

Abstract
Objectives:
To investigate voids in different root canal sealers using micro-CT and nano-CT, and to explore the feasibility of using nano-CT for quantitative analysis of sealer filling quality.
Methods:
30 extracted mandibular central incisors were randomly assigned into three groups according to the applied root canal sealers (Total BC Sealer, Sure Seal Root, AH Plus) by the single cone technique. Subsequently, micro-CT and nano-CT were performed to analyse the incidence rate of voids, void fraction, void volume and their distribution in each sample.
Results:
Micro-CT evaluation showed no significant difference among sealers for the incidence rate of voids or void fraction in the whole filling materials (p > 0.05), whereas a significant difference was found between AH Plus and the other two sealers using nano-CT (p < 0.05). All three sealers presented less void volume in the apical third; however, higher void volumes were observed in the apical and coronal thirds in AH Plus using micro-CT (p < 0.05), while nano-CT results displayed higher void volume in AH Plus among all the sealers and regions (p < 0.05).
Conclusions:
Bioactive sealers showed higher root filling rate, lower incidence rate of voids, void fraction and void volume than AH Plus under nano-CT analysis, when round root canals were treated by the single cone technique. The disparate results suggest that the higher resolution of nano-CT have a greater ability of distinguishing internal porosity, and therefore suggesting the potential use of nano-CT in quantitative analysis of filling quality of sealers.
Keywords: MicroCT, nanostructures, root canal filling materials, dental seal, endotonic obturation
Introduction
Complete and adequate filling of root canals is one of the main challenges of the endodontic treatment to ensure long-term successful prognosis.1 Gutta-percha is a most frequently used root canal core material, which exhibits the necessary properties for root canal treatment, namely, minimal toxicity and ease of insertion. Despite that, a gutta-percha cone cannot fit perfectly alone owing to low adhesiveness to the canal walls and the complexity of root canal systems. This leads to unfavourable microbial leakages in the filled canals.2 To compensate for this, various sealer materials are developed and employed to fill the remaining irregular spaces between the gutta-percha cone and surrounding dentinal wall.3
One well-known sealer is AH Plus, an epoxy-resin-based material with high tissue compatibility, low solubility and a relatively short setting time.4 In view of these characteristics, AH Plus is currently regarded as the clinical reference standard endodontic sealer.5 Calcium silicate-based bioactive sealers, such as Total Fill BC Sealer and Sure Seal Root sealer, are becoming more popular due to their improved mechanical, chemical and cytocompatible properties.6 They are reported to be insoluble, premixed and hydrophilic, which could minimize the risk of void formation in the root canal sealers, and might even benefit from the pre-existing moisture in the root canals during their final setting.7 The existence of voids is of clinical relevance because only 1% shrinkage of sealers can result in voids and gaps that are large enough for penetration of bacteria and their noxious products.8 Nevertheless, the potential filling quality relating to the presence and distribution of voids along the dentin-sealer interface has not yet been clearly identified, especially for these newly developed bioactive sealers.
To evaluate the filling ability of sealers in canal obturation, traditionally, in vitro leakage models are employed for initial screening of new materials and to justify their superiority for clinical applications, although these models have limited clinical relevance.3 With the wide use of micro-CT, it has been possible to provide high-resolution 3-dimensional (3D) evaluation of the internal structure of root canals and even to characterize the presence of void volume in different root canal fillings and techniques.9–11 Recently, nanometer-scale X-ray CT (nano-CT) that produces ultra-precise radiographs using a high power nanofocus X-ray source with focal spot of only a few microns, can compete with many absorption contrast setups at synchrotron radiation facilities.12 Nano-CT imaging is believed to open new avenues toward precise characterization and quantification of tissue microarchitectures that were previously unreachable.13 However, this emerging powerful imaging modality has so far not been used to reveal the complex internal structures (i.e., voids and gaps) of the endodontic sealers.
The aim of the present study was(1) to quantitatively assess voids in representative root canal sealer models (Total Fill BC Sealer and Sure Seal Root), in comparison to a clinical reference standard AH Plus sealer using high-resolution non-destructive 3D imaging, and (2) to explore the feasibility of using nano-CT for quantitative analysis of filling quality of root canal sealers.
Methods and materials
The tests were performed on 30 freshly extracted human mandibular central incisors, which had been extracted for periodontal reasons. All the collected teeth were allowed to use in the lab research, after the verbal inform consent from the clinic. As indicated by a previous study,9 the highest possible difference for the quantitatively analyses of voids volume was 1.8 mm3. Hence, the minimum sample size required for this difference is 10 per group, according to the method described by Chan,14 based on p = 0.05 and80% power. The age and sex of sample donors were unknown. The inclusion criteria were the single-root, straight and round shape of the root without root caries, fractures or resorptions, which were confirmed by a pre-operative radiograph. All samples were cleaned and disinfected with 5.25% of sodium hypochlorite (NaClO) for 2 h. Next, they were stored in distilled water at room temperature for 1 month before root canal preparation.
