

Abstract
Background
Although pedobarographic measurement is increasingly used for clinical and research purposes, relatively few published studies have investigated normative data. This study examined pedobarographic findings in young healthy adults with regard to sex-related differences and correlations among measurement indices.
Methods
Twenty young healthy adults (mean age, 22.4 years; standard deviation, 1.2 years; and 10 males and 10 females) were included. Weight bearing anteroposterior (AP) and lateral foot radiographs were taken, and dynamic pedobarographic data during treadmill walking and maximum ankle dorsiflexion were obtained. AP talo-first metatarsal angle, naviculocuboid overlap, lateral talo-first metatarsal angle, and plantar soft tissue thickness were measured on foot radiographs. Pedobarographic data including peak pressure and pressure-time integral were measured on five plantar segments: medial forefoot (MFF), lateral forefoot (LFF), medial midfoot (MMF), lateral midfoot (LMF), and heel.
Results
Male and female subjects significantly differed in body mass index (BMI, p < 0.001), AP talo-first metatarsal angle (p = 0.018), soft tissue thickness under the metatarsal head (p = 0.040) and calcaneal tuberosity (p < 0.001), maximum dorsiflexion during stance phase (p = 0.041), peak pressure on the MFF (p = 0.005) and LFF (p = 0.004), and pressure-time integral on the MFF (p = 0.018) and heel (p = 0.001). BMI was significantly correlated with soft tissue thickness under the metatarsal head (r = 0.521, p = 0.018) and calcaneal tuberosity (r = 0.585, p = 0.007), peak pressure on the MFF (r = 0.601, p = 0.005) and LFF (r = 0.487, p = 0.029), pressure-time integral on the heel (r = 0.552, p = 0.012), and total pressure-time integral (r = 0.755, p < 0.001). Maximum dorsiflexion demonstrated significant negative correlations with pressure-time integral on the MFF (r = −0.595, p = 0.007) and total pressure-time integral (r = −0.492, p = 0.032). Pressure-time integral varus/valgus index was significantly correlated with pressuretime integral forefoot/heel index (r = 0.472, p = 0.036).
Conclusions
Sex-related differences in pedobarographic examination were observed, which could provide useful information in setting appropriate treatment goals and obtaining appropriate control data. The effects of subtalar motion in distributing plantar pressure should be investigated in a future study.
Keywords: Foot, Pressure, Normal, Sex, Difference, Radiograph
Foot pressure measurement has been gaining in popularity since it was introduced to clinical and research use. Many conditions are associated with abnormal regional foot pressure and its distribution, including metatarsalgia, corn and callosity, heel pain, various foot deformities, and diabetic foot ulcer.1,2,3,4,5,6,7) Furthermore, some recent studies have investigated the relationship between plantar pressure and other musculoskeletal conditions, such as patellofemoral pain syndrome and leg length discrepancy.8,9)
Abnormally increased plantar pressure is considered to contribute to mechanical pain, and abnormal plantar pressure distribution can reflect biomechanical imbalance. 7,10) These relationships are the basis for the clinical use of pedobarography. Pressure is defined as force per unit area applied in a direction perpendicular to the surface of an object.11) Therefore, plantar pressure can be affected by many factors, such as subject's weight, contact surface, and acceleration at the time of ground contact, which could be modulated by mechanical properties of plantar soft tissue.12,13)
Peak pressure and pressure-time integral have been the most commonly used indices for the consideration of plantar pressure in clinical conditions. Peak plantar pressure was shown to associate with diabetic neuropathy and diabetic foot ulcer as well as foot discomfort in normal subjects.14,15) Pressure-time integral is also known to correlate with foot pain in patients with pes cavus.16)
However, foot pressure characteristics are not sufficiently well understood in normal subjects. Furthermore, few studies have assessed foot pressure features along with radiographic findings. The establishment of normative data would help to clearly define pathologic conditions as well as to set appropriate treatment goals. The authors hypothesized that male and female subjects would have different pedobarographic characteristics. So, the aim of this study was to examine the pedobarographic characteristics of young healthy adults with no foot problems with regard to sex-related differences and correlations among measurement indices.
METHODS
This prospective study was approved by the Institutional Review Board of Chung-Ang University (IRB No. 1041078-201411-HR-169-01), and informed consent was obtained from all participants.
Participants
Young adult volunteers were recruited and asked if they had any medical or surgical conditions. Of the subjects without any medical or surgical issues, those with the following conditions were further excluded: (1) previous foot or ankle trauma, (2) infection, (3) tumor, (4) congenital anomaly, (5) neuromuscular disease, (6) foot and ankle pain or discomfort, and (7) any other condition that could limit the subjects' activity. Ten male and 10 female young adults were ultimately included. Demographic data were collected and recorded, including age, sex, height, and weight. Anteroposterior (AP) and lateral foot radiographs were taken with a UT 2000 X-ray machine (Philips Research, Eindhoven, The Netherlands) set to 50 kVp and 5 mAs at a source-to-image distance of approximately 100 cm, with the participants in a standing position.
