

Introduction
Procedural full metal jacket (FMJ) results in an increasing number of high-risk ‘stent-loaded’ patients who are referred to cardiac surgeon and complete revascularization cannot be achieved with the conventional technique 1,2. The following report describes the technique used to allow en-block long-segment stent removal by coronary endarterectomy (CE) and left anterior descending (LAD) repair with left internal thoracic artery (LITA) graft.
CE consists in opening LAD in its middle portion. After that a proper plane has been found, a long arteriotomy is performed. Under direct vision and avoiding traction, the whole atherosclerotic core and the stents are dissected and removed en-block. The distal intima is tacked using 7/0 polypropylene suture.
Case 1
A 52-year-old male. Admitted for acute coronary syndrome because of three-vessel disease with a FMJ–LAD proximally occluded, with 50% of ejection fraction. Percutaneous coronary intervention allowed only a partial LAD reperfusion and patient was referred to surgery. The other three target vessels were grafted and the CE was performed (Fig. 1a). The LAD opening, 11 cm long, was repaired with a tailored on-lay vein patch and a pedicle LITA was anastomosed onto it. Postoperative course was uneventful and the patient was discharged on oral anticoagulation therapy. Patency of the LAD bypass graft was showed on coronary computed tomography angiography control, 6 months later (Fig. 1b).
Fig. 1.
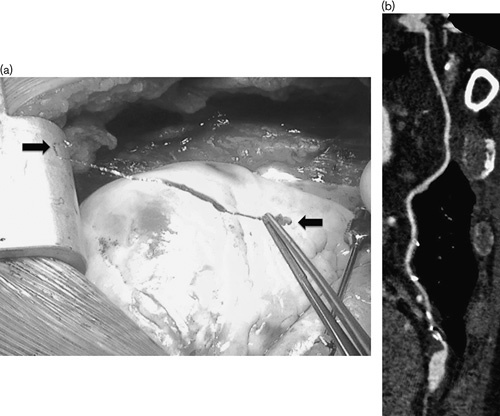
(a) Intraoperative photograph of endarterectomy. (b) Postoperative coronary computed tomography angiography of left internal thoracic artery anastomosed onto a vein hood left anterior descending repaired. Arrow showing FMJ stent.
Case 2
A 54-year-old male. Admitted for acute coronary syndrome because of three-vessel disease with a FMJ–LAD proximally occluded and ejection fraction of 45%. The patient was referred to surgery after ineffective several attempts of percutaneous coronary intervention. The other two target vessels were grafted and the CE on LAD was performed. The LAD opening, 4.5 cm long, was repaired using a skeletonized LITA as on-lay patch. Postoperative course was uneventful and the patient was discharged on dual antiplatelet, after coronary computed tomography angiography control that showed patency of the LAD bypass graft (Fig. 2a). Six months later, due to onset of acute chest pain a coronary angiography was performed showing subocclusion of right coronary artery graft, percutaneously treated, whereas the LITA–LAD graft was patent (Fig. 2b).
Fig. 2.

(a) Postoperative coronary computed tomography angiography of left internal thoracic artery to left anterior descending artery on-lay patch repair. (b) Postoperative angiography showing patency of left internal thoracic artery to left anterior descending on-lay patch.
Discussion
LAD is the major revascularization site in coronary surgery and incomplete revascularization of this vessel has been proven to be a predictor of higher long-term mortality after coronary artery bypass grafting 3. The presence of long stented segment LAD may result in having difficulties in finding an appropriate site for bypass grafting when conventional techniques are used. Therefore that could force bypass grafts to be anastomosed to a more distal site and the compromise runoff ‘per se’, decreasing graft patency 4.
Once FMJ procedures have been performed, the only effective way to adequately treat restenosis is by CE with stents extraction, followed by surgical revascularization.
Because stents cling firmly to the intima, the most suitable technique, in our experience, is performing CE under direct vision (open technique), rather than traction technique that could be associated either to the risk of ‘snowplow’ effect or to the risk of destruction of the artery 2,3,5.
In conclusion, CE with open technique represents a feasible and effective method for treating FMJ–LAD.
Acknowledgements
Conflicts of interest
There are no conflicts of interest.
References
- 1.Zwoliski R, Ostrowski S, Bany A, Ammer A, Jaszewski R. Surgical removal of stent from multiply stented vessel: problem with choice of place for anasthomosis ? One year follow-up. Kardiol Pol 2013; 71:615–617. [DOI] [PubMed] [Google Scholar]
- 2.Atoui R, Mohammadi S, Shum-Tim D. Surgical extraction of occluded stents: when stenting becomes a problem. Interact Cardiovasc Thorac Surg 2009; 9:736–738. [DOI] [PubMed] [Google Scholar]
- 3.Fukui T, Takanashi S, Hosoda Y. Coronary endarterectomy and stent removal in patients with in-stent restenosis. Ann Thorac Surg 2005; 79:558–563. [DOI] [PubMed] [Google Scholar]
- 4.Yilmazkaya B, Circi R, Circi UP, Gurkahraman S, Yukselen MA, Yondem OZ, Tasdemir O. Surgical approaches in left anterior descending artery in-stent stenosis. Ann Thorac Surg 2008; 85:1586–1590. [DOI] [PubMed] [Google Scholar]
- 5.Demirsoy E, Tandogan A, Yilmaz O, Tukenmez F, Tufekcioglu S, Sonmez B. Grafting the restenosed coronary artery after removal of multiple failed stents by endarterectomy. Tex Hear Inst J 2006; 33:262–263. [PMC free article] [PubMed] [Google Scholar]