

Abstract
Background and Aims
Peripheral nerve injury is one of the frequent complaints which is seen in the outpatient clinic of our medical institute. In previous studies we have reported on the benefits of low level laser therapy (LLLT) for central nerve system disorders, namely cerebrovascular accidents and cerebral palsy. The present study is a report on our experience of the effects of LLLT for peripheral nerve palsy.
Materials and Methods
Over the past 5 years, 13 subjects visited the out-patient clinic with the chief complaint of radial nerve palsy caused by compression of the nerve through with abnormal positioning, and sleeping posture at night. The patients were treated with LLLT. A 1000 mW semi-conductor laser device was used, delivering 830 nm in continuous wave at a dose of 20.1 J/cm2 /point, and five points were treated per session (i.e., 1 treatment) twice a week for 3 months (total 24 treatments). In 6 patients LLLT was combined with brace therapy.
Results
Modified Daniels' manual muscle testing was used to determine the effects of LLLT for the muscle power of the extensor carpi radialis, and on completing the treatment regimen excellent improvement was observed in 9 cases out of 13. Combination treatment (laser therapy with bracing) resulted in 4 excellent cases out of 6 cases. Discussions with the patients clarified that it was important for them to learn how to avoid the particular posture that could cause them radial nerve palsy in daily life in order to have continuous benefits from the treatment.
Conclusion
The present study demonstrated that LLLT was an effective form of treatment for radial nerve palsy. In addition, patients were advised to avoid any incorrect posture which might induce radial nerve palsy.
Keywords: Low Level Laser Therapy, Peripheral nerve injury, Radial nerve palsy, Posture education
Introduction
Since the middle of the 20th century, Low level laser therapy ( LLLT) has become popular and has been approved for clinical usage. LLLT with lasers such as the gallium aluminium arsenide (GaAlAs) or in earlier times helium-neon (HeNe), whose wavelengths fall in the waveband between 600 nm-984 nm, is regularly used for a variety of disorders in physical therapy.
LLLT has been shown to affect many cellular processes, although the mechanisms have not been fully defined. In previous studies our group has reported the benefits of LLLT for central nerve system disorders, namely cerebrovascular accidents and cerebral palsy. 1,2) Many authors have additionally reported significant effects of LLLT in acute and chronic painful and paralytic conditions such as rheumatoid arthritis, osteoarthritis, fibromyalgia, and the peripheral nerve neuropathies. 3–7)
Radial nerve palsy, which can result from a complex humerus fracture, direct nerve trauma, compressive neuropathies or neuritis, has been reported widely in the literature, with some controversy regarding its diagnosis and treatment. 8) The appropriate management of any case of radial nerve palsy depends primarily on an accurate determination of its cause, severity, duration and the level of involvement. In this article we report on our experience of treating patients with the axonotmesis type of the Seddon classification of t radial nerve palsy.
Subjects and Methods
1: Subjects
Thirteen patients (8 males and 5 females) between the age of 6 and 73 years with an average age of 46.4 yr took part in this study. All subjects were outpatients who visited the rehabilitation department of our hospital between April, 2012 and March, 2017 (Table 1). All patients visited the out-patient clinic within one week after onset of the complaint. They all had a definitive diagnosis of radial nerve palsy (axonotmesis type according to the Seddon classification, without surgical indication Table 2). Diagnosis was based on physical symptoms: complaints caused by trauma, reduced muscle power of the extensor carpi radialis muscle, sensory disturbance, positive Tinel's sign, and dropped hand deformity.
Table 1: Outline of Cases.
| case | age | sex | nerve | irradiation time | treatment of number of times | MMT*: ECR** |
||
|---|---|---|---|---|---|---|---|---|
| before | after | evaluation# | ||||||
| 1 | 73 | M | R-radial | 5 min | 24 times | 1 | 7 | E |
| 2 | 47 | M | L-radial | 5 | 24 | 2 | 8 | E |
| 3 | 70 | M | L-radial | 5 | 24 | 1 | 9 | E |
| 4 | 25 | F | R-radial | 5 | 24 | 1 | 9 | E*** |
| 5 | 26 | M | R-radial | 5 | 24 | 2 | 9 | E |
| 6 | 47 | M | R-radial | 5 | 24 | 1 | 2 | N |
| 7 | 44 | F | R-radial | 5 | 24 | 1 | 4 | F |
| 8 | 6 | M | L-radial | 5 | 24 | 1 | 9 | E *** |
| 9 | 48 | F | L-radial | 5 | 24 | 1 | 9 | E *** |
| 10 | 50 | M | L-radial | 5 | 24 | 1 | 9 | E *** |
| 11 | 48 | F | R-radial | 5 | 24 | 1 | 9 | E |
| 12 | 73 | F | L-radial | 5 | 24 | 1 | 2 | N *** |
| 13 | 46 | M | L-radial | 5 | 24 | 2 | 5 | F *** |
MMT (Manual Muscle Testing): Modified from Daniels' method
ECR: Extensor Carpi Radialis muscle
: Bracing
- Excellent (E) :7–9
- Good (G) :5–6
- Fair (F) :3–4
- No change (N) :1–2
- Worse/Side effect: --
Table 2: Seddon Classification (Seddon H: Three types of nerve injury. Brain 66:237‧288, 1943:).