Radiographic Measurement
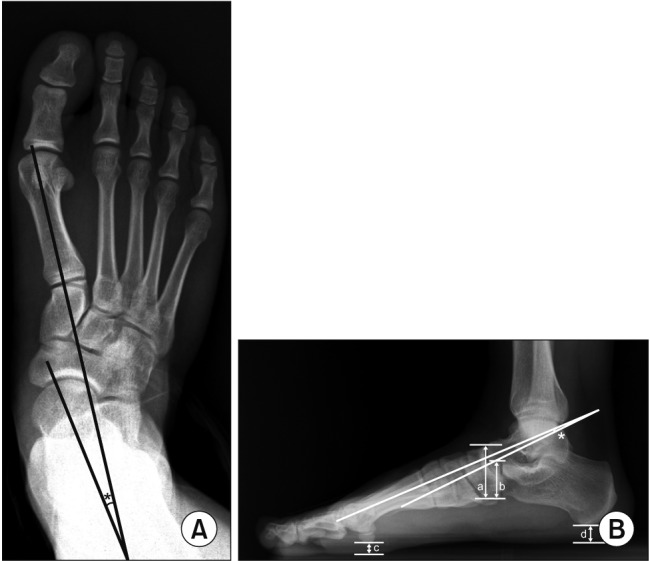
Radiographic indices were measured to evaluate the foot shape. AP talo-first metatarsal angle was measured on the AP weight bearing foot radiograph, and naviculocuboid overlap and lateral talo-first metatarsal angle were measured on the lateral weight bearing foot radiograph. The selection of radiographic indices was based on a previous study that investigated the reliability and validity of foot radiographic measurements.17) Plantar soft tissue thickness was measured under the first metatarsal head and calcaneal tuberosity (Fig. 1). Radiographic measurements were performed by an orthopedic surgeon (BCC) with 8 years of experience.
Fig. 1. Radiographic measurements. (A) On an anteroposterior weight bearing foot radiograph, anteroposterior talo-first metatarsal angle is measured (asterisk), which is defined as the angle between a line bisecting the first metatarsal bone and another line bisecting the talus. (B) On a lateral weight bearing foot radiograph, naviculocuboid overlap, lateral talo-first metatarsal angle, and plantar soft tissue thickness are measured. Naviculocuboid overlap is the ratio between the vertical height of navicular (a) and the vertical overlap (b) between the navicular and the cuboid. Lateral talo-first metatarsal angle (asterisk) is the angle between a line bisecting the first metatarsal bone and another line bisecting the talus. Plantar soft tissue thickness is measured under the first metatarsal head (actually sesamoids, c) and under the calcaneal tuberosity (d).
Measurement of Dynamic Foot Pressure and Maximum Ankle Dorsiflexion During Gait
Dynamic foot pressure measurements and kinematic data were collected simultaneously. For the acquisition of ankle kinematic data, markers were placed on all participants by a single skillful operator (YJK). Four reflective skin markers according to Plug in Gait marker set were placed on the heel, dorsum of the second metatarsal head, lateral malleolus, and anterior shank. The movement of each marker was captured by six motion capture cameras at a sampling rate of 100 Hz, retrieved, and analyzed digitally using a Vicon MX T-10 system (Vicon Motion Systems, Oxford, UK). As kinematic data, maximum ankle dorsiflexion was collected and recorded. Three gait trials were conducted and averaged to a single data set.
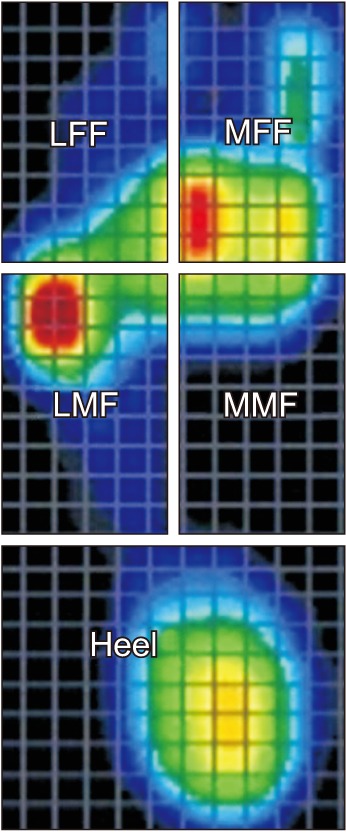
Dynamic foot pressure was measured using a treadmill pedobarograph system, FDM-TDSL (Zebris Medical, Isny Im Allgäu, Germany). The system has a belt consisting of a 150 × 50 cm2 running surface and 94.8 × 40.6 cm2 sensor surface containing 5,376 pressure-sensing cell/cm2. The sensors were connected to a computer to show the distribution of pressure at a sampling rate of 100 Hz as the subjects walked barefoot on the treadmill. The walking speed was set to be 3.2 km/hr, and all participants were asked to practice exercise walking at the predetermined speed for 5 minutes before testing. After the foot pressure data were obtained, the information was collected and processed with use of software specifically designed for the treadmill foot pressure measurement system. The area of measurement was divided equally into anterior, middle, and posterior thirds, and the anterior and middle thirds were further equally divided into medial and lateral halves.17,18) Therefore, five segments were defined: medial forefoot (MFF), lateral forefoot (LFF), medial midfoot (MMF), lateral midfoot (LMF), and heel (Fig. 2). The peak pressure and pressure-time integral were retrieved for the five segments of the foot. The distribution of pressuretime integral was calculated as a percentage reflecting the proportion of each segment of the sum of the five segments. The peak pressure varus/valgus index was defined as [(MFF + MMF) − (LFF + LMF)] / (MFF + MMF + LFF + LMF).17,18) The peak pressure forefoot/heel index was defined as (MFF − heel) / (MFF + heel). The pressure-time integral varus/valgus index was calculated using the same method as peak pressure, and the pressure-time integral forefoot/heel index was defined as (MFF + LFF − heel) / (MFF + LFF + heel).
