

Abstract
Objectives:
Lingual tonsilloliths are not as well-known to radiologists than palatine tonsilloliths, although they might be common in clinical practice. The aim of this investigation was to clarify the prevalence and imaging characteristics of lingual tonsilloliths using panoramic radiographs and CT images.
Methods:
This study included 2244 patients without pathology at the base of tongue who had undergone panoramic radiography and CT of the maxillofacial region. The size, number and position of lingual tonsilloliths relative to the mandible and tongue were evaluated.
Results:
Lingual tonsilloliths were observed in 33 (1.5%) and 108 (4.8%) of all patients on panoramic radiographs and CT images, respectively. The prevalence was higher in patients aged ≥40 years than in those aged < 40 years (χ2, p < 0.01). They appeared as small, round- or rod-shaped calcified bodies, and they always located closely anterior (1–17 mm) to the anterior border of oropharyngeal airway on panoramic radiographs. Lingual tonsilloliths were superimposed over the surrounding soft tissue inferior to the body of the mandible, posteroinferior to the angle of the mandible and posterior to the mandible in 16 (48.5%), 15 (45.5%) and 1 (3.0%) individual, respectively. A significant correlation was observed between the detectability on panoramic radiographs and size (Spearman’s r = 0.961, p < 0.01) of tonsilloliths, as revealed by CT images.
Conclusion:
Lingual tonsilloliths commonly appear on CT. They also appear on panoramic radiography and may superimpose the surrounding soft tissue of the mandible. Although lingual tonsilloliths may resemble other pathological calcifications including submandibular sialoliths and lingual osseous cholistoma, they can be differentiated by carefully observing panoramic radiographs. When clinicians detect calcified bodies near the base of tongue, lingual tonsilloliths should be included in the differential diagnoses.
Keywords: panoramic radiography, X ray computed tomography, tonsil, tongue, calculi
Introduction
Tonsilloliths are concretions within enlarged tonsillar crypts. Most tonsilloliths are asymptomatic and no treatment is required.1 However, recent studies suggest that tonsilloliths are clinically related to halitosis, throat irritation, dysphagia and foreign body sensation upon swallowing.2,3 Tonsilloliths might also cause glossopharyngeal neuralgia or orofacial pain,4 upper airway obstruction,5 and sleep disordered breathing.6 Furthermore, large tonsilloliths may cause life-threatening conditions including dyspnea, esophageal perforation and mediastinitis.7
Waldeyer’s tonsillar ring is composed of palatine, lingual, pharyngeal and Eustachian tube tonsils. Previous investigations revealed palatine tonsilloliths are commonly detected on CT and/or panoramic radiography (PR) at an incidence of 16–46.1% on CT and 7.3–13.4% on PR.8–13 On panoramic radiographs, palatine tonsilloliths may appear as multiple, poorly defined small radiopaque masses. Previous groups also showed the clinical importance of differentiating palatine tonsilloliths from pathological calcifications including submandibular sialoliths, phleboliths and calcification of the lymph nodes. Similar to palatine tonsilloliths, lingual tonsilloliths may appear incidentally based on empirical knowledge. However, only two case reports were found concerning lingual tonsilloliths;14,15 thus, the prevalence and characteristics of lingual tonsilloliths on clinical imaging are unknown.
Therefore, in this study, we aimed to clarify the prevalence and imaging characteristics of lingual tonsilloliths on PR and CT.
Methods and materials
This study was designed as a retrospective review and approved by the Ethics Committee of Tokushima University Hospital, Japan (No. 1580) for analysis of medical records and imaging data. Medical records and images were collected from 2244 consecutive patients with maxillofacial diseases and without tonsillar pathology who had both PR and CT taken between 2004 and 2012.
