

Abstract
Purpose: This article describes gluteus medius and minimus muscle thickness and hip abductor strength and function in healthy adults and explores the relationships between muscle thickness and function. Methods: Gluteus medius and minimus muscle thickness (B-mode ultrasound), isometric hip abductor strength (Biodex dynamometer), and lower extremity function (timed Trendelenburg test, Five-Times-Sit-to-Stand Test [FTSST], and lateral step-down test) were measured in healthy adults using a cross-sectional study design. Results: A total of 22 subjects were included: 10 men and 12 women, mean age 25.2 (SD 3.1) years, mean BMI 22.9 (SD 3.5) kilograms per metre squared. Muscle thickness of the gluteals was a mean 3.88 (SD 0.13) centimetres, and mean hip abductor peak torque was 111 (SD 43) newton-metres. FTSST mean time was 5.3 (SD 0.2) seconds, and median scores were 2.0 points for lateral step-down and 90 seconds for timed Trendelenburg. No significant relationships were found between gluteal muscle thickness and functional tests (rs=−0.28 to 0.37, ps=0.09–0.80) or strength (r=−0.24, p=0.28). Conclusion: Although hip abductors are key pelvic stabilizers for functional movements, gluteal muscle thickness was not associated with strength or function. This may be a result of agonist muscle activity, leading to an inability to isolate the gluteals, and to the ceiling effects of the functional tests.
Key Words: gluteal region, hip, muscle strength, skeletal muscle, ultrasound imaging
Abstract
Objectif : décrire l'épaisseur du muscle moyen glutéal et du muscle petit glutéal, la force et la fonction de l'abducteur de la hanche chez des adultes en santé et explorer les liens entre l'épaisseur et la fonction des muscles. Méthodologie : les chercheurs ont mesuré l'épaisseur du muscle moyen glutéal et du muscle petit glutéal (échographie en mode B), la force de l'abduction isométrique de la hanche (dynanomètre Biodex) et la fonction des jambes (test de Trendelenburg chronométré, test fonctionnel assis-debout de cinq répétitions [FTSST] et tests de descente latérale des marches) chez des adultes en santé dans le cadre d'une étude transversale. Résultats : au total, 22 sujets ont participé, soit 10 hommes et 12 femmes d'un âge moyen de 25,2 ans (ÉT 3,1 ans), d'un IMC moyen de 22,9 kg/m2 (ÉT 3,5 kg/m2). L'épaisseur moyenne des muscles glutéaux était de 3,88 cm (ÉT 0,13 cm), et la puissance de pointe moyenne de l'abducteur de la hanche, de 111 newton-mètres (ÉT 43 Nm). La durée moyenne du FTSST était de 5,3 secondes (ÉT 0,2 s), tandis que le score médian du test de descente latérale des marches était de 2,0 points, et celui du test de Trendelenburg chronométré, de 90 secondes. Il n'y avait pas de relation significative entre l'épaisseur des muscles glutéaux et les tests fonctionnels (r=−0,28 à +0,37, p=0,09 à 0,80) ou la force (r=−0,24, p=0,28). Conclusion : même si les abducteurs de la hanche sont des stabilisateurs essentiels du bassin lors des mouvements fonctionnels, l'épaisseur des muscles glutéaux ne s'associait ni à la force ni à la fonction. Ce peut être à cause de l'activité des muscles agonistes qui empêche d'isoler les muscles glutéaux, de même que des effets plafonds des tests fonctionnels.
Mots clés : échographie, fesse, force musculaire, hanche, muscle squelettique
The gluteus medius and gluteus minimus muscles are key lateral hip muscles that contribute to pelvic stability and lower extremity function,1 and they are frequently implicated in disorders of the pelvis, hip, and knee.2,3 To date, lateral hip muscle performance has primarily been evaluated using measures that target lateral pelvic stability, hip abductor strength, and balance.4 Muscle size is an important determinant of force-generating capacity,5 and it can be determined using ultrasound imaging. Muscle thickness has been shown to correlate with muscle function in other muscle groups such as the quadriceps and abdominal muscles.5,6 Recent studies have examined the hip musculature using ultrasound and reported high reliability7,8 and validity.8 However, the relationships among the structural characteristics of the gluteals, functional measures, and strength have yet to be investigated.
The objectives of this study were to describe gluteus medius and minimus muscle thickness, hip abductor strength, and lower extremity function in healthy men and women and to examine the relationships among these variables.
