

Abstract
Background
The prognostic value of hsCRP in contemporary multi-ethnic populations is unclear, particularly in statin users. The aim of this study was to characterize the prognostic utility of hsCRP for atherosclerotic CVD (ASCVD) risk prediction in a multi-ethnic population including non-users and users of statins followed for more than 13 years. Associations with heart failure (HF), atrial fibrillation (AF), venous thromboembolism (VTE), cancer, and all-cause death were also examined.
Methods and Results
We evaluated 6,757 participants from the Multi-Ethnic Study of Atherosclerosis (MESA; 1,002 using statins at baseline), median follow-up 13.2 years. Higher levels of hsCRP were associated with a higher risk of all study endpoints in the unadjusted Cox Proportional Hazards regression analyses, except AF. Among non-users of statins, hsCRP only remained associated with VTE after adjusting for ASCVD risk factors, and did not improve risk prediction. Among users of statins, hsCRP did not improve ASCVD risk prediction either, although it was strongly associated with incident HF (HR for hsCRP ≥2 vs <2 mg/L 3.99; 95% CI 2.02, 7.90) and all-cause death (HR 1.52; 95% CI 1.11, 2.08) in multivariable analyses, and hsCRP significantly improved prediction of HF (area under the curve [AUC] basic model 0.741, AUC basic+hsCRP 0.788).
Conclusions
The utility of hsCRP for ASCVD prediction was modest. On the other hand, hsCRP was associated with incident VTE in statin non-users, and all-cause mortality and HF in statin users. In the latter, hsCRP improved the prediction of incident HF events. This finding should be replicated in larger cohorts.
Keywords: Inflammation, C-reactive protein, prognosis, prediction, cardiovascular disease, heart failure
1. Introduction
Inflammation is a key common upstream factor in the pathogenesis of a number of diseases, including coronary atherothrombosis [1-4] and cancer [5-7]. Lifestyle interventions such as exercise, weight loss, and adherence to a healthy diet are known to reduce inflammation [8-10] and are associated with improved health outcomes [10-12].
Consistent with this, measures of subclinical inflammation such as high sensitivity C-reactive protein (hsCRP) have been proposed as tools to enhance disease risk assessment [13,14]. Specifically, the 2013 American College of Cardiology / American Heart Association (ACC/AHA) recommended using hsCRP ≥2 mg/L to augment 10-year atherosclerotic cardiovascular disease (CVD) risk assessment in asymptomatic individuals in whom preventive management is uncertain after traditional risk factor assessment [14]. Studies such as the 2008 Justification for the Use of Statins in Primary Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) [15] or recently the Canakinumab Anti-inflammatory Thrombosis Outcomes Study (CANTOS) [16] have also used hsCRP ≥2 mg/L to identify primary and secondary prevention populations at increased risk of events who might benefit from additional pharmacological interventions.
The independent prognostic value of hsCRP beyond traditional risk factors, however, has been reported to be modest in several primary prevention populations [17]. Also, the influence of statin therapy on the prognostic capacity of hsCRP is not fully understood. The purpose of this study was thus to characterize, in a contemporary, multi-ethnic population including non-users and users of statins, the prognostic utility of hsCRP for the prediction of atherosclerotic CVD (ASCVD) events, after a median of more than 13 years of follow-up. Additionally, given recent interest in inflammatory biomarkers across a spectrum of diseases, in exploratory analyses we also evaluated the prognostic value of hsCRP for the prediction of heart failure (HF), atrial fibrillation (AF), venous thromboembolism (VTE), cancer, and all-cause death.
2. Methods
2.1. Study Design
The Multi-Ethnic Study of Atherosclerosis (MESA) is a community-based, multi-center, NHLBI-funded cohort study of men and women from 4 race/ethnic groups recruited in 6 sites within the US. Details on the MESA study methods have been reported before [18] and are also available on the study website (https://www.mesa-nhlbi.org).
2.2. Study Population
All participants evaluated in MESA Visit 1 (N = 6,814) were considered for inclusion. Participants with missing information on hsCRP levels at Visit 1 or with no follow-up data were excluded. Two study populations were defined: a pure primary prevention population of MESA participants not using statins at baseline (“non-users of statins”), and a population free of known CVD but already using statins at MESA Visit 1 (“users of statins”) (Figure 1).
Figure 1. Study population, the Multi-Ethnic Study of Atherosclerosis (MESA).
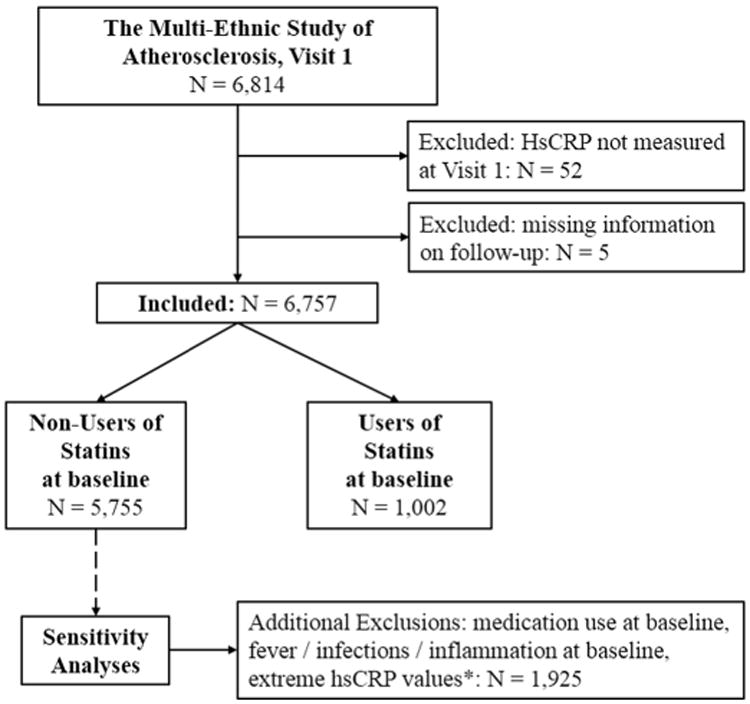
*: This sensitivity analysis excluded participants using statins, other lipid-lowering medications, aspirin, ADP-receptor inhibitor antiplatelet drugs, NSAIDs, steroids (oral/inhaled), cox-2 inhibitors, beta-blockers, ACEIs, ARBs, or oral antidiabetic medications at baseline; participants reporting at baseline fever, acute infections or joint inflammation in the last 2 weeks, and participants with extreme (>10 mg/L) HsCRP values at baseline (“restrictive population”, N =1,925)
Abbreviations: ACEI = angiotensin-converting-enzyme inhibitor; ADP = Adenosine diphosphate; ARB = angiotensin II receptor blockers; HsCRP = high sensitivity C reactive protein; NSAID = nonsteroidal anti-inflammatory drug
2.3. Assessment of HsCRP and Relevant Covariates
A number of evaluations were performed as part of MESA Visit 1. HsCRP was measured using a BNII nephelometer (N-High Sensitivity CRP; Dade Behring Inc, Deerfield, IL). Sociodemographic characteristics, family history of CHD, tobacco use, and medication use were self-reported using a standardized questionnaire. Resting blood pressure and waist circumference were measured following standardized protocols [18]. Fasting levels of total and high density lipoprotein (HDL) cholesterol, and blood glucose were measured at the MESA central laboratory at the University of Minnesota.