Fig. 2. Pedobarograph is analyzed by dividing the plantar surface into five segments. The foot consists of anterior third, middle third, and posterior third. Anterior and middle thirds are further divided into medial and lateral segments, producing medial forefoot (MFF), lateral forefoot (LFF), medial midfoot (MMF), and lateral midfoot (LMF). The posterior third is the heel segment.
Statistical Analysis
A priori sample size calculation was performed according to a previous study19) at the setting of an alpha error of 0.05 and a power of 0.8. Descriptive statistics including mean and standard deviation (SD) were used to summarize the patients' demographic data, radiographic measurements, kinematic data, and pedobarographic data. The normality of data distribution was determined using the Kolmogorov-Smirnov test. The variables were compared between male and female subjects using Student t-test. The correlations among variables were analyzed using Pearson correlation coefficients. Statistical analysis was performed using SPSS ver. 20.0 (IBM Corp., Armonk, NY, USA), and significance was set at p < 0.05.
RESULTS
Data from the 20 right feet of the 20 subjects were selected and analyzed. The mean age of the subjects was 22.4 years (SD, 1.2 years). There were 10 male subjects (mean age, 22.0 years; SD, 1.4 years) and 10 female subjects (mean age, 22.8 years; SD, 0.9 years). The male subjects had a mean height of 172.4 cm (SD, 3.7 cm), mean weight of 70.9 kg (SD, 5.4 kg), and mean body mass index (BMI) of 23.9 kg/cm2 (SD, 1.8 kg/cm2). The female subjects had a mean height of 161.6 cm (SD, 4.6 cm), mean weight of 52.2 kg (SD, 5.0 kg), and mean BMI of 20.0 kg/cm2 (SD, 1.9 kg/cm2).
On radiographic measurements, the mean AP talo-first metatarsal angle was 9.9° (SD, 8.0°), the mean naviculocuboid overlap was 0.6 (SD, 0.2), and the mean lateral talo-first metatarsal angle was 4.4° (SD, 6.7°). The mean plantar soft tissue thickness was 8.0 mm (SD, 2.3 mm) under the first metatarsal head and 11.7 mm (SD, 2.2 mm) under the calcaneal tuberosity.
Maximum ankle dorsiflexion during stance phase was 18.7° (SD, 7.2°) on average. The mean peak pressure on the MFF, LFF, MMF, LMF, and heel was 30.3 N/cm2 (SD, 8.0 N/cm2), 22.0 N/cm2 (SD, 8.0 N/cm2), 19.9 N/cm2 (SD, 6.3 N/cm2), 19.5 N/cm2 (SD, 7.1 N/cm2), and 26.9 N/cm2 (SD, 4.3 N/ cm2), respectively. The mean pressure-time integral on the MFF, LFF, MMF, LMF, and heel was 13.2 N·s/ cm2 (SD, 6.0 N·s/cm2), 7.6 N·s/cm2 (SD, 4.9 N·s/cm2), 3.3 N·s/cm2 (SD, 2.0 N·s/cm2), 8.5 N·s/cm2 (SD, 3.1 N·s/cm2), and 15.5 N·s/cm2 (SD, 3.3 N·s/cm2), respectively, which corresponded to 26.7% (SD, 9.9%), 15.5% (SD, 8.1%), 7.0% (SD, 3.8%), 18.0% (SD, 6.6%), and 32.7% (SD, 6.2%), respectively.
Male and female subjects showed significantly different BMI (p < 0.001), AP talo-first metatarsal angle (p = 0.018), soft tissue thickness under the metatarsal head (p = 0.040) and the calcaneal tuberosity (p < 0.001), maximum dorsiflexion during stance phase (p = 0.041), peak pressure on the MFF (p = 0.005) and LFF (p = 0.004), and pressuretime integral on the MFF (p = 0.018) and heel (p = 0.001). No sex-related differences were observed in peak pressure varus/valgus index, peak pressure forefoot/heel index, pressure-time integral varus/valgus index, or pressuretime integral forefoot/heel index (Table 1).
Table 1. Data Summary and Difference between Male and Female Subjects.
