20.0) | |
| -Unknown | −11(15.1) | −7(17.5) | |
| PMBL | 5(6.8) | 4(10.0) | |
| Transformed | 23(31.5) | 11(27.5) | |
| Relapse < 1 year (De novo histology) | 20(44.4) | 9(36.0) | 0.27b |
| IPI score at transplant, no. (%) | |||
| 0 | 49(67.1) | 32(82.1) | 0.09b |
| >0 | 24(32.9) | 7(17.9) | |
| PET status at transplant, no. (%) | |||
| Negative | 26/34(76.5) | 34(85.0) | 0.35b |
| Positive | 8/34(23.5) | 6(15.0) | |
| CD34-positive cells infused, 106/kg | |||
| Median | 5.5 | 5.7 | 0.46a |
| Range | 0.9*-17.3 | 2.8-35.4 | |
Wilcoxon rank-sum test;
Chi-square test;
Fisher exact test; R-BEAM, carmustine, etoposide, cytarabine, and melphalan with rituximab; 90YIT, yttrium-90 ibritumomab tiuxetan; PR, partial response; CR, complete response; SD, stable disease; LDH, lactate dehydrogenase; GCB, germinal center B-cell–like; PMBL, primary mediastinal large B-cell lymphoma; IPI, International Prognostic Index; PET, positron emission tomography; ICE, ifosfamide, carboplatin, and etoposide; IE, ifosfamide and etoposide; AP, high-dose cytarabine and cisplatin.
Graft from bone marrow
Engraftment
Peripheral-blood progenitor cells were the source of the autologous grafts for 111 (98%) patients, in the four groups. Two patients in Group A received marrow cells. The median numbers of CD34-positive cells infused in the 90YIT-R-BEAM and R-BEAM groups were 5.7 × 106/kg and 5.5 × 106/kg, respectively (P = 0.46). The median times to recovery of absolute neutrophil count to ≥ 0.5 × 109 cells/L in the 90YIT-R-BEAM and R-BEAM groups were 9.5 days (range, 7-30) and 11 days (range, 8-30), respectively (P < 0.001), and the median times to a platelet count of >20 × 109 cells/L were 11.5 days (range, 2-30) and 11 days (range, 6-30), respectively (P = 0.64).
Survival