Root canal preparation
All teeth crowns were removed to make a standardized root length of 12 mm. The coronal parts of roots were examined with an operation microscope (OPMI pico; Zeiss Co., Jena, Germany) and selected only if the canal shape was round for the standardized operation. An ISO size #10 K-File (Maillefer, Ballaiges, Switzerland) was inserted into the root canal until the tip was just visible beyond the apex. Working length was determined by subtracting 0.5 mm from this length. The canals were prepared using a crown-down technique with EndoSequence rotary nickel titanium files (Brasseler, Savannah, GA). The finishing file was ISO size 40/0.06. During the instrumentation, root canals were irrigated with 2 ml of 5.25% NaClO. Next, the smear layer was removed using 17% of EDTA for 1 min. The final rinse was performed with 3 ml of 5.25% NaClO and 3 ml of distilled water. Then root canals were dried using paper points. Root canal sealers were prepared in accordance with the manufacturer's recommendations and then obturated with single cone technique by the same professional expert with more than 10-year clinical experience in endodontics (BC), who was kept blinded with another observer for the later imaging analyses but not for the obturation operation. The roots were divided randomly into three groups (each 10 roots). Group I was filled with AH Plus sealer (Dentsply DeTrey, Konstanz, Germany) and 40/0.06 gutta-percha (Maillefer, Ballaiges, Switzerland); Group II was filled with Total Fill BC sealer (FKG Dentaire SA, Switzerland) and 40/0.06 Total Fill BC points (FKG Dentaire SA, Switzerland); Group III was filled with Sure Seal Root sealer and 40/0.06 gutta-percha (Maillefer, Ballaiges, Switzerland). After the filling process, roots were stored at 37°C and in 100% humidity for 10 days. Periapical radiographs of all samples were then taken from two different angulations to ensure the filling quality.
Micro-CT and Nano-CT acquisition
A high-resolution micro-CT device (Bruker Skyscan 1172, Kontich, Belgium) was used to scan the specimens at a voxel size of 13.73µm, 100 kV, 100µA, 360˚ of rotation, 0.5 mm of Al filter, a 0.7 ˚ of rotation step, 250 ms exposure. The total scanning time for the root sample was around 1 h. Beam hardening correction and optimal contrast limits were used in accordance with manufacturer’s instructions and based on the initial scanning and reconstructiontests.
Nano-CT scans were performed with the Phoenix NanoTom S (GE Sensing & Inspection Technologies GmbH, Wunstorf, Germany) using a voxel size of 1.58µm, 115 kV, 80 µA, respectively, 0.1 mm Cu filter, 360˚ of rotation, 500 ms exposure, 9.2 W power and mode 1 for tube operation. The total scanning time for the whole root sample was around 4 h.
Imaging reconstruction and processing
Image reconstruction was performed with NRecon software (ver. 1.6.10.4, Skyscan, Kontich, Belgium) using the modified algorithm described by Feldkamp et al,15 to obtain axial, two-dimensional, 1000 × 1000 pixel images. The reconstruction parameters ring artefact correction and smoothing were fixed at zero. The images were reconstructed to show 2-dimensional slices of the roots. In total, 1023 cross-sectional images were reconstructed from whole volume in micro-CT while 6885 cross-sectional images from nano-CT. After the image reconstruction, CTAn (ver. 1.16.1.0, Skyscan, Aartselaar, Belgium) software was used for the 3D volumetric visualization and analysis of the root canals by both micro-CT and nano-CT scanning.
The presence of voids was assessed in 2D slices in each section on a 21.3-inch flat-panel colour-active matrix TFT medical display (NEC MultiSync MD215MG, Munich, Germany) with a resolution of 2048–2560 at 75 Hz and 0.17 mm dot pitch operated at 11.9 bits. New cross-sectional images were prepared perpendicular to the long axis of the root, starting at the most apical part of the root. The selected sections had an interval of 0.5 mm which resulted 254 average number of cross-sectional images. The same selection procedure was performed for nano-CT images with an interval of 0.02 mm and 596 cross-sectional images. Initially, each sample was divided into three regions, from the apical end to the top of the root at a level of 0–4 mm (apical), 4–8 mm (middle), and 8–12 mm (coronal). For all the micro-CT images (Figure 1) and nano-CT images (Figure 2), two observers (BC and KO) could independently adjust the magnification of sections, who were both blinded to the group allocation to minimize observer bias. In case of disagreement between the observers, the sections were re-examined until a consensus was reached.