| Variable | Male | Female | p-value |
|---|---|---|---|
| No. of subjects | 10 | 10 | - |
| Age (yr) | 22.0 ± 1.4 | 22.8 ± 0.9 | 0.151 |
| Height (cm) | 172.4 ± 3.7 | 161.6 ± 4.6 | < 0.001 |
| Weight (kg) | 70.9 ± 5.4 | 52.2 ± 5.0 | < 0.001 |
| Body mass index (kg/m2) | 23.9 ± 1.8 | 20.0 ± 1.9 | < 0.001 |
| Radiographic measurement | |||
| AP talo–1st MT angle (°) | 5.8 ± 6.7 | 14.0 ± 7.3 | 0.018 |
| NC overlap (%) | 55.4 ± 21.0 | 64.1 ± 17.2 | 0.323 |
| Lat talo–1st MT angle (°) | 1.8 ± 5.4 | 6.9 ± 7.3 | 0.091 |
| MT soft tissue thickness (mm) | 9.1 ± 1.8 | 7.0 ± 2.4 | 0.040 |
| Heel soft tissue thickness (mm) | 13.2 ± 1.5 | 10.1 ± 1.6 | < 0.001 |
| Maximum ankle DF (°) | 14.9 ± 3.5 | 22.1 ± 9.2 | 0.041 |
| Dynamic pedobarograph | |||
| Peak pressure (N/cm2) | |||
| MFF | 34.3 ± 6.3 | 25.9 ± 5.5 | 0.005 |
| LFF | 26.1 ± 6.9 | 17.2 ± 5.3 | 0.004 |
| MMF | 17.9 ± 8.4 | 23.1 ± 6.1 | 0.130 |
| LMF | 18.2 ± 5.6 | 17.0 ± 4.0 | 0.587 |
| Heel | 28.1 ± 4.4 | 25.6 ± 3.3 | 0.161 |
| Varus/valgus index | 0.08 ± 0.1 | 0.18 ± 0.1 | 0.088 |
| Forefoot/heel index | 0.09 ± 0.2 | 0.00 ± 0.1 | 0.144 |
| Pressure-time integral (N·s/cm2) | |||
| MFF | 214,565.6 ± 58,427.4 | 129,139.7 ± 85,697.2 | 0.018 |
| LFF | 110,719.6 ± 66,340.0 | 93,713.5 ± 60,193.6 | 0.556 |
| MMF | 62,144.2 ± 28,512.4 | 34,159.3 ± 31,265.9 | 0.051 |
| LMF | 152,185.6 ± 43,529.9 | 116,827.3 ± 51,751.4 | 0.116 |
| Heel | 255,374.7 ± 36,546.2 | 185,314.5 ± 37,591.3 | 0.001 |
| Varus/valgus index | 0.03 ± 0.2 | −0.15 ± 0.4 | 0.190 |
| Forefoot/heel index | 0.10 ± 0.2 | 0.04 ± 0.3 | 0.573 |
Values are presented as mean ± standard deviation.
AP: anteroposterior, MT: metatarsal, NC: naviculocuboid, Lat: lateral, DF: dorsiflexion, MFF: medial forefoot, LFF: lateral forefoot, MMF: medial midfoot, LMF: lateral midfoot.
BMI was significantly correlated with soft tissue thickness under the metatarsal head (r = 0.521, p = 0.018) and calcaneal tuberosity (r = 0.585, p = 0.007), peak pressure on the MFF (r = 0.601, p = 0.005) and LFF (r = 0.487, p = 0.029), pressure-time integral on the heel (r = 0.552, p = 0.012), and total pressure-time integral (r = 0.755, p < 0.001). Maximum dorsiflexion demonstrated a significant negative correlation with pressure-time integral on the MFF (r = −0.595, p = 0.007) and total pressure-time integral (r = −0.492, p = 0.032). Pressure-time integral varus/ valgus index was significantly correlated with pressuretime integral forefoot/heel index (r = 0.472, p = 0.036), pressure-time integral on the MFF (r = 0.772, p < 0.001), MMF (r = 0.620, p = 0.004), and peak pressure varus/valgus index (r = 1.000, p < 0.001) (Table 2).
Table 2. Correlations between the Radiographic and Pedobarographic Variables.
| Variable | BMI | MaxDF | AP talo–1st MT angle | NC overlap | Lat talo–1st MT angle | MT thickness | Heel thickness | MFF (PP) | LFF (PP) | MMF (PP) | LMF (PP) | Heel (PP) | Varus/valgus (PP) | Forefoot/heel (PP) | MFF (PTI) | LFF (PTI) | MMF (PTI) | LMF (PTI) | Heel (PTI) | Varus/valgus (PTI) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MaxDF | −0.248 (p = 0.307) | |||||||||||||||||||
| AP talo–1st MT angle | −0.287 (p = 0.221) | 0.243 (p = 0.316) | ||||||||||||||||||
| NC overlap | −0.273 (p = 0.244) | 0.010 (p = 0.968) | 0.212 (p = 0.370) | |||||||||||||||||
| Lat talo–1st MT angle | −0.234 (p = 0.322) | −0.169 (p = 0.489) | 0.454 (p = 0.045) | 0.571 (p = 0.008) | ||||||||||||||||
| MT thickness | 0.521 (p = 0.018) | 0.009 (p = 0.970) | −0.057 (p = 0.813) | −0.509 (p = 0.022) | −0.410 (p = 0.072) | |||||||||||||||
| Heel thickness | 0.585 (p = 0.007) | −0.125 (p = 0.610) | −0.180 (p = 0.447) | −0.307 (p = 0.188) | −0.329 (p = 0.157) | 0.514 (p = 0.020) | ||||||||||||||
| MFF (PP) | 0.601 (p = 0.005) | −0.372 (p = 0.116) | 0.164 (p = 0.490) | −0.261 (p = 0.267) | −0.103 (p = 0.667) | 0.523 (p = 0.018) | 0.668 (p = 0.001) | |||||||||||||
| LFF (PP) | 0.487 (p = 0.029) | −0.024 (p = 0.921) | −0.078 (p = 0.745) | −0.401 (p = 0.080) | −0.529 (p = 0.017) | 0.485 (p = 0.030) | 0.728 (p < 0.001) | 0.671 (p = 0.001) | ||||||||||||