2.4. Event Ascertainment
Every 9 to 12 months, MESA interviewers contacted each study participant to inquire them about hospital admissions, CVD outpatient diagnoses and procedures. Medical encounters were also identified through additional sources of information including cohort clinic visits, participant call-ins, medical record abstractions and obituaries (see https://www.mesa-nhlbi.org for further details).
Hard CHD events were defined as the composite of non-fatal myocardial infarction, death from CHD, or resuscitated cardiac arrest. Hard ASCVD events were defined as a composite endpoint including hard CHD events, stroke, other atherosclerotic death, or other CVD death. The term ASCVD rather than CVD is used throughout to indicate that this study endpoint did not include AF or HF events.
Incident HF, AF, VTE, cancer and all-cause death were also evaluated in exploratory analyses. HF events were adjudicated by a MESA adjudication committee, and were defined by the presence of suggestive symptoms such as shortness of breath or edema, a physician diagnosis of HF, and documented medical treatment for HF. AF was identified from hospital records by the presence of International Classification of Diseases, Ninth Revision (ICD-9) diagnosis codes 427.31 or 427.32, or from self-report. Non-CVD endpoints (VTE, cancer) were identified from hospital records using ICD-9 codes (see Table S1 of the Supplementary Appendix for the specific lists of codes).
2.5. Statistical Analysis
For the purposes of this study, hsCRP levels were modeled in a number of ways: as a binary exposure using the 2 mg/L cutpoint [14-16], as a categorical variable of increasing levels of hsCRP (<1, 1 – 2.99 and ≥3 mg/L, which were similar to tertiles of hsCRP in the two study populations), and as a continuous exposure. For the latter, log-transformation was used to account for the right skewed distribution.
Unadjusted incidence rates of each of the study endpoints, and unadjusted Kaplan-Meier cumulative survivor function curves, were calculated by categories of hsCRP. Log-rank tests were used to compare survivor function curves.
Cox proportional hazards regression models were used to evaluate the associations between hsCRP levels and the occurrence of each of the study endpoints, adjusting for a number of potential confounders. Four hierarchical models were used for this purpose: model 1 was unadjusted; model 2 adjusted for age, sex, race/ethnicity and education; and model 3 further adjusted for tobacco use (current/former/never smoker), diabetes, total cholesterol, HDL cholesterol, systolic blood pressure, medication use for hypertension, and chronic aspirin use (all assessed at MESA Visit 1). An additional model was used to evaluate the effect of further adjusting for waist circumference, which is known to be closely related to hsCRP [19] (Model 4).
To evaluate improvement in discrimination with hsCRP, the area under the receiver-operator characteristic curve (AUC) was calculated for each of the study endpoints, for models including clinical risk factors alone and models including clinical risk factors plus levels of hsCRP. Specifically for hard ASCVD events, the net reclassification improvement (NRI) [20] was also computed, comparing the performance of 10-year prediction models with and without hsCRP. For this analysis, the 5% and 7.5% 10-year ASCVD risk thresholds defined by the ACC/AHA were used, scaled to account for a longer median follow-up in MESA. Finally, the Akaike Information Criterion [21] (AIC) was also calculated for models without and with hsCRP. This parameter assesses the performance of regression models and is used for model selection; among a finite set of models, the one with the lowest value is considered to have the best performance. All main analyses (except for NRI) were performed stratified by baseline statin use.
To assess the robustness of the results, the analyses were repeated in a subgroup of individuals free of fever, acute infections, or inflammatory symptoms during the two weeks preceding MESA Visit 1, and not treated at baseline with any of the most frequently used drugs known to affect levels of hsCRP: statins, other lipid-lowering medications, aspirin, ADP-receptor inhibitor antiplatelet drugs, NSAIDs, steroids (oral / inhaled), Cox-2 inhibitors, beta-blockers, ACEIs, ARBs, or oral antidiabetic medications [22] (“restrictive sensitivity analysis population”, Figure 1),
A p value of <0.05 was considered the threshold for statistical significance. All analyses were performed using Stata software version 14 [23].
3. Results
3.1. Study Population
The study population included 6,757 MESA participants, 5,755 of which were non-users of statins at baseline (median age 62 years, 53% women) and 1,002 used statins at MESA Visit 1 (median age 67 years, 53% women) (Figure 1). Median follow-up was 13.2 years.
3.2. Baseline Distribution of HsCRP
Among non-users of statins, median baseline hsCRP levels were 1.94 mg/L (interquartile range [IQR] 0.85, 4.34), and the hsCRP ≥3 mg/L stratum comprised the largest proportion of participants (Figure S1a of the Supplementary Appendix). Among statin users, median hsCRP levels were 1.65 mg/L (IQR 0.75, 3.75), and the prevalence of hsCRP <1 mg/L was the largest of the 4 strata considered (Figure S1b). Both distributions were markedly right-skewed (Figure S2).
3.3. Baseline Characteristics of the Study Participants
Among non-users of statins, the prevalence of female sex, African-American and Hispanic race/ethnicities, and lower education level were higher with higher hsCRP levels (Table 1). Regarding clinical features, higher levels of hsCRP were associated with a worse profile for almost every risk factor considered, except age and total cholesterol. Similar trends were observed among users of statins, including higher levels of total cholesterol with higher hsCRP. Findings were similar when participants were stratified using a cut-point of 2 mg/L (Table S2).
Table 1.
