

Abstract
INTRODUCTION:
Providing health promotion and communication learning opportunities for medical students practising their theoretical information into action, addressing the health problems, and trying to find suitable and feasible interventions is very much neededto learn and experience directly about healthrelated behavior in the community. Health promotion practice of PRECEDE-PROCEED model, is used as the foundation of this Family Outreach and Empowerment Program (FOEP). This study aims to implement and evaluate FOEP as an effective health promotion learning model for undergraduate medical students.
METHODS:
Two hundred and forty-four medical students joined the program for the whole weeks. The reports were evaluated to assess their activities throughout the process. Evaluation was done using the assessment checklists based on PRECEDE-PROCEED framework. Data collected from the assessment will be processed and analyzed using the IBM SPSS Statistics 22 program.
RESULTS:
Two hundred and forty-four report's has been evaluated, the report's scores in the category very good is 136, good 64, enough 26, bad 12 and very bad 6. The main problem in FOEP is behavior (37,6%) and the most alternate intervention choosen is education (232).
DISCUSSION:
The most intervention used by students for FOEP was education because it has been proven that can demonstrate feasibility, effectivity, increase knowledge control, and self-efficacy among disease.
CONCLUSION:
Student's reports was already satisfied.
Keywords: Family outreach and empowerment, student, health promotion
Introduction
Sustainable development goals (SDGs) is the latest international development agreement replacing the old agreement called millennium development goals (MDGs).[1] SDGs has been already implemented since year 2015 and expected to reach the goal in 2030. The SDGs consist of documents as thick as 35 pages which had been dealt by more than 190 countries which contain 17 objectives and 169 development targets.
Seventeen objectives with 169 targets are expected to address the underdevelopment countries around the world, both in developed countries (excessive consumption and production, and inequality) and developing countries (poverty, health, education, protection of marine and forest ecosystems, urban, sanitation, and drinking water availability).[1]
From the experiences of the MDGs (2000 2015), Indonesia has not succeeded in reducing maternal mortality, access to sanitation and drinking water, and a decrease in HIV-AIDS prevalence.[1]
Seventeen goals in SGDs are eliminating poverty, ending hunger, health, and wellbeing for all walks of life, good quality education, gender equality, availability of clean water and sanitation, access to affordable energy, economic growth, innovation and infrastructure, reducing inequality, sustainable development, sustainable consumption and production, preventing the impacts of climate change, safeguarding marine resources, maintaining terrestrial ecosystem, peace and justice, and revitalizing global partnerships.[2]
Medical students have at least three contingent roles that can be played for the achievement of SDGs goals.[3,4,5] The goal of SDGs that is focused on health personnel is goal number three, which is the health for all layers of the population. As an agent of health, when linked directly to SDGs, the agentofhealth becomes the front guard in fostering good relationship to the public.[3] The aim is to make people more concerned with their health and ultimately understand that being healthy is a valuable thing.
As an agent of change,[4] we expecting that the health quality of Indonesian society continues to increase and reach the SDGs in 2030 to come. Medical students can be a driver of change by sharing their knowledge and inviting people to change.[4]
Medical students as an agent of development synergize with the role of an agent of change.[4] Every efforts made for better change, primarily toward SDGs, can be maintained and developed in the future.[5]
Providing health promotion and communication learning opportunities for medical students practising their theoretical information into action, addressing the health problems, and trying to find suitable and feasible interventions is very much needed. Students will be able to learn and experience directly about health-related behavior in the community. Health promotion practice of PRECEDE-PROCEED model, a comprehensive framework in assessing individual needs, problems, and concerns to design, implement, and evaluate personalized health programs, is used as the foundation of this Family Outreach and Empowerment Program (FOEP). This study aims to implement and evaluate FOEP as an effective health promotion learning model for undergraduate medical students.
Method
The FOEP was a 5-week program, aimed for medical students in their 3rd year. During this program, every student was responsible for one family to assess and to be taken care of, with emphasize on their behavior and environment problems, as well as their personal health problems.
