

Abstract
We use daily diary data from the Disability and Use of Time supplement to the 2013 Panel Study of Income Dynamics (n=1162) to evaluate: (1) the extent to which marital/partner support and strain moderate the effects of disability on five activity-related emotions (happy, calm, sad, frustration, worry) and overall negative and positive emotion among older married, cohabiting, and dating persons; and (2) whether such patterns differ significantly by gender. Marital support buffers against negative emotions and increases feelings of calm among severely impaired women. By contrast, support intensifies negative emotions and decreases feelings of calm among severely impaired men. Relationship strain also intensifies the effect of severe impairment on men’s frustration, sadness, worry, and negative mood, but has negligible effects on the negative emotions of men with low impairment and women. Frequent support and criticism may threaten highly impaired older men’s sense of autonomy and emotional well-being.
Keywords: disability, intimate relationships, older adults, social support, well-being
The aging of the U.S. population is widely documented. By 2030, persons ages 65 and older will account for more than one-fifth of the U.S. population, with similar patterns projected for most wealthy developed nations (Federal Interagency Forum on Aging-Related Statistics 2012). Most older adults eventually develop chronic conditions and may require assistance and support from significant others. Disablement affects more than 40 percent of older adults in the United States, with rates increasing with advancing age (Freedman et al. 2013). Economic costs associated with late-life disablement and dependence are well documented (Anderson et al. 2011), and mounting research documents the personal and psychological challenges for older adults and their families (Bierman 2012; Caputo and Simon 2013).
Disablement has negative consequences for psychological well-being, most notably depressive symptoms (Bierman 2012; Chan et al. 2011), yet few studies explore whether these patterns are contingent upon the level of emotional support and strain experienced in one’s marriage or romantic relationship. Intimate relationships are an important source of support for older adults, especially as they manage age-related conditions that limit functioning and social participation (Mancini and Bonanno 2006). With advancing age, one’s work and childrearing responsibilities subside, rendering one’s marital/romantic relationship increasingly salient to emotional well-being (Lang and Carstensen 2002).Yet late-life partnerships, even long-term marriages, are not uniformly supportive and may be marked by unpleasant or critical interactions that compound the emotional distress accompanying disablement (Boerner et al. 2014). However, we know of no studies exploring the complex ways that positive and negative aspects of late-life romantic partnerships buffer or amplify the deleterious psychological effects of disablement.
Drawing on stress buffering (Cohen and Wills 1985) and amplification (Ingersoll-Dayton, Morgan, and Antonucci 1997) perspectives, we evaluate the extent to which the effects of disablement on older adults’ daily emotions are buffered by positive or amplified by negative aspects of one’s marital, cohabiting, or dating relationship. We explore whether these patterns differ by gender, given well-documented gendered patterns of marital interaction among older couples (Carr, Cornman, and Freedman 2016). We use 24-hour diary data from the 2013 Disability and Use of Time supplement to the 2013 Panel Study of Income Dynamics, which assesses five discrete emotions while engaged in daily activities on the diary day: happiness, calm, worry, sadness, and frustration. These momentary measures of mood may be less susceptible to recall bias than aggregated retrospective measures of psychological health (Stone and Mackie 2014), and less likely than depressive symptom scales to underestimate men’s vulnerability to disablement-related distress (Stommel et al. 1993). Understanding how relationship strain and support moderate the effects of disablement on older adults’ emotions is an important goal; it reveals the influence of socioemotional context in the disablement process, and may highlight appropriate sites of intervention for the 25 million older adults with an activity-limiting disability (Federal Interagency Forum on Aging-Related Statistics 2012).
BACKGROUND
Disablement and Daily Emotions among Older Adults
Older adults commonly develop chronic health conditions that impair their physical, cognitive, and sensory capabilities (Freedman et al. 2013). These impairments may limit their activities and alter their daily routines, carrying implications for their psychological well-being. Disability and impairment are associated with more frequent depressive symptoms, and compromised life satisfaction and self-esteem (Gayman, Turner, and Cui 2008; Mancini and Bonanno 2006; Ormel et al. 2002). Longitudinal studies demonstrate that these effects operate from disability to distress, rather than vice-versa (Gayman et al. 2008; Ormel et al. 2002). Disability has been characterized as requiring a “fundamental reorientation to daily functioning and renegotiation of participation in the social world” (Bierman and Statland 2010:631). These adjustments may be distressing; persons with impairments that are not readily accommodated may have a reduced ability to carry out daily activities, maintain social relationships, and live independently (Taylor and Lynch 2004). They also may give up work or leisure activities that were once a source of enjoyment, and may feel their autonomy and independence are undermined (Freedman et al. 2012).
Research documents that disability takes a psychological toll, yet this work focuses almost exclusively on depressive symptoms or life satisfaction, rather than discrete emotions such as frustration, anxiety, or happiness (Chipperfield, Perry, and Weiner 2003). Commonly-used depressive symptoms checklists may underestimate men’s and overestimate women’s emotional vulnerability, as they are skewed toward somatic and emotional symptoms (e.g. crying, feeling lethargic) that are more culturally acceptable for women (Stommel et al. 1993). Consequently, our knowledge is limited regarding the potentially far-reaching emotional consequences of disablement (Carstensen et al. 2000).
Additionally, studies of psychological adjustment to functional decline typically use retrospective assessments capturing psychological well-being over an extended time period, such as the past week (Bierman 2012; Bookwala and Franks 2005; Warner and Kelley-Moore 2012). Retrospective measures may be more susceptible to recall and positivity biases than momentary measures capturing current emotional state, especially among older adults (Stone and Mackie 2014). Retrospective measures may not adequately capture older adults’ negative emotions, given their tendency to recall more positive than negative information, and offer more positive recollections than their younger counterparts (Reed and Carstensen 2012). Thus, we focus on the link between disability and two positive (happy, calm) and three negative (frustrated, sad, worried) emotions experienced while engaged in activity on the diary day, as well as aggregated negative and positive mood scales. We conduct supplementary analyses using a life satisfaction measure, to explore the distinctive ways that discrete daily emotions (versus an evaluative measure of well-being) may respond to functional impairment.
Intimate Relationships as a Moderator of Disablement-Related Distress
Research drawing on stress buffering (Cohen and Wills 1985) and stress process (Pearlin 1999) models suggests that the emotional toll imposed by later-life disablement is less acute for persons who possess coping resources, especially social support. The adverse psychological consequences of disablement are buffered for persons who are married versus unmarried (Bierman 2012), who receive informal versus formal support (Chan et al. 2011), and who receive higher versus lower levels of emotional support in their marriages (Bookwala 2011; Mancini and Bonanno 2006). This support may foster a positive reinterpretation of one’s adverse experiences, or may provide resources needed to renegotiate physical challenges and readjustments to one’s social roles and activities (Cohen and Wills 1985).
Supportive marital relations may be a particularly crucial resource for coping with disablement and impairment. Marriages marked by high levels of support, understanding, and warmth, and low levels of criticism and conflict, may engender effective problem-solving, responsiveness to the ailing partner’s needs, and communication that conveys care and nurturance (Bookwala 2011; Choi and Marks 2006; Mancini and Bonanno 2006). Marriage or marriage-like relationships are a particularly salient source of emotional support in later life. With advancing age, older adults pare down the number of social contacts they maintain and grow increasingly reliant on their spouse/partner (Lang and Carstensen 2002).
Although a handful of studies suggest that marital support may buffer against the deleterious psychological consequences of disablement (Bookwala 2011; Mancini and Bonanno 2006), important questions remain unaddressed. First, prior studies have focused primarily on positive aspects of marriage, such as marital satisfaction (Bookwala 2011), or have used aggregated scales that do not differentiate strain versus support (Mancini and Bonanno 2006). This is an important limitation, as negative aspects of intimate relationships are more salient to one’s emotional health than positive aspects, especially in later life (Choi and Marks 2008; Proulx, Helms, and Buehler 2007). Older spouses report more frequent positive and less frequent negative interactions than younger couples (Henry et al. 2007) and are more likely to avoid conflict (Birditt and Fingerman 2005), rendering these atypical negative interactions highly salient to one’s emotional well-being.
Marital strains may intensify the negative emotional consequences of disablement via a process of stress amplification (Ingersoll-Dayton et al. 1997) or exacerbation (August, Rook, and Newsom 2007). These models suggest that stressors experienced simultaneously are more detrimental to well-being than individual or isolated stressors because accumulated strains may undermine one’s capacity to cope. Strained or conflicted interpersonal relations are one of the most powerful sources of chronic stress. Although the direct effects of relationship strain, and especially marital strain, for emotional well-being are widely documented (Proulx et al. 2007; Rook 1984), few studies explore the extent to which conflicted relationships amplify the harmful effects of other chronic and acute stressors. Amplification may occur in two ways: relationship conflict may be especially upsetting in high-stress contexts, such as managing one’s own functional limitations, or strained relationships may intensify the emotional toll of impairment by undermining one’s sense of competence or failing to provide sufficient support (August et al. 2007).
