

Psoralen plus ultraviolet A (PUVA) photochemotherapy combines the use of psoralen and long-wave ultraviolet A (UVA) radiation. The phototherapeutic effects of PUVA result from photochemical reactions. PUVA therapy can be administered in various methods such as conventional UV chambers, psoralen with sunlight as source of UV light PUVASOL, bath PUVA, bath suit PUVA, soak PUVA, and turban PUVA. The advantage of using topical psoralen is that it avoids the adverse effects associated with the oral PUVA therapy and is being increasingly used in the treatment of psoriasis. However, it is known to cause increased phototoxicity, and in conditions like vitiligo, the spotty repigmentation is not cosmetically acceptable. Psoralen bath plus UVA therapy is known as bath PUVA therapy. Bath PUVA treatment for psoriasis was first reported by Fischer and Alsins in 1976. Bath PUVA is administered by mixing 37.5 mL of 1% 8-methoxypsoralen in 100 Lof water to obtain a concentration of 3.75 mg/L.[1] In bath suit PUVA, bathing suit of flannel material (stitched to suit the patient) is dipped in this solution for 5 min and worn for 15 min with a raincoat over it to prevent evaporation of the solution, and the patient is then immediately exposed to UVA in a whole-body phototherapy chamber. Bath PUVA needs plenty of water. Bath tub is not easily available and bath suit needs special suit, and treatment is cumbersome. We planned to modify the therapy by mixing psoralen with cleansing lotion and coined it as SOAP PUVA. The choice is due to the solubility factor as 8-MOP being insoluble in water.
We reported a novel method of delivering 8-MOP uniformly all over the skin within a short time and on subsequent exposure to UV light. Because8-MOP was not soluble in water, we tried to dissolve it in commercially available moisturizing lotion (cetaphil) and synthetic detergent (cetaphil cleansing lotion). As it dissolved well in cleansing lotion, we decided to use it for our study [Figure 1]. As the method was new, we initially tried to standardize the procedure and determine the minimal pigmentation dose (MPD). The project was done in a single healthy subject with no existing dermatological disease requiring phototherapy. We started by using 1:100 dilution of methoxsalen that was prepared by mixing 0.1 mL of methoxsalen with 9.9 mL of cleansing lotion. The mixture was applied over the back [Figure 2]. The paste was left over for 5 min after which it was wiped with water-soaked gauze. The template cloth was worn along with goggles to protect the eyes. The area was exposed to UVA light (0–3J) with 0.5-J increments. The plan was to observe for MPD after 48 h and delayed pigmentation upto 7 days. No erythema and pigmentation was observed upto 7 days. We increased the concentration to 1:80, and the same procedure was repeated with no erythema or pigmentation. The concentration was increased to 1:60 and the same procedure was repeated. Erythema was observed at 2.5 J after 48 h [Figure 3] and pigmentation was observed after 5 days.
Figure 1.
Psoralen completely soluble in cleansing lotion
Figure 2.

Psoralen and cleansing lotion mixture applied over the back
Figure 3.
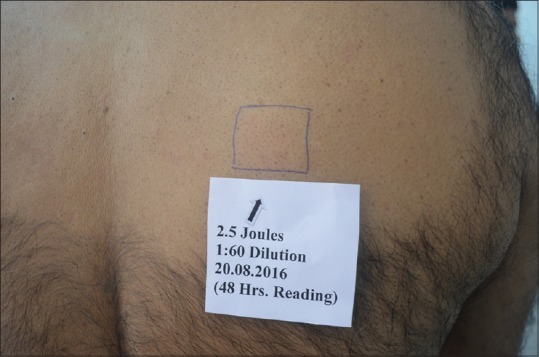
Erythema observed after 48 h at 2.5 J
Oral PUVASOL is effective but is time-consuming because the exposure to UV light occurs after 2 h and the intensity of sunlight varies. It also becomes difficult for children and working women. To overcome these issues bath PUVA was introduced, but it requires consumption of a large quantity of water. Pai and Srinivas introduced bathsuit tPUVA [2] to overcome this but the suit had to be worn for 15 min and was practically difficult.
The main purpose of this study was to identify the method and use it with exposure to sunlight. The plan was to increase the concentration of psoralen rather increase the exposure time because we wanted to deliver it in a shorter period and the irradiance of sunlight was much lower than the irradiance of UV light in artificial chambers. The limitation was that it was done on a single subject, and the results might have varied. We plan to conduct further studies on a larger scale to determine the ideal dilution and use it as a viable alternative for delivering PUVA therapy.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Pai SB, Shetty S. Guidelines for bath PUVA, bathing suit PUVA and soak PUVA. Indian J Dermatol Venereol Leprol. 2015;81:559–67. doi: 10.4103/0378-6323.168336. [DOI] [PubMed] [Google Scholar]
- 2.Pai S, Srinivas CR. Bath suit delivery of 8-MOP for PUVA therapy. Indian J Dermatol Venereol Leprol. 1992;58:142. [Google Scholar]