

Sir,
An 18-year-old girl presented to us with fleshy growths in her mouth and white and black pigmented lesions on her skin. She was born of nonconsanguineous marriage, was normal at birth, and her mother gave no history of miscarriages. The skin lesions appeared a few months after birth and the fleshy growths began when she was 7 years old.
Cutaneous examination revealed multiple hyper and depigmented macules and atrophic patches on her scalp, face, trunk, and extremities following the lines of Blaschko [Figure 1]. The atrophic lesions of the forearm and groin had multiple small soft swellings suggestive of subcutaneous fat herniations. She had multiple fleshy papillomatous growths on her tongue, buccal mucosa, lips, left nasal cavity, both palpebral conjunctivae [Figure 2], left auditory canal, anus, and genitalia. She had asymmetry of the face, wide nose, low set ears, left corneal opacity, oligodontia and linear enamel defects [Figure 3], hypoplastic left index finger and right little finger [Figure 4] linear dystrophy of nails, hypohidrosis, umbilical hernia, and absent pubic and axillary hair.
Figure 1.

Hyperpigmented macules and depigmented atrophic macules following lines of blaschko on the back
Figure 2.

Fleshy papillomas on upper lip, palate, tongue, and left nasal cavity
Figure 3.

Oligodontia and linear enamel defects of teeth; note papilloma of the upper lip and atrophic macules on the chin
Figure 4.

Hypoplastic left index finger and right little finger; note linear dystrophy in the nail of the left ring finger
Her routine blood investigations and ultrasound abdomen were normal. X-ray of the left hand showed hypoplasia of the index finger. Histopathology of an atrophic skin lesion showed lobules of fat in the reticular dermis with haphazardly arranged collagen bundles [Figure 5]. Histopathological examination of the mass in left ear revealed squamous cell papilloma. Based on the clinical features and histopathology, a diagnosis of focal dermal hypoplasia (Goltz syndrome) was made. She was counseled about the disease and was referred to ophthalmologist and ENT surgeon for excision of papillomas.
Figure 5.
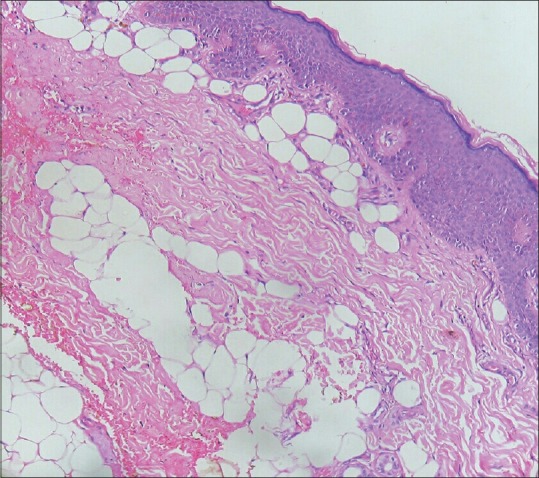
Accumulation of fat globules in reticular dermis with haphazardly arranged collagen bundles [H and E, ×20]
Focal dermal hypoplasia is a rare genetic disorder characterized by hypoplasia and dysplasia of mesoectodermal structures including skin, skeletal system, eyes, teeth, and soft tissues.[1] It is a rare disorder with approximately 300 cases reported worldwide.[2] The cause is attributed to the presence of a pathogenic variant of PORCN gene on chromosome Xp11.23, which is important in wnt signaling pathway and embryonic tissue development.[2,3] It can be sporadic or X-linked dominant. Live born affected males exhibit somatic mosaicism.[2] Prenatal diagnosis can be done in high-risk pregnancies by molecular analysis of DNA from fetal blood or amniotic fluid.[4]
The cutaneous features of Goltz syndrome are atrophic, white patches, linear or reticular hyper or hypopigmented macules, fat herniations, telangiectasia, and mucocutaneous papillomas.[5] Other cutaneous features include hyper or hypohidrosis, brittle scalp hair, lack of hair on scalp and pubis, as well as absent, dystrophic, and grooved nails.[5] Skeletal defects are seen in 60–70% of the patients.[3] It includes microcephaly, kyphosis, scoliosis, asymmetry of the face, trunk or extremities, hypoplasia of digits, syndactyly and polydactyly, lobster claw defect, and osteopathia striata.[3,5] Ocular anomalies include chorioretinal and iris colobomas, micro or anophthalmia, cataracts, conjunctival and eyelid papillomas, strabismus, nystagmus, corneal opacities, and epiphora.[5] Dental anomalies found are vertical enamel grooving, agenesis, irregular spacing, and malocclusion of teeth.[5] Other findings include diaphragmatic hernia, absent or horse-shoe kidney, atrial septal defect, truncus arteriosus, and mental retardation.[3,6]
Histopathology of atrophic skin lesion shows thinning of dermis with a decrease in collagen fibers and accumulation of adipocytes in the dermis. Ishii et al. proposed that the presence of adipocytes in dermis may be due to dysplasia rather than hypoplasia of dermis.[7]
Our patient had typical features of Goltz syndrome, among which the most striking was the presence of extensive mucocutaneous papillomas.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that name and initial will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Goltz RW. Focal dermal hypoplasia syndrome: An update. Arch Dermatol. 1992;128:1108–11. [PubMed] [Google Scholar]
- 2.Bostwick B, Van den Veyver IB, Sutton VR. Focal Dermal Hypoplasia. 2008 May 15 [Last updated on 2016 Jul 21] In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Bean LJH, Medford HC, et al., editors. GeneReviews® [Internet] Seattle (WA): University of Washington, Seattle; 1993-2017. [Last accessed on 2017 Aug 29]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1543. [Google Scholar]
- 3.Srinivas SM, Hiremagalore R. Focal dermal hypoplasia: A rare case report. Indian J Dermatol. 2015;60:106. doi: 10.4103/0019-5154.147876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mary L, Scheidecker S, Kohler M, Lombardi MP, Delezoide AL, Auberger E, et al. Prenatal diagnosis of focal dermal hypoplasia: Report of three fetuses and review of the literature. Am J Med Genet Part A. 2017;173(A):479–86. doi: 10.1002/ajmg.a.37974. [DOI] [PubMed] [Google Scholar]
- 5.Goltz RW, Henderson RR, Hitch JM, Ott JE. Focal dermal hypoplasia syndrome. A review of the literature and report of two cases. Arch Derm. 1970;101:1–11. doi: 10.1001/archderm.101.1.1. [DOI] [PubMed] [Google Scholar]
- 6.Riyaz N, Riyaz A, Chandran R, Rakesh SV. Focal dermal hypoplasia (Goltz syndrome) Indian J Dermatol Venereol Leprol. 2005;71:279–81. doi: 10.4103/0378-6323.16624. [DOI] [PubMed] [Google Scholar]
- 7.Ishii N, Baba N, Anaizuka I, Nakajima H, Ono S, Amemiya F. Histopathological study of focal dermal hypoplasia (Goltz syndrome) Clin Exp Dermatol. 1992;17:24–6. doi: 10.1111/j.1365-2230.1992.tb02527.x. [DOI] [PubMed] [Google Scholar]