Studies exploring the extent to which negative aspects of marriage moderate the effects of disablement on well-being have yielded conflicting results. Bookwala and Franks (2005) found that more frequent disagreements intensified the effects of disability on depressive symptoms, whereas Warner and Kelley-Moore (2012) found no evidence that marital strain moderated the effect of activity limitations on older adults’ loneliness. Thus, we evaluate the extent to which positive (e.g., support) and negative (e.g., criticism) aspects of one’s intimate relationship moderate the effects of disablement on discrete daily emotions. We expect that strain will exacerbate whereas support will mitigate against the distressing effects of disablement, consistent with core themes of stress process and amplification models.
Research on the stress-buffering effects of relationship quality has a further limitation; it focuses exclusively on married persons. Although marriage is by far the most common romantic relationship among current cohorts of older adults, rates of cohabitation and long-term dating (e.g., “living apart together”) have risen steeply over the past two decades (Brown, Lee, and Bulanda 2006). DUST assesses the quality of intimate relationships for unmarried persons in cohabiting or dating relationships, so we include these often neglected subpopulations in our analysis. This is an important consideration because married persons have lower rates of disablement than their unmarried counterparts (Caputo and Simon 2013); studies focused on married persons only are based on disproportionately healthier subsamples. Thus, all analyses adjust for whether one is in a married, cohabiting, or dating relationship.
Gender Differences in the Moderating Effects of Relationship Quality
We also explore gender differences in the extent to which relationship quality buffers against or amplifies the effects of disablement on daily emotions. Few studies have explored this question, despite strong theoretical claims that the protective (or distressing) effects of relationship support (or strain) might vary by gender (Bloch, Haase, and Levenson 2014; Boerner et al. 2014).We expect that strain and support will play stronger moderating roles for men than women, reflecting gendered patterns of support among older adults. Men are typically reliant on their wives/partners for personal care, and are less likely to extend beyond the romantic dyad for emotional and instrumental support (Bierman 2012; Katz, Kabeto, and Langa 2000). Women play a more active role than men in communicating, instigating change in a partner’s behavior, initiating and pursuing disagreements, and conveying concerns about the relationship (Bloch et al. 2014; Carr et al. 2016); these potentially distressing conversations may exacerbate the negative emotions associated with men’s impairment. Men, by contrast, take a more passive approach to addressing relationship issues; their feelings toward the relationship may not be clearly transmitted to their partner and thus may be less consequential in moderating the effects of disablement on emotional well-being (Bloch et al. 2014).
In sum, we use daily diary data from DUST to investigate: (1) the extent to which the association between disability and daily emotion is moderated by marital/partner support and strain; and (2) whether such patterns differ significantly by gender. We measure disability with an indicator of impairment severity quartile, given research documenting a non-linear association between disablement and well-being (Chan et al. 2011). Analyses are adjusted for two other aspects of the disablement process: the presence of any disability, and duration of the limiting condition.
Our analyses also are adjusted for other coping resources (or liabilities) that may confound the associations among relationship quality and daily emotions, including the personality traits neuroticism and agreeableness, which are associated with the dispositional tendency to offer positive versus negative appraisals of one’s experiences and relationships (Gunthert, Cohen, and Armeli 1999). We control for emotional support from other family members, which may have direct effects on daily emotions, and may reduce the relative importance of intimate partner support (McIlvane and Reinhardt 2001). All analyses are adjusted for demographic and socioeconomic factors that are well established correlates of disablement, relationship quality, and emotional well-being (Choi and Marks 2008; Freedman et al. 2012). Finally, we control for characteristics of the specific activities to which one was referring when describing their emotions on the diary day; the daily emotion measures capture feelings while performing up to three randomly selected activities.
DATA AND METHODS
Data
Data were from the 2013 Disability and Use of Time (DUST) supplement to the 2013 Panel Study of Income Dynamics (PSID). The PSID started in 1968 and is the longest running longitudinal study of a representative sample of families in the United States. The original sample included 18,000 individuals in approximately 5,000 families. All respondents from the original sample and anyone born to or adopted by one of these families have been followed. From 1968 to 1997, families were interviewed annually and since 1997 biennially. Reinterview rates surpass 95% and the sample of families now exceeds 9,000. Adult children who have left their parents’ households have been followed. With the use of sampling weights, the design produces a nationally representative cross-section of families annually (McGonagle et al. 2012).
The DUST supplement was administered to households in which the head or partner was age 60 or older as of December 31, 2012 (Freedman and Cornman 2015). Spouses or partners also were interviewed, regardless of their age. Each respondent and spouse/cohabiting partner was interviewed twice by telephone about one randomly selected weekday and weekend day. Spouses/partners were interviewed about the same day. Of the 1,698 eligible households, 1,217 completed at least one interview, for a response rate of 71.7%.
The DUST instrument is a 30 to 40 minute diary, which was paired during the first of two interviews with a 15 to 20 minute supplemental questionnaire which assessed global and activity-related well-being, functioning, personality, relationship quality, and time use. To obtain a balanced sample of days, respondents were systematically assigned interview days that would yield one weekday and one weekend diary. The diary asked about all activities on the previous day, beginning at 4 a.m. and continuing until 4 a.m. the day of the interview. Respondents also reported how they felt while doing up to three activities randomly selected from their diaries, a validated approach to measuring activity-related emotion known as the Day Reconstruction Method (Kahneman et al. 2004).
For 1,776 respondents, 3,505 diaries were completed, yielding momentary emotion reports for 9,955 randomly selected activities. We excluded 167 spouses and partners under age 60, and 447 unpartnered persons, to ensure that our sample represents older adults (ages 60 and older) who are married, cohabiting, or in a romantic relationship. The final analytic sample comprised 1,162 respondents reporting on 6603 activities. Of the 6603 activity reports, 3415 were provided by 609 men and 3188 by 553 women.
Measures
Activity-related daily emotions
Our dependent variables were positive and negative emotion measures, which capture how happy, calm, frustrated, sad, and worried one felt while doing each of the three randomly selected diary activities. Response categories ranged from 0 (not at all) to 6 (very). Zero order correlations among the five items ranged from −0.28 (calm and sad) to 0.60 (sad and worried), suggesting that each represents a statistically and conceptually distinct emotion. We also constructed a positive emotion index, which summed responses for happy and calm, and a negative emotion index which summed responses to sad, frustrated and worried. We conducted supplementary analyses using the measure: “taking all things together, how satisfied are you with your life these days?” Response categories ranged from 0 (not at all) to 6 (very). This measure offered an overall evaluation of one’s life, whereas the other outcomes captured one’s mood when performing an activity on the diary day.
Marital/romantic relationship quality
Relationship quality was assessed with six items drawn from a standardized instrument reflecting both strain and affective support (Schuster, Kessler, and Aseltine 1990). Married persons were asked about their relationship with their spouse, cohabitants rated their cohabiting partner, and persons in a non-coresidential romantic relationship evaluated their romantic partner. Support (α = 0.75) indicated how much: “you can open up to your spouse/partner if you need to talk about your worries,” “your spouse/partner appreciates you,” and “your spouse/partner understands the way you feel about things.” Strain (α = 0.72) referred to how much your spouse/partner: “argues with you,” “makes you feel tense,” and “gets on your nerves.” Response categories ranged from 1 (not at all) to 4 (a lot). Responses were averaged and higher values reflected more of an attribute.
Markers of disablement
Severity of impairment
Severity of impairment was constructed from questions assessing whether respondents experienced common impairments in the last seven days, and if so, on how many days the impairment limited their activities (none, 1-2 days, 3-4 days, 5 or more days). Impairments included: breathing problems; heart or circulation problems; stomach problems; back or neck problems; limited strength or movement in one’s shoulders, arms, or hands; limited strength or movement in one’s hips, legs, knees, or feet; low energy or easily exhausted; and difficulty remembering everyday things. These items formed a one-factor severity scale (ranging from 0 to 32, α = 0.75), with all but two factor loadings exceeding 0.40 (stomach problems and memory problems, which we retained for completeness). We recoded continuous scores into quartiles, consistent with prior work detecting nonlinear associations between impairment severity and well-being (Chan et al. 2011).
Presence of a disability
Presence of a disability was measured using six items developed for the U.S. Census and the companion American Community Survey (ACS) to identify the U.S. population with disabilities (Weathers 2005). Respondents indicated whether they experienced each of the following: serious difficulty hearing; serious difficulty seeing even when wearing glasses; serious difficulty concentrating, remembering or making decisions because of a physical, mental or emotional condition; serious difficulty walking or climbing stairs; difficulty dressing or bathing; difficulty doing errands alone such as visiting a doctor’s office or shopping because of a physical, mental, or emotional condition. A dichotomous measure indicated the presence of any disability. The correlation between this measure and impairment severity was 0.48, suggesting each captures distinct aspects of disablement.