The median follow-up intervals for surviving patients was 11.8 years for group A, 8.1 years for group B, 4.8 years for group C, and 4.1 years for group D. There were no significant differences in survival outcome between the R-BEAM and 90YIT-R-BEAM groups, with 5-year DFS rates of 62% (95% confidence interval [CI], 0.50-0.73) and 65% (95% CI, 0.50-0.80), respectively (P = 0.82; Fig. 1A) and 5-year OS rates of 73% (95% CI, 0.62-0.83) and 77% (95% CI, 0.64-0.90), respectively (P = 0.65; Fig. 1B). We found no differences in 5-year DFS (P = 0.99, Supplementary Fig. A1) or OS rates (P = 0.46) between the four groups analyzed separately.
Figure 1.
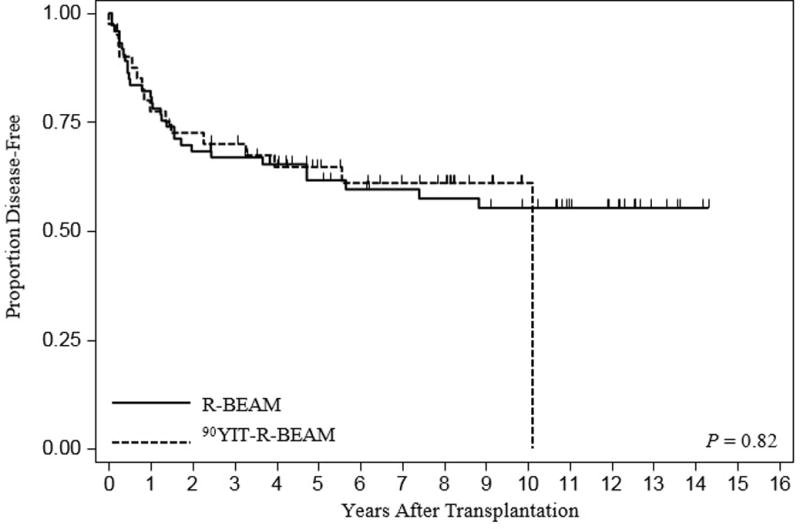
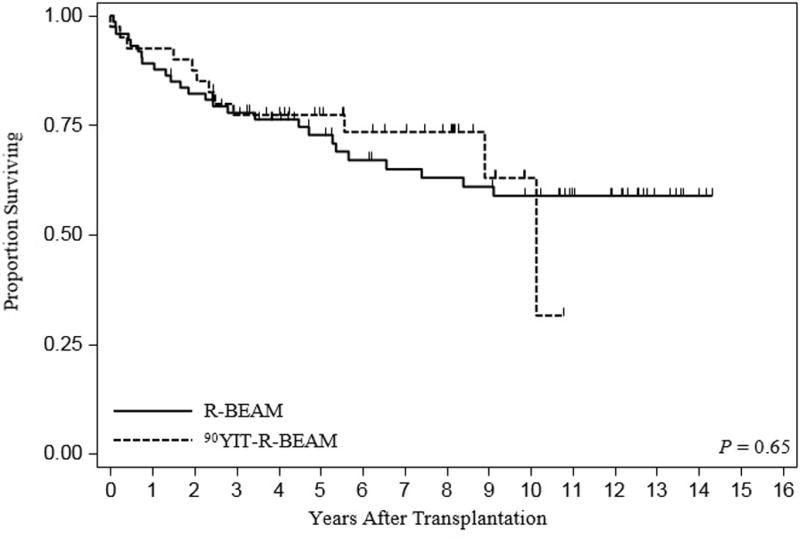
(A) Kaplan-Meier survival curves of disease-free survival with and without radioimmunotherapy. (B) Kaplan-Meier survival curves of overall survival with and without radioimmunotherapy.
We also compared survival outcomes between histologic subtypes, although this covariate was not part of the objectives of the original protocols. We observed similar 5-year OS rates (P = 0.52) and DFS rates (P = 0.64) for patients with transformed DLBCL or for patients with mediastinal DLBCL, or DLBCL with a GCB or non-GCB immunophenotype (Fig. 2A and B).
Figure 2.
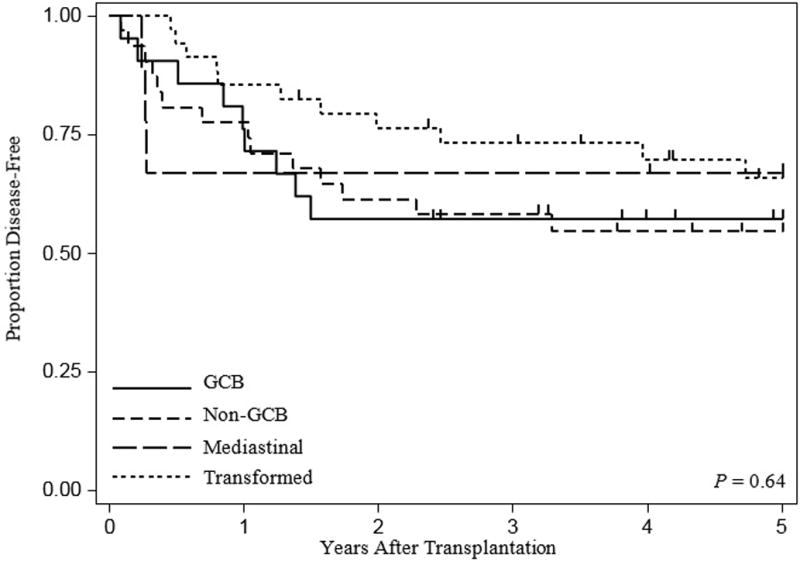
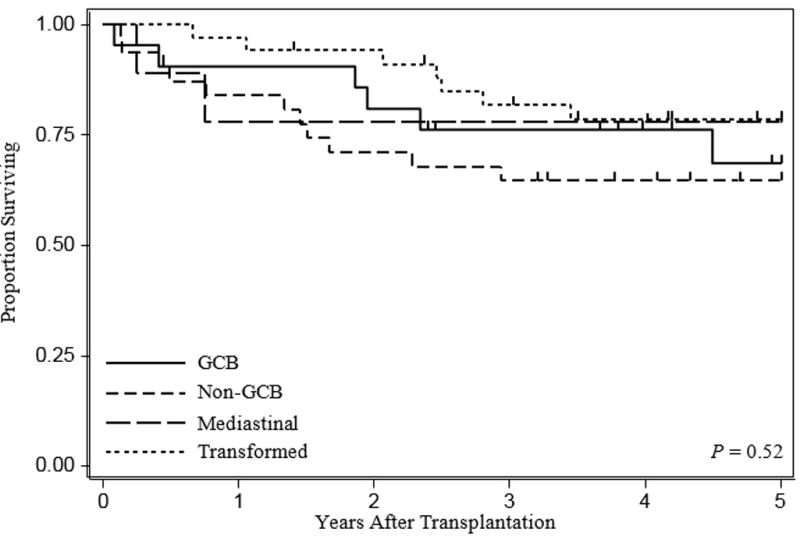
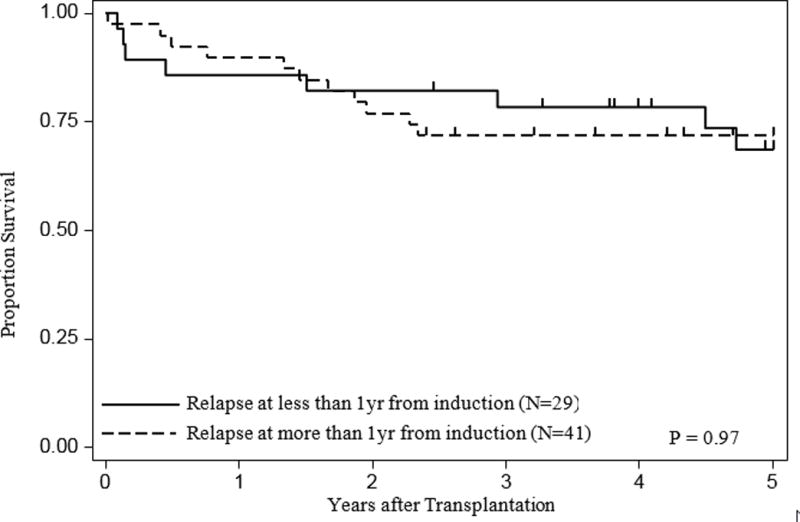
(A) Kaplan-Meier survival curves of disease-free survival according to histologic immunophenotypes. (B) Kaplan-Meier survival curves of overall survival according to histologic immunophenotypes. (C) Kaplan-Meier survival curves of overall survival in patients with de novo DLBCL according to time of relapse <1 vs > 1 year) from their induction chemotherapy
Prognostic factors
On univariate analysis, OS was significantly worse for patients with a serum beta2-microglobulin level of >2 mg/L, IPI score of >0 prior chemo-mobilization, prior chemotherapy regimens >3, and PET positivity at the time of study enrollment (Table 2). All of these factors except beta2-microglobulin level remained predictors of OS on multivariate analysis (Table 3).
Table 2.
Univariate analyses for disease-free survival and overall survival