Figure 1. Renderings of three different filling materials scanned with micro-CT (voxel size = 13.73 µm) showing the 3D volumes of voids after the root canal treatment. The details of internal (arrowhead), external (arrows), and combined voids (stars) are clearly presented in AH Plus (a), Total Fill BC Sealer (b) and Sure Seal Root (c).
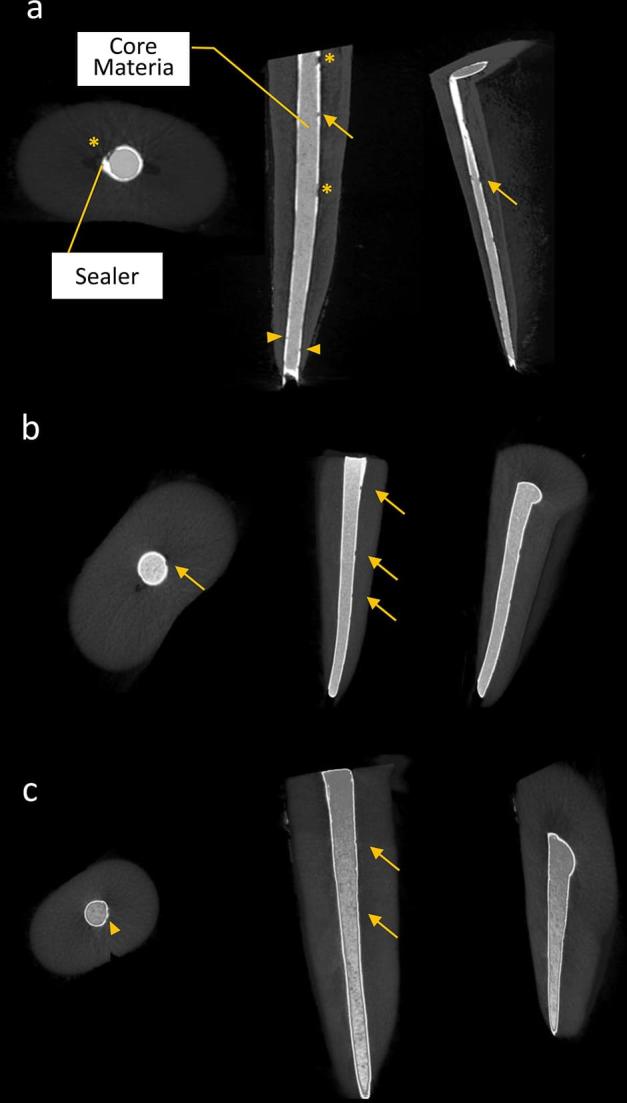
Figure 2. Renderings of three different filling materials scanned with nano-CT images (voxel size = 1.58 µm), which shows improved contrast and details on the 3D volumes of voids after the root canal treatment, in comparison with micro-CT images. The details of internal (arrowhead), external (arrows), and combined voids (stars) are clearly presented in AH Plus (a), Total Fill BC Sealer (b) and Sure Seal Root (c) in the coronal, middle and apical third, respectively.

For calculation of the voids in 3D volumes (Figures 1 and 2), namely, internal voids (inside the sealer), external voids (along the internal root canal wall or the external surface of core materials) and combined voids (a combination of internal and external voids), the original grayscale images were processed with a Gaussian low-pass filter for noise reduction, and then an automatic segmentation threshold was used to subtract dentin from gutta-percha, sealer, and voids using CTAn (ver. 1.16.1.0, Skyscan). A standard thresholding (binarization) process was used for corresponding imaging modality, detailed in a previous study,16 which entailed processing the range of gray levels to obtain a repeatable imposed image of only black and white pixels. Then, separately for each slice, a region of interest was manually selected with a single object to ensure the calculation of the incidence rate of voids, the void fraction (defined as the volume of internal/external/combined voids over the whole filling materials) and the distribution of void volume (Figures 1 and 2).
Statistical analysis
Kruskal–Wallis test was performed and then, in cases where statistically significant p values were found, Mann–Whitney’s U post-hoc tests carried out for the pairwise comparisons. All the analyses were performed with the SPSS software (ver. 20.0; Chicago, IL) assuming a significance level of α = 0.05.
Results
The presence of voids in the whole filling materials (core materials and sealers) was summarized in Tables 1 and 2. Regarding the micro CT results (Table 1), a high incidence rate of voids was found within each sealer material and no significant difference was found among the root filling sealers (p = 0.718). Moreover, there was no significant difference in terms of root filling rate and void fraction (p > 0.05). Additionally, considering the different root thirds (Table 2), a considerable decrease of void volume in the apical third was observed, with significant differences between AH Plus and other two sealers in apical and coronal third of the teeth (p < 0.05). However, no difference in the middle third was observed for all tested sealers (p > 0.05).
Table 1.