Duration of underlying limiting conditions
Duration of underlying limiting conditions was calculated from items on the 1999 to 2013 core PSID waves. Every two years respondents were asked whether a doctor ever told them they have a given condition (e.g., diabetes, arthritis) and, if so, whether it limits their normal daily activities a lot, somewhat, just a little or not at all. We identified limiting conditions as those that limit activities “a lot” or “somewhat.” For respondents reporting a limiting condition in 2013, we identified the earliest year in which the condition was reported and calculated the duration.
Sociodemographic and psychosocial controls
We controlled for factors that may confound associations among the disablement measures, relationship quality, and daily emotion. First, we controlled for two personality attributes: neuroticism and agreeableness. Neuroticism (α = 0.66) reflects how much one reported that they worry, are nervous, and handle stress well (reverse-coded).1 Agreeableness (α = 0.45) refers to how much a respondent felt they are forgiving, kind, and rude (reverse-coded). Responses categories were not at all, a little, some, or a lot. Items were drawn from a brief version of the Big 5 personality assessment (Gerlitz and Schupp 2005). Second, we controlled for quality of family relationships beyond the spouse/partner dyad (α = 0.47); respondents reported how much (not at all, a little, some, a lot) their families appreciate them, argue with them (reverse-coded), are too demanding (reverse-coded), and can be relied on. Responses were averaged, and higher values reflect more positive assessments.
Demographic characteristics included marital status (cohabiting/romantic relationship vs. married), age (in five year age groups), gender, race (black/not black), and number of living children. Our unmarried category combined cohabiting and dating persons as the sample sizes of 41 and 70, respectively, are too small to be treated separately. Socioeconomic status characteristics included educational attainment, 2012 family income (in quartiles), and 2013 family wealth (in quartiles); the latter two were drawn from the 2013 PSID. The PSID collects detailed information about taxable income (e.g., earnings) and cash transfers (e.g., Social Security benefits) received by the head, spouse and other adult family members. Assets referred to the value of nine resources/liabilities such as home equity and debt. Missing components for income and wealth were imputed (Heeringa et al. 2013). The two measures were moderately correlated (r = 0.56).
Activity characteristics
Because daily emotion was assessed in the context of diary day activities, we controlled for whether the activity was performed at home (vs. elsewhere), with whom the activity was done (with a spouse/cohabiting or romantic partner, with others; reference category was alone/not ascertained); whether the respondent considered the diary day to be a typical day; and which of 11 categories best captured the nature of the activity (work, volunteering, caregiving, socializing, exercise, going out, laundry, household chores, cooking, financial management, shopping).
Missing data were minimal; across our study’s focal variables (i.e., disablement, relationship quality, daily emotion), 2.9% (n=21) or fewer respondents were missing data on any one measure. Given the low levels of missing data (and trivial impact on variance estimates), we used mean imputation rather than more complex multiple imputation techniques.
Analytic Strategy
We first provide descriptive statistics for all measures, and assess gender differences using t-tests (continuous measures) or Chi square tests (categorical measures). Second, we evaluate the main effects of disablement and relationship support and strain on each of the five activity-related emotions, and the two summed measures using multilevel linear regression, which accounts for clustering of random activities within individuals. Models were estimated separately for men and women, and gender differences in coefficients were tested with interaction terms (and denoted with superscripts).Third, we evaluated two-way interaction terms between impairment severity and relationship support and strain, to assess moderation effects. We present and discuss interaction terms for the highest impairment severity quartile only, as it was the only statistically significant two-way interaction term of those estimated. This is consistent with prior work showing that buffering effects are most pronounced in high stress contexts (Chan et al. 2011; Mancini and Bonanno 2006). Finally, we evaluated whether the main effects of severity and relationship quality, and two-way interactions between the two (i.e., moderation analyses) differed significantly by gender. Analyses were run in Stata 14.1 and were weighted. Sampling weights took into account sample design and adjusted for nonresponse (Freedman and Cornman 2015).
RESULTS
Bivariate Analyses
Table 1 shows levels of each discrete emotion, by gender. Respondents report high levels of positive emotions including happy and calm (M=4.96 and 5.33 out of 6, respectively), and relatively low levels of frustration, worry and sadness (M=0.79, 0.52, and 0.37, respectively). Women report significantly higher levels of sadness compared to men (0.43 vs. 0.30, p < .05). Life satisfaction levels are high (M=5.1), and do not differ by gender.
Table 1.
Activity-Related Emotion and Life Satisfaction by Gender Among Older Persons Who Are Married, Cohabiting, or in a Romantic Relationship, DUST 2013
| Total | Male | Female | ||||
|---|---|---|---|---|---|---|
|
| ||||||
| Mean | Standard deviation | Mean | Mean | t-test | p-value | |
| Life satisfaction | 5.11 | 0.99 | 5.10 | 5.12 | 0.30 | 0.76 |
| Activity-related emotion | ||||||
| (Range: 0 to 6) | ||||||
| Happy | 4.96 | 1.18 | 4.95 | 4.96 | 0.17 | 0.866 |
| Calm | 5.33 | 1.17 | 5.33 | 5.33 | −0.05 | 0.963 |
| Positive Affect (0-12) | 10.29 | 2.03 | 10.28 | 10.29 | 0.08 | 0.937 |
| Frustrated | 0.79 | 1.48 | 0.77 | 0.81 | 0.63 | 0.526 |
| Worried | 0.52 | 1.19 | 0.50 | 0.53 | 0.72 | 0.471 |
| Sad | 0.37 | 1.07 | 0.30 | 0.43 | 2.46 | 0.014 |
| Negative affect (0-18) | 1.67 | 3.03 | 1.56 | 1.77 | 1.43 | 0.153 |
| Weighted % of respondents | 100 | 49 | 51 | |||
Notes: Positive affect is the summed score of happy and calm. Negative affect is the summed scores for frustrated, sad, and worried.
Sample size comprises 6601 activities from 1162 respondents; 3414 activities were provided by 609 men and 3187 reports by 553 women.
Table 2 shows that a substantial share (43%) of older persons have any disability. The duration of one’s limiting condition averages slightly over two years for women and slightly under for men (2.3 vs. 1.7 years, p < .01). Women are more likely than men to be in the upper two quartiles of impairment severity, although these differences are only marginally significant. Men report significantly better quality relationships than women, with higher levels of spousal support (3.6 vs. 3.4, p < .001) and lower levels of strain (2.1 vs. 2.2, p < .01). Men and women do not differ with respect to marital status; 9.3% are in a nonmarital partnership. Men and women also differ with respect to coping resources. Women have the disadvantage of higher neuroticism scores (1.3 vs. 1.0, p < .01), yet the advantages of higher levels of agreeableness (2.6 vs. 2.4, p < .01) and support from other family members (3.4 vs. 3.3, p < .05).
Table 2.
Means (Standard Deviations) and Proportions by Gender Among Older Persons who are Married, Cohabiting, or in a Romantic Relationship, DUST 2013
| Total | Male | Female | Sig. | |
|---|---|---|---|---|
| Disablement | ||||
| Any disability | 43.1 | 43.9 | 42.2 | |
| Severity of impairments | ||||
| Quartile 1 (lowest) | 30.0 | 33.2 | 26.3 | |
| Quartile 2 | 24.6 | 24.9 | 24.1 | |
| Quartile 3 | 28.1 | 27.2 | 29.1 | |
| Quartile 4 (highest) | 17.4 | 14.6 | 20.5 | |
| Duration of limiting condition (years) | 2.0 (4.2) | 1.7 (3.8) | 2.3 (4.7) | ** |
| Marital/Romantic Relationship Quality | ||||
| Overall relationship quality (Range: 0-4) | 3.2 (0.6) | 3.2 (0.5) | 3.1 (0.6) | ** |
| Support | 3.5 (0.6) | 3.6 (0.5) | 3.4 (0.6) | ** |
| Strain | 2.2 (0.7) | 2.1 (0.7) | 2.2 (0.7) | ** |
| Psychosocial Resources | ||||
| Neuroticism (Range: 0-3) | 1.1 (0.7) | 1.0 (0.7) | 1.3 (0.7) | ** |
| Agreeableness (Range: 0-3) | 2.5 (0.5) | 2.4 (0.5) | 2.6 (0.4) | ** |
| Family relationship quality (Range: 0-4) | 3.3 (0.6) | 3.3 (0.6) | 3.4 (0.6) | * |
| Demographic Characteristics | ||||
| Age (years) | ||||
| 60-64 | 34.7 | 31.3 | 38.4 | * |
| 65-69 | 27.1 | 27.2 | 27.0 | |
| 70-74 | 15.6 | 14.7 | 16.8 | |
| 75-79 | 11.1 | 13.2 | 8.8 | |
| 80+ | 11.5 | 13.6 | 9.0 | |
| Black (vs. not black) | 6.4 | 6.4 | 6.5 | |
| Cohabiting/romantic partner (vs. married) | 9.3 | 9.0 | 9.7 | |
| Number of living adult children | 2.8 (1.7) | 2.8 (1.6) | 2.8 (1.7) | |
| Socioeconomic Status | ||||
| Education | ||||
| < 12 years | 8.9 | 9.6 | 8.2 | ** |
| 12 years | 28.7 | 22.2 | 36.0 | |
| >12 years | 62.4 | 68.2 | 55.8 | |
| Family Income, 2012 | ||||
| 1st quartile (lowest) | 14.5 | 13.4 | 15.7 | |
| 2nd quartile | 25.7 | 25.0 | 26.6 | |
| 3rd quartile | 28.0 | 28.3 | 27.7 | |
| 4th quartile | 31.8 | 33.4 | 30.0 | |
| Wealth, 2013 | 31.8 | 33.4 | 30.0 | |
| 1st quartile (lowest) | 17.6 | 16.6 | 18.7 | |
| 2nd quartile | 22.6 | 23.2 | 21.9 | |
| 3rd quartile | 29.0 | 29.1 | 28.8 | |
| 4th quartile | 30.9 | 31.1 | 30.6 | |
| Activity Characteristics | ||||
| Activity type – activities done yesterday | ||||
| Work for pay | 8.8 | 12.0 | 5.7 | ** |
| Volunteer | 0.8 | 1.1 | 0.4 | |
| Care for others | 2.4 | 2.0 | 2.8 | |
| Socialize | 5.1 | 3.9 | 6.2 | ** |
| Exercise | 2.8 | 3.2 | 2.5 | |
| Go out for pleasure | 2.7 | 3.1 | 2.4 | |
| Laundry | 1.1 | 0.4 | 1.7 | ** |
| Household chores | 7.6 | 8.4 | 6.9 | |
| Prepared food | 8.3 | 4.7 | 11.7 | ** |
| Financial management | 2.1 | 1.7 | 2.4 | |
| Shopping/errands | 9.1 | 8.2 | 10.0 | |
| With whom activity was performed | ||||
| Alone or N/A | 57.2 | 57.2 | 57.2 | ** |
| With spouse | 30.7 | 32.9 | 28.5 | |
| With others | 12.2 | 10.0 | 14.3 | |
| Activity done at home (vs. other places) | 53.9 | 48.8 | 58.8 | ** |
| Yesterday was typical (vs. not) | 64.0 | 68.0 | 60.2 | ** |
Note: t-tests were conducted for continuous measures and χ2 tests for categorical measures. In correcting for survey design, Stata converts the χ2 test of independence into an F-test. Statistically significant gender differences denoted as:
p < .05 and
p < .01. Sample size for activity reports is 6601 activities from 1162 respondents.