| Covariate | Disease-free survival | Overall survival | ||||
|---|---|---|---|---|---|---|
|
|
||||||
| HR | 95% CI | P | HR | 95% CI | P | |
| Conditioning regimen | ||||||
| 90YIT-R-BEAM | 1.00 | 1.00 | ||||
| R-BEAM | 1.08 | 0.57-2.06 | 0.82 | 1.20 | 0.54-2.66 | 0.65 |
| Age | 1.03 | 1.00-1.06 | 0.10 | 1.03 | 0.99-1.07 | 0.18 |
| Sex | ||||||
| Male | 1.00 | 1.00 | ||||
| Female | 1.11 | 0.60-2.05 | 0.75 | 1.04 | 0.49-2.20 | 0.92 |
| Disease status at transplant | ||||||
| PR | 1.00 | 1.00 | ||||
| CR | 0.77 | 0.41-1.47 | 0.43 | 0.80 | 0.36-2.71 | 0.57 |
| SD | 1.91 | 0.57-6.40 | 0.30 | 3.03 | 0.87-10.57 | 0.08 |
| No. of prior chemotherapies | ||||||
| Total chemotherapies | 1.51 | 1.05-2.18 | 0.03 | 1.54 | 0.99-2.40 | 0.05 |
| ≤3 | 1.00 | 1.00 | ||||
| >3 | 2.20 | 1.10-4.39 | 0.03 | 3.02 | 1.05-8.74 | 0.04 |
| LDH level at transplant | ||||||
| Normal | 1.00 | 1.00 | ||||
| Elevated | 2.20 | 1.10-4.39 | 0.03 | 2.21 | 0.97-5.03 | 0.06 |
| Beta2-microglobulin level | ||||||
| ≤2 | 1.00 | 1.00 | ||||
| >2 | 1.75 | 0.92-3.36 | 0.09 | 2.34 | 1.03-5.31 | 0.04 |
| Histologic subtype | ||||||
| GCB | 1.00 | 1.00 | ||||
| Non-GCB | 1.04 | 0.45-2.41 | 0.92 | 1.32 | 0.49-3.58 | 0.58 |
| PMBL | 0.80 | 0.22-2.95 | 0.73 | 0.78 | 0.16-3.87 | 0.76 |
| Transformed | 0.65 | 0.27-1.56 | 0.33 | 0.66 | 0.22-1.97 | 0.46 |
| Relapse from induction (de novo histology) | ||||||
| <1 year | 1.00 | 1.00 | ||||
| >1 year | 0.75 | 0.35-1.59 | 0.45 | 0.98 | 0.39-2.44 | 0.97 |
| Salvage therapy pre-transplant | ||||||
| ICE/IE | 1.00 | 1.00 | ||||
| AP | 1.13 | 0.55-2.31 | 0.74 | 1.15 | 0.48-2.78 | 0.75 |
| Other | 1.40 | 0.64-3.07 | 0.40 | 1.50 | 0.60-3.76 | 0.39 |
| IPI score at transplant | ||||||
| 0 | 1.00 | 1.00 | ||||
| >0 | 3.14 | 1.69-5.86 | <0.001 | 3.31 | 1.57-6.95 | <0.001 |
| PET status at transplant | ||||||
| Negative | 1.00 | 1.00 | ||||
| Positive | 3.40 | 1.52-7.63 | <0.001 | 5.59 | 2.26-13.9 | <0.001 |
| Amount of CD34-positive cells infused | 0.88 | 0.78-1.00 | 0.06 | 0.87 | 0.74-1.02 | 0.09 |