Panoramic radiographs were obtained using Veraviewepocs (Morita, Osaka, Japan) with standard locus and image processing. CT images were obtained using Aquilion (Toshiba, Tokyo, Japan) with 16-row multidetectors. The scan parameters were as follows: tube voltage was fixed at 140 kVp, both scan thickness and reconstruction thickness were 1 mm and the scanning plane was parallel to the occlusal plane and/or inferior border of the mandible. Images were obtained using both standard soft tissue and bone algorithms. All images were observed on display monitors used for medical purposes.
Prior to the cumulative study, interobserver agreement was calculated by κ statistics. We randomly selected 200 panoramic radiographs and CT images of 200 patients. Two radiologists (AT and CS) independently evaluated the presence of lingual tonsilloliths on those images. The interobserver κ was 0.86 (almost perfect) for panoramic radiographs and 1.00 (perfect) for CT images, respectively. This result tells that the interobserver difference might be negligible in detecting lingual tonsilloliths. Therefore, the complete evaluation for 2244 patients was performed by a single radiologist (AT). The presence of lingual tonsilloliths on panoramic radiographs was evaluated as follows. The locations of tonsilloliths were classified into two categories and three regions (Figure 1). Category 1 was defined as calcifications that were superimposed over the mandible. Category 2 was defined as calcifications that were superimposed over the soft tissue surrounding the mandible. Category 2 was divided into three regions as follows: inferior to the body of the mandible (region 1), posteroinferior to the angle of the mandible (region 2) and posterior to the ramus of the mandible (region 3). Then, the size of lingual tonsilloliths on panoramic radiographs were evaluated. To evaluate the location of lingual tonsilloliths relative to the tongue, the soft tissue shadow that coincides with the anterior border of the oropharyngeal airway on panoramic radiograph was defined as the posterior edge of the base of tongue. The distance between the center of lingual tonsilloliths and the posterior edge of the base of tongue was measured (Figure 2). We selected the largest tonsil as the representative one in patients with multiple tonsilloliths. In the measurement on panoramic radiographs, we calculated based on the pixel size, which was 96 × 96 µm on DICOM format. As the lingual tonsilloliths were located apart from the focal trough, we could not apply the magnification factor of this apparatus, which was 1.3 on the focal trough. Therefore, we did not correct the dimensions on panoramic radiographs.
Figure 1.
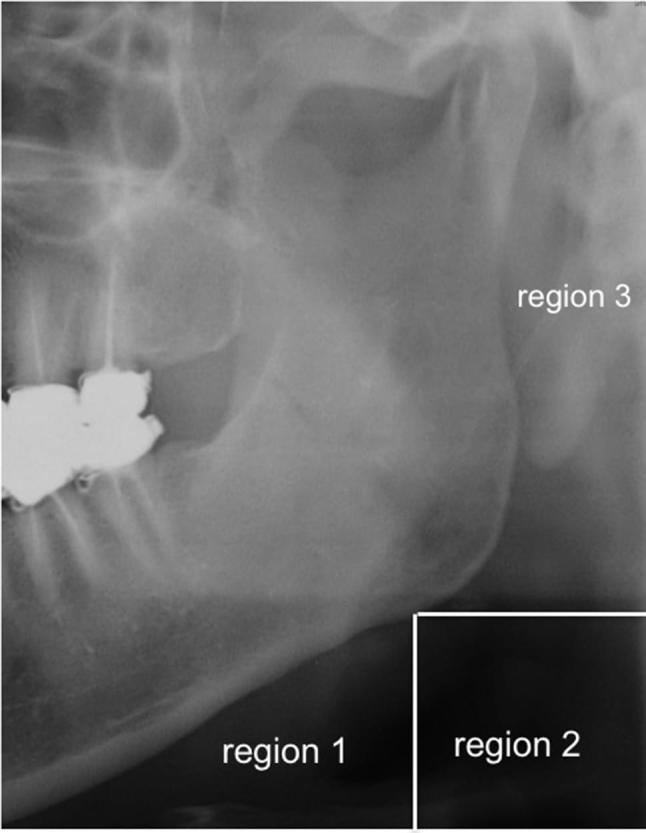
Locations of lingual tonsilloliths that were superimposed over the soft tissue surrounding the mandible on panoramic radiographs. Region 1: inferior to the body of the mandible; Region 2: posteroinferior to the angle of the mandible; Region 3: posterior to the ramus of the mandible.