Baseline characteristics of the study participants by baseline statin use and hscrp strata, the Multi-Ethnic Study of Atherosclerosis (MESA).
| Non-Users of Statins at Baseline (N = 5,755) | Users of Statins at Baseline (N = 1,002) | |||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| HsCRP (mg/L) | < 1 (N = 1,682) | 1 – 2.99 (N = 1,947) | ≥ 3 (N = 2,126) | P Value | < 1 (N = 340) | 1 – 2.99 (N = 343) | ≥ 3 (N = 319) | P Value |
| Age, years | 59 (51, 69) | 62 (53, 70) | 61 (53, 69) | <0.001 | 67 (59, 73) | 67 (60, 72) | 66 (59, 71) | 0.373 |
| Women | 712 (42.3) | 947 (48.6) | 1,376 (64.7) | <0.001 | 140 (41.2) | 169 (49.3) | 223 (69.9) | <0.001 |
| Race/ethnicity | ||||||||
| Non-Hispanic White | 681 (40.5) | 733 (37.7) | 755 (35.5) | <0.001 | 146 (42.9) | 163 (47.5) | 124 (38.9) | <0.001 |
| African American | 352 (20.9) | 508 (26.1) | 717 (33.7) | 77 (22.7) | 95 (27.7) | 116 (36.4) | ||
| Hispanic | 272 (16.2) | 471 (24.2) | 568 (26.7) | 51 (15.0) | 61 (17.8) | 66 (20.7) | ||
| Chinese American | 377 (22.4) | 235 (12.1) | 86 (4.1) | 66 (19.4) | 24 (7.0) | 13 (4.1) | ||
| Education | ||||||||
| Less than college | 502 (29.9) | 710 (36.6) | 846 (40.0) | <0.001 | 116 (34.2) | 130 (37.9) | 136 (42.6) | 0.049 |
| Technical school certificate, assoc. degree | 791 (47.1) | 900 (46.4) | 968 (45.8) | 144 (42.5) | 142 (41.4) | 136 (42.6) | ||
| Bachelor's degree, graduate or prof. school | 386 (23.0) | 329 (17.0) | 301 (14.2) | 79 (23.3) | 71 (20.7) | 47 (14.7) | ||
| Waist circumference, cm | 90 (83, 98) | 97 (89, 105) | 102 (93, 113) | <0.001 | 95 (87, 102) | 100 (94, 109) | 105 (96, 115) | <0.001 |
| Family history of CHD | 578 (36.7) | 750 (41.1) | 881 (44.3) | <0.001 | 169 (51.7) | 168 (51.4) | 158 (52.8) | 0.929 |
| Current smoker | 185 (11.0) | 233 (12.0) | 360 (17.0) | <0.001 | 20 (5.9) | 32 (9.3) | 45 (14.1) | 0.006 |
| Diabetes | 124 (7.4) | 211 (10.8) | 296 (14.0) | <0.001 | 72 (21.2) | 65 (19.0) | 83 (26.0) | 0.082 |
| SBP, mmHg | 122 (21) | 126 (21) | 129 (22) | <0.001 | 127 (22) | 130 (21) | 133 (22) | 0.004 |
| Medications for hypertension | 373 (22.2) | 542 (27.8) | 777 (36.6) | <0.001 | 164 (48.2) | 190 (55.4) | 198 (62.1) | 0.002 |
| Total cholesterol, mg/dL | 192 (32) | 199 (36) | 197 (37) | <0.001 | 177 (30) | 182 (32) | 186 (38) | 0.003 |
| HDL cholesterol, mg/dL | 50 (41, 61) | 48 (40, 59) | 48 (40, 58) | <0.001 | 51 (43, 60) | 46 (40, 56) | 49 (42, 57) | 0.002 |
| Aspirin use at baseline | 272 (16.9) | 337 (18.1) | 336 (16.4) | 0.393 | 123 (38.3) | 111 (33.8) | 104 (34.0) | 0.404 |
Data presented as mean (SD), median (IQR) or N (%). Percentages may not sum 100% due to rounding
Abbreviations: CHD = coronary heart disease; HDL = high density lipoprotein; HsCRP = high sensitivity C-reactive protein; SBP = systolic blood pressure.
3.4. Unadjusted Incidence Rates
Among non-users of statins, higher hsCRP levels were associated with higher unadjusted event rates of each of the study endpoints, although event rates of AF and cancer were slightly lower for the hsCRP ≥3 mg/L stratum than for the 1–3 mg/L group (Table S3). Overall event rates were higher for users of statins, the highest being those for all-cause death and cancer. Statin users with hsCRP ≥3 mg/L had the highest rates of each of the study endpoints, except for AF (Table S3).
When participants were stratified using a 2 mg/L cut-point (Table S4), among both non-users and users of statins hsCRP ≥2 mg/L was associated with higher event rates of each of the study endpoints compared to hsCRP <2 mg/L.
3.5. Kaplan-Meier Cumulative Survivor Function Analyses
The results of the Kaplan-Meier survivor function analyses (Figures S3 and S4) were consistent with the unadjusted rates. Among non-users of statins, individuals in the ≥3 mg/L hsCRP stratum had the worst cumulative survival for all study endpoints, except AF and cancer.
HsCRP was even more informative among users of statins, in which the higher event rates resulted in more divergent curves. In this population, hsCRP ≥3 mg/L was associated with the worst cumulative survival for all study endpoints, except AF. This was particularly true for HF and all-cause death, in which individuals with hsCRP ≥3 mg/L had a markedly worse survival than the other two strata.
3.6. Multivariable-adjusted Associations between HsCRP and Study Endpoints
Among non-users of statins, adjusting for sociodemographic characteristics (Figure S5, upper panel) there was a graded association between higher levels of hsCRP and the risk of each of the study endpoints, except for CHD. Further adjustment for traditional ASCVD risk factors (Figure S5, lower panel) resulted in weaker associations, particularly for CHD, ASCVD, cancer, and all-cause death. On the other hand, hsCRP ≥3 mg/L (as compared to <1 mg/L) remained strongly associated with HF and VTE. Associations were weaker in the binary analyses using the hsCRP 2 mg/L cut-point (Table 2a).
Table 2a.