HR, hazard ratio; CI, confidence interval; PR, partial response; CR, complete response; SD, stable disease; LDH, lactate dehydrogenase; GCB, germinal center B-cell-like; PMBL, primary mediastinal large B-cell lymphoma; IPI, International Prognostic Index; PET, positron emission tomography; ICE, ifosfamide, carboplatin, and etoposide; IE, ifosfamide and etoposide; AP, high-dose cytarabine and cisplatin.
Table 3.
Multivariate analysis for disease-free survival and overall survival
| Covariate | DFS | OS | ||||
|---|---|---|---|---|---|---|
|
| ||||||
| HR | 95% CI | P | HR | 95% CI | P | |
| Regimen | ||||||
| R-BEAM vs. 90YIT-R-BEAM | 1.26 | 0.62-2.46 | 0.511 | 1.20 | 0.44-3.34 | 0.716 |
| No. of prior chemotherapies | 1.78 | 1.17-2.62 | 0.005 | 2.00 | 1.08-3.61 | 0.022 |
| IPI score at transplant, >0 vs. 0 | 3.70 | 1.93-7.10 | <0.001 | 3.26 | 1.21-8.61 | 0.017 |
| PET status at transplant, positive v negative | 3.29 | 1.22-8.80 | 0.010 | |||
DFS, disease-free survival; OS: overall survival; HR, hazard ratio; CI, confidence interval; IPI, International Prognostic Index; PET, positron emission tomography.
Potential predictors of DFS were also analyzed by univariate analysis, which showed that elevated LDH, IPI score of >0 prior chemo-mobilization, number of prior chemotherapy regimens, and PET positivity were significant prognostic factors for DFS (Table 2). The number of prior chemotherapy regimens and IPI score remained significant predictors of DFS on multivariate analysis (Table 3). We observed no significant effect on DFS or OS for salvage chemotherapy regimen or histologic subtype.
Seventy patients had de novo DLBCL. Twenty-nine (41.4%) patients experienced a relapse within one year of their initial induction chemotherapy, and 41 (58.6) beyond one year. We observed no significant difference in 5-year DFS or OS between the two groups (Table 2; Fig. 2C). Similar results were observed, when analysis was limited to those patients with known GCB and non-GCB histologic subtypes.