Evaluation of FOEP reports was conducted to analyze the skills of the undergraduate medical students of Sriwijaya University in writing the report of the FOEP.
The students were expected to assess their family's problems, choosing priorities, constructing and implementing interventions, evaluating and making follow-up plan after their session was finished.
Two hundred and forty-four medical students of Sriwijaya University joined the program for the whole 5 weeks, with every weekend was set as consultation and self-reflection day, and in their last day, they made a full report of their activities. Their reports were evaluated to assess their activities throughout the process.
Evaluation was done using the assessment checklist based on PRECEDE-PROCEED framework. The data collected from the assessment will be processed and analyzed using the IBM SPSS Statistics for Windows, Version 22.0, Arkmond, New York. This report use descriptive or univariate statistic analysis.
Every family has been given consent by the students themselves and the choices of participations are voluntary.
Results
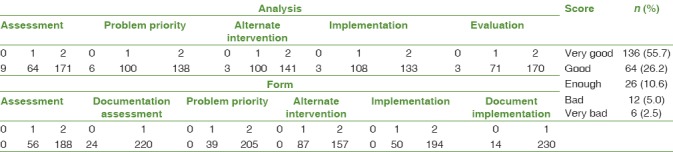
The highest percentage of student scores was in the category of very good (136) followed by good (64), enough (26), bad (12), and very bad (6).
In Table 1, we found some cells filled with 0. That means the student did not make any analysis on some of the FOEP report. In assessing the report of FOEP, we look at the completeness of reports from the assessment stage, assessment of documentation, priority issues, alternative interventions, and implementation of documentation. In general, students have compiled the report completely.
Table 1.
Family outreach and empowerment program score report (n=244)
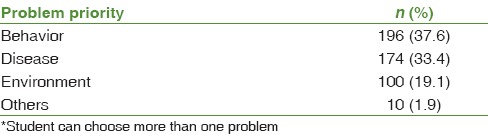
The priority problem is divided into three major groups. The groups are behavior, disease, and environment. Apart from the three categories, they are classified into other categories such as economic and educational issues. The main problem we found in FOEP as shown in Table 2 is behavior (37.6%), followed by disease (33.4%), environment (19.1%), and others (1.9%).
Table 2.
Problem priority*
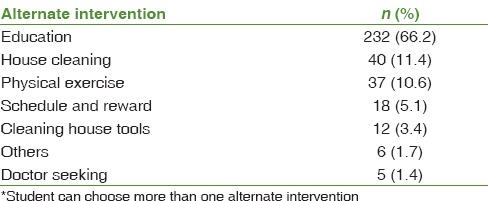
As seen in Table 3, Almost every student use education as alternate intervention, as many as 232 and then followed by 40 students using house cleaning, 37 students use physical exercise, 18 students use schedule and reward, 12 students use cleaning house tools, 5 students use doctor seeking, and 6 students use other interventions.
Table 3.
Alternate intervention*
Discussion
FOEPis one of the health education programs that has been approved and has impact in health problems.[6] In this program, medical students also play an important role inside of it.[7] The aim of this research is they can approach health promotion and assessing the concerned family.
Student's reports on their activities are examined; resulted in a quite satisfactory 55.7% rate of completeness in fulfilling steps of PRECEDE-PROCEED with no dropout throughout the program. The best rate of step completion and analysis were found in assessment stage. As comparison to the similar previous study which showing most students complete good FOEP (87%), this study already shows satisfactory results too.
Students reported that the FOEP program was effective in improving their confidence and ability in communicating, constructing fun interventions, negotiating, and giving counseling to family members; also, they were more aware that health problems need to be taken care as a whole concept, instead of just in one clinical perception. The students also recommend this program to continue for next year.
Although there were some concerns in their choice of health intervention alternatives and implementations, they still rely on basic counseling and education as the intervention instead of doing more creative, personalized, and behavior-changing intervention.