An overview of the incidence rate of voids, root filling rate and the void fraction (internal, external and combined) in the whole root canal filling materials in micro-CT images
| Root canal filling materials | n | Mean (%) | SD | Kruskall–Wallis H test | ||
|---|---|---|---|---|---|---|
| p value | Pairwise comparisons | |||||
| Incidence rate of voids | Total BC Sealer (1) | 10 | 62.8 | 34.2 | 0.718 | 1–3 2–3 |
| Sure Seal Root(2) | 10 | 64.2 | 38.5 | |||
| AH Plus(3) | 10 | 68.3 | 38.8 | |||
| Total | 30 | 65.1 | 37.1 | |||
| Root filling rate | Total BC Sealer(1) | 10 | 97.816 | 1.299 | 0.588 | 1–3 2–3 |
| Sure Seal Root(2) | 10 | 98.072 | 1.358 | |||
| AH Plus(3) | 10 | 97.442 | 1.280 | |||
| Total | 30 | 97.776 | 1.312 | |||
| Internal voids | Total BC Sealer(1) | 10 | 0.622 | 0.202 | 0.612 | 1–3 2–3 |
| Sure Seal Root(2) | 10 | 0.611 | 0.192 | |||
| AH Plus(3) | 10 | 0.730 | 0.238 | |||
| Total | 30 | 0.654 | 0.210 | |||
| External voids | Total BC Sealer(1) | 10 | 0.942 | 0.613 | 0.936 | 1–3 2–3 |
| Sure Seal Root(2) | 10 | 0.722 | 0.512 | |||
| AH Plus(3) | 10 | 0.887 | 0.570 | |||
| Total | 30 | 0.850 | 0.565 | |||
| Combined voids | Total BC Sealer(1) | 10 | 0.620 | 0.438 | 0.840 | 1–3 2–3 |
| Sure Seal Root(2) | 10 | 0.592 | 0.382 | |||
| AH Plus(3) | 10 | 0.961 | 0.537 | |||
| Total | 30 | 0.724 | 0.452 |
Table 2.
The void volume of the root canal filling materials in micro-CT images at different root regions (apical, middle and coronal thirds)
| Region | Root canal filling materials | n | Mean(mm3) | SD | p value | Pairwise comparisions |
|---|---|---|---|---|---|---|
| Apical third | Total BC Sealer (1) | 10 | 0.301 | 0.134 | p < 0.05 | 1–3 2–3 |
| Sure Seal Root (2) | 10 | 0.324 | 0.155 | |||
| AH Plus (3) | 10 | 0.498 | 0.216 | |||
| Middle third | Total BC Sealer (1) | 10 | 0.398 | 0.192 | p > 0.05 | 1–3 2–3 |
| Sure Seal Root (2) | 10 | 0.412 | 0.250 | |||
| AH Plus (3) | 3 | 0.425 | 0.275 | |||
| Coronal third | Total BC Sealer (1) | 10 | 0.928 | 0.480 | p < 0.05 | 1–3 2–3 |
| Sure Seal Root (2) | 10 | 0.955 | 0.492 | |||
| AH Plus (3) | 10 | 1.427 | 0.744 | |||
| Overall total | 30 | 0.629 | 0.243 |
Regarding the nano-CT evaluations (Table 3), there was an even higher incidence rate of voids within each sealer material compared to the micro-CT results. Total BC and Sure Seal sealers showed less incidence rate of voids (p < 0.04) and higher root filling rate (p < 0.05) than AH Plus. Significantly higher voids fraction in terms of internal, external and combined voids were found in AH Plus, when compared with Total BC and Sure Seal Root sealers (p < 0.05). Moreover, there was a considerable decrease of void volume in the apical third (Table 4). Additionally, AH Plus was distinguished from the other two sealers, which showed the highest void volumes at all root levels (p < 0.05).
Table 3.