Figure 2.

Posterior edge of the base of tongue (soft tissue shadow that coincides with the anterior border of oropharyngeal airway; arrows), lingual tonsillolith (arrowhead) and distance from the base of tongue to center of lingual tonsillolith (double-headed arrow) on panoramic radiographs.
Using CT images, the number and diameter of lingual tonsilloliths were also evaluated. Panoramic radiographs and CT images were observed separately at least 2 weeks apart, and the findings of PR not obtained during CT observation. After CT evaluation, panoramic radiographs were then re-evaluated to determine whether the calcifications matched those on CT images. If the calcifications on PR were proven to be other than lingual tonsilloliths on CT, then they were excluded from the study. 42 enostoses (dense bone islands), 36 submandibular sialoliths, 19 remarkable atherosclerotic calcifications, 4 calcified lymph nodes, 3 remnants of contrast media within parotid glands and 1 osteoma cutis were excluded as pathological conditions. 11 calcified stylohyoid ligaments and three partial calcifications of thyroid cartilages were also excluded as physiological conditions.
Commercially available software (SPSS v. 23.0.0; IBM Corp., Armonk, NY) was used for data evaluation. Categorical values were compared using the chi-square test, and relationships between categorical values were assessed using Spearman’s rank correlation coefficient. The results were considered significant at p < 0.05.
Results
Lingual tonsilloliths were found in 108 (4.8%) of 2244 individuals on CT images (Table 1). These patients included 55 males and 53 females. On panoramic radiographs, lingual tonsilloliths were found in 33 (1.5%) of 2244 individuals. These patients included 21 males and 12 females; no sex differences were observed. Panoramic radiographs showed 30.6% of lingual tonsilloliths detected via CT images. The prevalence was higher in older patients than younger patients on both panoramic radiographs and CT images (Table 2). The prevalence of lingual tonsilloliths in patients aged 40–49 years was significantly higher than those aged 30–39 years on CT (p < 0.01). The prevalence was also higher in patients aged ≥40 years than in those aged <40 years (p < 0.01).
Table 1.
Sex differences in the detection rate of lingual tonsilloliths on PR and CT
| Sex | Total | PR | CT | Detection rate of PR | ||
| Presence (%) | Presence (%) | |||||
| Male | 1060 | 21 | (1.9) | 55 | (5.2) | 38.2% |
| Female | 1184 | 12 | (1.0) | 53 | (4.5) | 22.6% |
| Total | 2244 | 33 | (1.5) | 108 | (4.8) | 30.6% |
PR, panoramic radiography.
Table 2.
Prevalence of lingual tonsilloliths by age group
| Age | Total | PR | CT | ||
| (Years) | Presence (%) | Presence (%) | |||
| <9 | 25 | 0 | (0.0) | 0 | (0.0) |
| 10–19 | 182 | 0 | (0.0) | 1 | (0.5) |
| 20–29 | 210 | 1 | (0.5) | 1 | (0.5) |
| 30–39 | 229 | 0 | (0.0) | 1 | (0.4)a |
| 40–49 | 257 | 2 | (0.8) | 14 | (5.4) |
| 50–59 | 433 | 6 | (1.4) | 26 | (6.0) |
| 60–69 | 446 | 15 | (3.4) | 37 | (8.3) |
| 70–79 | 322 | 6 | (1.9) | 22 | (6.8) |
| 80–89 | 126 | 3 | (2.4) | 6 | (4.8) |
| >90 | 14 | 0 | (0.0) | 0 | (0.0) |
| Total | 2244 | 33 | (1.5) | 108 | (4.8) |
PR, panoramic radiography.