In this study, the most intervention used by students for FOEP was education, as it shows 66.7% compared to other intervention. They tend to choose education rather than the other intervention because it has been proven in the previous study in the United States that education can demonstrate the feasibility and effectivity for promoting health education; also, education aimed at increasing knowledge control and self-efficacy among disease.[8]
Beside having the advantages, education also has flaws such as difficulties to communication with family members; the family afraid to tell or explain about their problems; bad communication techniques of students; and decreased empathy from students.[9,10]
Media promotion such as video, brochure, cartoon, or poster can help people to learn easily about health promotion. People's formal education affects their way to understand, so it is important to choose properly the media that is going to be used.[11] Verbal promotion is less effective than media promotion, especially with something that can be used such as props, model, figure, or mannequin.[12]
Otherwise, in the assessment, many of the students did not complete the report as expected. Some of them showed unsatisfied result in the assessment. One of the causes is students tend to do procrastination or the report was made in short time at the deadline. Procrastinating makes report quality worse.[13]
The other problem for students is time limitation to write FOEP report. Beside writing the report, they also have to attend the daily lecture activities; this caused the time to communicate with their concerned family and write the report limited. In fact, every person averagely need 10 min to explain and tell their problem to other person.[14]
This study showed that students are more concern about document completeness than the quality of report's analysis.
This report also shows that the students chose behavior as the most priority problem, showing 37.6%. Behavioral health is essential to the realization of healthy communities and healthy individuals. Students prefer to choose behavior intervention because of the appropriateness, cost-effectiveness, affordability, acceptability, and sustainability of the intervention followed thereafter.[15] Behavioral change is important for healthy communities. Good behavior such as maintaining health will increase someone's quality of life and prosperous, for example, by doing some sanitary activities and maintaining healthy life.[16] It shows that the students not only concern about biological problem but also psychosocial and mental health problem. In general, the students often miss psychosocial problem and tend to concern about their biology or physical problem than their mental health.[17]
There are factors that also affect FOEP report, which are lecturer's teaching method and student's motivation. The good method that lecturers use could affect their student to accept the topics. Every teacher have a responsibility to presents, explains, responsible for the contents of the materials in the learning process in college.[18] Therefore, studying must be known as active, constructive, and self-regulated process, so the students will get academic achievement.[19]
Motivation to study affects the student's achievement. Motivation is an encouragement that pushes student to study. Motivation can be form of verbal, physic, or psychosocial response. It is important for every student to have motivation to gain a good achievement in education.[20]
Simultaneusly, Student's ability to study effectively would growth from adolescence. They were started from how they are organizing and setting their study purpose, planning and monitoring, scheduling, and motivating their self and environment.[19,21] Student's ability to organize learning pattern is different from one to another student. There are some factors that influence academic achievement on student, which are (a) their ability to understand, (b) time management, and (c) learning strategy.[21]
Assignment becomes a factor that affects student's performance. Assignment becomes indicator how far the student understands about the topic. For medical students, assignment is given at every block that they passed.[22]
Conclusion
Exposure to the community can be done early in undergraduate level, as medical students can make an impact in addressing health problems in the community
Student's skills in making FOEP report were basically good
The most used intervention by the students for FOEP is education
More inputs about variety of health promotion strategies should be introduced to ensure more effective interventions that leading to behavioral change and to resolve health problems
Community-related activities were also useful to increase medical students' confidence dealing with other people and insights of the importance of health promotion and prevention.
Suggestion
First, lecture can be given before FOEP activity. Students need to know the system and procedures about FOEP. Second, template could be helping students to minimalize error of writing FOEP. Third, students write FOEP report with supervisor.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
Thanks to all medical students of Sriwijaya University for participating in this research and staff of Public Health Sciences and Community Medicine Department, Faculty of Medicine, Sriwijaya University.
References
- 1.Hoelman M, Parhusip B, Eko S, Bahagijo S. Jakarta: Infid; 2015. SGDs Guide for Local Government. [Google Scholar]
- 2.Sustainable Development Knowledge Platform. SDGs & Topics. [Last accessed on 2016 Aug 20]. Available from: https://www.sustainabledevelopments.un.org/topics .