Causes of death
At the time of data analysis, death had been reported in 28 patients (24.8%). The most common cause of death was progression or relapse (n = 23), followed by non–relapse-related mortality (n = 5). The 5-year rate of secondary hematologic malignancies in all patients was 6.2%. Four additional patients developed secondary solid-organ malignancies, with a cumulative incidence of 3.5%. There was no significant difference in the rates of secondary malignancies between patients receiving R-BEAM and those receiving 90YIT-R-BEAM.
Discussion
This report shows that the addition of in vivo therapy with rituximab during autologous stem cell collection and immediately after ASCT in patients with chemotherapy-sensitive relapsed DLBCL offers 5-year DFS and OS rates of 62% and 73%, respectively. These results confirm those reported previously by our group in 2005 (13), in a study of 57 DLBCL patients also included in the present report and who have a median follow-up time of 11.8 years for those surviving. All patients in our study were exposed to rituximab prior to ASCT, a feature that was reported by others to have a negative impact on survival. Our data suggest that the treatment can overcome the negative prognosis associated with non-GCB subtype and time to relapse from induction chemotherapy in patients with de novo DLBCL. The addition of 90YIT to R-BEAM did not have any additional benefit.
Studies have shown that high-dose (25) or more frequent doses (26) of rituximab may increase the response rate in B-cell malignancies. In the study by O’Brien and colleagues (25), fifty patients with chronic lymphocytic leukemia or other mature B-cell lymphoid leukemia were treated with four weekly infusions of rituximab. The first dose was 375 mg/m2 for all patients; dose escalation began with dose 2 but was held constant for each patient. Escalated doses were from 500 to 2,250 mg/m2. Response rates of 22% to 75% were found to correlate with dose (P = 0.007). Similarly, significant dose-response relationships to rituximab have been described in clinical or murine models of non-Hodgkin lymphoma (27). The important in vivo purging role of rituximab was evaluated prospectively by Magni et al (11) in 15 patients with CD20+ mantle cell or follicular lymphoma who received two cycles of intensive sequential chemotherapy, each of which was followed by 2 doses of rituximab and a growth factor for the purpose of autologous stem cell collection. The harvested cells were negative for clonal cells in 93% of cases compared to 40% of controls (P = 0.007) who received chemotherapy alone without - or with just two doses of rituximab. Our approach using high-dose rituximab with ASCT also has been reported to significantly decrease the risk of relapse (P = 0.02) in mantle cell lymphoma patients who underwent ASCT (28). We believe that the use of high-dose rituximab in our trials as part of the stem cell collection and immediately after ASCT for just two doses could target occult residual disease in harvested stem cells and treat minimal residual disease after transplantation. There is an increasing body of evidence that high-dose rituximab may also impact OS rates after allogeneic transplantation. In a recent multi-center study involving patients with follicular lymphoma who received an allogeneic transplant (29), OS was significantly higher among patients who had a higher median serum rituximab concentration versus a lower serum concentration at day +28 after their transplant with a 2-year OS of 96% (95% CI, 0.77-0.10) vs. 67% (95% CI, 0.47-0.82), respectively, P = 0.01.
Relapsed disease was the major reason for failure in our study as in others. In our study, the encouraging survival outcomes in our study were independent of cell-of-origin or timing of relapse after induction chemotherapy. Instead, IPI > 0 immediately preceding stem cell collection and the number of chemotherapy regimens received prior to transplantation were predictive of OS, DFS and relapse. Innovative strategies such as the use of immunotherapy post-transplantation in this setting are currently undertaken at our center (30).
Secondary hematologic malignancies remain a non-negligible complication after high-dose radioimmunotherapy or high dose chemotherapy followed by ASCT, with comparable 5 years incidence ranging between 5-15%. In our report, 5 cases of myelodysplasia and 2 cases of acute myelogenous leukemia were identified at 5-year follow-up after the transplantation procedure. There was no significant difference in the rates of secondary malignancies when radioimmunotherapy was added to the conditioning.
In conclusion, this study shows that conditioning with rituximab during stem cell collection and immediately after ASCT produces high survival rates in patients with relapsed DLBCL undergoing ASCT who were previously exposed to rituximab. Our results were independent of the cell-of-origin or timing of relapse after induction chemotherapy. The addition of radioimmunotherapy to the conditioning does not provide additional benefit. Continuous randomized trials are ongoing to establish the dose of rituximab in this setting.