Multivariate Analyses
Main effects analysis
In Table 3, Model 1 shows a statistically significant association between impairment severity and positive emotions, where successive quartiles of severity are associated with significantly lower levels of happiness, calm, and overall positive emotion (relative to those in the lowest quartile). For example, the far left panel shows a monotonic effect of impairment severity on happiness for both men (b = −0.20, −0.42, and −0.53), and women (b = −0.15, −0.27, −0.70), relative to the lowest severity quartile. The effects of impairment do not differ by gender at lower levels of severity, although the effect for the top quartile of severity is significantly larger for women than men for all three positive outcomes. We also found an inverse association between impairment severity and life satisfaction, although effects did not differ by gender (tables available from authors).
Table 3.
Summary of Multi-level Regression Models Evaluating Effects of Disablement and Marital/Romantic Relationship Quality on Positive Activity-Related Emotion by Gender
| Happy | Calm | Positive Affect | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | |||||||
| M | W | M | W | M | W | M | W | M | W | M | W | |
| Disability | ||||||||||||
| Has a disability (vs. not) | .08 (.08) |
.08 (.05) |
.08 (.08) |
.07 (.04) |
.08 (.09) |
−.07 (.08) |
.08 (.09) |
−.07 (.08) |
.16 (.17) |
.00 (.13) |
.16 (.17) |
−.01 (.12) |
| Severity of Impairment: Quartile | ||||||||||||
| 2nd | −.20** (.07) |
−.15 (.17) |
−.21** (.06) |
−.15 (.17) |
−.08 (.17) |
−.16** (.01) |
−.09 (.17) |
−.15** (.00) |
−.29** (.10) |
−.31 (.18) |
−.29** (.11) |
−.31 (.17) |
| 3rd | −.42** (.04) |
−.27* (.12)b |
−.42** (.04) |
−.28* (.12)b |
−.17** (.02) |
−.26** (.05) |
−.18** (.02) |
−.27** (.08) |
−.59** (.03) |
−.53** (.17) |
−.60** (.02) |
−.54** (.20) |
| 4th (top) | −.53** (.03) |
−.70** (.12)a |
−1.67 (1.95) |
−1.46 (1.70) |
−.15* (.06) |
−.57** (.11)a |
1.32* (.62) |
−.05 (.94) |
−.68** (.02) |
−1.26** (.01)a |
−.36 (2.60) |
−1.51 (2.62) |
| Duration of disability (years) | .01 (.01) |
.01 (.01) |
.01 (.01) |
.01 (.01) |
−.00 (.01) |
.02** (.01) |
−.01 (.02) |
.02** (.01) |
.00 (.02) |
.02 (.01) |
.00 (.02) |
.03* (.01) |
| Quality Romantic Relationship | ||||||||||||
| Support | .12 (.09) |
.29** (.02)a |
.08 (.15) |
.23** (.05) |
.12 (.09) |
.11 (.08) |
.17 (.09) |
.12 (.09) |
.24 (.18) |
.39** (.06) |
.24 (.25) |
.35* (.14) |
| Strain | −.14 (.13) |
−.03 (.14)a |
−.16 (.17) |
−.03 (.08) |
−.12 (.14) |
−.06* (.03) |
−.08 (.18) |
−.02 (.11) |
−.26 (.26) |
−.09 (.12) |
−.24 (.35) |
−.06 (.04) |
| Marital Status | ||||||||||||
| Romantic partner (vs. married) | .02 (.02) |
−.13** (.03)a |
.02 (.02) |
−.13** (.01)a |
−.17 (.09) |
.01 (.15)a |
−.17 (.10) |
.02 (.16)a |
−.16* (.07) |
−.11 (.12) |
−.16 (.09) |
−.11 (.15) |
| Interactions | ||||||||||||
| Impair Q4 × support | .23 (.38) |
.21 (.33) |
−.27** (.04) |
−.04 (.02)a |
−.03 (.42) |
.17 (.35) |
||||||
| Impair Q4 × strain | .15 (.27) |
.02 (.30) |
−.24 (.23) |
−.16 (.33) |
−.10 (.51) |
−.14 (.63) |
||||||
| Constant | 4.42** (.63) |
3.63** (.75) |
4.59** (.91) |
3.81** (.43) |
4.55** (.61) |
5.13** (.35) |
4.35** (.68) |
5.05** (.48) |
8.99** (1.23) |
8.78** (.42) |
8.95** (1.59) |
8.87** (.04) |
Notes:
p < .05 and
p < .01.
Models run separately by gender, M denotes men, W women. Model 1 includes main effects of relationship quality, severity of impairment, and all controls. Model 2 adds interaction effect of relationship quality by highest quartile of impairment severity. All models adjusted for age, race, and education, number of children, marital status, neuroticism, agreeableness, family support, education, income, wealth, and characteristics of activities. Gender differences in coefficients were assessed by pooling male and female samples and estimating models with covariates and interaction terms interacted with gender… Statistically significant differences (p < .05) are denoted with the superscript a and marginally significant differences (p < .10) are denoted with superscript b.
Table 4 shows that, relative to those in the lowest quartile, those in the most severe impairment quartile have significantly elevated levels of frustration (b =0 .45 and 0.41), worry (b=0.22 and 0.55), sadness (b=0.23 and 0.45), and overall negative mood (b = 0.87 and 1.45) among men and women respectively. We find significantly larger effects among women for the outcome of worry only.
Table 4.
Summary of Regression Models Evaluating Effects of Disablement and Marital/Romantic Relationship Quality on Negative Activity-Related Emotion by Gender.