Methods
We conducted a cross-sectional, prospective study, which was approved by the University of Toronto's Health Sciences Research Ethics Board (REB no. 29560). Healthy men and women aged 20–40 years volunteered to participate in the study, conducted between January and March 2014. Individuals were excluded if they had lower extremity or low-back pain, had sustained injuries in the previous 6 months, or had any underlying conditions associated with muscle atrophy or impaired mobility.
Participants were asked to refrain from performing exercise for 24 hours before testing. B-mode ultrasound (using the LOGIQ e, GE Healthcare, Chicago, IL) was used to image the gluteus medius and minimus (frequency=8–12 MHz, gain=56–58 decibels, depth=6–8 cm). Participants were positioned in supine, and the probe was placed 2 centimetres above the superior aspect of the greater trochanter, along the line of the iliac crest and parallel to the muscle fibres. One of two trained investigators (MF or YQ) captured three images per participant. Muscle thickness was measured between the superficial and the deep aponeurosis of the gluteus medius and minimus and summed for total thickness (see Figure 1). Measurements were conducted by two investigators (SK and LW, blinded to subject) using open-source software (OsiriX version 3.9, Pixmeo, Geneva, Switzerland). The average measurement from three images was used for analysis. Before testing the study subjects, the ultrasound imaging protocol was practised on three pilot subjects, who were not included in the final data set. Two investigators (MF and YQ) piloted the image acquisition protocol, and two independent investigators (SK and LW), blinded to the subjects, piloted the image analysis protocol.
Figure 1.
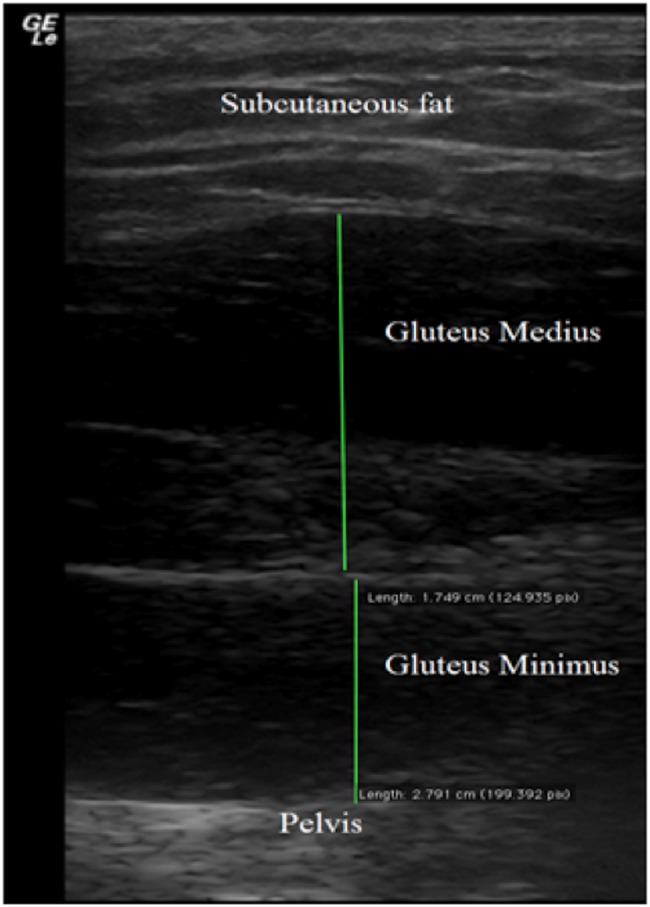
Ultrasound image of the gluteus medius and minimus muscles (frequency=8.0M Hz, gain=58 dB, depth=7.0 cm). Muscle thickness was expressed as a sum of both muscles.
Although few functional performance tests have established validity and reliability for assessing patients with hip pathology,9 three tests were selected for this study that target the evaluation of gluteus medius and minimus muscle function. First, the timed Trendelenburg test was used to measure the length of time the pelvis could be maintained in the frontal plane during single-leg stance.9 This test was selected because of its high sensitivity and specificity for detecting dysfunction of the gluteus medius and minimus muscles and because there is evidence supporting its relationship to hip abductor function.9,10 Coloured-dot stickers were placed bilaterally on the posterior superior ischial spine to help with visualization, and the participant stood barefoot with the non-stance leg in approximately 30° hip flexion, arms crossed over the chest, and pelvis and trunk aligned in midline. Timing was started once the participant was in position and ended when the participant could no longer keep the pelvis aligned in the midline, upright position or maintain a single-leg stance, up to a maximum of 90 seconds.
The second test was the Five-Times-Sit-to-Stand Test (FTSST),11 which was conducted with the participant seated, arms crossed over the chest, feet on the floor, and back resting against a chair (standard seat height of 43 cm). Timing began on the word “Go” and ended when the participant returned to the seated position on the fifth repetition.