| MMF (PP) | −0.109 (p = 0.647) | 0.072 (p = 0.770) | 0.152 (p = 0.522) | 0.058 (p = 0.808) | 0.164 (p = 0.490) | −0.002 (p = 0.994) | −0.179 (p = 0.450) | 0.041 (p = 0.865) | −0.224 (p = 0.342) | |||||||||||
| LMF (PP) | 0.163 (p = 0.492) | 0.232 (p = 0.339) | −0.112 (p = 0.638) | −0.184 (p = 0.436) | −0.335 (p = 0.149) | 0.223 (p = 0.345) | 0.298 (p = 0.201) | 0.229 (p = 0.332) | 0.429 (p = 0.059) | 0.515 (p = 0.020) | ||||||||||
| Heel (PP) | 0.401 (p = 0.080) | −0.056 (p = 0.821) | −0.236 (p = 0.317) | 0.131 (p = 0.582) | −0.112 (p = 0.640) | 0.058 (p = 0.809) | 0.023 (p = 0.923) | −0.038 (p = 0.872) | 0.142 (p = 0.549) | −0.112 (p = 0.639) | 0.117 (p = 0.623) | |||||||||
| Varus/valgus (PP) | 0.206 (p = 0.383) | −0.330 (p = 0.167) | −0.089 (p = 0.708) | −0.128 (p = 0.589) | −0.448 (p = 0.048) | 0.218 (p = 0.357) | 0.065 (p = 0.784) | 0.384 (p = 0.095) | 0.477 (p = 0.033) | 0.001 (p = 0.998) | 0.151 (p = 0.526) | −0.014 (p = 0.954) | ||||||||
| Forefoot/heel (PP) | 0.304 (p = 0.192) | −0.293 (p = 0.224) | 0.268 (p = 0.254) | −0.291 (p = 0.214) | −0.053 (p = 0.824) | 0.410 (p = 0.072) | 0.562 (p = 0.010) | 0.855 (p < 0.001) | 0.484 (p = 0.031) | 0.085 (p = 0.722) | 0.108 (p = 0.651) | −0.537 (p = 0.015) | 0.315 (p = 0.177) | |||||||
| MFF (PTI) | 0.431 (p = 0.058) | −0.595 (p = 0.007) | −0.236 (p = 0.317) | −0.193 (p = 0.414) | −0.352 (p = 0.128) | 0.305 (p = 0.192) | 0.154 (p = 0.516) | 0.362 (p = 0.117) | 0.422 (p = 0.064) | −0.222 (p = 0.347) | 0.107 (p = 0.654) | 0.234 (p = 0.321) | 0.772 (p < 0.001) | 0.179 (p = 0.450) | ||||||
| LFF (PTI) | 0.252 (p = 0.284) | −0.409 (p = 0.082) | −0.197 (p = 0.405) | −0.081 (p = 0.734) | 0.254 (p = 0.280) | 0.235 (p = 0.318) | −0.015 (p = 0.949) | −0.046 (p = 0.847) | −0.193 (p = 0.415) | −0.003 (p = 0.990) | 0.065 (p = 0.786) | 0.287 (p = 0.220) | −0.258 (p = 0.271) | −0.177 (p = 0.456) | 0.300 (p = 0.198) | |||||
| MMF (PTI) | 0.406 (p = 0.076) | 0.084 (p = 0.732) | −0.048 (p = 0.841) | −0.134 (p = 0.573) | −0.415 (p = 0.069) | 0.326 (p = 0.161) | 0.345 (p = 0.136) | 0.575 (p = 0.008) | 0.562 (p = 0.010) | −0.022 (p = 0.927) | 0.087 (p = 0.714) | 0.035 (p = 0.885) | 0.620 (p = 0.004) | 0.465 (p = 0.039) | 0.254 (p = 0.280) | −0.556 (p = 0.011) | ||||
| LMF (PTI) | 0.284 (p = 0.225) | 0.183 (p = 0.453) | −0.199 (p = 0.400) | 0.132 (p = 0.580) | 0.015 (p = 0.950) | 0.032 (p = 0.893) | 0.376 (p = 0.102) | 0.087 (p = 0.716) | −0.019 (p = 0.935) | −0.289 (p = 0.217) | −0.152 (p = 0.523) | 0.136 (p = 0.566) | −0.572 (p = 0.008) | 0.030 (p = 0.900) | −0.402 (p = 0.079) | −0.047 (p = 0.844) | 0.093 (p = 0.695) | |||
| Heel (PTI) | 0.552 (p = 0.012) | −0.139 (p = 0.569) | −0.484 (p = 0.031) | −0.093 (p = 0.696) | −0.336 (p = 0.147) | 0.087 (p = 0.715) | 0.568 (p = 0.009) | 0.201 (p = 0.395) | 0.430 (p = 0.059) | −0.566 (p = 0.009) | −0.097 (p = 0.685) | 0.379 (p = 0.099) | −0.023 (p= 0.924) | −0.006 (p = 0.982) | 0.115 (p = 0.630) | −0.105 (p = 0.661) | 0.292 (p = 0.212) | 0.581 (p = 0.007) | ||
| Varus/valgus (PTI) | 0.206 (p = 0.383) | −0.330 (p = 0.167) | −0.089 (p = 0.708) | −0.128 (p = 0.589) | −0.448 (p = 0.048) | 0.218 (p = 0.357) | 0.065 (p = 0.784) | 0.384 (p = 0.095) | 0.477 (p = 0.033) | 0.001 (p = 0.998) | 0.151 (p = 0.526) | −0.014 (p = 0.954) | 1.000 (p < 0.001) | 0.315 (p = 0.177) | 0.772 (p < 0.001) | −0.258 (p = 0.271) | 0.620 (p = 0.004) | −0.572 (p = 0.008) | −0.023 (p = 0.924) | |
| Forefoot/heel (PTI) | 0.137 (p = 0.565) | −0.566 (p = 0.012) | −0.061 (p = 0.797) | −0.114 (p = 0.633) | 0.047 (p = 0.844) | 0.284 (p = 0.226) | −0.144 (p = 0.545) | 0.202 (p = 0.392) | 0.017 (p = 0.944) | 0.155 (p = 0.515) | 0.113 (p = 0.635) | 0.048 (p = 0.840) | 0.472 (p = 0.036) | 0.129 (p = 0.589) | 0.738 (p < 0.001) | 0.634 (p = 0.003) | −0.126 (p = 0.596) | −0.565 (p = 0.009) | −0.435 (p = 0.055) | 0.472 (p = 0.036) |
BMI: body mass index, MaxDF: maximum dorsiflexion, AP: anteroposterior, MT: metatarsal, NC: naviculocuboid, Lat: lateral, MFF: medial forefoot, PP: peak pressure, LFF: lateral forefoot, MMF: medial midfoot, LMF: lateral midfoot, PTI: pressure-time integral.