| Frustration | Worry | Sad | Negative Affect | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||||||
| Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | |||||||||
| M | W | M | W | M | W | M | W | M | W | M | W | M | W | M | W | |
| Disability | ||||||||||||||||
| Has a disability (vs. not) | −.07 (.14) |
.10 (.09) |
−.07 (.13) |
.12 (.12) |
.09 (.12) |
−.06 (.07)a |
.09 (.12) |
−.04 (.03) |
−.05 (.07) |
−.07 (.08)a |
−.05 (.06) |
−.04 (.04) |
−.03 (.33) |
−.02 (.05) |
−0.04 (0.30) |
0.04 (0.06) |
| Severity of Impairment: Quartile | ||||||||||||||||
| 2nd | −.00 (.09) |
.08** (.02) |
.01 (.08) |
.08** (.01) |
.08 (.10) |
.25** (.03) |
.09 (.10) |
.25** (.03) |
.07 (.06) |
.14** (.05) |
.07 (.05) |
.14** (.05) |
.16 (.26) |
.46** (.09) |
0.18 (0.23) |
0.47** (0.09) |
| 3rd | .13 (.17) |
.28** (.02) |
.14 (.17) |
.27** (.01) |
.07** (.01) |
.30** (.09)a |
.08** (.01) |
.29** (.08)a |
.11** (.03) |
.14 (.11) |
.11** (.03) |
.13 (.10) |
.32 (.20) |
.72** (.18) |
0.34 (0.19) |
0.69** (0.17) |
| 4th (top) | .41** (.07) |
.45** (.07) |
−2.76** (.75) |
1.62** (.27)a |
.22** (.07) |
.55** (.01)a |
−1.85** (.38) |
2.27 (1.30)a |
.23 (.22) |
.45** (.05) |
−1.95** (.29) |
2.80** (.47)a |
.87* (.36) |
1.45** (.03) |
−6.44** (0.74) |
6.63** (0.62)a |
| Duration of disability (years) | .00 (.02) |
.00 (.00) |
.01 (.02) |
.00 (.00) |
−.00 (.02) |
.01 (.01) |
−.00 (.02) |
.01 (.01) |
.01 (.02) |
−.00 (.01) |
.01 (.02) |
.00 (.01) |
.00 (.05) |
.01 (.03) |
0.01 (0.05) |
0.02 (0.02) |
| Quality Romantic Relationship | ||||||||||||||||
| Support | −.06** (.01) |
−.27* (.11) |
−.15** (.02) |
−.21** (.06) |
−.02 (.13) |
−.13 (.10) |
−.08 (.12) |
−.05** (.01) |
−.08 (.05) |
−.15* (.07) |
−.14** (.05) |
−.03 (.04) |
−.16 (.18) |
−.55 (.28) |
−0.36* (0.15) |
−0.28** (0.10) |
| Strain | .13 (.13) |
.09 (.06) |
.03 (.13) |
.14** (.01) |
.09 (.13) |
.05** (.01) |
.02 (.13) |
.12** (.04) |
.08 (.09) |
.02 (.01) |
.01 (.10) |
.10** (.00) |
.30 (.35) |
.16* (.07) |
0.06 (0.36) |
0.36** (0.07) |
| Marital Status | ||||||||||||||||
| Romantic partner (vs. married) | .08 (.26) |
.09 (.08) |
.10 (.26) |
.10 (.07) |
.14 (.07) |
.03* (.01) |
.15* (.07) |
.05* (.02) |
−.05 (.13) |
.08 (.14) |
−.04 (.12) |
.10 (.15) |
.15 (.46) |
.19*** (.05) |
0.19 (0.45) |
0.25** (0.06) |
| Interactions | ||||||||||||||||
| Impair Q4 × support | .51** (.19) |
−.23* (.10)a |
.35** (.09) |
−.33 (.31)b |
.35** (.03) |
−.46*** (.06)a |
1.17** (0.24) |
−1.01** (0.34)a |
||||||||
| Impair Q4 × strain | .62** (.08) |
−.17 (.23)a |
.38** (.06) |
−.26* (.12)a |
.43** (.02) |
−.35* (.14)a |
1.44** (0.13) |
−0.78** (0.24)a |
||||||||
| Constant | 1.29** (.13) |
.80* (.36) |
1.72** (.02) |
.56 (.42) |
.61 (.81) |
.37 (.19) |
.89 (.75) |
.03 (.17) |
.41 (.61) |
.39 (.58) |
.70 (.64) |
−.09 (.56) |
2.23 (1.51) |
1.57** (.38) |
3.22* (1.39) |
0.51** (0.07) |
Notes:
p < .05 and
p < .01. Models run separately by gender, M denotes men, W women. Model 1 includes main effects of relationship quality, severity of impairment, and all controls. Model 2 further includes interaction effect of relationship quality by highest quartile of impairment severity. All models adjusted for age, race, and education, number of children, marital status, neuroticism, family support, education, income, wealth, and characteristics of activities. Gender differences in coefficients were assessed by pooling male and female samples and estimating models with covariates and interaction terms interacted with gender. Statistically significant differences (p < .05) are denoted with the superscript a and marginally significant differences (p < .10) are denoted with superscript b.
Associations between relationship quality and daily emotions reveal expected, albeit weak, patterns. Marital support is associated inversely with negative emotions and positively with positive emotions, yet few associations are statistically significant in the fully adjusted models. Support is significantly and inversely related to frustration among men and women, yet is inversely related to sadness and positively related to happiness and overall positive mood for women only. Similarly, marital strain is associated with significantly elevated worry and overall negative mood, and lower levels of calm for women only. Supplementary analyses show that marital support (b = .38 and .29, p < .01) and strain (b = −.20 and −.17, p < .05) are significantly related to life satisfaction among men and women, respectively. However, gender stratified analyses (not shown) reveal only one statistically significant gender difference: marital support is a stronger predictor of happiness among women relative to men (b = 0.29 vs. 0.12). In sum, our focal predictors reveal expected associations with the outcome measures, although impairment and marital/partner relations are more strongly linked to the emotions of women than men. By contrast, we do not find significant differences in the effects of impairment or marital quality on life satisfaction, considered an evaluative versus emotional aspect of well-being.
Moderation effects analysis
Our moderation analyses reveal that relationship quality significantly moderates the effects of top quartile impairment, but not the second or third quartiles. Significant moderation effects emerged for only one of the positive emotion outcomes: marital support moderates the effect of severe impairment for men’s (but not women’s) feelings of calm. Results are plotted in Figure 1, for ease of interpretation. For men in the lowest impairment quartile and women in both lowest and highest impairment quartiles, support has a slight protective effect on feelings of calm, indicated by the parallel lines. By contrast, support undermines, albeit slightly, feelings of calm among the most impaired men. In supplementary analyses, we found no significant differences between men and women in the moderation analyses for the outcome of life satisfaction.
Figure 1.
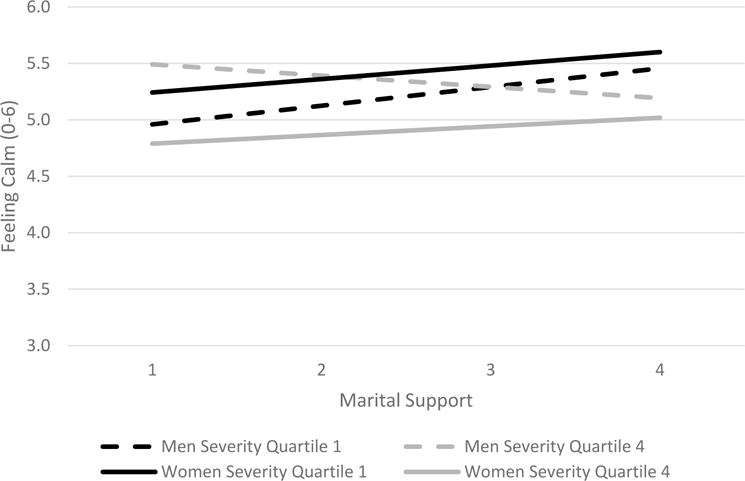
Feeling Calm – Interaction between Marital Support and Severity by Gender
We find strong evidence that relationship quality moderates the effect of severe impairment (top quartile) on negative emotions, yet these effects operate very differently for men and women. Models 2 in Table 4 show that two-way interaction terms between support and impairment severity are statistically significant for men and women for each of the four negative emotion outcomes, and the superscripts denote that these patterns differ significantly by gender. Spousal/partner support buffers against all four negative emotion outcomes for the most impaired women, a finding consistent with stress buffering perspectives. Support also has a modest protective effect for men and women in the lowest impairment quartile. As marital support increases, levels of frustration, worry, sadness, and overall negative emotion decline slightly among men and women in the lowest impairment category, and decline more steeply among women with highest impairment. In sharp contrast, support intensifies all four negative emotion outcomes among men with the most severe impairment.
For ease of interpretation, we plotted the results for frustration in Figures 2a & 2b. Among women with the most severe impairment, each one point increase in support is associated with a one-half point decrease in frustration. Highly impaired women with the lowest levels of marital support report frustration scores that are 1.4 points higher than their counterparts with the highest levels of support (2.2 vs. 0.8). By contrast, among highly impaired men, each one point increase in marital support is associated with a one-third point increase in frustration levels, with comparable patterns for the outcomes sadness, worry, and overall negative emotion.
Figure 2a.
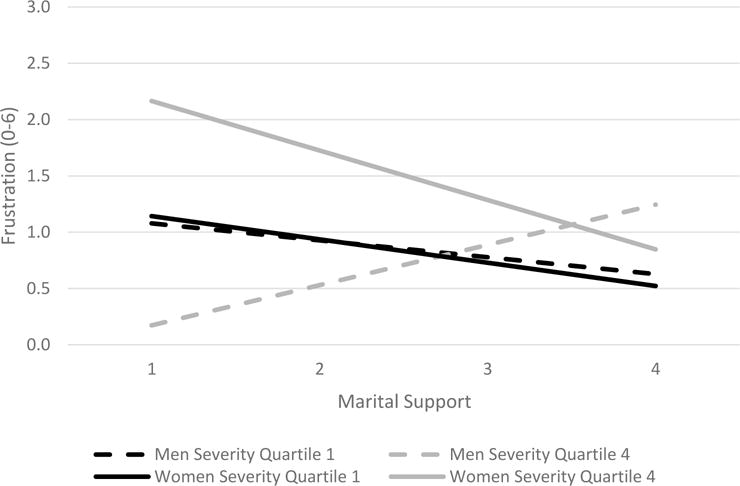
Feeling Frustrated – Interaction between Marital Support and Severity by Gender
Figure 2b.