Hazard ratios from Cox proportional hazards regression models for each of the study endpoints, non-users of statins at baseline.
| Main Study Endpoints | Exploratory Study Endpoints | |||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Hard CHD | Stroke | Hard CVD | Heart Failure | Atrial Fibrillation | VTE | Cancer (Any) | All-cause Death | |
| HsCRP ≥ 2 vs < 2 mg/L (Ref) | ||||||||
| Model 1 | 1.05 (0.84, 1.30) | 1.45 (1.11, 1.89) | 1.20 (1.01, 1.42) | 1.24 (0.97, 1.58) | 1.06 (0.88, 1.29) | 1.56 (1.19, 2.05) | 1.22 (1.05, 1.41) | 1.21 (1.06, 1.37) |
| Model 2 | 1.08 (0.86, 1.36) | 1.37 (1.04, 1.81) | 1.20 (1.00, 1.43) | 1.26 (0.97, 1.62) | 1.15 (0.95, 1.41) | 1.37 (1.03, 1.81) | 1.24 (1.07, 1.44) | 1.26 (1.10, 1.44) |
| Model 3 | 0.94 (0.74, 1.18) | 1.10 (0.83, 1.47) | 1.00 (0.83, 1.20) | 1.03 (0.79, 1.35) | 1.09 (0.88, 1.34) | 1.30 (0.97, 1.74) | 1.16 (0.99, 1.36) | 1.17 (1.02, 1.34) |
| Model 4 | 0.90 (0.71, 1.14) | 1.14 (0.85, 1.53) | 0.98 (0.81, 1.19) | 0.95 (0.72, 1.25) | 1.03 (0.83, 1.28) | 1.14 (0.84, 1.55) | 1.13 (0.96, 1.32) | 1.17 (1.02, 1.34) |
Data presented as hazard ratios from Cox proportional hazards regression models
Model 1 was crude (unadjusted)
Model 2 adjusted for age at baseline, sex, race/ethnicity and education
Model 3 adjusted for the variables in Model 2 plus tobacco use, diabetes, total cholesterol, HDL cholesterol, systolic blood pressure, medication use for hypertension, chronic aspirin use (all assessed at baseline)
Model 4 adjusted for the variables in Model 3 plus waist circumference at baseline
Abbreviations: CHD = coronary heart disease; ASCVD = atherosclerotic cardiovascular disease; HDL = high density lipoprotein; HsCRP = high sensitivity C-reactive protein; VTE = venous thromboembolism
Among users of statins, most associations between hsCRP ≥3 mg/L (as compared to <1 mg/L) and each of the study endpoints were stronger than among non-users (Figure S6, upper panel). On the other hand, due to a smaller sample size the 95% confidence intervals (CIs) were wider. As for non-users of statins, multivariable-adjusted associations with CHD and ASCVD were almost null (Figure S6, lower panel). On the other hand, the associations with HF and all-cause death were strong –particularly for HF– and none of them included the null value. In the binary analyses (Table 2b), hsCRP ≥2 mg/L (as compared to <2 mg/L) was strongly associated with VTE, death, and especially with incident HF.
Table 2b.
Hazard ratios from the Cox proportional hazards regression models for each of the study endpoints, users of statins at baseline.
| Main Study Endpoints | Exploratory Study Endpoints | |||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Hard CHD | Stroke | Hard ASCVD | Heart Failure | Atrial Fibrillation | VTE | Cancer (Any) | All-cause Death | |
| HsCRP ≥ 2 vs < 2 mg/L (Ref) | ||||||||
| Model 1 | 1.23 (0.80, 1.90) | 1.32 (0.74, 2.37) | 1.18 (0.82, 1.70) | 3.33 (1.83, 6.04) | 0.85 (0.55, 1.31) | 1.93 (1.06, 3.50) | 1.30 (0.94, 1.80) | 1.42 (1.07, 1.89) |
| Model 2 | 1.43 (0.91, 2.26) | 1.30 (0.71, 2.40) | 1.33 (0.91, 1.95) | 4.33 (2.31, 8.14) | 0.97 (0.62, 1.54) | 1.76 (0.94, 3.29) | 1.42 (1.01, 2.00) | 1.60 (1.18, 2.16) |
| Model 3 | 1.11 (0.69, 1.79) | 1.08 (0.56, 2.07) | 1.07 (0.71, 1.60) | 3.99 (2.02, 7.90) | 0.87 (0.54, 1.41) | 1.63 (0.85, 3.13) | 1.31 (0.92, 1.87) | 1.52 (1.11, 2.08) |
| Model 4 | 1.11 (0.68, 1.81) | 1.10 (0.56, 2.15) | 1.07 (0.71, 1.61) | 3.74 (1.86, 7.51) | 0.74 (0.46, 1.21) | 1.37 (0.71, 2.66) | 1.25 (0.87, 1.79) | 1.44 (1.05, 1.99) |
Data presented as hazard ratios from Cox proportional hazards regression models
Model 1 was crude (unadjusted)
Model 2 adjusted for age at baseline, sex, race/ethnicity and education
Model 3 adjusted for the variables in Model 2 plus tobacco use, diabetes, total cholesterol, HDL cholesterol, systolic blood pressure, medication use for hypertension, chronic aspirin use (all assessed at baseline)
Model 4 adjusted for the variables in Model 3 plus waist circumference at baseline
Abbreviations: CHD = coronary heart disease; ASCVD = atherosclerotic cardiovascular disease; HDL = high density lipoprotein; HsCRP = high sensitivity C-reactive protein; VTE = venous thromboembolism
In both non-users and users of statins, further adjustment for waist circumference (model 4) resulted in a modest attenuation of the point estimates for most positive associations.
3.7. Independent Predictive Value of HsCRP for the Prediction of ASCVD
Among both non-users and users of statins, addition of hsCRP to models including traditional ASCVD risk factors resulted in negligible, non-statistically significant improvements in the AUC for the prediction of hard CHD, stroke, and hard ASCVD events, regardless of the hsCRP modeling approach used (Table 3). Similar results were observed in the AIC analyses (Table S5), in which addition of hsCRP resulted in minimal, if any, improvements in the performance of the models.
Table 3.