DISCUSSION
This study investigated dynamic plantar pressure during walking in young healthy adults, focusing on normal values and the distribution of peak pressure and pressure-time integral, sex-related differences, and correlations among the variables. Male subjects demonstrated higher peak pressure on the MFF and LFF and pressure-time integral on the MFF and heel than female subjects. Female subjects demonstrated thinner plantar soft tissue and greater dorsiflexion during gait than male subjects.
Men and women are anatomically different,20) and their anthropometric and biomechanical properties are also considered to differ. However, there have been few studies investigating sex-related differences in foot pressure. A previous study reported a different angle of center of pressure progression during normal gait between the two sexes.2) Another study reported no significant sex-related differences in normalized midfoot contact area or plantar pressure values between males and females.21) Yet, another study found no significant sex differences in peak pressure, contact time, pressure-time integral, or instant of peak pressure, although male subjects had a larger contact area, pressure-time integral, and maximum force in some specific areas.22) These inconsistent results might be attributable to experimental conditions (barefoot vs. in-shoe), measurement area of the foot, and measurement parameters. Our study demonstrated significant sex-related differences in plantar soft tissue thickness, maximum dorsiflexion during stance phase, peak pressure on the MFF and LFF, and pressure-time integral on the MFF and heel. However, we could not further evaluate whether these differences were caused by sex-specific characteristics or by the effect of body size and ankle kinematics due to the small sample size. Multiple regression analysis with a larger number of subjects would help to clarify this issue.
Along with sex-related difference in plantar pressure, a previous study suggested that different ethnic groups might have different foot pressure characteristics.23) Foot pressure measurement is increasingly used for clinical and research purposes in diabetic foot ulcer, footwear or orthosis, foot deformities, and sports activities.1,3,4,14,16,18,24,25,26,27) It is necessary to establish normal data according to sex and ethnic groups in order to help clinicians and researchers set appropriate treatment goals and obtain appropriate control data.
Male subjects demonstrated greater peak pressure on the MFF and LFF as well as greater pressure-time integral on the MFF and heel than female subjects. Male subjects also had greater plantar soft tissue thickness on metatarsal heads and heel. Considering that no participants had any pain or discomfort, the question arises as to the result whether greater soft tissue thickness can bear and adapt to the greater peak pressure or pressure-time integral. Another hypothetical explanation is that male and female subjects have different pressure thresholds for pain and discomfort, but this possibility requires further study. A previous study reported that the location of the sole, the area of the pressure exerted, and the velocity of the pressure could affect pain and discomfort in the human foot,28) which suggests the possibility that males and females might have different pressure thresholds.
Higher BMI was found to correlate with increased peak pressure on the MFF and LFF, pressure-time integral on the heel, and total pressure-time integral as well as greater plantar soft tissue thickness. Currently, it remains unknown whether the thicker plantar soft tissue could capacitate the increased peak plantar pressure and pressure-time integral, or whether the increased loading to the plantar surface would cause discomfort and pain as a pathogenetic condition in obese subjects. A more comprehensive study including both normal controls and patients with pressure-related disease could elucidate this issue.