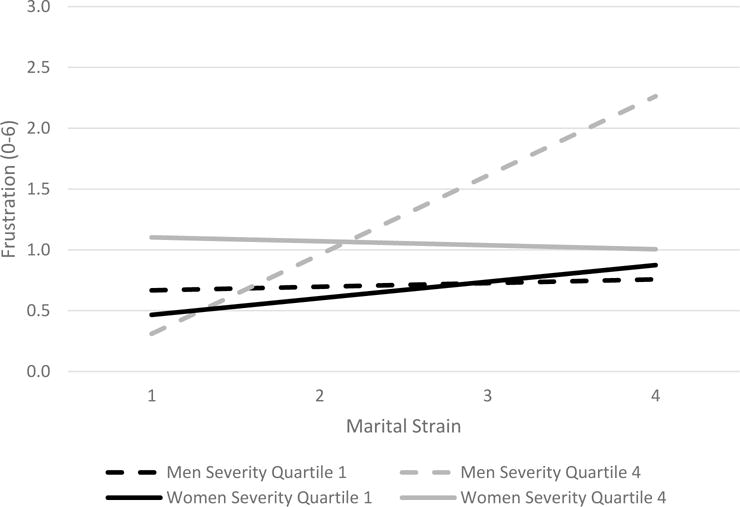
Feeling Frustrated – Interaction between Marital Strain and Severity by Gender
A different scenario emerges for relationship strain. Strain has a negligible effect on the negative emotions of men in the lowest impairment category and women, yet a sizeable effect on the negative emotions of the most impaired men. Comparable patterns emerge for the outcomes of sadness, worry, frustration, and overall negative emotion. Once again, we plot results for frustration as an exemplar. Figure 2b shows that the association between marital strain and frustration is virtually flat for low impairment men and all women. By contrast, each one point increase in marital strain is associated with a .7 point increase in the frustration levels of men in the highest impairment quartile. At the highest levels of marital strain, severely impaired men report frustration scores that are 1.5 points higher than their counterparts in the lowest impairment group (M=2.3 vs. 0.8). A comparable gap is not evidenced among women; at high levels of marital/relationship strain, the mean frustration levels of lowest- versus highest-impairment women are similar (M=0.9 vs. 1.0). Thus, the effects of severe impairment on men’s negative emotions are amplified as marital/romantic strain increases, and the deleterious effects of relationship strain are most acute among men with the most severe impairments.
DISCUSSION
Our study uses daily diary data to explore whether associations between disability and daily emotion are conditional upon marital/romantic partnership strain and support. Four key findings emerged. First, the severity of one’s impairment has far reaching effects on older adults’ daily emotions, with significantly larger effects for women than men across all three positive mood outcomes and one negative emotion (worry). These patterns may reflect gender differences in emotional display, where women feel freer to express emotions that suggest vulnerability, such as worry (Brody and Hall 2010). Older women also may be less likely than men to receive instrumental support from their partners, rendering disablement more distressing (Katz et al. 2000). We cannot fully explore this with DUST, as direct care from a romantic partner is assessed for coresidential partners only. We re-estimated all analyses for married and cohabiting partners only, and found that the effects of impairment on women’s daily emotions barely changed after controlling for the receipt of instrumental support from partner (results available from authors).
Second, we found strong evidence of stress buffering processes for women only. Relationship support buffers against feelings of frustration, sadness, worry, and negative mood and heightened feelings of calm among women with the most severe impairment. For example, among women with the lowest levels of marital support, those with highest impairment report frustration scores more than one point higher than their lowest-impairment counterparts, although this gap diminishes to less than a one-third point difference among women in highly supportive unions. Consistent with stress buffering perspectives, our results suggest that emotional support from one’s spouse or partner may foster a positive reinterpretation of one’s adverse experiences, or may provide older women with the emotional and instrumental resources needed to renegotiate physical challenges and readjustments to their social roles and activities (Bookwala 2011; Mancini and Bonanno 2006). We suspect that the protective effects of support for highly impaired women (but not men) may reflect gender differences in the experience and cultural meaning of help receipt. Quantitative and qualitative studies suggest that the receipt of spousal support is more salient to the well-being of older women than men, as they are more comfortable receiving support, especially under adverse conditions such as severe impairment (Acitelli and Antonucci 1994; Allen and Wiles 2004). Open-ended interviews with impaired older women suggest that “receiving support [is]… positioned as part of maintaining overall independence, rather than anathema to it” (Allen and Wiles 2004:677).
Third, marital/partner support does not buffer against negative emotion among older men. Rather, higher levels of marital support are associated with higher levels of frustration, sadness, worry, and overall negative emotion, and reduced feelings of calm among men with the most severe impairment. At first blush this finding is counterintuitive yet on closer inspection, two explanations are possible, although longitudinal data are required to sort out definitive answers. Wives and female partners may give greater support to men who are easily prone to frustration, sadness, and worry, or who are most troubled by their impairment.
Alternatively, the results may reveal a potentially “dark side” of social support for some older men (Rook 1984). Men with high levels of impairment may find their sense of independence and competence threatened by high levels of support (Allen and Wiles 2014; Galdas, Cheater, and Marshall 2005). These perceived threats to autonomy may be particularly relevant to the emotion of frustration, the outcome for which we detected the strongest patterns. Frustration is an emotional reaction to the thwarted pursuit of a personal goal; autonomy and self-determination may be such goals for older men (Berkowitz 1989). Some studies further suggest that intensive support, especially from a close significant other, may be detrimental to older men facing chronic stressors such as disablement. Spouses, especially wives, may become “overinvolved and overbearing” when offering support to their impaired partner, because their own quality of life also depends on the partner’s successful management of his impairment (Coyne, Wortman, and Lehman 1988). For men, in particular, this support and surveillance may undermine his sense of masculinity and autonomy, ultimately intensifying his negative emotions (Gerschick and Miller 1995).
Fourth, marital strain amplifies the effects of severe impairment among men only. Conversely, relationship strain is very weakly linked to negative emotions among women, and among men with minimal impairment. The effects of severe limitation on men’s sadness, frustration, and negative mood intensify as their reports of relationship strain increase. These patterns are consistent with research on stress amplification and exacerbation (August et al. 2007; Ingersoll-Dayton et al. 1997). Romantic relationships marked by strife may reduce one’s capacity to cope effectively with the chronic strains associated with disablement including social isolation, undermined sense of competence, and loss of satisfying activities such as hobbies or volunteering (Freedman et al. 2012).
Why did we find evidence of amplification among men only? We suspect these patterns reflect gender differences in the meaning and experience of marital strain in later life. Men are less likely than women to both notice and respond to marital difficulties (Carstensen, Gottman, and Levenson 1995), thus those who perceive and acknowledge strain may be particularly sensitive to their marriage’s emotional climate. Spouses are particularly salient to older men’s emotional lives, because their broader networks of coworkers, friends, and families decrease with advancing age (Lang and Carstensen 2002). Finally, criticism or demands from a wife may be well-intended health advice which, like support, may undermine his sense of competence and autonomy (Coyne et al. 1998).
Limitations
Our study has several limitations. First, although DUST is embedded in a longitudinal panel, our analysis used only contemporaneous measures of relationship quality and activity-related emotion. Therefore we cannot ascertain causal ordering; current emotions may bias appraisals of relationship quality (Schwarz and Strack 1999). Our concerns are partly allayed by a meta-analysis showing that the association between marital quality and well-being is stronger when well-being is the dependent variable (Proulx et al. 2007).
Second, we did not explicate the mechanisms through which relationships buffer against or intensify emotions associated with disablement-related stress. For instance, persons with emotionally strained relationships might receive ineffective personal care from their partners, compromising their ability to manage disablement. We conducted supplementary analyses among those co-residing with a partner, and controlled for the receipt of instrumental support from one’s partner due to one’s own health needs. The inclusion of this simple indicator did not alter our multivariate results. However, future studies could explore specific types of help given and the perceived effectiveness of this help in fostering one’s capacity to manage daily activities. Understanding how emotional and instrumental support together buffer against the strains of disablement is a fruitful area for future research.
Third, DUST does not include a general measure of emotional well-being, such as depressive symptoms (Radloff 1977), thus we could not evaluate whether patterns evidenced for activity-related mood differ from those detected with an aggregated or global measure. However, we replicated all analyses using a global life satisfaction measure. This measure was associated with impairment in expected ways, yet we found no evidence of gender differences either in effects of impairment, or in our moderation analyses. Global life satisfaction is a relatively stable orientation that captures how people evaluate their lives relative to some standard, such as their expectation for how life should be (Schwarz and Strack 1999). By contrast, activity-related emotions are assessments of lives as individuals live them. The two measures are highly correlated, yet life satisfaction is more responsive to enduring aspects of quality of life, such as impairment, whereas daily mood is more responsive to contemporaneous and immediate circumstances and thus provides a novel approach for understanding older adults’ daily emotional lives (Kahneman et al. 2004).