An overview of the incidence rate of voids, root filling rate and the void fraction (internal, external and combined) in the whole root canal filling materials in nano-CT images
| Root canal filling materials | n | Mean (%) | SD | Kruskall–Wallis H Test | ||
|---|---|---|---|---|---|---|
| p value | Pairwise comparisons | |||||
| Incidence rate of voids | Total BC Sealer (1) | 3 | 65.2 | 36.1 | p < 0.04 | 1–3 2–3 |
| Sure Seal Root (2) | 3 | 67.6 | 37.9 | |||
| AH Plus(3) | 3 | 78.3 | 44.2 | |||
| Total | 9 | 70.3 | 39.4 | |||
| Root filling rate | Total BC Sealer (1) | 3 | 98.114 | 1.402 | p < 0.05 | 1–3 2–3 |
| Sure Seal Root (2) | 3 | 98.105 | 1.400 | |||
| AH Plus(3) | 3 | 96.550 | 1.180 | |||
| Total | 9 | 97.589 | 1.327 | |||
| Internal voids | Total BC Sealer (1) | 3 | 0.588 | 0.282 | p < 0.05 | 1–3 2–3 |
| Sure Seal Root (2) | 3 | 0.604 | 0.296 | |||
| AH Plus(3) | 3 | 1.253 | 0.522 | |||
| Total | 9 | 0.815 | 0.366 | |||
| External voids | Total BC Sealer (1) | 3 | 0.840 | 0.590 | p < 0.05 | 1–3 2–3 |
| Sure Seal Root (2) | 3 | 0.820 | 0.580 | |||
| AH Plus(3) | 3 | 1.380 | 0.772 | |||
| Total | 9 | 1.013 | 0.647 | |||
| Combined voids | Total BC Sealer (1) | 3 | 0.458 | 0.132 | p < 0.05 | 1–3 2–3 |
| Sure Seal Root (2) | 3 | 0.471 | 0.180 | |||
| AH Plus(3) | 3 | 0.817 | 0.296 | |||
| Total | 9 | 0.582 | 0.452 |
Table 4.
The void volume of the root canal filling materials in nano-CT images at different root regions (apical, middle and coronal thirds)
| Region | Root canal filling materials | n | Mean(mm3) | SD | p value | Pairwise comparisions |
|---|---|---|---|---|---|---|
| Apical third | Total BC Sealer (1) | 3 | 0.414 | 0.276 | p < 0.05 | 1–3 2–3 |
| Middle third | Total BC Sealer (1) | 3 | 0.480 | 0.290 | p < 0.05 | 1–3 2–3 |
| Sure Seal Root (2) | 3 | 0.481 | 0.290 | |||
| AH Plus (3) | 3 | 0.703 | 0.401 | |||
| Coronal third | Total BC Sealer (1) | 3 | 0.918 | 0.480 | p < 0.05 | 1–3 2–3 |
| Sure Seal Root (2) | 3 | 0.910 | 0.470 | |||
| AH Plus (3) | 3 | 1.602 | 0.922 | |||
| Overall total | 9 | 0.735 | 0.422 |
Discussion
In general, the goals of root canal filling in the endodontic treatment should be(1) to prevent leakage of oral fluids containing bacteria and their products from the oral environment to the apical periodontium through the root canal; and (2) to hinder the exit to the periapex of microorganisms that resisted to root canal disinfection and instrumentation.17 In the current study, micro-CT and nano-CT imaging could discriminate three different kinds of voids in all tested sealers, which may serve as a niche for the remaining and transferred bacteria. Since the bacteria in the internal voids are captive in an inconvenient environment, they may grow and migrate easier to the apical region in external or combined voids and thus lead to apical periodontitis.18
Previous studies evaluated the filling quality using various techniques, such as dye leakage, microbial penetration and histological sections.19,20In vitro measurements of dye penetration were either linear or volumetric, where the dye penetrated around voids or within the root fillings. Histological sections can be performed at the millimeter scale, but a tissue loss corresponding to the abrasive track of the saw would occur during sectioning and therefore less material was left to assess. Microbial penetration seems to be a more biologically relevant outcome, but the technique was limited in revealing only voids extending through the full length of the root filling.21 This study using high-resolution imaging allowed further exploration of 3D precise internal structures of the sealer materials at the nanometer scale in a nondestructive way.
The single cone technique was selected in the study because of its simplicity and because it is less operator-dependent compared to other root filling techniques, and may be better indicated in round-canal teeth prepared to the shape of the instruments used.22 It was suggested that single cone is a frequently used root filling techniques.21 The use of matched-taper gutta-percha points relies on the original canal shape and the ability to create a tapered circular preparation.22 Endodontic sealers differed in physical properties and this might be relevant in determining the sealing ability of sealers. The dimensional stability of AH Plus sealer has been already demonstrated and its application was widely proposed through long-term practice.23,24 Therefore, in this study AH Plus was used as the clinical reference standard and compared to other sealers and similar-sized round root canals were prepared for the standardization.
As demonstrated, all tested sealers had less void volume in the apical third, which was in accordance with another micro-CT study on AH Plus and mineral trioxide aggregate sealers using thermafil obturation technique.16 Celikten et al also reported a significant decrease of void formation in the apical third, where roots were filled with bioceramic sealers, ActiV GP, and AH Plus by single cone technique.25 It could be assumed that greater pressure during the root canal preparation may reduce the presence of voids within the tested sealers in the apical third, regardless of the obturation techniques.