Area under the receiver operating characteristic curve (AUC) analyses for each of the study endpoints comparing a prediction model including socio-demographic features and cardiovascular risk factors and the same model plus hsCRP, by baseline statin use.
| Model Without HsCRP | Model With HsCRP, ≥ 2 vs < 2 | Model With HsCRP, categoricala | Model With HsCRP, log-transformed | ||
|---|---|---|---|---|---|
| Non-Users of Statins at baseline | |||||
|
| |||||
| Main | Hard CHD | 0.729 | 0.729 | 0.730 | 0.729 |
| Stroke | 0.719 | 0.719 | 0.721 | 0.720 | |
| Hard ASCVD | 0.727 | 0.727 | 0.728 | 0.728 | |
|
| |||||
| Exploratory | Heart Failure | 0.778 | 0.778 | 0.779 | 0.778 |
| Atrial Fibrillation | 0.736 | 0.736 | 0.737 | 0.737 | |
| VTE | 0.682 | 0.683 | 0.690 | 0.685 | |
| Cancer (any) | 0.700 | 0.701 | 0.700 | 0.700 | |
| All-cause Death | 0.813 | 0.813 | 0.813 | 0.813 | |
|
| |||||
| Users of Statins at baseline | |||||
|
| |||||
| Main | Hard CHD | 0.705 | 0.707 | 0.705 | 0.705 |
| Stroke | 0.733 | 0.733 | 0.737 | 0.737 | |
| Hard ASCVD | 0.718 | 0.718 | 0.718 | 0.718 | |
|
| |||||
| Exploratory | Heart Failure | 0.741 | 0.788b | 0.778c | 0.768 |
| Atrial Fibrillation | 0.676 | 0.676 | 0.687 | 0.678 | |
| VTE | 0.719 | 0.730 | 0.718 | 0.719 | |
| Cancer (any) | 0.682 | 0.687 | 0.684 | 0.686 | |
| All-cause Death | 0.744 | 0.747 | 0.747 | 0.748 | |
For this analysis, hsCRP was modelled as a categorical variable: <1 mg/L, ≥1 - <3 mg/L, ≥3 mg/L
P value of the comparison with the model without hsCRP was 0.038
P value of the comparison with the model without hsCRP was 0.053
All other P values for the comparisons between each of the models including hsCRP and the model without hsCRP were >0.100 All models included the following variables: age at baseline, sex, race/ethnicity, education, tobacco use, diabetes, total cholesterol, HDL cholesterol, systolic blood pressure, medication use for hypertension, and chronic aspirin use (all assessed at baseline)
Abbreviations: AUC = area under the curve; CHD = coronary heart disease; ASCVD = atherosclerotic cardiovascular disease; HsCRP = high sensitivity C reactive protein; VTE = venous thromboembolism
The results of the NRI analysis for the prediction of hard ASCVD events among non-users of statins (Table S6) were consistently ≈0 when comparing models including hsCRP to those including traditional risk factors alone.
3.8. Independent Predictive Value of HsCRP for the Prediction of the Exploratory Endpoints
Among non-users of statins, addition of hsCRP resulted in very small (if any), non-statistically significant improvements in the AUC for all exploratory endpoints (Table 3). The same was true among users of statins, except for the prediction of HF. For this exploratory endpoint, addition of hsCRP resulted in a large, statistically significant improvement in the AUC. Similar results were observed in the AIC analyses (Table S5), in which addition of hsCRP resulted in small, if any, improvements in the performance of the models, except for HF.
3.9. Sensitivity Analyses
For the sensitivity analyses (Tables S7 – S11 and Figures S7 – S9), 1,925 MESA participants were included in the “restrictive population” (median age 58 years, 47% women). This population was younger and had a lower baseline burden of some risk factors than the non-user population included in the main analyses. Baseline hsCRP levels were also lower (median 1.41 mg/L, IQR 0.67 – 2.95). The independent predictive value of hsCRP in terms of AUC and NRI was once again very small (if any) and non-statistically significant for all endpoints evaluated, although improvements in the AUC tended to be slightly larger than those observed in the non-user population included in the main analyses.
4. Discussion
In a multi-ethnic population including non-users and users of statins, higher levels of hsCRP were associated with a number of health outcomes including ASCVD, HF, VTE, cancer, and all-cause death. However, only a few associations remained statistically significant after adjusting for traditional CVD risk factors. HsCRP did not improve the prediction of ASCVD events in both non-users and users of statin therapy after 13 years of follow-up. On the other hand, in the latter hsCRP significantly improved HF risk prediction, although this observation should be replicated in larger cohorts.
These results have implications for understanding the pathobiology of common diseases. The strong, positive, prospective associations between hsCRP, a marker of inflammation, and the incidence of conditions as disparate as stroke, HF, VTE or cancer provide support to the notion of inflammation as a common upstream cause of disease [1-7]. In this sense, the recent CANTOS trial provided further, experimental evidence for a causal link between inflammation and CVD [16], and inflammation and cancer [24]. Second, the lack of independent associations between hsCRP and ASCVD endpoints after adjustment for traditional risk factors suggests that the association may be explained predominantly by traditional risk factors alone [25,26]. On the other hand, the persistence of independent associations between hsCRP and some exploratory study endpoints including all-cause death suggests that for non-atherosclerotic endpoints, inflammation may not only operate through its association with traditional ASCVD risk factors but also via other pathways; although residual confounding is another potential explanation. Third, the fact that independent associations were only slightly attenuated after accounting for waist circumference suggests that despite their strong association, hsCRP may capture additional prognostic information beyond this anthropometric measure.
Besides biological insights, our findings also have important clinical implications. Among non-users of statins, addition of hsCRP to models including sociodemographic characteristics and traditional risk factors resulted in no improvement in ASCVD prediction. This is consistent with the results from previous studies, in which hsCRP was found to be a poor risk assessment tool in primary prevention settings once traditional risk factors have been accounted for [27,28]. The results are also consistent with previous evaluations in MESA using shorter follow-up periods [29,30].
Our analysis on statin-naïve MESA participants provides an update to those assessments using a longer follow-up, adjusting for additional key features (including baseline aspirin use), and exploring associations with other, non-atherosclerotic endpoints. Importantly, previous studies have suggested that in primary prevention populations, tests assessing early stages of disease such as the coronary artery calcium score for the detection of atherosclerosis and the prediction of CHD and ASCVD, are more robust and informative than hsCRP [29-32]. Current ACC/AHA primary prevention risk assessment guidelines present hsCRP and all other tests at the same level of recommendation [14]; however, our findings together with those from prior research suggest that hsCRP ≥2 mg/L performs poorly for ASCVD risk assessment in apparently healthy individuals, and future guidelines may consider downgrading this recommendation as compared to other tools such as the coronary artery calcium score. Of note, the 2016 European CVD risk assessment guidelines do not support the use of hsCRP for further risk stratification [33].