Despite these limitations, our study reveals the complex role that disablement and marital/partner relations play in the daily emotional lives of older adults – especially with respect to negative emotions including worry, sadness, and frustration. Although early work on emotional reactivity suggests that older adults are less likely to perceive or express negative emotions relative to younger persons, contemporary work using momentary measures reveals that discrete and complex emotions such as frustration and sadness are relatively common among older adults (Carstensen et al. 2000). However, little is known about how these emotions respond to age-related health declines including disablement and activity limitation (Chipperfield et al. 2003). Our study is among the first we know of to show gender differences in how impairment severity affects older adults’ daily emotions, and how these associations are conditioned by relationship strain and support. We find frustration to be a particularly promising yet rarely studied outcome in relationships and health research. Experimental social psychologists have found that persistent frustration may lead to aggressive thoughts or behaviors (Berkowitz 1989). Spouses who experience high levels of frustration may be at risk of aggressing against one another, especially if they have experienced age-related cognitive changes that diminish impulse control (Hall and O’Connor 2004). Frustration also may intensify with further declines in physical functioning, as older adults increasingly face obstacles to carrying out their hobbies and daily activities (Taylor and Lynch 2004). Programs targeting disabled older adults and their spouse/partner caregivers should consider the couple’s history of relationship strain, support, and conflict and the implications for emotional well-being.
Acknowledgments
An earlier version of this paper was presented at the 2016 annual meetings of the Population Association of America.
FUNDING
This research was funded by a grant from the National Institute on Aging, P01AG029409. The views expressed are those of the authors alone and do not represent the views of their employers or the funding agency.
Biographies
Deborah Carr is a professor of sociology and interim director of the Institute for Health, Health Care Policy, and Aging Research at Rutgers University. She is a life course sociologist whose research focuses on stress, health, and well-being over the life course. Her recent publications focus on later-life marriage and marital transitions, bereavement, and end-of-life issues. She is editor-in-chief of Journal of Gerontology: Social Sciences.
Jennifer Cornman is an independent research consultant. She is a social demographer whose research focuses on socioeconomic status, health, wellbeing and social support among older adults in the United States and Taiwan
Vicki A. Freedman is a research professor at the University of Michigan’s Institute for Social Research. Her research focuses on the consequences of population aging for disability, long-term care, and related public health issues. Her recent publications focus on late-life disability trends, time use and wellbeing in later life, the role of environmental factors in late-life health and disability, and associated measurement issues.
Footnotes
We also constructed a two-item neuroticism scale, dropping “worrisome” because of concerns about endogeneity with the worry measure of activity-related emotion. We use the three-item scale in our final analyses because the alpha is considerably better (0.66 vs 0.48). We re-estimated all multivariate analyses using the two-item scale, and coefficients of the focal variables did not change more than 10% in magnitude.
Contributor Information
Deborah Carr, Rutgers University.
Jennifer Cornman, Jennifer Cornman Consulting.
Vicki A. Freedman, University of Michigan
References
- Acitelli Linda K, Antonucci Toni C. Gender Differences in the Link between Marital Support and Satisfaction in Older Couples. Journal of Personality and Social Psychology. 1994;67(4):688–698. doi: 10.1037//0022-3514.67.4.688. [DOI] [PubMed] [Google Scholar]
- Allen Ruth ES, Wiles Janine L. Receiving Support When Older: What Makes it OK? The Gerontologist. 2014;54(4):670–682. doi: 10.1093/geront/gnt047. [DOI] [PubMed] [Google Scholar]
- Anderson Wayne L, Wiener Joshua M, Finkelstein Eric A, Armour Brian S. Estimates of National Health Care Expenditures Associated with Disability. Journal of Disability Policy Studies. 2011;21(4):230–240. [Google Scholar]
- August Kristin J, Rook Karen S, Newsom Jason T. The Joint Effects of Life Stress and Negative Social Exchanges on Emotional Distress. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2007;62(5):S304–S314. doi: 10.1093/geronb/62.5.s304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berkowitz Leonard. Frustration-aggression Hypothesis: Examination and Reformulation. Psychological Bulletin. 1989;106(1):59–73. doi: 10.1037/0033-2909.106.1.59. [DOI] [PubMed] [Google Scholar]
- Bierman Alex. Functional Limitations and Psychological Distress Marital Status as Moderator. Society and Mental Health. 2012;2(1):35–52. [Google Scholar]
- Bierman Alex, Denise Statland. Timing, Social Support, and the Effects of Physical Limitations on Psychological Distress in Late Life. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2010;65(5):S631–S639. doi: 10.1093/geronb/gbp128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Birditt Kira S, Fingerman Karen L. Do We Get Better at Picking our Battles? Age Group Differences in Descriptions of Behavioral Reactions to Interpersonal Tensions. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2005;60(3):P121–P128. doi: 10.1093/geronb/60.3.p121. [DOI] [PubMed] [Google Scholar]
- Bloch Lian, Haase Claudia M, Levenson Robert W. Emotion Regulation Predicts Marital Satisfaction: More than a Wives’ Tale. Emotion. 2004;14(1):130–144. doi: 10.1037/a0034272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boerner Kathrin, Jopp Daniela S, Carr Deborah, Sosinsky Laura, Kim Se-Kang. ’His’ and ‘Her’ Marriage? The Role of Positive and Negative Marital Characteristics in Global Marital Satisfaction among Older Adults. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2014;69(4):S579–S589. doi: 10.1093/geronb/gbu032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bookwala Jamila. Marital Quality as a Moderator of the Effects of Poor Vision on Quality of Life among Older Adults. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2011;66(5):S605–S616. doi: 10.1093/geronb/gbr091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jamila Bookwala, Franks Melissa M. Moderating Role of Marital Quality in Older Adults’ Depressed Affect: Beyond the Main-effects Model. Journal of Gerontology Series B: Psychological Sciences. 2005;60(6):S338–S341. doi: 10.1093/geronb/60.6.p338. [DOI] [PubMed] [Google Scholar]
- Brody Leslie R, Hall Judith A. Gender, Emotion, and Socialization. In: Chrisler JC, McCreary DR, editors. Handbook of Gender Research in Psychology. NY: Springer; 2010. pp. 429–454. [Google Scholar]
- Brown Susan L, Lee Gary R, Bulanda Jennifer Roebuck. Cohabitation among Older Adults: A National Portrait. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2006;61(2):S71–S79. doi: 10.1093/geronb/61.2.s71. [DOI] [PubMed] [Google Scholar]
- Caputo Jennifer, Simon Robin W. Physical Limitation and Emotional Well-being Gender and Marital Status Variations. Journal of Health and Social Behavior. 2013;54(2):241–257. doi: 10.1177/0022146513484766. [DOI] [PubMed] [Google Scholar]
- Carr Deborah, Cornman Jennifer C, Freedman Vicki A. Does Marital Quality Protect Against Distress? Marital Quality and Momentary Negative Mood in Later Life. Journal of Gerontology Series B: Psychological & Social Sciences. 2016;71:S177–S187. doi: 10.1093/geronb/gbv073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carstensen Laura L, Gottman John M, Levenson Robert W. Emotional Behavior in Long-term Marriage. Psychology and Aging. 1995;10(1):140–149. doi: 10.1037//0882-7974.10.1.140. [DOI] [PubMed] [Google Scholar]
- Carstensen Laura L, Monisha Pasupathi Ulrich Mayr, Nesselroade John R. Emotional Experience in Everyday Life across the Adult Life Span. Journal of Personality and Social Psychology. 2000;79(4):644–655. [PubMed] [Google Scholar]
- Chan Natalie, Antsey Kaarin J, Windsor Tim D, Luszcz Mary A. Disability and Depressive Symptoms in Later Life: The Stress-buffering Role of Informal and Formal Support. Gerontology. 2011;57(2):180–189. doi: 10.1159/000314158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chipperfield Judith G, Perry Raymond P, Weiner Bernard. Discrete Emotions in Later Life. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2003;58(1):P23–P34. doi: 10.1093/geronb/58.1.p23. [DOI] [PubMed] [Google Scholar]