The bioceramic root canal filling materials are generally recommended, due to small particle size (less than 2 µm), excellent level of viscosity,26 minimal or no shrinkage during the setting phase,27 nonetheless, the voids of the sealers in the dentin-sealer interface have not been completely understood. The present micro-CT test at a resolution of 13.73 µm showed that the filling quality of all tested sealers were almost the same for the incidence rate of voids and the void fraction. Similarly, another micro-CT investigation with a resolution of 19.1µm failed to distinguish between two thrermo-plasticized gutta-percha techniques (Thermafil and System B) and a cold gutta-percha technique (single point) in terms of percentage of filling and void distribution in the whole filling materials.28 In contrast, from the nano-CT results, when a voxel-resolution of 1.58 µm was achieved, it was found that an obvious increase of void fraction and void volume in AH Plus, compared with the bioceramic sealers. This was consistent with a previous finding, which reported underestimation of void volume while using lower resolution micro-CT.29 Even although micro-CT is considered as the gold standard for analysis of filling quality,30 the evidence from this study has suggested that there might be a threshold of voxel-resolution for the quantitative analysis of voids of endodontic sealers by 3D imaging tools.
As far as authors are aware, this is the first study using nano-CT to quantify the spatial distribution of voids within the root sealers rather than the whole filling materials. The nano-CT used in this study could generate more than 9 W power at the target sample, enabling enough penetration of dentin tissue and sealers. Moreover, the high-quality imaging may be attributable to its precise overall system design, such as granite-based manipulator, an air-conditioned cabinet, an air-bearing rotating unit as well as vibration insulation of the manipulator.31 Therefore, it revealed more details regarding voids with an obvious reduction of voids in the apical third, closing to a histology-resolution imaging modality. While in micro-CT, there might be a certain number of voids which cannot be detected due to the lower image resolution. Besides, laboratory-based micro-CT was confined to the imaging contrast with respect to low-density root filling materials.29 It is probably for these reasons that significant differences could be observed among bioceramic sealers and AH Plus in this study.
Avoiding voids in the sealer is of importance for root canal treatment, especially when the shrinkage or degradation of sealers and the core materials would happen or in the cases where obturation relies more on sealers than the core materials, i.e. single cone technique. It makes sense that excellent radiopaque, well consistent, limited shrinkage and degradation, at least within the due bounds, are a prerequisite for newlydeveloped sealers to secure their clinical performance. Further researches are needed to understand the clinical impacts of these voids for endodontic treatment failure in a longer observation during intraoral functioning.
It is worth noting that nano-CT imaging modality would put an extensive strain on computer processing compared to micro-CT. The size of tested root physically restricted the achievable voxel size for scanning the whole sample and thus make it impossible to apply the nanofocus mode in this study. Besides, given potential confounding factors in the endodontic treatment, ie., the method of disinfection, obturation technique and final restoration, voids is only one of the known factors that could influence the quality of root filling quality and thus it is still too soon to decide the clinical performance of these sealers based on the current imaging analyses of the filling quality. Despite these limitations, it appears promising to use nano-CT to illuminate the low-density differences and poor contrast that exist among dentin, sealers and voids.
Conclusions
All tested sealers had less void volume in the apical third. Total Fill BC and Sure Seal Root sealers possess not only less void fraction in either forms (internal, external or combined voids), but also less void volume in either root levels than AH Plus, when treated by the single cone technique in round root canals. Additionally, although both micro-CT and nano-CT imaging allowed the observation of the internal structure of sealers in the dentin-sealer interface, nano-CT imaging showed greater ability in detecting the incidence rate of voids, void fraction and void volume than that of micro-CT imaging, suggesting its feasibility for quantitative analysis of filling quality of root canal sealers. Further study is needed to define the potential over-time changes of the voids and their degree of clinical relevance, and thus improve clinical application and long-term performance of the root canal sealers.
Funding
Financially supported by Scientific and Technological Research Council of Turkey (BIDEB 2219 under application No.1059B191501516) and São Paulo Research Foundation (FAPESP, Brazil, No. 2014/17744-5). Fellowship support from Research Foundation – Flanders (FWO, Belgium).
Contributor Information
Yan Huang, Email: yanhuangcn@gmail.com.
Berkan Celikten, Email: berkancelikten@yahoo.com.tr.
Karla de Faria Vasconcelos, Email: karlafav13@gmail.com.
Laura Ferreira Pinheiro Nicolielo, Email: laura.nicolielo@kuleuven.be.
Nicholas Lippiatt, Email: nickabeta@gmail.com.
Arda Buyuksungur, Email: barda@metu.edu.tr.
Reinhilde Jacobs, Email: reinhilde.jacobs@uzleuven.be.
Kaan Orhan, Email: call53@yahoo.com.