Among individuals already using statins, the value of hsCRP for the prediction of ASCVD events was also very modest. On the other hand, our exploratory analyses suggest that hsCRP may have a relevant role for the prediction of incident HF in these individuals. To our knowledge, this is the first study to assess the prognostic utility of hsCRP in a multi-ethnic population of statin users. In MESA, participants were free of clinically-overt CVD at baseline [18]; nonetheless, it seems reasonable to assume that the subgroup of participants using statins represented a higher baseline risk subgroup – indeed, in our study these patients were older and had a higher prevalence of diabetes, hypertension medication use and chronic aspirin use than non-users of statins. In high-risk populations, in which interpretation of traditional risk factors may be challenging due to the effect of therapies, and in which the role of other tools such as the coronary artery calcium score may have less value, hsCRP may provide an inexpensive, readily available, zero radiation tool identifying individuals at increased risk of myocardial dysfunction, who may get the greatest benefit from additional interventions [16].
Our observation for HF is consistent with the results of previous mechanistical studies, in which there were independent associations between markers of subclinical inflammation and the development of early ventricular dysfunction [34-39]. Nevertheless, in most of these studies follow-up was short and stratification by statin use was not considered. Our findings are also consistent with research showing associations between inflammatory diseases and HF, including non-ischaemic forms of HF [40]. Potential mechanisms underlying this association could include subclinical ischemia, or impaired iron homeostasis [41] leading to dysfunction of the myocyte, among other mechanisms. HF is considered one of the greatest public threats of our time [42], and tools aiding the identification of individuals at increased risk of HF may become of great value for patients, clinicians, and health systems. However, the finding regarding the predictive capacity of hsCRP for HF, although promising, should be considered hypothesis-generating, and should be replicated in larger cohorts of statin users.
Finally, we also observed a strong, independent association between hsCRP levels and VTE, although it is possible that this link could operate via alternative, non-vascular mechanisms not accounted for in the models, such as increased incidence of cancer [43], or bone fractures [44], among others. Interestingly statins, which markedly lower hsCRP levels, reduced the incidence of VTE in the JUPITER trial [45]. Studies using adjudicated events rather than ICD-9 codes, which are known to have a modest validity for VTE particularly in non-high risk individuals [46], and adjusting for body mass index [47] will provide more insight on this association.
Study Limitations
Some potential limitations of this study are worth discussing. First, information on prevalent inflammatory diseases and on the use of immunosuppressive drugs was not collected in MESA Visit 1. Nevertheless, because MESA included overall “healthy” adults [18], their prevalence would be expected to be low. Moreover, the results were robust to the exclusion of individuals with recent joint inflammation.
Second, the multivariable models used in the analyses were the same across all endpoints, rather than tailored to each condition. This could partly explain the stronger associations between hsCRP and the exploratory, non-atherosclerotic CVD endpoints, and the small changes in estimates between adjustment for multivariable models 2 and 3 for those endpoints. However, the factors included in the models are also considered key factors leading to the development of HF among individuals free of known CVD [48]; therefore, this is unlikely to fully explain the strong association between hsCRP and incident HF observed among statin users.
Third, inclusion of two study populations and assessment of multiple endpoints may have increased the risk of finding spurious associations due to chance. Nonetheless, the strong association between hsCRP and HF was robust and present in all analyses performed in the statin user group, including Cox regression, AUC and AIC. Also, this association is consistent with prior evaluations performed in MESA [34-39].
Finally, the limited sample size particularly of the statin user group precluded performing analyses stratified by age, sex and race-ethnicity. Future studies in larger populations will help better understand the specific prognostic value of hsCRP in each of these subgroups.
5. Conclusions
Our findings support the role of inflammation as an upstream mechanism in the pathogenesis of a number of diseases, although for ASCVD, inflammation may be a downstream mediator resulting from the presence of traditional risk factors. From a risk assessment standpoint, hsCRP, the most widely used measure of inflammation, does not improve ASCVD risk prediction beyond traditional risk factors in either statin-naïve individuals or in patients already using statins. On the other hand, hsCRP may have a role for the prediction of incident HF in statin users; however, this observation should be replicated in larger cohorts of statin users.
Supplementary Material
Highlights.
- HsCRP, the most widely used measure of inflammation, does not improve ASCVD risk prediction beyond traditional risk factors in statin-naïve individuals
- The utility of hsCRP for ASCVD prediction is also modest in individuals treated with statins
- Nevertheless, hsCRP may have a role for the prediction of incident HF in statin users, although this observation should be replicated in larger cohorts of statin users
Acknowledgments
The authors thank the other investigators, the staff, and the participants of MESA for their valuable contributions. A full list of participating MESA investigators and institutions can be found at http://www.mesa-nhlbi.org
Funding: This research was supported by contracts HHSN268201500003I, N01-HC-95159, N01-HC-95160, N01-HC-95161, N01-HC-95162, N01-HC-95163, N01-HC-95164, N01-HC-95165, N01-HC-95166, N01-HC-95167, N01-HC-95168 and N01-HC-95169 from the National Heart, Lung, and Blood Institute, and by grants UL1-TR-000040, UL1-TR-001079, and UL1-TR-001420 from NCATS.
Abbreviations And Acronyms
- ACC/AHA
American College of Cardiology/American Heart Association
- AF
atrial fibrillation
- AUC
area under the receiver-operator characteristic curve
- CANTOS
Canakinumab Anti-inflammatory Thrombosis Outcomes Study
- CHD
coronary heart disease
- CVD
cardiovascular disease
- HDL
high density lipoprotein
- HF
heart failure
- HsCRP
high sensitivity C-reactive protein
- ICD-9
International Classification of Diseases, Ninth Revision
- JUPITER
Justification for the Use of Statins in Primary Prevention an Intervention Trial Evaluating Rosuvastatin
- MESA
Multi-Ethnic Study of Atherosclerosis
- VTE
venous thromboembolism
Footnotes
Authorship and Submission Statement: All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation. All authors have contributed significantly to the preparation of this manuscript, and have approved the final article. The work described in the present manuscript has not been published previously, is not under consideration for publication elsewhere, and, if accepted, will not be published elsewhere in the same form, in English or in any other language, including electronically without the written consent of the copyright-holder.