Supplementary Material
Translational Relevance.
The outcomes of autologous stem cell transplantation (ASCT) in patients with relapsed diffuse large B cell lymphoma (DLBCL) have not significantly changed over the last 15 years with a cure rate of less than 40%. The activated b-cell histologic subtype has been described to be associated with poor survivals.
Occult disease during stem cell collection may contribute to relapse. In a prior study, we have shown that concurrent administration of rituximab with stem cell collection for in vivo purging and immediately after autologous stem cell transplantation for two doses could induce promising results with a 2-year overall survival rate of 80% and a disease-free survival rate of 67%, significantly better than those who did not receive rituximab. The short follow-up and small numbers of patients included could not provide, however, firm conclusions. In addition, there is a paucity of information regarding the impact of this strategy in patients with activated b-cell histologic subtype and whether the addition of radio-immunotherapy could further improve the outcomes in patients with poor prognosis.
In this manuscript we report confirmatory results of 11.8-years median follow-up time on our initial trial, with additional confirmatory results from the 2 subsequent prospective trials using the same eligibility criteria with or without the addition of radio-immunotherapy to the conditioning. All patients had been previously exposed to rituximab. We also evaluated the outcomes in histologic subtypes of DLBCL and found similar survival outcomes, irrespective of their timing of relapse (< vs. > 1 year) after their initial induction chemotherapy, or type of salvage therapy pre-ASCT. The addition of radio-immunotherapy did not confer a further survival benefit. Hence the addition of rituximab pre-and post-transplantation has a clear effect on outcomes in DLBCL patients undertaking ASCT.
Acknowledgments
This work was supported by the National Health Institutes of under award number P30CA016672. In addition, trial NCT01538472 was supported by Biogen Idec.
Footnotes
Disclosures of Potential Conflicts of Interest
The Authors declare no conflict of interest.
References
- 1.Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, Siebert R, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127:2375–90. doi: 10.1182/blood-2016-01-643569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lenz G, Staudt LM. Aggressive lymphomas. N Engl J Med. 2010;362:417–29. doi: 10.1056/NEJMra0807082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Philip T, Guglielmi C, Hagenbeek A, Somers R, Van der Lelie H, Bron D, et al. Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy-sensitive non-Hodgkin’s lymphoma. N Engl J Med. 1995;333:1540–45. doi: 10.1056/NEJM199512073332305. [DOI] [PubMed] [Google Scholar]
- 4.Gisselbrecht C, Glass B, Mounier N, Singh Gill D, Linch DC, Trneny M, et al. Salvage regimens with autologous transplantation for relapsed large B-cell lymphoma in the rituximab era. J Clin Oncol. 2010;28:4184–90. doi: 10.1200/JCO.2010.28.1618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mounier N, Canals C, Gisselbrecht C, Cornelissen J, Foa R, Conde E, et al. High-dose therapy and autologous stem cell transplantation in first relapse for diffuse large B cell lymphoma in the rituximab era: an analysis based on data from the European blood and marrow transplantation registry. Biol Blood Marrow Transplant. 2012;18:788–93. doi: 10.1016/j.bbmt.2011.10.010. [DOI] [PubMed] [Google Scholar]
- 6.Alizadeh AA, Eisen MB, Davis RE, Ma C, Lossos IS, Rosenwald A, et al. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature. 2000;403:503–11. doi: 10.1038/35000501. [DOI] [PubMed] [Google Scholar]
