

Abstract
Homocystinuria is a genetic inborn error of metabolism due to the deficiency of cystathionine β-synthase resulting in increased serum homocysteine and methionine and decreased cysteine which predisposes affected individuals to arterial and venous thromboembolic phenomena. We present a case of homocystinuria who presented to us as a calcified right atrial mass during the evaluation for lower respiratory tract infection. Our case reveals an unusual mix of findings using imaging with multiple detector computed tomography and radiographs.
Keywords: Calcified cardiac mass, cardiac thrombus, homocystinuria
INTRODUCTION
Cardiac calcifications may be nonspecific or they may be indicators of some local or systemic pathology. Cardiac calcifications are most often seen in coronary atherosclerotic disease. Other causes include vascular, toxic, inflammatory, and degenerative disease. In children, causes of cardiac calcifications include chromosomal disorders, intrauterine infections, hyperparathyroidism, and inborn errors of metabolism. Calcifications may also be seen in cardiac tumors, most commonly in myxomas, fibromas, and teratomas.[1] Intracavitary tumors of the right atrium are rare and may be primary or metastatic. Metastatic tumors of the heart are more common than primary. Metastases usually involve the pericardium and rarely produce intracavitary masses.[2] In children, the metastatic cardiac disease is even rarer than adults with sarcoma, lymphoma, testicular cancer, and Wilms tumor being common primaries.[3] Transesophageal imaging frequently adds additional important information to the assessment of mass lesions and should always be considered when image quality is inadequate or pertinent clinical questions remain unanswered with surface imaging.[4] Computed tomography and cardiac magnetic resonance imaging are being increasingly used in the characterization and evaluation of cardiac masses.
CASE REPORT
A 13-year-old boy was referred to our hospital for the evaluation of mental retardation due to poor performance at school. The parents gave a history of delayed milestones as compared to siblings and multiple respiratory tract infections. There was no history of visual disturbances, trauma, or central venous catheterization. The patient had two elder sisters, both of whom had no known medical issues. There was no history of mental retardation or sudden cardiac death in the first degree relatives of the mother or father. Physical examination revealed a weight for age and height for age below 3rd centile with a high arched palate, slender extremities, and long thin fingers. “Thumb sign” was positive. No kyphosis or scoliosis was present. Ophthalmological examination revealed bilateral ectopia lentis. Chest examination revealed bilateral basal crepts. Chest radiograph showed a calcified mass in the right hilar region and prominent bilateral bronchovascular markings. The patient underwent contrast-enhanced computed tomography for the evaluation of the hilar mass which was found to be a densely calcified mass in the right atrium with a calcified tail extending into superior vena cava (SVC) and the right subclavian vein. Bronchiectasis was seen in both lungs [Figures 1 and 2]. Echocardiography performed subsequently showed a nonmobile right atrial mass adherent to the endocardium with dense posterior acoustic shadowing. The lack of mobility, the absence of myocardial continuity, no relation to foramen ovale, and morphology of the mass, especially the extension into the SVC suggested that the mass represented a calcified thrombus. Coagulation studies showed prolongation of PT and aPTT with elevation of fasting plasma homocysteine (235 μmol/l) and elevated methionine (139.3 μmol/l). Radiographs of his hands showed diffuse osteopenia with long fingers [Figure 3]. Elevated levels of homocysteine may be found in deficiencies of vitamin B12 or folic acid and in other disorders of methionine metabolism; however, the severity of homocysteinemia with coexisting methioninemia, Marfanoid features, and mental retardation suggest the diagnosis of homocystinuria. The patient was then started on pyridoxine, folic acid, and vitamin B12, and then referred to a higher center for the surgical management of the right atrial mass.
Figure 1.
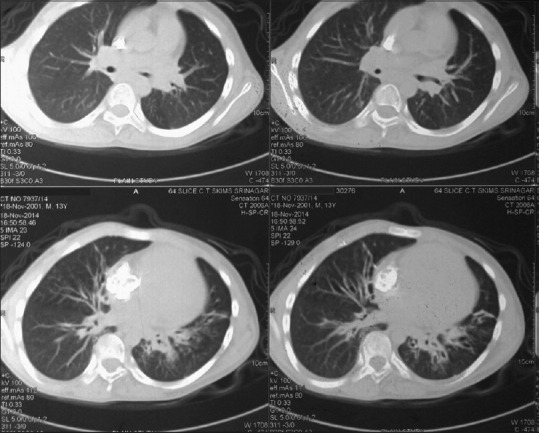
Computed tomography showing the calcified right atrial mass with a calcified tail extending into superior vena cava, bronchiectasis seen in the right middle lobe
Figure 2.