Declaration of Conflicts of Interest: The authors declare that they have no conflicts of interest relevant to the content of this manuscript.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Ross R. The pathogenesis of atherosclerosis: a perspective for the 1990s. Nature. 1993;362:801–9. doi: 10.1038/362801a0. [DOI] [PubMed] [Google Scholar]
- 2.Alexander RW. Inflammation and coronary artery disease. N Engl J Med. 1994;331:468–9. doi: 10.1056/NEJM199408183310709. [DOI] [PubMed] [Google Scholar]
- 3.Ridker PM, Cushman M, Stampfer MJ, Tracy RP, Hennekens CH. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. N Engl J Med. 1997;336(14):973–9. doi: 10.1056/NEJM199704033361401. [DOI] [PubMed] [Google Scholar]
- 4.Ridker PM. From C-Reactive Protein to Interleukin-6 to Interleukin-1: Moving Upstream To Identify Novel Targets for Atheroprotection. Circ Res. 2016;118(1):145–56. doi: 10.1161/CIRCRESAHA.115.306656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Coussens LM, Werb Z. Inflammation and cancer. Nature. 2002;420(6917):860–7. doi: 10.1038/nature01322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Erlinger TP, Platz EA, Rifai N, Helzlsouer KJ. C-reactive protein and the risk of incident colorectal cancer. JAMA. 2004;291(5):585–90. doi: 10.1001/jama.291.5.585. [DOI] [PubMed] [Google Scholar]
- 7.Wang J, Lee IM, Tworoger SS, et al. Plasma C reactive protein and risk of breast cancer in two prospective studies and a meta-analysis. Cancer Epidemiol Biomarkers Prev. 2015;24(8):1199–206. doi: 10.1158/1055-9965.EPI-15-0187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nimmo MA, Leggate M, Viana JL, King JA. The effect of physical activity on mediators of inflammation. Diabetes Obes Metab. 2013;15(3):51–60. doi: 10.1111/dom.12156. [DOI] [PubMed] [Google Scholar]
- 9.Allison MA, Jensky NE, Marshall SJ, Bertoni AG, Cushman M. Sedentary behavior and adiposity-associated inflammation: the Multi-Ethnic Study of Atherosclerosis. Am J Prev Med. 2012;42(1):8–13. doi: 10.1016/j.amepre.2011.09.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Casas R, Sacanella E, Urpí-Sardà M, et al. Long-Term Immunomodulatory Effects of aMediterranean Diet in Adults at High Risk of Cardiovascular Disease in the PREvención conDIeta MEDiterránea (PREDIMED) Randomized Controlled Trial. J Nutr. 2016;146(9):1684–93. doi: 10.3945/jn.115.229476. [DOI] [PubMed] [Google Scholar]
- 11.Patnode CD, Evans CV, Senger CA, Redmond N, Lin JS. Behavioral Counseling to Promote a Healthful Diet and Physical Activity for Cardiovascular Disease Prevention in Adults Without Known Cardiovascular Disease Risk Factors: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. 2017;318(2):175–193. doi: 10.1001/jama.2017.3303. [DOI] [PubMed] [Google Scholar]
- 12.Khera AV, Emdin CA, Drake I, et al. Genetic Risk, Adherence to a Healthy Lifestyle, and Coronary Disease. N Engl J Med. 2016;375(24):2349–2358. doi: 10.1056/NEJMoa1605086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ridker PM, Buring JE, Rifai N, Cook NR. Development and validation of improved algorithms for the assessment of global cardiovascular risk in women: the Reynolds Risk Score. JAMA. 2007;297(6):611–619. doi: 10.1001/jama.297.6.611. [DOI] [PubMed] [Google Scholar]
- 14.Goff DC, Jr, Lloyd-Jones DM, Bennett G, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 Suppl 2):S49–73. doi: 10.1161/01.cir.0000437741.48606.98. [DOI] [PubMed] [Google Scholar]
- 15.Ridker PM, Danielson E, Fonseca FA, et al. JUPITER Study Group. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008;359(21):2195–207. doi: 10.1056/NEJMoa0807646. [DOI] [PubMed] [Google Scholar]
- 16.Ridker PM, Everett BM, Thuren T, et al. CANTOS Trial Group. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N Engl J Med. 2017 Aug 27; doi: 10.1056/NEJMoa1707914. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 17.Yousuf O, Mohanty BD, Martin SS, et al. High-sensitivity C-reactive protein and cardiovascular disease: a resolute belief or an elusive link? J Am Coll Cardiol. 2013;62(5):397–408. doi: 10.1016/j.jacc.2013.05.016. [DOI] [PubMed] [Google Scholar]
- 18.Bild DE, Bluemke DA, Burke GL, et al. Multi-ethnic study of atherosclerosis: objectives and design. Am J Epidemiol. 2002;156(9):871–81. doi: 10.1093/aje/kwf113. [DOI] [PubMed] [Google Scholar]
- 19.Brooks GC, Blaha MJ, Blumenthal RS. Relation of C-reactive protein to abdominal adiposity. Am J Cardiol. 2010;106(1):56–61. doi: 10.1016/j.amjcard.2010.02.017. [DOI] [PubMed] [Google Scholar]
- 20.Pencina MJ, D'Agostino RB, Vasan RS. Statistical methods for assessment of added usefulness of new biomarkers. Clin Chem Lab Med. 2010;48(12):1703–11. doi: 10.1515/CCLM.2010.340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Akaike H. A new look at the statistical model identification. IEEE Transactions on Automatic Control. 1974;19(6):716–723. doi: 10.1109/TAC.1974.1100705. MR 0423716. [DOI] [Google Scholar]
- 22.Prasad K. C-reactive protein (CRP)-lowering agents. Cardiovasc Drug Rev. 2006;24(1):33–50. doi: 10.1111/j.1527-3466.2006.00033.x. [DOI] [PubMed] [Google Scholar]
- 23.StataCorp. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP; 2015. [Google Scholar]
- 24.Ridker PM, MacFadyen JG, Thuren T, Everett BM, Libby P, Glynn RJ CANTOS Trial Group. Effect of interleukin-1β inhibition with canakinumab on incident lung cancer in patients with atherosclerosis: exploratory results from a randomised, double-blind, placebo-controlled trial. Lancet. 2017;390(10105):1833–1842. doi: 10.1016/S0140-6736(17)32247-X. [DOI] [PubMed] [Google Scholar]
- 25.Al Rifai M, DeFilippis AP, McEvoy JW, et al. The relationship between smoking intensity and subclinical cardiovascular injury: The Multi-Ethnic Study of Atherosclerosis (MESA) Atherosclerosis. 2017;258:119–130. doi: 10.1016/j.atherosclerosis.2017.01.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lakoski SG, Cushman M, Palmas W, Blumenthal R, D'Agostino RB, Jr, Herrington DM. The relationship between blood pressure and C-reactive protein in the Multi-Ethnic Study of Atherosclerosis (MESA) J Am Coll Cardiol. 2005;46(10):1869–74. doi: 10.1016/j.jacc.2005.07.050. [DOI] [PubMed] [Google Scholar]