The third test, the lateral step-down test,12 was conducted with the participant standing with both legs on a 20-centimetre stool with hands on hips. Participants were instructed to keep their trunk straight while lowering their non-dominant leg to the ground until their toes touched the floor and then to return to the starting position. Markers were placed on the anterior superior iliac spine, tibial tuberosity, and second toe. The test was video recorded for later scoring using a 6-point system (lowest score of 0 reflecting better performance).12 Each of the functional tests was performed three times, with 1-minute breaks in between, and the best time or score was used for analysis.
Maximal voluntary isometric contraction (MVIC) of the hip abductors was measured using the Biodex System 4 (Biodex Medical Systems, Shirley, NY).13 Subjects were positioned in side lying, with the Biodex pad placed on the distal femur above the knee joint and a strap placed across the pelvis for stabilization. The axis of rotation of the Biodex was aligned posteriorly at the level of the greater trochanter. MVIC was measured at 0° hip abduction. Subjects performed five trials, each held for 5 seconds, with 1-minute rests in between.13 Verbal encouragement was given during each contraction. The average of the three closest torque values out of the five trials was used for analysis (average coefficient of variance=3.6%).
We performed our statistical analysis using IBM SPSS Statistics, version 21 (IBM Corp., Armonk, NY). Descriptive statistics (mean and SD) were used to describe demographics and outcome variables. Pearson or Spearman correlation coefficients were used to examine the relationships among muscle thickness, strength, and function.
Results
An initial 38 respondents were screened for eligibility, of whom 16 were excluded because of musculoskeletal pain or injuries. Data on the 22 included subjects are summarized in Table 1. Women had significantly lower mean peak hip abductor torque (86 [SD 21] newton metres [Nm] vs. 140 [SD 44] Nm, respectively; 95% CI: 22, 88, p=0.004), even after normalization to BMI (3.95 [SD 1.02] Nm/kg/m2 vs. 5.92 [SD 1.99] Nm/kg/m2, respectively; 95% CI: 0.46, 3.48, p=0.01). No significant difference was found in mean muscle thickness between women and men (3.79 [SD 0.73] cm vs. 4.00 [SD 0.44] cm, respectively; 95% CI: −0.31, 0.75, p=0.40). A ceiling effect was observed for both the lateral step-down test (20 out of 22 scoring ≤2 points) and timed Trendelenburg (18 out of 22 reached the maximum time of 90 s).
Table 1.
Demographics and Hip Muscle Structure and Function (n=22)
| Mean (SD)* |
||||
| Variable | Range | Men (n=10) | Women (n=12) | Total |
| Age, y | 23–34 | 25 (3) | 25 (3) | 25 (3) |
| Height, m | 1.54–1.88 | 1.76 (0.06) | 1.64 (0.05) | 1.69 (0.08) |
| Weight, kg | 42.6–86.2 | 73.6 (9.0) | 59.3 (11.0) | 68.5 (12.3) |
| BMI, kg/m2 | 17.2–33.2 | 23.8 (2.5) | 22.1 (4.2) | 22.9 (3.5) |
| Muscle thickness (cm) | 2.31–5.05 | 4.00 (0.44) | 3.79 (0.73) | 3.88 (0.13) |
| Peak hip abductor torque, Nm | 47–202 | 140 (44) | 86 (21) | 111 (43) |
| Five-Times-Sit-to-Stand Test, s | 4.1–7.2 | 5.2 (0.9) | 5.3 (0.8) | 5.3 (0.2) |
| Lateral step-down score; median (range) | 0–3 | 2 (0–3) | 1 (0–2) | 2 |
| Timed Trendelenburg, s; median (range) | 65.3–90.0 | 90 (65.3–90) | 90 (73.9–90) | 90 |
Except where otherwise indicated.
No significant correlation was found between muscle thickness and peak torque (r=−0.24, p=0.28). Correlations between muscle thickness and strength with functional tests ranged from −0.28 to 0.18 (ps=0.20–0.83). The highest correlation coefficient was found between muscle thickness and FTSST (r=0.37, p=0.09).
Discussion
This study provides a preliminary description of hip abductor muscle thickness, strength, and function in healthy men and women; it can be used for comparison with future studies on individuals with hip pathology. Gluteus medius and minimus muscle thickness was not associated with hip abductor strength or functional tests, likely owing either to the inability to isolate these muscles during hip abduction or to compound movements of the lower extremity. Thus, muscle thickness measurements may provide unique information about hip abductor muscle structure that cannot be captured by functional testing.