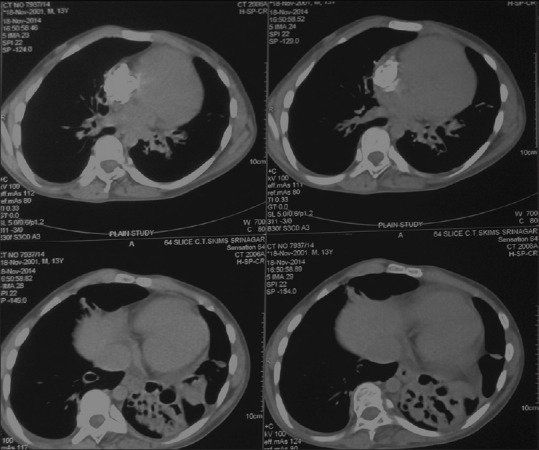
Computed tomography showing bronchiectasis in both lower lobes, with adjacent consolidation on the left side
Figure 3.

Diffuse osteopenia in radiograph of both hands
DISCUSSION
Homocystinuria is a genetic inborn error of metabolism due to the deficiency of cystathionine β-synthase resulting in increased serum homocysteine and methionine and decreased cysteine.[5] Patients with this disorder are initially normal at birth. During infancy, nonspecific features are present, which include developmental delays, and failure to thrive.[6] Typical manifestations occur later and include mental retardation, osteoporosis, marfanoid characteristics, lens dislocation, and thrombophilic tendencies.[7] The course of the disease is such that approximately 40% experience a vascular event by the time they are 20 years of age.[8]
Atrial thrombosis has been reported in patients with central venous catheters, ventriculoatrial shunts, and pacing electrodes.[1,9] Atrial thrombi are more common than myxomas; however, in cases, where the thrombus is pedunculated, it may be difficult to distinguish between the two on imaging.[10]
Calcified cardiac masses not related to thrombosis have been reported and are descriptively termed calcified amorphous tumor of the heart.[11] This patient had a known predisposing factor to thrombus formation, and therefore, the mass likely represented a calcified thrombus. To the best of our knowledge, such a presentation of homocystinuria as a calcified right atrial mass has not been reported. Calcified thrombi are important differentials to be considered when evaluating hyperdense cardiac masses, and an assessment for deranged coagulation profile should be performed in such patients.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Watts MA, Innes BJ. Calcified atrial thrombus: Complication of central venous hyperalimentation. Tex Heart Inst J. 1984;1s1:76–9. [PMC free article] [PubMed] [Google Scholar]
- 2.Panidis IP, Kotler MN, Mintz GS, Ross J. Clinical and echocardiographic features of right atrial masses. Am Heart J. 1984;107:745–58. doi: 10.1016/0002-8703(84)90324-7. [DOI] [PubMed] [Google Scholar]
- 3.Tao TY, Yahyavi-Firouz-Abadi N, Singh GK, Bhalla S. Pediatric cardiac tumors: Clinical and imaging features. Radiographics. 2014;34:1031–46. doi: 10.1148/rg.344135163. [DOI] [PubMed] [Google Scholar]
- 4.Peters PJ, Reinhardt S. The echocardiographic evaluation of intracardiac masses: A review. J Am Soc Echocardiogr. 2006;19:230–40. doi: 10.1016/j.echo.2005.10.015. [DOI] [PubMed] [Google Scholar]
- 5.Mudd SH, Skovby F, Levy HL, Pettigrew KD, Wilcken B, Pyeritz RE, et al. The natural history of homocystinuria due to cystathionine beta-synthase deficiency. Am J Hum Genet. 1985;37:1–31. [PMC free article] [PubMed] [Google Scholar]
- 6.Eslamiyeh H, Ashrafzadeh F, Akhondian J, Beiraghi Toosi M. Homocystinuria: A Rare disorder presenting as cerebral sinovenous thrombosis. Iran J Child Neurol. 2015;9:53–7. [PMC free article] [PubMed] [Google Scholar]
- 7.Disorders of transsulfuration. In: Mudd SH, Levy HL, editors; Stanbury JB, Wyngaarden JB, Frederickson DS, Goldstein JL, Brown MS, editors. Metabolic and Molecular Bases of Inherited Disease. New York: McGraw-Hill; 1983. [Google Scholar]
- 8.vd Berg W, Verbraak FD, Bos PJ. Homocystinuria presenting as central retinal artery occlusion and longstanding thromboembolic disease. Br J Ophthalmol. 1990;74:696–7. doi: 10.1136/bjo.74.11.696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gabriele OF, Clark D. Calcified thrombus of the superior vena cava. Complication of ventriculoatrial shunt. Am J Dis Child. 1969;117:325–7. doi: 10.1001/archpedi.1969.02100030327014. [DOI] [PubMed] [Google Scholar]
- 10.Scheffel H, Baumueller S, Stolzmann P, Leschka S, Plass A, Alkadhi H, et al. Atrial myxomas and thrombi: Comparison of imaging features on CT. AJR Am J Roentgenol. 2009;192:639–45. doi: 10.2214/AJR.08.1694. [DOI] [PubMed] [Google Scholar]
- 11.Reynolds C, Tazelaar HD, Edwards WD. Calcified amorphous tumor of the heart (cardiac CAT) Hum Pathol. 1997;28:601–6. doi: 10.1016/s0046-8177(97)90083-6. [DOI] [PubMed] [Google Scholar]