

Abstract
A case of the right pulmonary artery-to- left atrial fistula with atrial septal defect (ASD) is presented. The fistula was detected after the patient developed desaturation following surgical closure of the ASD. It was managed with a transcatheter (trans-RPA route) closure of the fistula using a 12-mm Amplatzer ventricular septal defect closure device.
Keywords: Atrial septal defect, device closure, pulmonary artery-to-left atrial fistula
INTRODUCTION
Pulmonary arteriovenous fistula is an abnormal communication between a pulmonary artery (PA) and pulmonary vein with the absence of capillary network that links the two. The right pulmonary artery-to- left atrial fistula is a type of pulmonary arteriovenous fistula.[1]
Here, we present a case of RPA-to-left atrial fistula with atrial septal defect (ASD) and its management.
CASE REPORT
A 4-year-old boy presented to our outpatient department with a history of recurrent lower respiratory tract infection since childhood. He had no history of cyanosis, and the examination was significant for an ejection systolic murmur at the pulmonary area. His blood O2 saturation on room air was within normal limits.
Transthoracic echocardiography suggested a 2-cm ostium secundum atrial septal defect (OS ASD) (left-to-right shunt) with deficient superior vena cava (SVC) margins. There was normal systemic and pulmonary venous drainage, and no other associated cardiac lesions were noted.
The patient was taken up for surgical patch closure after due informed consent. Cardiopulmonary bypass (CPB) was established using aorto-bicaval cannulation and mild hypothermia (32°C). Aorta was clamped and antegrade cardioplegia was perfused. After right atriotomy, a solitary OS-ASD was found. There was normal pulmonary venous drainage. However, there was a slightly aneurysmal outpouching on the right side of the left atrium (LA), and right pulmonary veins were opening into this aneurysmal sac. A small additional opening in the aneurysmal sac where right pulmonary veins were opening was noted and this was probed. The distal end seemed to be directed into the right lung. No intervention was done for it as it was thought to be an abnormal opening of a right lobar pulmonary vein into LA. Pericardial patch closure of ASD was done. However, on weaning the patient off, CPB blood SpO2 dropped down to 72%.
A transthoracic echocardiogram with saline contrast was performed which demonstrated intact ASD patch. SVC and inferior vena cava were seen draining into the right atrium (RA). This ruled out patch dehiscence or routing of caval blood into LA. However, there was delayed appearance of contrast in LA after a couple of cardiac cycles without any identifiable source.
Decision was taken to shift the patient to the catheterization laboratory for an emergent catheterization study. Cardiac catheterization revealed a large RPA-to-left atrial fistula [Figure 1].
Figure 1.

Fluoroscopy with right pulmonary artery injection demonstrating the right pulmonary artery-to-left atrial fistula (arrow)
The fistula was closed with a 12-mm Amplatzer ventricular septal defect closure device using a trans-RPA approach [Figures 2 and 3]. Post procedure, the patient's saturation improved immediately to 100% and the patient had uneventful postoperative course. The patient was discharged on postoperative day 5 on aspirin and anticoagulant. He is healthy on 1-year follow-up.
Figure 2.
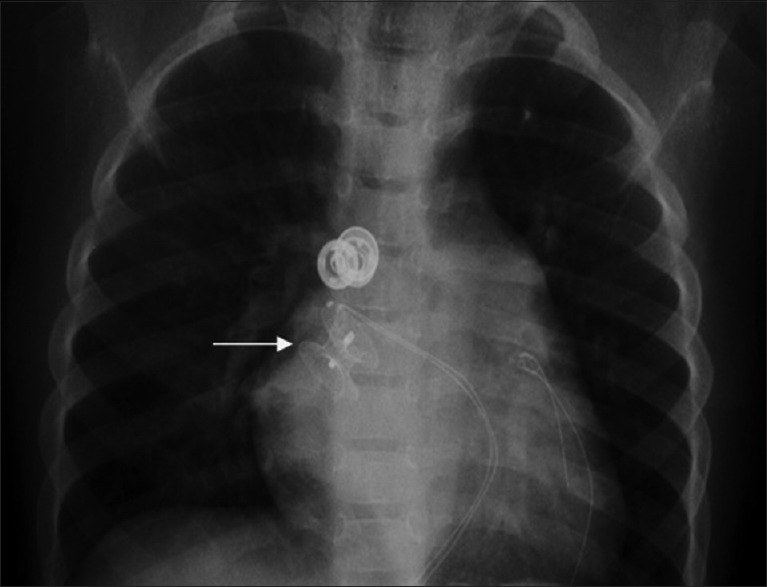
Plain radiograph of the chest (posteroanterior view) with the radiopaque shadow of the Amplatzer device in situ
Figure 3.