The prevalence of lingual tonsilloliths in patients aged 40–49 years was significantly higher than in those aged 30–39 years on CT (p < 0.01). The prevalence was also higher in patients aged ≥40 years than in those aged <40 years (p < 0.01).
On panoramic radiographs, lingual tonsilloliths were predominantly superimposed over the soft tissue surrounding the mandible (category 2) (Table 3). They were located in region 1 (inferior to the body of the mandible) in 16 individuals (48.5%) (representative images, Figure 3a–c), region 2 (posteroinferior to the angle of the mandible) in 15 individuals (45.5%) (representative images, Figure 3d–f) and region 3 (posterior to the ramus of the mandible) in 1 individual (3.0%) (representative images, Figure 3g–i). Lingual tonsilloliths were also superimposed over the mandible (category 1) in one individual (3.0%) (representative images, Figure 3j–l).
Table 3.
Location and prevalence of lingual tonsilloliths on PR
| Location | Number of patients (%) | |
| Category 1: ramus of mandible | 1 | (3.0) |
| Category 2: soft tissue | ||
| Region 1: inferior to the body of the mandible | 16 | (48.5) |
| Region 2: posteroinferior to the angle of the mandible | 15 | (45.5) |
| Region 3: posterior to the ramus of the mandible | 1 | (3.0) |
Figure 3.

Panoramic radiographs (a, d, g, j), axial CT images (b, e, h, k) and sagittal reconstructed CT images (c, f, i, l) of lingual tonsilloliths. (a-c) Representative images of a lingual tonsillolith (arrowhead) inferior to the body of the mandible (region 1). (d–f) Representative images of a lingual tonsillolith (arrowhead) posteroinferior to the angle of the mandible (region 2). (g-i) Representative images of a lingual tonsillolith (arrowhead) posterior to the ramus of the mandible (region 3). (j-l) Representative images of a lingual tonsillolith (arrowhead) near the base of the mandible (category 1).
The sizes of lingual tonsilloliths ranged from 1 to 4 mm on CT. The detection rate of PR increased with increasing size (Spearman’s r = 0.961, p < 0.01) (Table 4). On CT, 1–8 tonsilloliths could be observed in a single patient. However, the detection rate of PR was not related to the number of tonsilloliths (Spearman’s r = 0.259, p > 0.05) (Table 5).
Table 4.
Size of lingual tonsilloliths on CT and detectability of PR
| Size on CT (mm) | Number of patients detected by PR | Number of patients detected by CT | Detection rate of PR compared with CT (%) |
| 1 | 10 | 49 | 20.4 |
| 2 | 18 | 46 | 39.1 |
| 3 | 4 | 12 | 33.3 |
| 4 | 1 | 1 | 100.0 |
| Total | 33 | 108 | 30.6 |
PR, panoramic radiography.
A significant correlation was observed between the detectability on panoramic radiographs and size of tonsilloliths (Spearman’s r = 0.961, p < 0.01).
Table 5.
Number of lingual tonsilloliths on CT and detectability of PR
| Number on CT | Number of patients detected by PR | Number of patients detected by CT | Detection rate of PR compared with CT (%) |
| 1 | 20 | 82 | 24.4 |
| 2 | 10 | 17 | 58.8 |
| 3 | 2 | 4 | 50.0 |
| 4 | 0 | 2 | 0.0 |
| 5 | 0 | 2 | 0.0 |
| 6 | 0 | 0 | N/A |
| 7 | 0 | 0 | N/A |
| 8 | 1 | 1 | 100.0 |
| Total | 33 | 108 | 30.6 |
N/A, not applicable; PR, panoramic radiography. No significant correlation was observed between the detection rate on panoramic radiographs and the number of tonsilloliths (Spearman’s r = 0.259, p > 0.05).
