

Sir,
The occurrence, of myocarditis following diphtheria-tetanus-pertussis (DPT) vaccine, is implicated to the pertussis component.[1] We describe one such incidence developing after 48 h of DPT vaccination in a 6 week old female infant with a large ventricular septal defect (VSD) and biochemical evidence of acute kidney injury.
A 6-week-old female infant presented to us in severe respiratory distress and intermittent low-grade fever developing 2 days after the DPT vaccination. She was born to a primigravida through normal vaginal delivery with a birth weight of 3 kg and had an uneventful perinatal period. At presentation, she was severely tachypneic and tachycardiac with cold peripheries, feeble pulses, and hypotensive (62/36 mmHg). Systemic examination revealed bilateral crepitations and wheeze, with a 2/6 short systolic murmur over the left sternal border. The liver was palpable 5 cm below right costal margin, soft in consistency. The baby was urgently shifted to pediatric Intensive Care Unit under radiant warmer and put on high-flow humidified nasal oxygen therapy. Arterial blood gas done showed metabolic acidosis (pH 7.10) and hypoxia.
Chest X-ray showed cardiomegaly with a left ventricle (LV) type apex and pulmonary venous congestion [Figure 1]. Electrocardiogram showed sinus tachycardia with nonspecific ST depression in precordial leads [Figure 2]. Echo was done at the bedside which showed biventricular dysfunction with LV ejection fraction of 25% (severe dysfunction), moderate mitral regurgitation, and a slightly malaligned large subaortic VSD [Figures 3 and 4]. Laboratory investigations showed normal hemogram, but erythrocyte sedimentation rate and C-reactive protein were high. Renal parameters were deranged while creatine kinase MB and liver enzymes were elevated [Table 1]. Ultrasound for the kidneys was normal.
Figure 1.

Chest X-ray showing cardiomegaly with left ventricular type of apex and pulmonary venous congestion
Figure 2.

Electrocardiogram showing sinus tachycardia with nonspecific ST segment changes in the precordial leads
Figure 3.
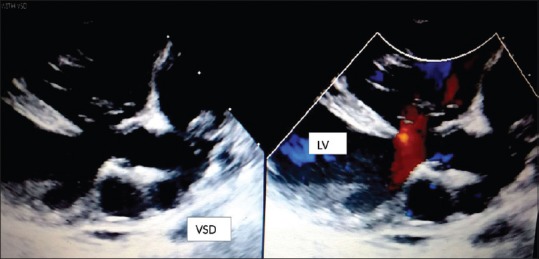
Parasternal long axis view showing malaligned large subaortic ventricular septal defect shunting left to right and a dilated left ventricle
Figure 4.

Apical four chamber view showing dilated all four chambers with moderate mitral regurgitation jet
Table 1.
Periodic patient response

The infant was kept nil orally on two-third maintenance fluids intravenously. Management included oxygen, injection furosemide infusion at 0.1 mg/kg/h, and intravenous dobutamine at 5 mg/kg/min (2 days). As apparently asymptomatic, young infant with no preceding viral illness developed severe respiratory distress following DPT vaccination a possibility of postvaccinal (DPT) myocarditis was suspected. Keeping this in mind, the patient was started on injection methylprednisolone at 2 mg/kg/day. She continued to have high-grade intermittent fever for the next 48 h but showed gradual improvement with decrease in heart rate, respiratory rate, and remission of fever. Biochemical parameters and inflammatory markers also settled gradually [Table 1]. Steroids were stopped after 2 days when repeat echo showed normal biventricular function. Injection furosemide was changed to oral furosemide at 2 mg/kg/day with oral digoxin at 10 mg/kg/day on day 3 of admission. The patient was discharged after 4 days on oral furosemide and digoxin. Due to the possibility of the pertussis component being the causative agent, the patient was given acellular pertussis vaccine with diphtheria and tetanus toxoid at 10 weeks. She did not show any reaction to acellular pertussis vaccine apart from a single episode of low-grade fever. She is under follow-up on antifailure drugs and is gaining weight albeit at the lower rate, awaiting VSD closure at 3–6 months of age.
Myocarditis following DPT vaccine is very rare. We attributed this in our case because the symptomatology occurred after the inoculation. The patient additionally had a serendipitous finding of a large VSD. Other similar reports[2,3,4] are in structurally normal heart [Table 2].
Table 2.
Different reports including the present case

The proposed mechanism of myocarditis following a vaccination is due to maladaptive immune dysfunction.[5] The component of vaccine causing this immune dysfunction is not clear. However, based on this hypothesized etiology, some workers propose using anti-inflammatory agents either ibuprofen or steroids.[3]
This report highlights a very rare phenomenon occurring in a patient with a large VSD. The age of presentation matches with a natural history of presentation of large posttricuspid shunts (VSD and patent ductus arteriosus). The submission further emphasizes the management of such a rare case and the safety of acellular pertussis vaccine following such an incidence. In contrast, the other workers[2,3,4] have avoided giving diphtheria and pertussis component.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Helle EP, Koskenvou K, Heikkila J, Pikkarainen J, Weckstrom P. Myocardial complications of immunizations. Ann Clin Res. 1978;10:280–7. [PubMed] [Google Scholar]
- 2.Amsel SG, Hanukoglu A, Fried D, Wolyvovics M. Myocarditis after triple immunization. Arch Dis Child. 1986;61:404–5. doi: 10.1136/adc.61.4.403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Karakurt C, Koçak G, Akıncı A, Elkıran O. Myocarditis after diphtheria-tetanus-whole cell pertussis and polio vaccination: Case report. Ann Pediatr Card. 2009;16:37–9. [Google Scholar]
- 4.Wu SJ, Sun S, Li JY, Hu PY, Chien CY. Acute fulminant myocarditis after diphtheria, polio, and tetanus vaccination. Asian Cardiovasc Thorac Ann. 2006;14:e111–2. doi: 10.1177/021849230601400627. [DOI] [PubMed] [Google Scholar]
- 5.Murphy JG, Wright RS, Bruce GK, Baddour LM, Farrell MA, Edwards WD, et al. Eosinophilic-lymphocytic myocarditis after smallpox vaccination. Lancet. 2003;362:1378–80. doi: 10.1016/S0140-6736(03)14635-1. [DOI] [PubMed] [Google Scholar]