Whittaker and Emery7 found mean gluteal muscle thickness to be 3.27 (SD 0.39) centimetres in adolescent female athletes (aged 14–17 years). Our data show slightly higher values, which may be attributed to the inclusion of men and mature adults in our sample. Other studies have reported slightly higher mean gluteal muscle thickness in healthy women,14,15 but muscle thickness measurements may differ because of the positioning of the subject or the location at which the images were obtained.
Similar to previous studies, we found that hip abductor torque was lower in women than in men, even when normalized to body size.13 We did not find a correlation between muscle thickness and strength, which may be a result of other muscles (gluteus maximus and tensor fasciae latae) contributing to isometric hip abduction.16,17 Previous research has suggested that isolating the gluteus medius and minimus from all the other lumbopelvic musculature may not be possible.18 The association between muscle size and strength may also have been limited by our measurement of muscle thickness rather than the muscle cross-sectional area or thickness at several sites, because those measurements may be a more accurate representation of muscle size. Architectural parameters such as cross-sectional area, pennation angle, and fibre length also affect the torque-generating capacity of a muscle, which could be explored in future studies of the gluteals. Our study's small sample size may also have been a limitation.
We did not find a significant relationship between hip abductor muscle size or strength and the functional tests. Although the timed Trendelenburg and lateral step-down tests are designed to examine lateral pelvic stability, they may not isolate the gluteals sufficiently, and healthy individuals may demonstrate ceiling effects.11 Although weak hip abductors are associated with poor FTSST scores in people with lower extremity pathology, the quadriceps and hamstrings also contribute to this task.19 Although our results did not show an association between hip abductor torque and gluteal muscle thickness and functional tests in a healthy population, this relationship should be further examined in people with known hip abductor muscle weakness.
Conclusion
This study provides preliminary data from healthy adults on the structural and functional characteristics of the hip abductors. Gluteus medius and minimus muscle thickness did not correlate with hip abductor strength or lower extremity function; this may be because we could not isolate these muscles during the functional tests as well as because of ceiling effects in some measurements. Future studies in individuals with hip pathology could examine muscle thickness and other aspects of muscle architecture to elucidate the relationship between muscle structure and function in a clinical population.
Key Messages
What is already known on this topic
The gluteus medius and minimus are important muscles for lateral hip stability and lower extremity function. The thickness of these muscles can be reliably assessed using ultrasound imaging.
What this study adds
This study provides preliminary data that characterize the structure and function of the hip abductor muscles in healthy men and women. The function of the small hip abductors is difficult to isolate using functional tests; however, using ultrasound imaging these muscles can be visualized in vivo. The use of ultrasound in future studies is warranted to examine hip abductor muscle structure in people with hip pathology.
Contributor Information
Lisa Whiler, Department of Physical Therapy, University of Toronto, Toronto.
Michael Fong, Department of Physical Therapy, University of Toronto, Toronto.
Seungjoo Kim, Department of Physical Therapy, University of Toronto, Toronto.
Anna Ly, Department of Physical Therapy, University of Toronto, Toronto.
Yuqian Qin, Department of Physical Therapy, University of Toronto, Toronto.
Euson Yeung, Department of Physical Therapy, University of Toronto, Toronto.
Sunita Mathur, Department of Physical Therapy, University of Toronto, Toronto.