- 7.Lenz G, Wright G, Dave SS, Xiao W, Powell J, Zhao H, et al. Stromal gene signatures in large-B-cell lymphomas. N Engl J Med. 2008;359:2313–23. doi: 10.1056/NEJMoa0802885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Thieblemont C, Briere J, Mounier N, Voelker HU, Cuccuini W, Hirchaud E, et al. The germinal center/activated b-cell subclassification has a prognostic impact for response to salvage therpay in relapsed/refractory diffuse large b-cell lymphoma: a bio-CORAL study. J Clin Oncol. 2011;29:4079–87. doi: 10.1200/JCO.2011.35.4423. [DOI] [PubMed] [Google Scholar]
- 9.Gribben JG, Freedman AS, Neuberg D, Roy DC, Blake KW, Woo SD, et al. Immunologic purging of marrow assessed by PCR before autologous bone marrow transplantation for B-cell lymphoma. N Engl J Med. 1991;325:1525–33. doi: 10.1056/NEJM199111283252201. [DOI] [PubMed] [Google Scholar]
- 10.van Besien K, Loberiza FR, Bajorunaite R, Armitage JO, Bashey A, Burns LJ, et al. Comparison of autologous and allogeneic hematopoietic stem cell transplantation for follicular lymphoma. Blood. 2003;102:3521–29. doi: 10.1182/blood-2003-04-1205. [DOI] [PubMed] [Google Scholar]
- 11.Magni M, Di Nicola M, Devizzi L, Matteucci P, Lombardi F, Gandola L, et al. Successful in vivo purging of CD34-containing peripheral blood harvests in mantle cell and indolent lymphoma: evidence for a role of both chemotherapy and rituximab infusion. Blood. 2000;96:864–69. [PubMed] [Google Scholar]
- 12.Galimberti S, Guerrini F, Morabito F, Palumbo GA, Di Raimondo F, Papineschi F, et al. Quantitative molecular evaluation in autotransplant programs for follicular lymphoma: efficacy of in vivo purging by rituximab. Bone Marrow Transplant. 2003;32:57–63. doi: 10.1038/sj.bmt.1704102. [DOI] [PubMed] [Google Scholar]
- 13.Khouri IF, Saliba RM, Hosing C, Okoroji GJ, Acholonu S, Anderlini P, et al. Concurrent administration of high-dose rituximab before and after autologous stem-cell transplantation for relapsed aggressive B-cell non-Hodgkin’s lymphomas. J Clin Oncol. 2005;23:2240–47. doi: 10.1200/JCO.2005.08.012. [DOI] [PubMed] [Google Scholar]
- 14.Nademanee A, Forman S, Molina A, Fung H, Smith D, Dagis A, et al. A phase 1/2 trial of high-dose yttrium-90 – ibritumomab tiuxetan in combination with high-dose etoposide and cyclophosphamide followed by autologous stem cell transplantation in patients with poor-risk or relapsed non-Hodgkin lymphoma. Blood. 2005;106:2896–902. doi: 10.1182/blood-2005-03-1310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Winter JN, Inwards DJ, Spies S, Wiseman G, Patton D, Erwin W, et al. Yttrium-90 ibritumomab tiuxetan doses calculated to deliver up to 15 Gy to critical organs may be safely combined with high-dose BEAM and autologous transplantation in relapsed or refractory B-cell non-Hodgkin’s lymphoma. J Clin Oncol. 2009;27:1653–59. doi: 10.1200/JCO.2008.19.2245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mei M, Wondergem MJ, Palmer JM, Shimoni A, Hasenkamp J, Tsai NC, et al. Autologous transplantation for transformed non-Hodgkin lymphoma using an yttrium-90 ibritumomab tiuxetan conditioning regimen. Biol Blood Marrow Transplant. 2014;20:2072–75. doi: 10.1016/j.bbmt.2014.07.028. [DOI] [PubMed] [Google Scholar]
- 17.Briones J, Novelli S, Garcia-Marco JA, Tomás JF, Bernal T, Grande C, et al. Autologous stem cell transplantation after conditioning with yttrium-90 ibritumomab tiuxetan plus BEAM in refractory non-Hodgkin diffuse large B-cell lymphoma: results of a prospective, multicenter, phase II clinical trial. Haematologica. 2014;99:505–10. doi: 10.3324/haematol.2013.093450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Shimoni A, Avivi I, Rowe JM, Yeshurun M, Levi I, Or R, et al. A randomized study comparing yttrium-90 ibritumomab tiuxetan (Zevalin) and high-dose BEAM chemotherapy versus BEAM alone as the conditioning regimen before autologous stem cell transplantation in patients with aggressive lymphoma. Cancer. 2012;118:4706–14. doi: 10.1002/cncr.27418. [DOI] [PubMed] [Google Scholar]