- Choi Heejeon, Marks Nadine F. Transition to Caregiving, Marital Disagreement, and Psychological Well-being: A Prospective US National Study. Journal of Family Issues. 2006;27(12):1701–1722. [Google Scholar]
- Cohen Sheldon, Wills Thomas A. Stress, Social Support, and the Buffering Hypothesis. Psychological Bulletin. 1985;98(2):310–357. [PubMed] [Google Scholar]
- Coyne James C, Wortman Camille B, Lehman Darrin R. The Other Side of Support: Emotional Overinvolvement and Miscarried Help. In: Gottlieb BH, editor. Marshaling Social Support: Formats, Processes, and Effects. Newbury Park, CA: Sage; 1988. pp. 305–330. [Google Scholar]
- Federal Interagency Forum on Aging-related Statistics. Older Americans 2012: Key Indicators of Well-being. Washington, DC: U.S. Government Printing Office; 2012. [Google Scholar]
- Freedman Vicki A, Cornman Jennifer C. The Panel Study of Income Dynamics Second Supplement on Disability and Use of Time User Guide. Ann Arbor, MI: Institute for Social Research, University of Michigan; 2015. [Google Scholar]
- Freedman Vicki A, Spillman Brenda C, Andreski Patti M, Cornman Jennifer C, Crimmins Eileen M, Kramarow Ellen, Lubitz James, Martin Linda G, Merkin Sharon S, Schoeni Robert F, Seeman Teresa E, Waidmann Timothy A. Trends in Late-life Activity Limitations in the United States: An Update from Five National Surveys. Demography. 2013;50(2):661–671. doi: 10.1007/s13524-012-0167-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freedman Vicki A, Stafford Frank, Schwarz Norbert, Conrad Frederick, Cornman Jennifer C. Disability, Participation, and Subjective Well-being among Older Couples. Social Science and Medicine. 2012;74(4):588–596. doi: 10.1016/j.socscimed.2011.10.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galdas Paul M, Cheater Francine, Marshall Paul. Men and Health Help‐Seeking Behaviour: Literature Review. Journal of Advanced Nursing. 2005;49(6):616–623. doi: 10.1111/j.1365-2648.2004.03331.x. [DOI] [PubMed] [Google Scholar]
- Gayman Mathew D, Turner R Jay, Cui Ming. Physical Limitations and Depressive Symptoms: Exploring the Nature of the Association. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2008;63(4):S219–S228. doi: 10.1093/geronb/63.4.s219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jean-Yves Gerlitz, Schupp Jürgen. Assessment of Big Five Personality Characteristics in the SOEP. Berlin: Deutsches Institut für Wirtschaftsforschung; 2005. [Google Scholar]
- Gerschick Thomas J, Miller Adam S. Coming to Terms: Masculinity and Physical Disability. In: Sabo E, Gordon D, editors. Men’s Health and Illness: Gender, Power, and the Body. Thousand Oaks, CA: Sage; 1995. pp. 183–204. [Google Scholar]
- Gunthert Kathleen Cimbolic, Cohen Lawrence H, Armeli Stephen. The Role of Neuroticism in Daily Stress and Coping. Journal of Personality and Social Psychology. 1999;77(5):1087–1100. doi: 10.1037//0022-3514.77.5.1087. [DOI] [PubMed] [Google Scholar]
- Hall Kathryn A, O’Connor Daniel W. Correlates of Aggressive Behavior in Dementia. International Psychogeriatrics. 2004;16(2):141–158. [PubMed] [Google Scholar]
- Heeringa Steven G, Berglund Patricia A, McGonagle Kate, Schoeni Robert. Panel Study of Income Dynamics User Guide. Ann Arbor, MI: Institute for Social Research, University of Michigan; 2013. [Google Scholar]
- Henry Nancy JM, Berg Cynthia A, Smith Timothy W, Paul Florsheim. Positive and Negative Characteristics of Marital Interaction and their Association with Marital Satisfaction in Middle-aged and Older Couples. Psychology and Aging. 2007;22(3):428–441. doi: 10.1037/0882-7974.22.3.428. [DOI] [PubMed] [Google Scholar]
- Ingersoll-Dayton Berit, Morgan David, Antonucci Toni. The Effects of Positive and Negative Social Exchanges on Aging Adults. Journals of Gerontology: Psychological Sciences. 1997;52(4):P190–P199. doi: 10.1093/geronb/52b.4.s190. [DOI] [PubMed] [Google Scholar]
- Kahneman Daniel, Krueger Alan B, Schkade David A, Schwarz Norbert, Stone Arthur A. A Survey Method for Characterizing Daily Life Experience: The Day Reconstruction Method. Science. 2004;306(5702):1776–1780. doi: 10.1126/science.1103572. [DOI] [PubMed] [Google Scholar]
- Katz Steven J, Kabeto Mohammed, Langa Kenneth M. Gender Disparities in the Receipt of Home Care for Elderly People with Disability in the United States. Journal of American Medical Association. 2000;284(23):3022–3027. doi: 10.1001/jama.284.23.3022. [DOI] [PubMed] [Google Scholar]
- Lang Frieder R, Carstensen Laura L. Time Counts: Future Time Perspective, Goals, and Social Relationships. Psychology and Aging. 2002;17(1):125–139. doi: 10.1037/0882-7974.17.1.125. [DOI] [PubMed] [Google Scholar]
- Mancini Anthony D, Bonanno George A. Marital Closeness, Functional Disability, and Adjustment in Late Life. Psychology and Aging. 2006;21(3):600–610. doi: 10.1037/0882-7974.21.3.600. [DOI] [PubMed] [Google Scholar]
- McGonagle Katharine A, Schoeni Robert F, Sastry Naryan, Freedman Vicki A. The Panel Study of Income Dynamics: Overview, Recent Innovations, and Potential for Life Course Research. Longitudinal and Life Course Studies. 2012;3(2):268–284. doi: 10.14301/llcs.v3i2.188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McIlvane Jessica M, Reinhardt Joann P. Interactive Effect of Support from Family and Friends in Visually Impaired Elders. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2001;56(6):P374–P382. doi: 10.1093/geronb/56.6.p374. [DOI] [PubMed] [Google Scholar]
- Ormel Johan, Rijsdijk Frühling V, Sullivan Mark, van Sonderen Eric, Kempen Gertrudis IJM. Temporal and Reciprocal Relationship between IADL/ADL Disability and Depressive Symptoms in Late Life. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2002;57(4):P338–P347. doi: 10.1093/geronb/57.4.p338. [DOI] [PubMed] [Google Scholar]
- Pearlin Leonard I. The Stress Process Revisited. In: Aneshensel CS, Phelan JC, editors. Handbook of the Sociology of Mental Health. NY: Springer; 1999. pp. 395–415. [Google Scholar]
- Proulx Christine M, Helms Heather M, Buehler Cheryl. Marital Quality and Personal Well‐Being: A Meta‐analysis. Journal of Marriage and Family. 2007;69(3):576–593. [Google Scholar]
- Radloff Lenore. The CES-D Scale: A Self-report Depression Scale for Research in the General Population. Applied Psychological Measurement. 1977;1(3):381–401. [Google Scholar]
- Reed Andrew E, Carstensen Laura L. The Theory behind the Age-related Positivity Effect. Frontiers in Psychology. 2012;3 doi: 10.3389/fpsyg.2012.00339. Retrieved October 12, 2016 ( http://journal.frontiersin.org/article/10.3389/fpsyg.2012.00339/full). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rook Karen S. The Negative Side of Social Interaction: Impact on Psychological Well-being. Journal of Personality and Social Psychology. 1984;46(5):1097–1108. doi: 10.1037//0022-3514.46.5.1097. [DOI] [PubMed] [Google Scholar]
- Schuster Tonya L, Kessler Ronald C, Aseltine Robert H., Jr Supportive Interactions, Negative Interactions, and Depressed Mood. American Journal of Community Psychology. 1990;18(3):423–438. doi: 10.1007/BF00938116. [DOI] [PubMed] [Google Scholar]
- Norbert Schwarz, Strack Fritz. Reports of Subjective Well-being: Judgmental Processes and their Methodological Implications. In: Kahneman D, Diener E, Schwarz N, editors. Well-being: The Foundations of Hedonic Psychology. NY: Russell-Sage; 1999. pp. 61–84. [Google Scholar]
- Stommel Manfred, Given Barbara A, Given Charles W, Kalaian Hripsime A, Schulz Richard, Ruth McCorkle. Gender Bias in the Measurement Properties of the Center for Epidemiologic Studies Depression Scale (CES-D) Psychiatry Research. 1993;49(3):239–250. doi: 10.1016/0165-1781(93)90064-n. [DOI] [PubMed] [Google Scholar]
- Stone Arthur A, Mackie Christopher., editors. Subjective Well-Being: Measuring Happiness, Suffering, and Other Dimensions of Experience. Washington, DC: National Academies Press, National Research Council; 2014. [PubMed] [Google Scholar]
- Taylor Miles G, Lynch Scott M. Trajectories of Impairment, Social Support, and Depressive Symptoms in Later Life. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2004;59(4):S238–S246. doi: 10.1093/geronb/59.4.s238. [DOI] [PubMed] [Google Scholar]
- Warner David F, Jessica Kelley-Moore. The Social Context of Disablement among Older Adults: Does Marital Quality Matter for Loneliness? Journal of Health and Social Behavior. 2012;53(1):50–66. doi: 10.1177/0022146512439540. [DOI] [PubMed] [Google Scholar]
- Weathers Robert II. A Guide to Disability Statistics from the American Community Survey. Ithaca, NY: Cornell University; 2005. [Google Scholar]