Computerized tomography scan (transverse view) showing the Amplatzer device positioned in the right pulmonary artery-to-left atrial fistula
DISCUSSION
Embryologically, incomplete degeneration of septum between the arterial and venous plexus of the pulmonary vascular bed or defective capillary loops leading to formation of thin-walled sacs result in formation of pulmonary arteriovenous fistulas. A pulmonary vein connected to this fistula is absorbed into LA, resulting in a PA–LA fistula.[2]
Agenesis of a lung lobe and consequent absence of pulmonary capillary bed is another explanation.[3] In one patient, it was thought to represent the original vascular connection of an accessory lung lobe.[4] Less than 100 cases of PA-to-LA fistula have been reported,[2] almost all of them from right PA to LA. Only three cases of left PA-to-LA fistula have been reported.[5,6,7,8]
The fistula in our patient was Type I as described by De Souza e Silva et al., where the fistula connects RPA to LA, but PA and veins are normal.[9] The lung lower lobe RPA branch drains directly into the LA while the right lower pulmonary vein is absent in Type II fistula. In Type III, pulmonary veins drain into the right PA to LA fistula. ASD is commonly associated anomaly with these fistulas.[7]
RPA-to-LA fistula might be encountered associated with OS-ASD. It should always come to mind if an aneurysmal sac is attached to the right of left atrium or an extra opening is seen in the roof of the left atrium. However, this finding has not been reported in the literature previously. Angiographic investigation is required as a clinical diagnosis of RPA-to-left atrium communication is difficult. Surgery provides a complete cure and should be performed with the patient on CPB. Elective surgery is the best treatment to prevent chronic arterial hypoxemia, systemic thromboembolic complications, congestive heart failure, and shunt-derived pulmonary hypertension.
This case is unique because there was no preoperative cyanosis. This was presumably because the RPA blood was directed from the left atrium (LA) to the RA. The cyanosis manifested postoperatively, after ASD closure as the left-to-right shunt was abolished, and only a right-to-left shunt remained (RPA to LA). A trans-RPA route was taken to close the fistula as the ASD had been closed. The transseptal approach is most commonly described in the literature as the preferred route.[10] Moreover, even though this was an incidental diagnosis at surgery, the case was managed successfully.
CONCLUSION
RPA-to-left atrial fistula is a very rare entity occasionally encountered with OS-ASD. Its correct diagnosis and management are essential to prevent catastrophic postoperative complications.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Moyer JH, Glantz G, Brest AN. Pulmonary arteriovenous fistulas; physiologic and clinical considerations. Am J Med. 1962;32:417–35. doi: 10.1016/0002-9343(62)90131-6. [DOI] [PubMed] [Google Scholar]
- 2.Ohara H, Ito K, Kohguche N, Okhawa Y, Akasak T, Takarada M, et al. Direct communications between the right pulmonary artery and left atrium. J Thorac Cardiovasc Surg. 1979;77:742–7. [PubMed] [Google Scholar]
- 3.Lucas RV, Jr, Lund GW, Edwards JE. Direct communication of a pulmonary artery with the left atrium. An unusual variant of pulmonary arteriovenous fistula. Circulation. 1961;24:1409–14. doi: 10.1161/01.cir.24.6.1409. [DOI] [PubMed] [Google Scholar]
- 4.Kroeker EJ, Admas HD, Leon AS, Pouget JM. Congenital communication between a pulmonary artery and the left atrium. Physiological observations and review of the literature. Am J Med. 1963;34:721–5. doi: 10.1016/0002-9343(63)90111-6. [DOI] [PubMed] [Google Scholar]
- 5.Mohanty SR, Yadav R, Kothari SS, Airan B. Right pulmonary artery left atrium communication. Ann Thorac Surg. 2000;69:269–71. doi: 10.1016/s0003-4975(99)01192-3. [DOI] [PubMed] [Google Scholar]
- 6.Thakkar BM, Raval A, Oswal N. Transcatheter closure of left pulmonary artery to left atrium fistula in a neonate using amplatzer duct occluder I. J Invasive Cardiol. 2014;26:E91–4. [PubMed] [Google Scholar]
- 7.Karnik AM, Nilsson U, Vijayaraghavan G, Hashmi J, Shuhaiber H. Direct communication between left pulmonary artery and the left atrium. Chest. 1989;96:937–9. doi: 10.1378/chest.96.4.937. [DOI] [PubMed] [Google Scholar]
- 8.Sambasivam KA, Dhanawade SM, Krishnaswami S. Direct communication between left pulmonary artery and left atrium. Ind Heart J. 1995;47:40–1. [Google Scholar]
- 9.De Souza e Silva NA, Giuliani ER, Ritter DG, Davis GD, Pluth JR. Communication between right pulmonary artery and left atrium. Am J Cardiol. 1974;34:857–63. doi: 10.1016/0002-9149(74)90710-3. [DOI] [PubMed] [Google Scholar]
- 10.Vadlamudi K, Verma S, Christopher J, Penumatsa RR, Koneti NR. Transcatheter closure of large right pulmonary artery-to-left atrial fistula. Ann Pediatr Cardiol. 2013;6:188–90. doi: 10.4103/0974-2069.115282. [DOI] [PMC free article] [PubMed] [Google Scholar]