Type 1 Neurapraxia:
|
Type 2 Axonotmesis
|
Type 3 Neurotmesis
|
2: Methods
We used a 1000 mW semiconductor laser device, the MDL 2001 (Matsushita Electric Corporation, Tokyo, Japan), delivering 830 nm in continuous wave for treatment of the radial nerve palsy patients. Each point was irradiated with a dose of 20.1 J/cm2 with an exposure time of 30 s (Table 3). Five points were irradiated (Figure 1) per session (comprising 1 treatment) twice a week for 3 months (total 24 treatment sessions). We excluded those patients who had used or were using steroid therapy to ascertain better the effect of the LLLT intervention. In 6 patients LLLT was combined with brace therapy. The study was conducted under the principles of the Declaration of Helsinki (2011). The trial was conducted with the approval of the Ethics Committee of the Toho University School of Medicine, Institutional Review Board (IRB). The purpose and potential outcomes of the trial were explained to all participants, and they gave written informed consent to participate the study.
Table 3: Low Level Laser Therapy Device Specifications.
| Laser Element | Semiconductor Laser Diode Ga-Al-As: Gallium Aluminium Arsenide | |
| Model | MDL-2001 model | |
| Manufacturer | Matsushita Electric Corporation, Tokyo, Japan | |
| Wavelength | 830 ± 15 nm | |
| Output | 1000 mW ± 20% | |
| Mode | Continuous wave mode Contact mode with positive pressure | |
| Irradiated area | diameter in 14 mm: actual area in 1.5 cm2 | |
| Irrariation time | 30 sec | |
| Energy density | 20.1 J/cm2 | |
| Power Supply | 100 VAC, 50–60 Hz |
Figure 1:
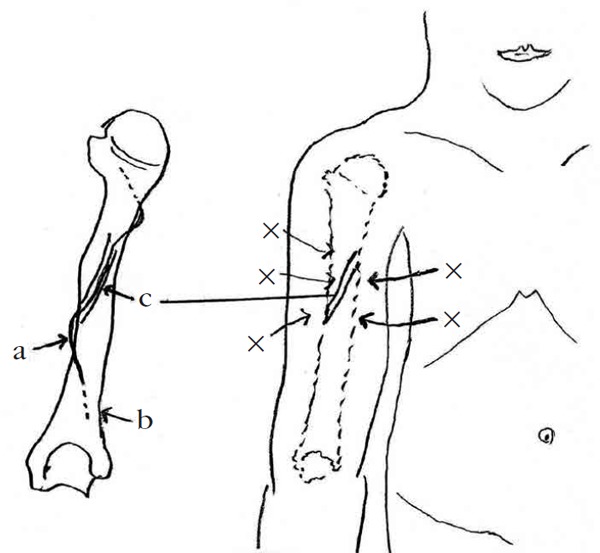
- a: radial nerve
- b: humerus
- c: spiral groove of humerus
- x: irradiation-points-
Evaluation of Manual Muscle Testing (MMT) of the extensor carpi radials muscle:
The muscle power was assessed after treatment sessions with an MMT scale (Table 4-a,b). After treatment, the muscle power of the extensor carpi radialis was measured to assess any changes in Daniels' manual muscle testing results.
Table 4-a: MMT: Manual Muscle Testing (Daniels' Grading System).
| 0: | no contraction |
| 1: | slight contraction |
| 2 | completes range of motion with gravity eliminated |
| 3: | completes range of motion against gravity |
| 4: | completes range of motion against gravity with some resistance at end range |
| 5: | completes range of motion against gravity with full resistance at end range |
Table 4-b: MMT (Manual Muscle Testing).
| Daniels' Method | Modified from Daniels' Method |
|---|---|
| 0 | 1 |
| 1 | 2 |
| 2 | 3 |
| 3-: between 2 and 3 | 4 |
| 3: | 5 |
| 3+: between 3 and 4 | 6 |
| 4: | 7 |
| 4+: between 4 and 5 | 8 |
| 5: | 9 |
Lifestyle education for the patients:
In addition to the LLLT sessions, patients were advised to continue their normal living style. We give them written instructions containing specific advice on maintaining a good posture to avoid any trigger positions associated with radial nerve palsy caused by nerve compression through abnormal positioning, and bad sleeping posture at night.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics, version 24, IBM Company. The Wilcoxon signed rank test was applied to comparison of MMT evaluation scores between before and after LLLT. The Mann-Whitney U-test was applied to comparison of increments in the MMT score between the bracing and non-bracing groups. Significance level was set at 0.05.