- 3.Crisp N, Chen L. Global supply of health professionals. N Engl J Med. 2014;370:950–7. doi: 10.1056/NEJMra1111610. [DOI] [PubMed] [Google Scholar]
- 4.Harding F, Charlton R. Reflective writing as an agent for change. BMJ Careers. 2016 [Google Scholar]
- 5.Lawrence WG, Krauter MW. Mountain View: Mayfield Publishing Company; 1999. Health Promoting Planning an Educational and Environmental Approach. [Google Scholar]
- 6.Ririanty M. application of PRECEDE-PROCEED Theory in the Success Of Family Folder Program for Preventing Transmission of TB on a FamilyUniversity of Jember. 2014 [Google Scholar]
- 7.College of Medicine Tucson. Mobile Health Program. Family & Community Medicine. 2017. [Last accessed on 2016 Sep 15]. Available from: http://www.fcm.medicine.arizona.edu/outreach/mobile-health-program .
- 8.National Institute of Health. Washington DC: National Academic Press (US); 2001. Health and Behavior: The Interplay of Biological, Behavioral, and Societal Influence. [PubMed] [Google Scholar]
- 9.Ha JF, Longnecker N. Doctor-patient communication: A review. Ochsner J. 2010;10:38–43. [PMC free article] [PubMed] [Google Scholar]
- 10.DiMatteo MR. The role of the physician in the emerging health care environment. West J Med. 1998;168:328–33. [PMC free article] [PubMed] [Google Scholar]
- 11.Komala L, Novianti E, Subekti P. Strategy of Health Promotion Media Selection in the Prevention of HIV/AIDS at Garut District. Acta Diurna. 2014;10:34–43. [Google Scholar]
- 12.Notoadmodjo S. Jakarta: Rineka Cipta; 2012. Health Promotion and Health Behavior. [Google Scholar]
- 13.Rief W. Analyzing the problems in managing patients with medically unexplained symptoms. J Gen Intern Med. 2007;22:704–6. doi: 10.1007/s11606-007-0151-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Andersson SO, Ferry S, Mattsson B. Factors associated with consultation length and characteristics of short and long consultations. Scand J Prim Health Care. 1993;11:61–7. doi: 10.3109/02813439308994904. [DOI] [PubMed] [Google Scholar]
- 15.SAMHSA. Disaster Planning Handbook for Behavioural Health Treatment Programs. [Last accessed on 2017 Dec 01]. Available from: http://www.stoore.samhsa.gov/shin/content//SMA13-4779/SMA13-47779.pdf .
- 16.Adliyani ZO. The effect of human behaviour for healthy life. Majority. 2015;4:109–14. [Google Scholar]
- 17.Gulbrandsen P, Fugelli P, Sandvik L, Hjortdahl P. Influence of social problems on management in general practice: Multipractice questionnaire survey. BMJ. 1998;317:28–32. doi: 10.1136/bmj.317.7150.28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Tri S. Relationship Between Learning Motivation, Learning Independence and Academic Guidance on Student Achievement at Stikes A. Yani Yogyakarta. Family Medicine Study Program Postgraduate Program of Sebelas Maret University. 2009 [Google Scholar]
- 19.Wang B. Columbus: Ohio; 2004. Self-Regulated Learning Strategies and Self-Efficacy Beliefs of Children Learning English as a Second Language, Desertation, the Ohio State University. [Google Scholar]
- 20.Christyanti D, Mustami'ah D, Sulistiani W. Relationship between Self Adjustment to Academic Demands and Stress Tendencies in Students of Medical Faculty Hang Tuah University Surabaya. Jurnal Insan Media Psikologi. 2010;12:153–9. [Google Scholar]
- 21.Edwin Adrinata S, Sia T. Mahasiswa versus tugas: Prokrastinasi akademik dan conscientiousness. Indones Psychol J. 2007;22:352–74. [Google Scholar]
- 22.Henrik LB. California: Third Party Publishing Company; 1983. Expanding Health Horizons: From a General Systems Concept of Health to a National Health Policy. [Google Scholar]