The size of lingual tonsilloliths on panoramic radiographs ranged from 1 to 6 mm. In detail, 21 tonsilloliths (63.6%) were < 3 mm and 12 tonsilloliths (36.4%) were ≥ 3 mm (Table 6). Tonsilloliths < 3 mm were round-shaped, whereas tonsilloliths > 3 mm were generally rod-shaped. The distance between lingual tonsilloliths and the posterior edge of the base of tongue on panoramic radiographs ranged from 1 to 17 mm (Table 7). This distance was < 6 mm in 24 tonsilloliths (72.7%), 6–10 mm in six tonsilloliths (18.2%) and ≥ 10 mm in three tonsilloliths (9.1%). All tonsilloliths were located anterior to the base of tongue (Figure 4). Representative images of a lingual tonsillolith located mostly apart from the base of tongue are shown in Figure 4a–c. The tonsillolith was located 17 mm anteriorly from the edge of the base of tongue on panoramic radiographs. Representative images of a lingual tonsillolith located near the surface of the base of tongue are shown in Figure 4d–f.
Table 6.
Size of lingual tonsilloliths on PR
| Size on PR (mm) | Number of patients detected by PR (%) | |
| 1 | 8 | (24.2) |
| 2 | 13 | (39.4) |
| 3 | 6 | (18.2) |
| 4 | 2 | (6.1) |
| 5 | 3 | (9.1) |
| 6 | 1 | (3.0) |
| Total | 33 | (100.0) |
PR, panoramic radiography.
Table 7.
Distance between lingual tonsilloliths and the posterior edge of the base of tongue on PR
| Distance on PR (mm) | Number of patients detected by PR (%) | |
| 1 | 4 | (12.1) |
| 2 | 9 | (27.3) |
| 3 | 3 | (9.1) |
| 4 | 3 | (9.1) |
| 5 | 5 | (15.2) |
| 6–10 | 6 | (18.2) |
| > 10 | 3 | (9.1) |
| Total | 33 | (100.0) |
PR, panoramic radiography.
Figure 4.

Location of lingual tonsilloliths relative to the soft tissue shadow of the base of tongue. Panoramic radiographs (a, d), axial CT images (b, e) and sagittal reconstructed CT images (c, f) of lingual tonsilloliths. Lingual tonsillolith (arrowheads) and soft tissue shadow of the base of tongue (arrows). (a–c) Representative images of a lingual tonsillolith located mostly apart from the base of tongue. The tonsillolith was located 17 mm anteriorly from the edge of the base of tongue on panoramic radiographs. (d–f) Representative images of a lingual tonsillolith located near the surface of the base of tongue.
Discussion
In the present study, PR detected lingual tonsilloliths in 1.5% of the study population, with a detection rate of 30.6% compared with CT findings. The size of lingual tonsilloliths significantly influenced detectability. Most lingual tonsilloliths were superimposed over the surrounding soft tissue of the mandible and located near the soft tissue shadow of the base of tongue on panoramic radiographs. To our knowledge, this is the first study to demonstrate the prevalence and imaging characteristics of lingual tonsilloliths both by PR and CT.
Tonsilloliths can be caused by chronic tonsillitis with infectious agents such as fungi, bacteria and Actinomyces combining with pus cells to serve as an ideal location for stone formation.16 Among them, palatine tonsilloliths are commonly encountered in clinical practice. Previous reports showed that palatine tonsilloliths were one of the most common findings among pathological and physiological calcifications in the head and neck region, with rates ranging from 16 to 46.1%.8–12 However, there are few reports regarding lingual tonsilloliths. To our knowledge, no reports are available in the English literature, and only two case reports have been published in the Japanese literature.14,15 In these reports, the main clinical symptom was discomfort or anterior neck pain. A foreign body such as fishbone was initially suspected by otolaryngologists in both cases because the symptoms appeared just after consuming food, and small calcified bodies were observed on CT. Furthermore, the prevalence of lingual tonsilloliths has not yet been reported. In this study, PR detected lingual tonsilloliths in 1.5% of the study population. Lingual tonsilloliths were confirmed to be more commonly observed when compared to diseases that require medical treatment including sialoliths or phleboliths. Therefore, clinicians should be aware of the high prevalence of lingual tonsilloliths and its imaging characteristics during PR observation. When abnormal calcifications are detected incidentally by PR, clinicians should diagnose the condition correctly as early as possible to minimize unnecessary diagnostic imaging.