Results
MMT Evaluation:
The muscle power of the extensor carpi radialis at the first visit and at the final visit are shown in the right-hand columns of Table 1, together with the classification of efficacy as follows: a score of 7–9, excellent (E); 5–6, good (G); 3–4, fair (F); and 1–2, no change (N). A negative value was used to denote exacerbation of the presence of adverse side effects. Nine cases of the 13 scored E, 0 cases scored G, and 2 each scored F and N. Zero cases showed any adverse events or exacerbation. This showed that LLLT was safe and effective in 69% of our 13 patients. The MMT score after LLLT was significantly higher than the score before LLLT (p = 0.0015). No significant difference was detected in the MMT score increment between the bracing and the non-bracing groups (p = 0.534).
Patient Lifestyle Guidance:
Patients were advised to avoid any posture which could induce radial nerve palsy by compression, and we advised the patients how to avoid incorrect positions in their Activities of Daily Living (ADL) and bad sleeping posture at night, as already mentioned in the Subjects and Methods section. After discussions with the patients, the lifestyle education was well understood in all cases, and the appropriate advice that was given. However, in the score-sheet filled out by patients after the treatment, there were many cases who did not precisely follow the lifestyle education; therefore, statistical analysis was not performed with regard to this parameter.
Discussion
Peripheral nerve injury is categorized according to the Seddon classification (three types per Table 2) based on the extent of damage to the nerve and surrounding connective tissues (endoneurial sheath), as follows. Type 1: Neurapraxia is an injury to a nerve which has interrupted conduction causing temporary paralysis and which is followed by a complete and rapid recovery, although any marked axonal degeneration can be associated with poor results. Type 2: Axonotmesis is axonal nerve damage (Wallerian degeneration) without the surrounding endoneurial sheath being severed. Type 3: Neurotmesis is a crushed peripheral nerve with complete severance of the axon and the endoneurial sheath.
The radial nerve is more commonly injured at a more proximal level on the arm where it spirals around the humerus. Injury at the spiral groove of the humerus is most commonly associated with humerus fracture, plus direct compression may occur with abnormal positioning during the day, and an abnormal sleeping posture.
The authors' investigations have shown that LLLT has a positive influence on nerve regeneration in human subjects. LLLT is widely employed in the treatment of a number of pathological conditions among musculoskeletal disorders including peripheral neuropathies. The fact that treatment of damaged nerves with appropriate LLLT regimens somehow restores poorly functioning or compromised nerves seems to be well accepted. 9) Both experimental and practical clinical evidence has shown that the low incident levels of laser energy at appropriate wavelengths and parameters can have a positive effect on regeneration of injured nerves, which is encouraging in its use. 8, 9).
A growing body of evidence exists that LLLT may stimulate nerve regeneration: this hypothesis was tested in rats, 10, 11) and has facilitated nerve regeneration in the experimental 12) and clinical studies. 9, 11) Many evidence lines have shown that peripheral nerve regeneration may be accelerated by physical agents, such as radiofrequency (RF) treatment, bracing, and ultrasound. LLLT has also been studied with regard to its potential by its positive role in peripheral nerve regeneration 12–16). However, some authors did not find any nerve conduction change in human beings or animals. 17, 18) This finding points to the importance of the use of appropriate wavelengths, intensities (irradiance or power density) and fluences when treating compromised nerves.
Generally, we treat cases of radial nerve palsy with medication, bracing, education in life style, physical therapy, and surgery in some cases. LLLT is simple and easy to administer without any side effects. Amongst others, Rochkind and Oliveira have reported that the study of peripheral nerve injuries has expanded the understanding of the processes and factors that contribute to nerve regeneration, improvement of biological conduction and the application of LLLT, perhaps in combination with the administration of growth-promoting molecules is proposed. 9, 14, 19) Although the potential mechanism of action may be somewhat speculative, the authors can surely conclude that the well-proven action of near-IR LLLT on the improvement of blood flow and neovascularization of devascularized neural tissue has a strong influence on nerve regeneration.
Conclusion
Our results in the present study confirmed that LLLT was an effective treatment for radial nerve palsy caused by compression with abnormal posture both during activities of daily living, and while sleeping. To obtain the maximum benefit from LLLT intervention, it is important to educate patients, and to reinforce good compliance with all advice given.