- 27.Emerging Risk Factors Collaboration. Kaptoge S, Di Angelantonio E, Pennells L, et al. C-reactive protein, fibrinogen, and cardiovascular disease prediction. N Engl J Med. 2012;367(14):1310–20. doi: 10.1056/NEJMoa1107477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Buckley DI, Fu R, Freeman M, Rogers K, Helfand M. C-reactive protein as a risk factor for coronary heart disease: a systematic review and meta-analyses for the U.S. Preventive Services Task Force. Ann Intern Med. 2009;151:483–95. doi: 10.7326/0003-4819-151-7-200910060-00009. [DOI] [PubMed] [Google Scholar]
- 29.Yeboah J, McClelland RL, Polonsky TS, et al. Comparison of novel risk markers for improvement in cardiovascular risk assessment in intermediate-risk individuals. JAMA. 2012;308(8):788–95. doi: 10.1001/jama.2012.9624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Yeboah J, Young R, McClelland RL, et al. Utility of Nontraditional Risk Markers in Atherosclerotic Cardiovascular Disease Risk Assessment. J Am Coll Cardiol. 2016;67(2):139–47. doi: 10.1016/j.jacc.2015.10.058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Blaha MJ, Budoff MJ, DeFilippis AP, et al. Associations between C-reactive protein, coronary artery calcium, and cardiovascular events: implications for the JUPITER population from MESA, a population-based cohort study. Lancet. 2011;378(9792):684–92. doi: 10.1016/S0140-6736(11)60784-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kavousi M, Elias-Smale S, Rutten JH, et al. Evaluation of newer risk markers for coronary heart disease risk classification: a cohort study. Ann Intern Med. 2012;156(6):438–44. doi: 10.7326/0003-4819-156-6-201203200-00006. [DOI] [PubMed] [Google Scholar]
- 33.Piepoli MF, Hoes AW, Agewall S, et al. Authors/Task Force Members. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR) Eur Heart J. 2016;37(29):2315–81. doi: 10.1093/eurheartj/ehw106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Rosen BD, Cushman M, Nasir K, et al. Relationship between C-reactive protein levels and regional left ventricular function in asymptomatic individuals: the Multi-Ethnic Study of Atherosclerosis. J Am Coll Cardiol. 2007;49(5):594–600. doi: 10.1016/j.jacc.2006.09.040. [DOI] [PubMed] [Google Scholar]
- 35.Yan RT, Fernandes V, Yan AT, et al. Fibrinogen and left ventricular myocardial systolic function: The Multi-Ethnic Study of Atherosclerosis (MESA) Am Heart J. 2010;160(3):479–86. doi: 10.1016/j.ahj.2010.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Choi EY, Yan RT, Fernandes VR, Opdahl A, Gomes AS, Almeida AL, Wu CO, Liu K, Carr JJ, McClelland RL, Bluemke DA, Lima JA. High-sensitivity C-reactive protein as an independent predictor of progressive myocardial functional deterioration: the multiethnic study of atherosclerosis. Am Heart J. 2012;164(2):251–8. doi: 10.1016/j.ahj.2012.05.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Harhay MO, Tracy RP, Bagiella E, et al. Relationship of CRP, IL-6, and fibrinogen with right ventricular structure and function: the MESA-Right Ventricle Study. Int J Cardiol. 2013;168(4):3818–24. doi: 10.1016/j.ijcard.2013.06.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Yan AT, Yan RT, Cushman M, et al. Relationship of interleukin-6 with regional and global left-ventricular function in asymptomatic individuals without clinical cardiovascular disease: insights from the Multi-Ethnic Study of Atherosclerosis. Eur Heart J. 2010;31(7):875–82. doi: 10.1093/eurheartj/ehp454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Bekwelem W, Lutsey PL, Loehr LR, et al. White blood cell count, C-reactive protein, and incident heart failure in the Atherosclerosis Risk in Communities (ARIC) Study. Ann Epidemiol. 2011;21(10):739–48. doi: 10.1016/j.annepidem.2011.06.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Onat A, Özbek M, Hayıroğlu MI. Rheumatoid Arthritis and Risk of Nonischemic Heart Failure: Closely Related Common Soil. J Am Coll Cardiol. 2017;70(5):687–688. doi: 10.1016/j.jacc.2017.04.064. [DOI] [PubMed] [Google Scholar]
- 41.Wessling-Resnick M. Iron homeostasis and the inflammatory response. Annu Rev Nutr. 2010;30:105–22. doi: 10.1146/annurev.nutr.012809.104804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Benjamin EJ, Blaha MJ, Chiuve SE, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation. 2017;135(10):e146–e603. doi: 10.1161/CIR.0000000000000485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Hisada Y, Mackman N. Cancer-associated pathways and biomarkers of venous thrombosis. Blood. 2017 Aug;:14. doi: 10.1182/blood-2017-03-743211. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Cauley JA, Barbour KE, Harrison SL, et al. Inflammatory Markers and the Risk of Hip and Vertebral Fractures in Men: the Osteoporotic Fractures in Men (MrOS) J Bone Miner Res. 2016;31(12):2129–2138. doi: 10.1002/jbmr.2905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Glynn RJ, Danielson E, Fonseca FA, Genest J, Gotto AM, Jr, Kastelein JJ, Koenig W, Libby P, Lorenzatti AJ, MacFadyen JG, Nordestgaard BG, Shepherd J, Willerson JT, Ridker PM. A randomized trial of rosuvastatin in the prevention of venous thromboembolism. N Engl J Med. 2009;360(18):1851–61. doi: 10.1056/NEJMoa0900241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Tamariz L, Harkins T, Nair V. A systematic review of validated methods for identifying venous thromboembolism using administrative and claims data. Pharmacoepidemiol Drug Saf. 2012;21(1):154–62. doi: 10.1002/pds.2341. [DOI] [PubMed] [Google Scholar]
- 47.Cushman M, O'Meara ES, Heckbert SR, Zakai NA, Rosamond W, Folsom AR. Body size measures, hemostatic and inflammatory markers and risk of venous thrombosis: The Longitudinal Investigation of Thromboembolism Etiology. Thromb Res. 2016;144:127–32. doi: 10.1016/j.thromres.2016.06.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Hippisley-Cox J, Coupland C. Development and validation of risk prediction equations to estimate future risk of heart failure in patients with diabetes: a prospective cohort study. BMJ Open. 2015;5(9):e008503. doi: 10.1136/bmjopen-2015-008503. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.