Maximum dorsiflexion was negatively correlated with pressure-time integral on the MFF and total pressuretime integral. This result supports the clinical consensus that patients with limited dorsiflexion due to tight Achilles tendon tend to have foot discomfort or pain caused by plantar pressure, which is also evidenced by a previous study reporting the effect of calf-stretching exercises.29) The correlation between medial-lateral balance (varus/ valgus index) and anterior-posterior balance (forefoot/ heel index) of the pressure-time integral is considered to be a function of the subtalar joint. Subtalar joint motion is a complex combination of three-dimensional movement, comprising plantar flexion, adduction, and inversion in one direction and dorsiflexion, abduction, and eversion in the opposite direction. We believe that this complex motion modulates the balance between medial-lateral and anterior-posterior direction. However, to the best of our knowledge, no study to date has investigated plantar pressure measurement with a multi-segment foot kinematic model. The multi-segment foot model must be integrated to clarify this correlation between medial-lateral and anterior-posterior balance and the role of the subtalar joint.
Before discussing the study results in detail, some limitations need to be addressed. First, the subject number was somewhat small, and the study results should be generalized with caution. Second, the pedobarographic measurement was conducted during treadmill walking. Some researchers have criticized treadmill walking as potentially different from ground walking, which could cause bias in evaluating kinematic and kinetic data during gait.30) Third, combined ankle and subtalar motion was evaluated as an ankle kinematics in this study. Separate evaluation of subtalar joint motion might have been more effective in investigating medial-lateral balance and adaptation, which could possibly have an effect on the varus/valgus index of foot pressure.
In conclusion, male and female young healthy adults showed different pedobarographic findings in this study. This result could provide useful information in setting appropriate treatment goals and obtaining appropriate control data.
ACKNOWLEDGEMENTS
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2017R1D1A1B03033913), Republic of Korea.
This study was presented as a poster in 2015 annual meeting of the Korean Orthopedic Association, Seoul, Korea.
Footnotes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
References
- 1.Barn R, Waaijman R, Nollet F, Woodburn J, Bus SA. Predictors of barefoot plantar pressure during walking in patients with diabetes, peripheral neuropathy and a history of ulceration. PLoS One. 2015;10(2):e0117443. doi: 10.1371/journal.pone.0117443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chiu MC, Wu HC, Chang LY. Gait speed and gender effects on center of pressure progression during normal walking. Gait Posture. 2013;37(1):43–48. doi: 10.1016/j.gaitpost.2012.05.030. [DOI] [PubMed] [Google Scholar]
- 3.Duffin AC, Kidd R, Chan A, Donaghue KC. High plantar pressure and callus in diabetic adolescents: incidence and treatment. J Am Podiatr Med Assoc. 2003;93(3):214–220. doi: 10.7547/87507315-93-3-214. [DOI] [PubMed] [Google Scholar]
- 4.Pataky Z, Golay A, Faravel L, et al. The impact of callosities on the magnitude and duration of plantar pressure in patients with diabetes mellitus: a callus may cause 18,600 kilograms of excess plantar pressure per day. Diabetes Metab. 2002;28(5):356–361. [PubMed] [Google Scholar]
- 5.Pauk J, Daunoraviciene K, Ihnatouski M, Griskevicius J, Raso JV. Analysis of the plantar pressure distribution in children with foot deformities. Acta Bioeng Biomech. 2010;12(1):29–34. [PubMed] [Google Scholar]
- 6.Salazar-Torres JJ, McDowell BC, Humphreys LD, Duffy CM. Plantar pressures in children with congenital talipes equino varus: a comparison between surgical management and the Ponseti technique. Gait Posture. 2014;39(1):321–327. doi: 10.1016/j.gaitpost.2013.07.119. [DOI] [PubMed] [Google Scholar]
- 7.Sullivan J, Burns J, Adams R, Pappas E, Crosbie J. Plantar heel pain and foot loading during normal walking. Gait Posture. 2015;41(2):688–693. doi: 10.1016/j.gaitpost.2015.01.025. [DOI] [PubMed] [Google Scholar]
- 8.Aliberti S, Costa MS, Passaro AC, Arnone AC, Sacco IC. Medial contact and smaller plantar loads characterize individuals with Patellofemoral Pain Syndrome during stair descent. Phys Ther Sport. 2010;11(1):30–34. doi: 10.1016/j.ptsp.2009.11.001. [DOI] [PubMed] [Google Scholar]
- 9.Nahas MR, Gawish HM, Tarshoby MM, State OI, Aboelyazid A. Effect of simulated leg length discrepancy on plantar pressure distribution in diabetic patients with neuropathic foot ulceration. J Wound Care. 2011;20(10):473–477. doi: 10.12968/jowc.2011.20.10.473. [DOI] [PubMed] [Google Scholar]