References
- 1: Kazuaki Tsuchiya, Takashi Harada, Toshio Ohshiro. (2008). Low level laser therapy(LLLT) for cerebral palsy. Laser Therapy. 17:29-33. [Google Scholar]
- 2: Nobuyuki Ushigome, Takashi Harada, Ikuko Ohkuni, Toshio Ohshiro. (2008) Low level laser therapy(LLLT) on spasticity caused by cerebral vascular accidents(CVAS). Laser Therapy. 17:95-99. [Google Scholar]
- 3: Kau T. (1989) Photobiology of Low-power Laser Effects. Health Physics. 56:691-704. [DOI] [PubMed] [Google Scholar]
- 4: Ozdemir F, Birtane M, Kokino S. (2001) The clinical efficacy of low power laser therapy on pain and function in cervical osteoarthritis. Clin Rheumatol. 20:181-184. [DOI] [PubMed] [Google Scholar]
- 5: Gur A, Karakoc M, Nas K. (2002). Efficacy of low power laser therapy in fibromyalgia. Lasers Med Sci. 17:57-61. [DOI] [PubMed] [Google Scholar]
- 6: Becckerman H, de Bie RA, Bouter LM. (1992). The efficacy of laser therapy for musculoskeletal and skin disorders: A criteria-based meta-analysis of randomized clinical trials. Phys Ther. 72:483-491. [DOI] [PubMed] [Google Scholar]
- 7: Masakado Y, Kawakami M, Suzuki K, Abe L, Ota T, Kimura A. (2008). Clinical neurophysiology in the diagnosis of peroneal nerve palsy. Keio J Med. 57:84-89. [DOI] [PubMed] [Google Scholar]
- 8: Gerd Bodner, Wolfgang Buchberger, Michael Schocke. (2001). Radial Nerve Palsy Associated with Humeral Fracture. Radiology 219:811-816. [DOI] [PubMed] [Google Scholar]
- 9: Rochkind S. Phototherapy in peripheral nerve injury for muscle preservation and nerve regeneration. Photomed Laser Surg. 2009; 27: 219-220. [DOI] [PubMed] [Google Scholar]
- 10: Chen YS, Hsu SF, Chiu CW, Lin JG, Chen CT, Yao CH. (2005). Effect of low-power pulsed laser on peripheral nerve regeneration in rats. Microsurgery. 25:83-89. [DOI] [PubMed] [Google Scholar]
- 11: De Medinaceli L, Derenzo E, Wyatt R. (1984). Rat sciatic function index data management system digitized input. Comput Biomed Res. 17:185-192. [DOI] [PubMed] [Google Scholar]
- 12: Basford JR, Hallman HO, Matsumoto JY, Moyer SK, Buss JM, Baxter GD. (1993). Effects of 830nm continuous wave laser diode irradiation on median nerve function in normal subjects. Lasers Surg Med. 13:597-604. [DOI] [PubMed] [Google Scholar]
- 13: Bagis S, Comelekoglu U, Sahin G, Buyukaklli B. (2002). Acute electrophysiologic effect of pulsed gallium-arsenide low energy laser irradiation on configuration of compound nerve action potential and nerve excitability. Lasers Sur Med. 30:376-380. [DOI] [PubMed] [Google Scholar]
- 14: De Medinaceli L, Derenzo E, Wyatt R. (1984). Rat sciatic function index data management system digitized input. Comput Biomed Res. 17:185-192. [DOI] [PubMed] [Google Scholar]
- 15: Oliveira EF, Mazzer N, Barbieri CH, Selli M. (2001). Correlation between functional index and morphometry to evaluate recovery of the rat sciatic nerve following crush injury: experimental study. J Recnstr Microsurg. 17:60-75. [DOI] [PubMed] [Google Scholar]
- 16: Nissan M, Rochkind S, Razon N, Bartal A. (1986). He-Ne Laser irradiation delivered transcutaneously: its effect on the sciatic nerve of rats. Lasers Surg Med. 6:435-438. [DOI] [PubMed] [Google Scholar]
- 17: Bagis S, Comelekoglu U, Coskun B, Milcan A, Buyukaklli B, Sahin G. (2003). No effect of GA-AS (904nm)laser irradiation on the intact skin of the injured rat sciatic nerve. Lasers Med Sci. 18:83-88. [DOI] [PubMed] [Google Scholar]
- 18: Wu W, Ponnudural R, Pott CB. (1987). Failure to confirm light-evoked response of peripheral nerve to low power helium-neon laser light stimulus. Brain Res. 401:407-408. [DOI] [PubMed] [Google Scholar]
- 19: Rochkind S. (2009). Phototherapy in peripheral nerve regeneration: From basic science to clinical study. Neurosurg Focus.; 26: E8. [DOI] [PubMed] [Google Scholar]