In the present study, the lingual tonsillolith detection rate of PR was 30.6% via CT. In our previous study, the palatine tonsillolith detection rate in the same cohort was similar (32.8%).13 Compared with palatine tonsilloliths, lingual tonsilloliths are generally smaller in size, fewer in number and located medially and away from the focal trough of the panoramic apparatus. Therefore, we hypothesized that the detection rate for lingual tonsilloliths by PR would be lower than that of palatine tonsilloliths. A potential explanation for the discrepancy might be as follows: because palatine tonsilloliths are frequently detected superimposed over the mandible on panoramic radiographs,13 small or faint tonsilloliths may be obscured. Additionally, the lingual tonsillolith detection rate was significantly higher in participants aged > 40 years in the present study. This same tendency was observed in our previous study concerning palatine tonsilloliths.13 Although the reason is unclear, it is possible that chronic oropharyngeal inflammation persists in older patients because of higher smoking rates and/or poor oral hygiene.17,18
On panoramic radiographs, lingual tonsilloliths were most frequently superimposed over the soft tissue surrounding the mandible (category 2), primarily located inferior to the mandible (48.5% in region 1) and posteroinferior to the mandible (45.5% in region 2). As these are also frequent sites for submandibular sialoliths, clinicians must be aware of the imaging characteristics of lingual tonsilloliths on panoramic radiographs to differentiate them from sialoliths. In particular, lingual tonsilloliths were located near the posterior edge of the base of tongue on panoramic radiographs, at a distance 1–17 mm anteriorly. On panoramic radiographs, the position of the posterior edge of the base of tongue relative to the mandible may change if the positioning or swallowing phase differs at imaging. Hence, the location of calcifications relative to the base of tongue might be more important in the differential diagnosis. Furthermore, lingual tonsilloliths ranged from 1 to 4 mm, which is generally smaller than sialoliths. Large lingual tonsilloliths were generally rod-shaped on panoramic radiographs, although most were round-shaped on CT images. We speculate that some of the large, rod-shaped lingual tonsilloliths may be horizontally distorted because they are at a distance from the focal trough of PR. Therefore, the imaging characteristics of lingual tonsilloliths are small, round- or rod-shaped calcified bodies located near the base of tongue on panoramic radiographs. These findings might provide helpful clues in the differential diagnosis of lingual tonsilloliths.
In the differential diagnosis of the lingual tonsilloliths, lingual osseous cholistoma, which was also known as lingual osteoma, should be considered. This lesion has been reported in less than 100 cases. Compared to the lingual tonsilloliths, lingual osseous cholistoma had a female prediction, and the mean age was 31.4 years. Most of these were located in the dorsum of the tongue and the size ranged from 0.5 to 5.0 cm.19,20 Other conditions, such as calcification of the stylohyoid ligament and thyroid or triticeal cartilage, should also be considered in the differential diagnosis. Moreover, pathological calcifications such as calcification of the lymph nodes, atherosclerotic calcification of the carotid or facial arteries, phleboliths, loose bodies from the vertebrae, cysticercosis, calcified acne, osteoma cutis (miliary osteoma of the skin), myositis ossificans and foreign bodies should be considered.1,8,16,21–24 The imaging characteristics of lingual tonsilloliths presented in this study will aid in the differentiation of these calcified conditions.