- 10.Peyer KE, Brassey CA, Rose KA, Sellers WI. Locomotion pattern and foot pressure adjustments during gentle turns in healthy subjects. J Biomech. 2017;60:65–71. doi: 10.1016/j.jbiomech.2017.06.025. [DOI] [PubMed] [Google Scholar]
- 11.Giancoli DC. Physics: principles with applications. 6th ed. Pearson: Upper Saddle River, NJ; 2004. p. 276. [Google Scholar]
- 12.Kanatli U, Yetkin H, Simsek A, Besli K, Ozturk A. The relationship of the heel pad compressibility and plantar pressure distribution. Foot Ankle Int. 2001;22(8):662–665. doi: 10.1177/107110070102200808. [DOI] [PubMed] [Google Scholar]
- 13.Monteiro M, Gabriel R, Aranha J, Neves e Castro M, Sousa M, Moreira M. Influence of obesity and sarcopenic obesity on plantar pressure of postmenopausal women. Clin Biomech (Bristol, Avon) 2010;25(5):461–467. doi: 10.1016/j.clinbiomech.2010.01.017. [DOI] [PubMed] [Google Scholar]
- 14.Sacco IC, Hamamoto AN, Tonicelli LM, Watari R, Ortega NR, Sartor CD. Abnormalities of plantar pressure distribution in early, intermediate, and late stages of diabetic neuropathy. Gait Posture. 2014;40(4):570–574. doi: 10.1016/j.gaitpost.2014.06.018. [DOI] [PubMed] [Google Scholar]
- 15.Wearing SC, Smeathers JE, Yates B, Urry SR, Dubois P. Bulk compressive properties of the heel fat pad during walking: a pilot investigation in plantar heel pain. Clin Biomech (Bristol, Avon) 2009;24(4):397–402. doi: 10.1016/j.clinbiomech.2009.01.002. [DOI] [PubMed] [Google Scholar]
- 16.Burns J, Crosbie J, Hunt A, Ouvrier R. The effect of pes cavus on foot pain and plantar pressure. Clin Biomech (Bristol, Avon) 2005;20(9):877–882. doi: 10.1016/j.clinbiomech.2005.03.006. [DOI] [PubMed] [Google Scholar]
- 17.Lee KM, Chung CY, Park MS, Lee SH, Cho JH, Choi IH. Reliability and validity of radiographic measurements in hindfoot varus and valgus. J Bone Joint Surg Am. 2010;92(13):2319–2327. doi: 10.2106/JBJS.I.01150. [DOI] [PubMed] [Google Scholar]
- 18.Riad J, Coleman S, Henley J, Miller F. Reliability of pediobarographs for paediatric foot deformity. J Child Orthop. 2007;1(5):307–312. doi: 10.1007/s11832-007-0053-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kandil OD, Aboelazm SN, Mabrouk MS. Foot biometrics: gender differences in plantar pressure distribution in standing position. Am J Biomed Eng. 2014;4(1):1–9. [Google Scholar]
- 20.Wunderlich RE, Cavanagh PR. Gender differences in adult foot shape: implications for shoe design. Med Sci Sports Exerc. 2001;33(4):605–611. doi: 10.1097/00005768-200104000-00015. [DOI] [PubMed] [Google Scholar]
- 21.Murphy DF, Beynnon BD, Michelson JD, Vacek PM. Efficacy of plantar loading parameters during gait in terms of reliability, variability, effect of gender and relationship between contact area and plantar pressure. Foot Ankle Int. 2005;26(2):171–179. doi: 10.1177/107110070502600210. [DOI] [PubMed] [Google Scholar]
- 22.Putti AB, Arnold GP, Abboud RJ. Foot pressure differences in men and women. Foot Ankle Surg. 2010;16(1):21–24. doi: 10.1016/j.fas.2009.03.005. [DOI] [PubMed] [Google Scholar]
- 23.Putti AB, Arnold GP, Abboud RJ. Differences in foot pressures between Caucasians and Indians. Foot Ankle Surg. 2010;16(4):195–198. doi: 10.1016/j.fas.2009.11.004. [DOI] [PubMed] [Google Scholar]
- 24.Fourchet F, Kelly L, Horobeanu C, Loepelt H, Taiar R, Millet G. High-intensity running and plantar-flexor fatigability and plantar-pressure distribution in adolescent runners. J Athl Train. 2015;50(2):117–125. doi: 10.4085/1062-6050-49.3.90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.McCormick CJ, Bonanno DR, Landorf KB. The effect of customised and sham foot orthoses on plantar pressures. J Foot Ankle Res. 2013;6:19. doi: 10.1186/1757-1146-6-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Melvin JM, Preece S, Nester CJ, Howard D. An investigation into plantar pressure measurement protocols for footwear research. Gait Posture. 2014;40(4):682–687. doi: 10.1016/j.gaitpost.2014.07.026. [DOI] [PubMed] [Google Scholar]
- 27.Pataky TC. Correlation between maximum in-shoe plantar pressures and clubhead speed in amateur golfers. J Sports Sci. 2015;33(2):192–197. doi: 10.1080/02640414.2014.932917. [DOI] [PubMed] [Google Scholar]
- 28.Xiong S, Goonetilleke RS, Jiang Z. Pressure thresholds of the human foot: measurement reliability and effects of stimulus characteristics. Ergonomics. 2011;54(3):282–293. doi: 10.1080/00140139.2011.552736. [DOI] [PubMed] [Google Scholar]
- 29.Macklin K, Healy A, Chockalingam N. The effect of calf muscle stretching exercises on ankle joint dorsiflexion and dynamic foot pressures, force and related temporal parameters. Foot (Edinb) 2012;22(1):10–17. doi: 10.1016/j.foot.2011.09.001. [DOI] [PubMed] [Google Scholar]
- 30.Garcia-Perez JA, Perez-Soriano P, Llana S, Martinez-Nova A, Sanchez-Zuriaga D. Effect of overground vs treadmill running on plantar pressure: influence of fatigue. Gait Posture. 2013;38(4):929–933. doi: 10.1016/j.gaitpost.2013.04.026. [DOI] [PubMed] [Google Scholar]