

A 57-year-old female presented with multiple asymptomatic firm, skin-colored, dome-shaped papules distributed primarily along the nasolabial folds, medial part of the eyebrows, forehead and dorsum of nose [Figure 1]. She first noticed the lesions during adolescence, after which they progressively increased in number.
Figure 1.

Dome-shaped papules distributed primarily along the nasolabial folds, nasal dorsum, medial part of eyebrows, and forehead
Dermoscopy (DermLite II hybrid m; 3Gen; polarized mode, 10× magnification) of papules revealed arborizing vessels, multiple milia-like cysts, and rosettes amidst a whitish background [Figure 2a–c]. With the clinical possibility of trichoepithelioma, biopsy was done which revealed islands and nests of basaloid cells along with multiple keratin cysts. Focal areas showed periadenexal lymphocytic infiltrate [Figure 3a and b].
Figure 2.
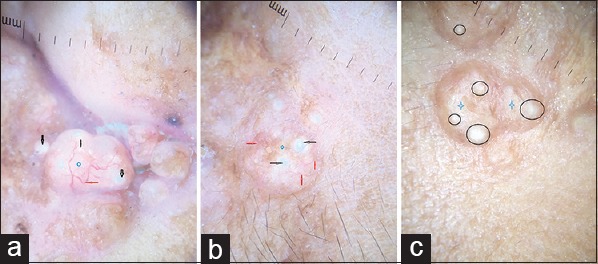
(a) Dermoscopy of trichoepithelioma shows multiple arborizing vessels (red arrows), milia-like cysts (black arrow) over a whitish background (blue diamond) (polarized, ×10). (b) Multiple branching vessels (red arrow) overlying a whitish background (diamond) with milia-like cysts (black arrow) (polarized, ×10). (c) Multiple milia-like cysts (black circles) overlying a whitish background (star) (nonpolarized ×10)
Figure 3.
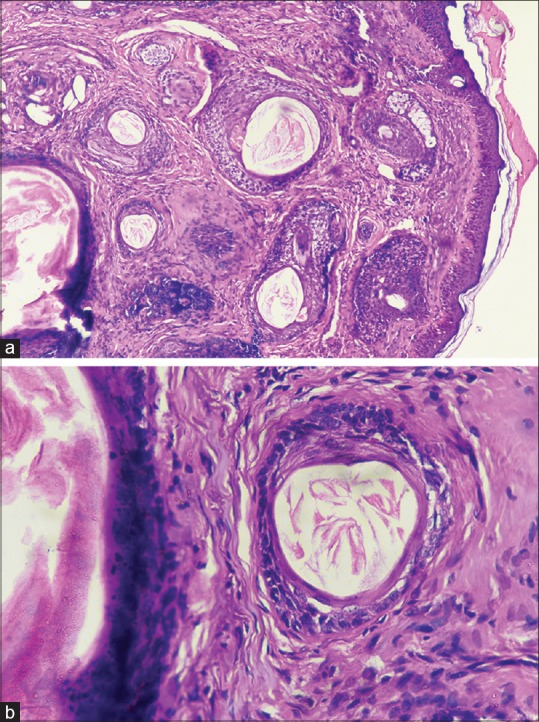
(a) Islands and nest of basaloid cells along with multiple keratin cysts (H and E, ×10). (b) Islands and nest of basaloid cells (H and E, ×40)
Trichoepithelioma is a benign neoplasm regarded as poorly differentiated hamartoma of the hair germ cells. It is divided into multiple familial, solitary, and desmoplastic subtypes. Malignant transformation to basal cell carcinoma (BCC) is rare and occurs late in the course of the disease. Dermoscopy findings in our case are in line with those previously described by Navarrete-Dechent et al. in their study.[1]
Although the clinical diagnosis was straight forward in our case, dermoscopy, being a non invasive procedure, is a useful tool for confirming the clinical diagnosis subverting the need for an invasive procedure such as biopsy. This is especially useful as many times patients are unwilling to undergo biopsy because of cosmetic concerns when lesions are on the face. Here, we wish to highlight the importance of dermoscopy in the diagnosis of trichoepithelioma. The dermsocopic finding of various differentials of trichoepithelioma are summarized in Table 1.
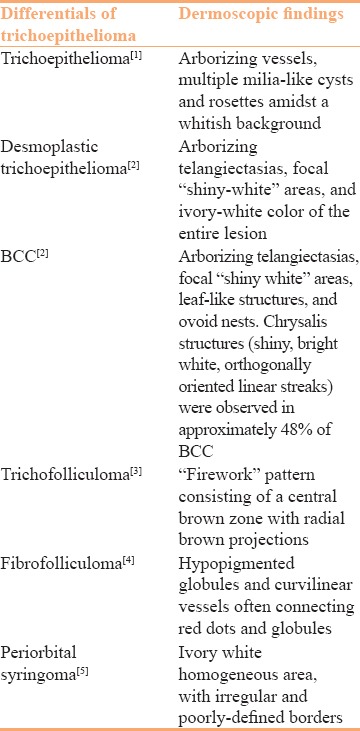
Table 1.
Dermoscopic findings of differentials of trichoepithelioma
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.5
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Dechent CV, Shirin B, Marghoob AA, Sergio G, Daniel M. Multiple familial trichoepithelioma: Confirmation via dermoscopy. Dermatol Pract Concept. 2016;6:10. doi: 10.5826/dpc.0603a10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Liebman TN, Jaimes-Lopez N, Balagula Y, Rabinovitz HS, Wang SQ, Dusza SW, et al. Dermoscopic features of basal cell carcinomas: Differences in appearance under non-polarized and polarized light. Dermatol Surg. 2012;38:392–9. doi: 10.1111/j.1524-4725.2011.02205.x. [DOI] [PubMed] [Google Scholar]
- 3.Panasiti V, Roberti V, Lieto P, Visconti B, Calvieri S, Perrella E. The “firework” pattern in dermoscopy. Int J Dermatol. 2013;52:1158–9. doi: 10.1111/j.1365-4632.2011.05122.x. [DOI] [PubMed] [Google Scholar]
- 4.Maressa CC, Euphemia W. Mu, Shane AM, David P, Iris K. Dermoscopic features of a solitary fibrofolliculoma on the left cheek. J Am Acad Dermatol. 2017;76:S8–9. doi: 10.1016/j.jaad.2016.03.041. [DOI] [PubMed] [Google Scholar]
- 5.Rodríguez SS, Ciancio RM, Cabo H. Dermoscopic study of periorbital syringoma. Med Cutan Iber Lat Am. 2015;43 [Google Scholar]