Conclusion
Lingual tonsilloliths commonly appeared and were detected with frequencies of 4.8% on CT images and 1.5% on panoramic radiographs. The detection rate of PR was 30.6% via CT. On panoramic radiographs, most lingual tonsilloliths were superimposed over the soft tissue surrounding the mandible. They appeared as small, round- or rod-shaped calcified bodies anterior to the soft tissue shadow of the base of tongue on panoramic radiographs. Clinicians should be aware that lingual tonsilloliths are not uncommon, and lingual tonsilloliths should be included in the differential diagnosis of calcified bodies over the soft tissue surrounding the mandible.
Contributor Information
Akira Takahashi, Email: atakahashi-dent@tokushima-u.ac.jp.
Chieko Sugawara, Email: sugawara@tph.gr.jp.
Keiko Kudoh, Email: kkudoh@tokushima-u.ac.jp.
Yoshiko Yamamura, Email: yamamura.yoshiko@tokushima-u.ac.jp.
Go Ohe, Email: go.ohe@tokushima-u.ac.jp.
Tetsuya Tamatani, Email: ttama@tokushima-u.ac.jp.
Youji Miyamoto, Email: miyamoto@tokushima-u.ac.jp.
References
- 1.de Moura MD, Madureira DF, Noman-Ferreira LC, Abdo EN, de Aguiar EG, Freire AR. Tonsillolith: a report of three clinical cases. Med Oral Patol Oral Cir Bucal 2007; 12: E130–3. [PubMed] [Google Scholar]
- 2.Pruet CW, Duplan DA. Tonsil concretions and tonsilloliths. Otolaryngol Clin North Am 1987; 20: 305–9. [PubMed] [Google Scholar]
- 3.Mandel L. Multiple bilateral tonsilloliths: case report. J Oral Maxillofac Surg 2008; 66: 148–50. doi: 10.1016/j.joms.2006.05.047 [DOI] [PubMed] [Google Scholar]
- 4.Siber S, Hat J, Brakus I, Biočić J, Brajdić D, Zajc I, et al. Tonsillolithiasis and orofacial pain. Gerodontology 2012; 29: e1157–e1160. doi: 10.1111/j.1741-2358.2011.00456.x [DOI] [PubMed] [Google Scholar]
- 5.Lo RH, Chang KP, Chu ST. Upper airway obstruction caused by bilateral giant tonsilloliths. J Chin Med Assoc 2011; 74: 329–31. doi: 10.1016/j.jcma.2011.05.011 [DOI] [PubMed] [Google Scholar]
- 6.Chang YL, Chen PY, Hung SH. Large tonsillolith: possible cause of sleep-disordered breathing. J Formos Med Assoc 2015; 114: 1293–4. doi: 10.1016/j.jfma.2014.11.005 [DOI] [PubMed] [Google Scholar]
- 7.Navas Cuellar JA, Lopez Bernal F, Ibanez Delgado F. Giant tonsillolith causing dyspnea, esophageal perforation, and mediastinitis. Emergencias 2015; 27: 280–80. [PubMed] [Google Scholar]
- 8.Aspestrand F, Kolbenstvedt A. Calcifications of the palatine tonsillary region: CT demonstration. Radiology 1987; 165: 479–80. doi: 10.1148/radiology.165.2.3659369 [DOI] [PubMed] [Google Scholar]
- 9.Fauroux MA, Mas C, Tramini P, Torres JH. Prevalence of palatine tonsilloliths: a retrospective study on 150 consecutive CT examinations. Dentomaxillofac Radiol 2013; 42: 0120429. doi: 10.1259/dmfr.20120429 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Oda M, Kito S, Tanaka T, Nishida I, Awano S, Fujita Y, et al. Prevalence and imaging characteristics of detectable tonsilloliths on 482 pairs of consecutive CT and panoramic radiographs. BMC Oral Health 2013; 13: 54. doi: 10.1186/1472-6831-13-54 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Takahashi A, Sugawara C, Kudoh T, Uchida D, Tamatani T, Nagai H, et al. Prevalence and imaging characteristics of palatine tonsilloliths