References
- 1. Kim D, Unger J, Lanovaz JL, et al. The relationship of anticipatory gluteus medius activity to pelvic and knee stability in the transition to single-leg stance. PM R. 2016;8(2):138–44. https://doi.org/10.1016/j.pmrj.2015.06.005. Medline:26079865. [DOI] [PubMed] [Google Scholar]
- 2. Fredericson M, Cookingham CL, Chaudhari AM, et al. Hip abductor weakness in distance runners with iliotibial band syndrome. Clin J Sport Med. 2000;10(3):169–75. https://doi.org/10.1097/00042752-200007000-00004. Medline:10959926. [DOI] [PubMed] [Google Scholar]
- 3. Souza RB, Powers CM. Differences in hip kinematics, muscle strength, and muscle activation between subjects with and without patellofemoral pain. J Orthop Sports Phys Ther. 2009;39(1):12–9. https://doi.org/10.2519/jospt.2009.2885. Medline:19131677. [DOI] [PubMed] [Google Scholar]
- 4. Grimaldi A. Assessing lateral stability of the hip and pelvis. Man Ther. 2011;16(1):26–32. https://doi.org/10.1016/j.math.2010.08.005. Medline:20888285. [DOI] [PubMed] [Google Scholar]
- 5. Strasser EM, Draskovits T, Praschak M, et al. Association between ultrasound measurements of muscle thickness, pennation angle, echogenicity and skeletal muscle strength in the elderly. Age (Dordr). 2013;35(6):2377–88. https://doi.org/10.1007/s11357-013-9517-z. Medline:23456136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Kim CY, Choi JD, Kim SY, et al. Comparison between muscle activation measured by electromyography and muscle thickness measured using ultrasonography for effective muscle assessment. J Electromyogr Kinesiol. 2014;24(5):614–20. https://doi.org/10.1016/j.jelekin.2014.07.002. Medline:25088820 [DOI] [PubMed] [Google Scholar]
- 7. Whittaker JL, Emery CA. Sonographic measures of the gluteus medius, gluteus minimus, and vastus medialis muscles. J Orthop Sports Phys Ther. 2014;44(8):627–32. https://doi.org/10.2519/jospt.2014.5315. Medline:25029916. [DOI] [PubMed] [Google Scholar]
- 8. Mendis MD, Wilson SJ, Stanton W, et al. Validity of real-time ultrasound imaging to measure anterior hip muscle size: a comparison with magnetic resonance imaging. J Orthop Sports Phys Ther. 2010;40(9):577–81. https://doi.org/10.2519/jospt.2010.3286. Medline:20479536. [DOI] [PubMed] [Google Scholar]
- 9. Kivlan BR, Martin RL. Functional performance testing of the hip in athletes: a systematic review for reliability and validity. Int J Sports Phys Ther. 2012;7(4):402–12. Medline:22893860. [PMC free article] [PubMed] [Google Scholar]
- 10. Hardcastle P, Nade S. The significance of the Trendelenburg test. J Bone Joint Surg Br. 1985;67(5):741–6. Medline:4055873. [DOI] [PubMed] [Google Scholar]
- 11. Whitney SL, Wrisley DM, Marchetti GF, et al. Clinical measurement of sit-to-stand performance in people with balance disorders: validity of data for the Five-Times-Sit-to-Stand Test. Phys Ther. 2005;85(10):1034–45. Medline:16180952. [PubMed] [Google Scholar]
- 12. Piva SR, Fitzgerald K, Irrgang JJ, et al. Reliability of measures of impairments associated with patellofemoral pain syndrome. BMC Musculoskelet Disord. 2006;7(1):33 https://doi.org/10.1186/1471-2474-7-33. Medline:16579850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Jacobs CA, Uhl TL, Mattacola CG, et al. Hip abductor function and lower extremity landing kinematics: sex differences. J Athl Train. 2007;42(1):76–83. Medline:17597947. [PMC free article] [PubMed] [Google Scholar]
- 14. Ikezoe T, Mori N, Nakamura M, et al. Atrophy of the lower limbs in elderly women: is it related to walking ability? Eur J Appl Physiol. 2011;111(6):989–95. https://doi.org/10.1007/s00421-010-1728-8. Medline:21082193. [DOI] [PubMed] [Google Scholar]
- 15. Fukumoto Y, Ikezoe T, Tateuchi H, et al. Muscle mass and composition of the hip, thigh and abdominal muscles in women with and without hip osteoarthritis. Ultrasound Med Biol. 2012;38(9):1540–5. https://doi.org/10.1016/j.ultrasmedbio.2012.04.016. Medline:22749818. [DOI] [PubMed] [Google Scholar]
- 16. Lee JH, Cynn HS, Choi SA, et al. Effects of different hip rotations on gluteus medius and tensor fasciae latae muscle activity during isometric side-lying hip abduction. J Sport Rehabil. 2013;22(4):301–7. https://doi.org/10.1123/jsr.22.4.301. Medline:23921296. [DOI] [PubMed] [Google Scholar]
- 17. Fujisawa H, Suzuki H, Yamaguchi E, et al. Hip muscle activity during isometric contraction of hip abduction. J Phys Ther Sci. 2014;26(2):187–90. https://doi.org/10.1589/jpts.26.187. Medline:24648628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Gottschalk F, Kourosh S, Leveau B. The functional anatomy of tensor fasciae latae and gluteus medius and minimus. J Anat. 1989;166:179–89. Medline:2621137. [PMC free article] [PubMed] [Google Scholar]
- 19. Davidson BS, Judd DL, Thomas AC, et al. Muscle activation and coactivation during Five-Time-Sit-to-Stand movement in patients undergoing total knee arthroplasty. J Electromyogr Kinesiol. 2013;23(6):1485–93. https://doi.org/10.1016/j.jelekin.2013.06.008. Medline:23953763. [DOI] [PubMed] [Google Scholar]