References
- 1.Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature - part 1. Effects of study characteristics on probability of success. Int Endod J 2007; 40: 921–39. doi: 10.1111/j.1365-2591.2007.01322.x [DOI] [PubMed] [Google Scholar]
- 2.Kandaswamy D, Venkateshbabu N, Gogulnath D, Kindo AJ. Dentinal tubule disinfection with 2% chlorhexidine gel, Propolis, morinda CitrifoliaJuice, 2% povidone iodine, and calcium hydroxide. Int Endod J 2010; 43: 419–23. doi: 10.1111/j.1365-2591.2010.01696.x [DOI] [PubMed] [Google Scholar]
- 3.Niu LN, Zhang W, Olsen M, De-Deus G, Eid AA, et al. Ability of new obturation materials to improve the seal of the root canal system: a review. Acta Biomater 2014; 10: 1050–63. doi: 10.1016/j.actbio.2013.11.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Guinesi AS, Faria G, Tanomaru-Filho M, Bonetti-Filho I. Influence of sealer placement technique on the quality of root canal filling by lateral compaction or single cone. Braz Dent J 2014; 25: 117–22. doi: 10.1590/0103-6440201302370 [DOI] [PubMed] [Google Scholar]
- 5.Keles A, Ahmetoglu F, Ocak MS, Dayi B, Bozkurt A, Orucoglu H. Comparative analysis of three different filling techniques and the effects of experimental internal resorptive cavities on apical microleakage. Eur J Dent 2014; 8: 32–7. doi: 10.4103/1305-7456.126237 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rodríguez-Lozano FJ, García-Bernal D, Oñate-Sánchez RE, Ortolani-Seltenerich PS, Forner L, Moraleda JM. Evaluation of cytocompatibility of calcium silicate-based endodontic sealers and their effects on the biological responses of mesenchymal dental stem cells. Int Endod J 2017; 50: 67–76. doi: 10.1111/iej.12596 [DOI] [PubMed] [Google Scholar]
- 7.Topçuoğlu HS, Karataş E, Arslan H, Yeter K. In vitro fracture resistance of roots obturated with epoxy resin-based, mineral trioxide aggregate-based, and bioceramic root canal sealers. J Endod 2013; 39: 1630–3. doi: 10.1016/j.joen.2013.07.034 [DOI] [PubMed] [Google Scholar]
- 8.Ørstavik D, Nordahl I, Tibballs JE. Dimensional change following setting of root canal sealer materials. Dent Mater 2001; 17: 512–9. doi: 10.1016/S0109-5641(01)00011-2 [DOI] [PubMed] [Google Scholar]
- 9.Celikten B, F Uzuntas CFC, I Orhan AIA, Tufenkci P, Misirli M, O Demiralp KOK, et al. Micro-CT assessment of the sealing ability of three root canal filling techniques. J Oral Sci 2015; 57: 361–6. doi: 10.2334/josnusd.57.361 [DOI] [PubMed] [Google Scholar]
- 10.De-Deus G, Scelza MZ, Neelakantan P, Sharma S, Neves ADAAA, Silva EEJ. Three-dimensional Quantitative porosity characterization of syringe-versus Hand-mixed set epoxy resin root canal sealer. Braz Dent J 2015; 26: 607–11. doi: 10.1590/0103-6440201300074 [DOI] [PubMed] [Google Scholar]
- 11.Huang Y, Orhan K, Celikten B, Orhan AI, Tufenkci P, Sevimay S. Evaluation of the sealing ability of different root canal sealers in the whole root canal: a combined study using SEM and micro-CT. J Appl Oral Sci 2017; 26: e20160584 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Withers PJ. X-ray nanotomography. Mater Today 2007; 10: 26–34. doi: 10.1016/S1369-7021(07)70305-X [Google Scholar]
- 13.Khoury BM, Bigelow EM, Smith LM, Schlecht SH, Scheller EL, Andarawis-Puri N, et al. The use of nano-computed tomography to enhance musculoskeletal research. Connect Tissue Res 2015; 56: 106–19. doi: 10.3109/03008207.2015.1005211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chan YH. Randomised controlled trials (RCTs)-sample size: the magic number? Singap Med J 2003; 44: 172–4. [PubMed] [Google Scholar]
- 15.Feldkamp LA, Goldstein SA, Parfitt AM, Jesion G, Kleerekoper M. The direct examination of three-dimensional bone architecture in vitro by computed tomography. J Bone Miner Res 1989; 4: 3–11. doi: 10.1002/jbmr.5650040103 [DOI] [PubMed] [Google Scholar]
- 16.Parrilli AP, Fini M, Prati C, Dummer PM. 3d micro-CT analysis of the interface voids associated with thermafil root fillings used with AH plus or a flowable MTA sealer. Int Endod J 2013; 46: 253–63. doi: 10.1111/j.1365-2591.2012.02124.x [DOI] [PubMed] [Google Scholar]