detected by CT in 2,873 consecutive patients. ScientificWorldJournal 2014; 2014: 1–4. doi: 10.1155/2014/940960 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ergun T, Lakadamyali H. The prevalence and clinical importance of incidental soft-tissue findings in cervical CT scans of trauma population. Dentomaxillofac Radiol 2013; 42: 20130216. doi: 10.1259/dmfr.20130216 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Takahashi A, Sugawara C, Kudoh T, Ohe G, Takamaru N, Tamatani T, et al. Prevalence and imaging characteristics of palatine tonsilloliths evaluated on 2244 pairs of panoramic radiographs and CT images. Clin Oral Investig 2017; 21: 85–91. doi: 10.1007/s00784-016-1752-0 [DOI] [PubMed] [Google Scholar]
- 14.Bando H, Uno T, Nin F, Tei K, Shinomiya T, Hisa Y. A case of calculus of the lingual tonsil. Practica Oto-Rhino-Laryngologica 2003; 96: 619–22. doi: 10.5631/jibirin.96.619 [Google Scholar]
- 15.Sakane S, Ikoma R, Niwa K, Oridate N. A case of lingual tonsil lithiasis suspected as a foreign body. Pract Otorhinolaryngol 2013; 106: 837–41. doi: 10.5631/jibirin.106.837 [Google Scholar]
- 16.Mesolella M, Cimmino M, Di Martino M, et al. Tonsillolith. case report and review of the literature. Acta Otorhinolaryngol Ital 2004; 24: 302–7. [PubMed] [Google Scholar]
- 17.Katanoda K, Saika K, Yamamoto S, Tanaka S, Oshima A, Nakamura M, et al. Projected cancer mortality among Japanese males under different smoking prevalence scenarios: evidence for tobacco control goal setting. Jpn J Clin Oncol 2011; 41: 483–9. doi: 10.1093/jjco/hyq247 [DOI] [PubMed] [Google Scholar]
- 18.Murakami Y, Ueshima H, Okamura T, Kadowaki T, Hozawa A, Kita Y, et al. Life expectancy among Japanese of different smoking status in Japan: NIPPON DATA80. J Epidemiol 2007; 17: 31–7. doi: 10.2188/jea.17.31 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Vered M, Lustig JP, Buchner A. Lingual osteoma: a debatable entity. J Oral Maxillofac Surg 1998; 56: 9–13. doi: 10.1016/S0278-2391(98)90906-5 [DOI] [PubMed] [Google Scholar]
- 20.Stanford JK, Spencer JC, Reed JM. Case presentation and images of a lingual osseous choristoma in a pediatric patient. Am J Otolaryngol 2015; 36: 753–4. doi: 10.1016/j.amjoto.2015.07.008 [DOI] [PubMed] [Google Scholar]
- 21.Almog DM, Tsimidis K, Moss ME, Gottlieb RH, Carter LC, et al. Evaluation of a training program for detection of carotid artery calcifications on panoramic radiographs. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000; 90: 111–7. doi: 10.1067/moe.2000.107056 [DOI] [PubMed] [Google Scholar]
- 22.Katz JO, Langlais RP, Underhill TE, Kimura K, et al. Localization of paraoral soft tissue calcifications: the known object rule. Oral Surg Oral Med Oral Pathol 1989; 67: 459–63. doi: 10.1016/0030-4220(89)90392-7 [DOI] [PubMed] [Google Scholar]
- 23.Sezer B, Tugsel Z, Bilgen C. An unusual tonsillolith. Oral Surg Oral Med Oral Pathol 2003; 95: 471–3. doi: 10.1067/moe.2003.65 [DOI] [PubMed] [Google Scholar]
- 24.Bayer S, Helfgen E-H, Bös C, Kraus D, Enkling N, Mues S, et al. Prevalence of findings compatible with carotid artery calcifications on dental panoramic radiographs. Clin Oral Investig 2011; 15: 563–9. doi: 10.1007/s00784-010-0418-6 [DOI] [PubMed] [Google Scholar]