- 19.Vose JM, Carter S, Burns LJ, Ayala E, Press OW, Moskowitz CH, et al. Phase III randomized study of rituximab/carmustine, etoposide, cytarabine, and melphalan (BEAM) compared with iodine-131 tositumomab/BEAM with autologous hematopoietic cell transplantation for relapsed diffuse large B-cell lymphoma: results from the BMT C. J Clin Oncol. 2013;31:1662–68. doi: 10.1200/JCO.2012.45.9453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hans CP, Weisenburger DD, Greiner TC, Gascoyne RD, Delabie J, Ott G, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood. 2004;103:275–82. doi: 10.1182/blood-2003-05-1545. [DOI] [PubMed] [Google Scholar]
- 21.Visco C, Li Y, Xu-Monette ZY, Miranda RN, Green TM, Li Y, et al. Comprehensive gene expression profiling and immunohistochemical studies support application of immunophenotypic algorithm for molecular subtype classification in diffuse large B-cell lymphoma: a report from the international DLBCL rituximab-CHOP consortiu. Leukemia. 2012;26:2103–13. doi: 10.1038/leu.2012.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Choi WW, Weisenburger DD, Greiner TC, Piris MA, Banham AH, Delabie J, et al. A new immunostain algorithm classifies diffuse large B-cell lymphoma into molecular subtypes with high accuracy. Clin Cancer Res. 2009;15:5494–502. doi: 10.1158/1078-0432.CCR-09-0113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Cheson BD, Horning SJ, Coiffier B, Shipp MA, Fisher RI, Connors JM, et al. Report of an international workshop to standardize response criteria for non-Hodgkin’s lymphomas. NCI Sponsored International Working Group. J Clin Oncol. 1999;17:1244–53. doi: 10.1200/JCO.1999.17.4.1244. [DOI] [PubMed] [Google Scholar]
- 24.Cheson BD, Pfistner B, Juweid ME, Gascoyne RD, Specht L, Horning SJ, et al. Revised response criteria for malignant lymphoma. J Clin Oncol. 2007;25:579–86. doi: 10.1200/JCO.2006.09.2403. [DOI] [PubMed] [Google Scholar]
- 25.O’Brien SM, Kantarjian H, Thomas DA, Giles FJ, Freireich EJ, Cortes J, et al. Rituximab dose-escalation trial in chronic lymphocytic leukemia. J Clin Oncol. 2001;19:2165–70. doi: 10.1200/JCO.2001.19.8.2165. [DOI] [PubMed] [Google Scholar]
- 26.Byrd JC, Murphy T, Howard RS, Lucas MS, Goodrich A, Park K, et al. Rituximab using a thrice weekly dosing schedule in B-cell chronic lymphocytic leukemia and small lymphocytic lymphoma demonstrates clinical activity and acceptable toxicity. J Clin Oncol. 2001;19:2153–64. doi: 10.1200/JCO.2001.19.8.2153. [DOI] [PubMed] [Google Scholar]
- 27.Daydé D, Ternant D, Ohresser M, Lerondel S, Pesnel S, Watier H, et al. Tumor burden influences exposure and response to rituximab: pharmacokinetic-pharmacodynamic modeling using a syngeneic bioluminescent murine model expressing human CD20. Blood. 2009;113:3765–72. doi: 10.1182/blood-2008-08-175125. [DOI] [PubMed] [Google Scholar]
- 28.Chakhachiro ZI, Saliba RM, Okoroji G-J, Korbling M, Alousi AM, Betul O, et al. Cytarabine, Ki-67, and SOX11 in patients with mantle cell lymphoma receiving rituximab-containing autologous stem cell transplantation during first remission. Cancer. 2013;119:3318–25. doi: 10.1002/cncr.28219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Laport GG, Wu J, Logan B, Bachanova V, Hosing C, Fenske T, et al. Reduced-intensity conditioning with fludarabine, cyclophosphamide, and high-dose rituximab for allogeneic hematopoietic cell transplantation for follicular lymphoma: a phase two multicenter trial from the Blood and Marrow Transplant Clinical Trials Network. Biol Blood Marrow Transplant. 2016;22:1440–14. doi: 10.1016/j.bbmt.2016.04.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Khouri IF, Fernandez Curbelo I, Turturro F, Jabbour E, Milton DR, Bassett RL, et al. Ipilimumab plus lenalidomide after allogeneic and autologous stem cell transplantation for patients with lymphoid malignancies. Clin Cancer Res. 2017 Dec 15; doi: 10.1158/1078-0432.CCR-17-2777. [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.