- 17.Saunders WP, Saunders EM. Coronal leakage as a cause of failure in root-canal therapy: a review. Endod Dent Traumatol 1994; 10: 105–8. doi: 10.1111/j.1600-9657.1994.tb00533.x [DOI] [PubMed] [Google Scholar]
- 18.Angerame D, De Biasi M, Pecci R, Bedini R, Tommasin E, Marigo L, et al. Analysis of single point and continuous wave of condensation root filling techniques by micro-computed tomography. Ann Ist Super Sanita 2012; 48: 35–41. doi: DOI: 10.4415/ANN_12_01_06 [DOI] [PubMed] [Google Scholar]
- 19.Xu Q, Fan MW, Fan B, Cheung GS, Hl H. A new quantitative method using glucose for analysis of endodontic leakage. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005; 99: 107–11. doi: 10.1016/j.tripleo.2004.06.006 [DOI] [PubMed] [Google Scholar]
- 20.Shemesh H, Wesselink PR. Leakage along apical root fillings with and without smear layer using two different leakage models: a two-month longitudinal ex vivo study. Int Endod J 2006; 39: 968–76. doi: 10.1111/j.1365-2591.2006.01181.x [DOI] [PubMed] [Google Scholar]
- 21.Bud MG, Wesselink PR. The quality of single cone and laterally compacted gutta-percha fillings in small and curved root canals as evidenced by bidirectional radiographs and fluid transport measurements. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009; 108: 946–51. doi: 10.1016/j.tripleo.2009.07.046 [DOI] [PubMed] [Google Scholar]
- 22.Gordon MP, Love RM, Chandler NP. An evaluation of.06 tapered gutta-percha cones for filling of.06 taper prepared curved root canals. Int Endod J 2005; 38: 87–96. doi: 10.1111/j.1365-2591.2004.00903.x [DOI] [PubMed] [Google Scholar]
- 23.Garrido AD, Lia RC, França SC, da Silva JF, Astolfi-Filho S, Sousa-Neto MD. Laboratory evaluation of the physicochemical properties of a new root canal sealer based on Copaifera multijuga oil-resin. Int Endod J 2010; 43: 283–91. doi: 10.1111/j.1365-2591.2009.01678.x [DOI] [PubMed] [Google Scholar]
- 24.McMichen FRSFR, Pearson G, Rahbaran S, Gulabivala K. A comparative study of selected physical properties of five root-canal sealers. Int Endod J 2003; 36: 629–35. doi: 10.1046/j.1365-2591.2003.00701.x [DOI] [PubMed] [Google Scholar]
- 25.Celikten B, Uzuntas CF, Orhan AI, Orhan K, Tufenkci P, Kursun S, et al. Evaluation of root canal sealer filling quality using a single-cone technique in oval shaped canals: an In vitroMicro-CT study. Scanning 2016; 38: 133–40. doi: 10.1002/sca.21249 [DOI] [PubMed] [Google Scholar]
- 26.Ersahan S, Aydin C. Dislocation resistance of iRoot SP, a calcium silicate-based sealer, from radicular dentine. J Endod 2010; 36: 2000–2. doi: 10.1016/j.joen.2010.08.037 [DOI] [PubMed] [Google Scholar]
- 27.Nagas E, Uyanik MO, Eymirli A, Cehreli ZC, Vallittu PK, Lassila LV, et al. Dentin moisture conditions affect the adhesion of root canal sealers. J Endod 2012; 38: 240–4. doi: 10.1016/j.joen.2011.09.027 [DOI] [PubMed] [Google Scholar]
- 28.Somma F, Cretella G, Carotenuto M, Pecci R, Bedini R, De Biasi M, et al. Quality of thermoplasticized and single point root fillings assessed by micro-computed tomography. Int Endod J 2011; 44: 362–9. doi: 10.1111/j.1365-2591.2010.01840.x [DOI] [PubMed] [Google Scholar]
- 29.Zaslansky P, Fratzl P, Rack A, Wesselink PR, Shemesh H. Identification of root filling interfaces by microscopy and tomography methods. Int Endod J 2011; 44: 395–401. doi: 10.1111/j.1365-2591.2010.01830.x [DOI] [PubMed] [Google Scholar]
- 30.AraujoAraújo VL, Souza-Gabriel AE, Cruz Filho AMDAM, PecoraPécora JD, Silva RG. Volume of sealer in the apical region of teeth filled by different techniques: a micro-CT analysis. Braz Oral Res 2016; 30: e27. doi: 10.1590/1807-3107BOR-2016.vol30.0027 [DOI] [PubMed] [Google Scholar]
- 31.Brunke O, Neuser E, Suppes A. High resolution industrial CT systems: advances and comparison with synchrotron-based CT : International symposium on digitalindustrial radiology and computed tomography. Vol.20 Pune: National Seminar & Exhibition on Non-Destructive Evaluation; 2011. 1–9. www.ndt.net/?id=17873. [Google Scholar]